
Abstract
Research has continued to demonstrate that exercise during pregnancy is safe. Growing evidence supports that exercise during pregnancy is beneficial for mother and fetus during gestation, with benefits persisting for the child into adulthood. Regardless of income or socioeconomic status, exercise during pregnancy is associated with increased incidence of full-term delivery. Additionally, normalization of birth measures, such as birth weight, occurs when women perform regular exercise throughout gestation. Measures of growth and development further indicate that exercise during pregnancy does not harm and may stimulate healthy growth throughout childhood. Measures of cognition and intelligence demonstrate that exercise during pregnancy causes no harm and may be beneficial. Overall, the benefits of exercise during pregnancy decrease the risk of chronic disease for both mother and child.
Introduction
In 2014, 41 million children were reported to be overweight or obese. 1 Being overweight or obese increases the risk of developing type 2 diabetes mellitus and cardiovascular disease (CVD).2–4 In part, the increased prevalence of obesity, overweight, and diabetes is due to negative lifestyle habits (ie, physical inactivity, diet lacking fruits and vegetables).3,4 Therefore, positive lifestyle habits (ie, physical activity) may act as a nonpharmaceutical therapy for obesity and overweight, thus delaying or preventing the onset of type 2 diabetes and CVD. Numerous physical activity interventions are being done to treat and prevent these conditions in children; however, the earliest intervention to treat these conditions is during pregnancy.
Reports state that over half of pregnant women in the US and Norway and 85% in Canada participate in physical activity during pregnancy.5–8 Women who exercise throughout gestation show significantly decreased risk of preeclampsia, hypertension, gestational diabetes mellitus (GDM), weight gain, rate of spontaneous abortion, congenital abnormalities, and incidence of preterm labor, and offspring have normal growth and development.9–16 The developmental origins hypothesis states that the in utero environment influences, or programs, fetal organ development, which has implications for the infants after birth into adulthood. 17 Since there is a growing body of evidence supporting the safety and efficacy of maternal exercise for the offspring, this article provides a review of human studies related to physical health of offspring exposed to maternal exercise throughout gestation and the risk of developing diseases later, such as GDM.
Gestational Age at Birth
Some research suggests that women who exercise may be more likely to deliver closer to the estimated due date.14,18–20 Although there are many studies that have compared gestational age between groups of women who exercise or not during pregnancy, most exercise was below the current recommended guidelines. The current guidelines of many nations suggest that pregnant women participate in at least 150 minutes per week of moderate-intensity aerobic activity.21–26 Three intervention studies have met the current guidelines for the frequency, intensity, and duration of exercise throughout pregnancy, two of which found no differences in gestational age between exercise and control groups.27,28 Furthermore, one study utilized aerobic activity only 28 and two studies used aerobic with resistance27,29 exercise to meet the guidelines. One of these studies found no difference in gestational age between women participating in varying intensity levels (below and at recommended guidelines) of exercise relative to controls. 29 A similar study using self-reported data found no difference in gestational age at birth between high-intensity (met guidelines), low-intensity (below guidelines), and control groups. 30 Of the high-quality studies, evidence suggests that exercise, regardless of amount or intensity, does not influence the length of gestation.
In conjunction with these findings, other studies suggest that this pattern may be different for low-income minorities. Several studies have observed that women of low socioeconomic status (SES) are less likely to seek prenatal care services 31 and have a positive association with preterm birth and work activity (walking and stair climbing). 32 However, pregnant women of minority ethnicity in low SES who participate in leisure-time exercise have decreased risk of preterm birth.32–34 Another study found that moderate-intensity exercise at least 30 minutes per day in low-income African American (AA) women was associated with decreased preterm births. 35 Similar to other study populations, pregnancy outcomes for women in low income/low SES associated with the necessity of walking to work or climbing stairs show increased adverse outcomes, while choosing to walk for health is associated with positive outcomes. These data should be interpreted with caution since the exercise data are self-reported and were either below the current recommended guidelines or not reported.
Birth Measures
Numerous studies have found that exercise during pregnancy, whether acute or chronic, is not harmful to the fetus and may benefit development in utero and after birth. 36 The primary measures to assess proper growth at birth are weight, length, and circumference measures.
Birth weight, in general, may show increase,19,20,37,38 decrease,39–43 or no change28,37,44–47 in response to exercise during pregnancy. To control for some variables, we focused on those studies that used exercise throughout pregnancy at the current recommended level, which left six studies to be reviewed on this topic. Of these six studies, two found increased,20,37 three found decreased,40,42,43 and one found no differences 28 in birth weight associated with maternal exercise. One of the studies reporting an increased birth weight, within normal weight ranges, also reports increased lean body mass and decreased fat mass 40 in exercise-exposed infants relative to infants of nonexercisers. The two studies that reported increased birth weight, within normal weight ranges, found a dose response, such that higher levels of intensity in the final weeks of pregnancy are associated with lower birth weights, while lower levels of intensity are associated with higher birth weights.20,37 Additionally, one study observed that higher levels of physical activity (above the recommended guidelines of 30 or more minutes, most, if not all, days of the week) protected against both large and small for gestational age infants.48–51 This parabolic relationship between infant birth weight and chronic disease morbidity later in life is of current research interest, such that small infants have an increased risk of developing CVD, type 2 diabetes, metabolic syndrome, and hypertension,52,53 while heavier infants are at an increased risk of developing obesity and type 2 diabetes.52–54 Finally, the one article that reports no difference in birth weight, regardless of exercise during pregnancy or not, is the only randomized control trial that had an exercise intervention throughout pregnancy at the recommended level of exercise, while all other articles utilized self-reported exercise. Altogether, these findings suggest that birth weight may be normalized by exercise during pregnancy; however, there are many other confounding factors of this crude measure of fetal growth. 55
In light of the fact that newborn birth weights have increased across generations, other factors related to health disparities of women may influence fetal growth as evidenced by birth weight. 54 Two large population-based cohort studies suggest that birth weight is determined mainly by nonexercise variables, such as maternal body composition, diet, uteroplacental blood flow, placental transfer of nutrients, and fetal genetics, with the influence of maternal exercise being minimal.48,56–58 These findings are supported by studies examining the influence of racial/ethnic group and physical activity on birth weight. One study examining the relationship of exercise activity in urban, low-income AA women found no association with exercise participation and low birth weight.33,34 Another study found that urban AA women have a positive association between exercise and birth weight. 59 Other research found that physical activity did not influence birth weight, but when controlling for maternal age, nationality, SES, substance use, and prenatal care, AAs were two times more likely to have low birth weight infants relative to whites. 60 However, when controlling for confounding variables, neither physical activity nor race/ethnicity influenced macrosomia, but maternal body mass index (BMI) was the main factor. 60 Despite attempts to decrease macrosomia in some populations, its occurrence is often due to cultural shifts. 61 Overall, these findings suggest that maternal exercise does not adversely influence birth weight.
Body morphometry (ie, circumferences) at birth can also be utilized as an indicator of fetal growth during gestation. In general, studies report similar morphometric parameters for newborns of both active and nonactive pregnant women. No differences are found in birth length of babies exposed or not exposed to gestational exercise.40,62–65 Three of these studies met the current guidelines for exercise level.40,48,65 One study found no differences in measurements of neonatal head circumference, abdominal circumference, and ponderal index, regardless of maternal exercise exposure, but also utilized self-reported exercise level. 40 A large Danish cohort study, using self-reported exercise level, found no differences in neonatal measures related to maternal exercise; however, they reported trends of decreasing birth length with increasing maternal exercise when controlling for confounding variables such as maternal BMI, age, and smoking (more common in lower income individuals). 48 The third study utilized an exercise intervention in physically active women, and despite lower energy intakes than recommended (ie, iron, dairy), birth measures were within normal ranges. 65 Overall, data suggest that maternal exercise does not adversely influence offspring growth measures.
Postnatal Measures
Although birth data are the most available and easiest to acquire, it does not provide a complete picture of changes that influence development after birth. 66 Studies are currently underway regarding the continued growth and development of children exposed to exercise in utero. At one year of age, there are no differences in growth measures (ie, height, weight, head circumference, chest circumference, abdominal circumference) between children exposed or not exposed to exercise in utero.15,16 Similarly, there are no differences in height and circumferences (arm, head, chest, abdominal) at five years of age, regardless of exercise exposure in utero. 67 A follow-up of children at five years of age found no differences in some measures of growth (ie, head and chest circumference); however, children exposed to exercise in utero weight less and had less fat mass relative to children from women who did not exercise while pregnant. 67 Current research is analyzing associations between body weight and fat in prepubertal children and associated factors in an effort to determine intrauterine programming toward or away from disease risk. One study finds, after adjusting for the child's BMI, age, sex, current physical activity level, and SES, that birth weight is a better predictor of percent body fat and height during childhood and adolescence compared to parental morphometries. 68 These findings support the idea that prepubertal body morphometric measures are programmed in utero.
Various measures have been used to determine offspring heart and nervous system health and development. For example, heart rate (HR) and HR variability, beat-to-beat fluctuation demonstrating cardiac autonomic nervous system maturation, are used during and after pregnancy to determine appropriate development of the fetus. Similar to an adult who is exercised trained, May et al69,70 found that exercise throughout gestation is associated with lower fetal HR and increased fetal HR variability that persists after birth. Further analysis demonstrated a dose-response relationship between maternal exercise intensity, or time, and offspring cardiac autonomic adaptation.71,72 It is important to note that the upper limit of maternal exercise was not tested in these studies; all participants trained in the moderate to vigorous range as recommended by the American Congress of Obstetricians of Gynecologists. 21 The differences in cardiac autonomic regulation are attributed to exercise exposure in utero since no other variables (ie, maternal age, maternal BMI, maternal education, etc.) are significantly associated with these findings.69,70 In addition, children exposed to exercise in utero exhibited no evidence of CVD into adulthood. 73 The persistence of healthy heart measures of offspring through childhood into adulthood supports the premise of prenatal programming.17,74
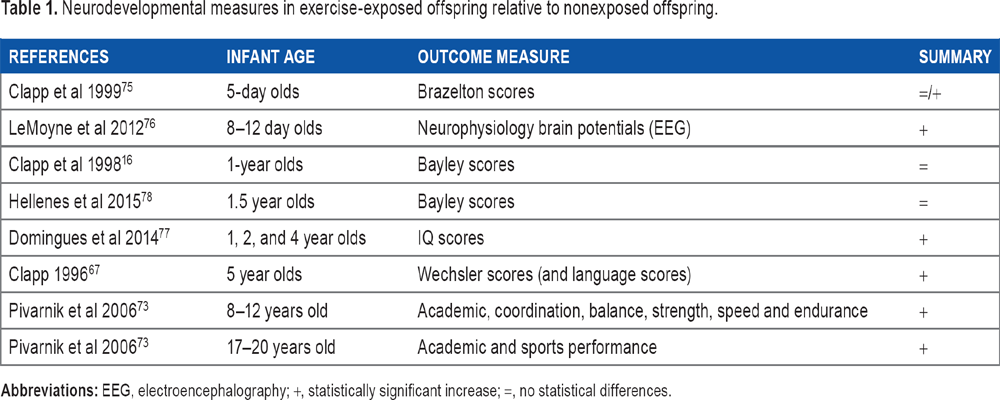
Other studies have used measures of neuromotor, cognition, and intelligence to determine if neurodevelopment is improved in offspring due to maternal exercise exposure. Overall, findings have been positive (Table 1) with most measurement tools: Brazelton scale, a measure of neonatal behavioral responses and neurodevelopment; 75 neurophysiological brain potentials; 76 intelligence quotient (IQ); 77 and Wechsler test scales. 67 Two studies showed equivalent cognition between exercise-exposed and nonexercise-exposed children, and both utilized the Bayley Scales of Infant Development, which assesses neonatal cognitive, motor, and behavioral development.16,78 Cognition, however, has been found to be associated with SES, mediated by environmental factors. 79 Furthermore, research shows that more education and higher SES are associated with exercise during pregnancy.5,80–86 Similar to the exercise and pregnancy studies, other studies have found that the fetus or children with slower HR and increased HR variability are associated with positive psychomotor and language developmental outcomes at 8 and 12 months of age, 87 2 years of age, 36 and 3 years of age 36 and have faster reaction times and attention during a task88,89 than children of similar age. Altogether, these findings support that exercise while pregnant may be beneficial to cardiac and neuromotor development of offspring.
Neurodevelopmental measures in exercise-exposed offspring relative to nonexposed offspring.
Gestational Diabetes
Being overweight or obese can lead to development of type 2 diabetes.3,4,90 Baeten et al 91 observed that one-third of women of reproductive age are overweight. This condition during pregnancy is similar to the nonpregnant state 10 and increases the risk of developing GDM. GDM is defined as the onset or first recognition of diabetes during pregnancy and is related to adverse maternal and neonatal health outcomes.92,93 Women with GDM and borderline GDM have increased risk of negative long-term effects on maternal and neonatal health.10,94 Gestational diabetic women and borderline GDM 93 have an increased risk of perinatal complications such as preeclampsia, 93 C-section, and induced delivery. 68 A recent study of primiparous women observed that GDM diagnoses were greater among women in lower SES levels. 95 They also found that the incidence of GDM was increased in women older than 35 years of age, with a greater incidence in those falling in lower SES levels. However, younger women had similar GDM incidence rates across all SES levels. Furthermore, the incidence of GDM was greatest in women of Asian background who were older and fell within the lowest levels of SES. 95 GDM also increases the risk of maternal development of type 2 diabetes, with 40% of GDM pregnancies diagnosed with type 2 diabetes postpartum. 93 Diabetes, or borderline diabetes, during gestation affects the intrauterine environment. At delivery, there are complications, such as macrosomia, shoulder dystocia, neonatal hypoglycemia, and hyperbilirubinemia.68,93 It has been suggested that GDM could affect the intrauterine environment, increasing the genetic risk of developing childhood obesity and/or type 2 diabetes in adulthood. 93
Physical activity during pregnancy, however, decreases the risk and incidence of GDM, in part by decreasing excessive gestational weight gain and stimulating a better control of glucose metabolism. 92 This phenomenon is also true for high-risk groups such as women who are overweight or obese prior to pregnancy, especially those who are inactive. Physical activity starting at the beginning of pregnancy can be used as an early therapy to prevent excessive weight gain and GDM. Women who develop GDM during pregnancy can utilize physical activity as an adjunctive therapy and are able to decrease their insulin therapy and thus have better metabolic control compared to sedentary pregnant women. 42
Conclusion
Evidence continues to grow in support of the notion that exercise during pregnancy is beneficial for fetal health and well-being, extending into childhood. Benefits for offspring are observable related to body weight and composition, cardiovascular health, and nervous system development. Exercise during pregnancy may elicit a prenatal programming effect, creating a healthy environment in utero during a critical time of organ development. Women of various SES and BMI can adopt healthy lifestyle behaviors that can positively impact postnatal health and decrease their child's risk of developing chronic diseases such as obesity, diabetes, and CVD.
Footnotes
Author Contributions
Conceived and designed the experiments: LM, CM. Analyzed the data: LM, CM, ORR. Wrote the first draft of the manuscript: LM, CM. Contributed to the writing of the manuscript: LM, CM, ORR. Agree with manuscript results and conclusions: LM, CM, ORR. Jointly developed the structure and arguments for the paper: LM, CM, ORR. Made critical revisions and approved final version: LM, CM, ORR. All authors reviewed and approved of the final manuscript.