
Abstract
Background:
Urinary tract infections and reproductive tract infections pose significant health risks, particularly among women living in challenging conditions. Unhygienic menstrual practices can exacerbate these risks, impacting physical and psychological well-being.
Objectives:
This study assessed the association between unhygienic menstrual care and self-reported urinary tract infection/reproductive tract infection symptoms among refugee women. In addition, it explored the association between these symptoms and mental health, specifically depressive symptoms.
Design:
This study adopted a cross-sectional observational design.
Methods:
This study was conducted between January and March 2023, involving 387 reproductive-age refugee women. Data collected included sociodemographic information and urinary tract infection/reproductive tract infection symptoms. In addition, we used the Menstrual Practice Needs Scale to evaluate menstrual hygiene practices and the Patient Health Questionnaire-9 for depressive symptoms. Statistical analysis was performed using Python version 3.9.12.
Results:
Of 387 refugee women, 92.25% reported having urinary or reproductive tract infection symptoms in the previous 3 months. Factors like older age (odds ratio = 1.764, 95% confidence interval = 1.083–2.873, p-value = 0.023), lower family income (odds ratio = 0.327, 95% confidence interval = 0.138–0.775, p-value = 0.011), lower educational level (odds ratio = 0.222, 95% confidence interval = 0.068–0.718, p-value = 0.012), and being married (odds ratio = 0.328, 95% confidence interval = 0.188–0.574, p-value < 0.001) were significantly associated with urinary or reproductive tract infection risk. Difficulties obtaining menstrual products and thus reusing them increased the odds of urinary or reproductive tract infection diagnosis (odds ratio = 2.452, 95% confidence interval = 1.497–4.015, p-value < 0.001). Women with urinary or reproductive tract infection symptoms exhibited higher Patient Health Questionnaire-9 scores than those without (12.14 ± 5.87 vs 9.99 ± 5.86, p-value < 0.001, respectively).
Conclusion:
This study highlights a high prevalence of urinary or reproductive tract infection symptoms among refugee women residing in camps in Jordan, which was associated with poor menstrual hygiene practices and depressive symptoms. To reduce the urinary tract infection/reproductive tract infection burden in marginalized communities, public health initiatives should enhance healthcare accessibility, provide reproductive education, and promote holistic well-being practices for refugee women.
Keywords
Introduction
Urinary tract infections (UTIs) and reproductive tract infections (RTIs) are global health issues that have a significant impact on individual well-being.1,2 UTIs, which are commonly caused by Escherichia coli and Klebsiella species, result in symptoms like dysuria, lower abdominal discomfort, frequency, and urgency. 3 Despite the existence of effective treatment options, UTIs remain a public health issue, as 50% of women have recurrent infections on an annual basis. 3 On the other hand, RTIs encompass infections that affect the reproductive system and are classified as part of communicable diseases primarily spread through sexual contact. 4 Nevertheless, they can also be transmitted from endogenous infections or iatrogenic via unsafe abortions and suboptimal delivery procedures. 4 Chlamydia and gonorrhea are the primary causative agents of RTIs. 4 Women with RTIs often complain of different symptoms, ranging from simple backache and lower abdominal pain to genital ulcers, vulvar itching, inguinal swelling, abnormal vaginal discharge, burning sensation, and dyspareunia. 4
The consequences of RTIs extend beyond the physical illness as they can lead to complications like infertility and adverse pregnancy outcomes.5,6 Therefore, addressing both UTIs and RTIs is crucial for safeguarding women’s health and overall well-being. In refugee camps with limited healthcare facilities and substandard living conditions, the challenges posed by UTIs and RTIs are further exacerbated. Displaced populations in these settings encounter obstacles, including compromised practices, economic instability, and psychological distress. 7 One crucial aspect of women’s health in refugee camps is managing hygiene effectively, and in these situations, there are complex challenges related to menstrual hygiene management (MHM). Many women face the issue of access to menstrual products and thus adopt unhygienic practices; for instance, a study conducted on Rohingya adolescent girls living in a refugee camp in Bangladesh revealed that more than 50% of women used clothes during menstruation, and notably, 10.89% used only underwear without absorbents. 8 These practices, such as reusing materials, greatly increase the chances of infections, including UTIs and respiratory tract infections (RTIs).
In Jordan, the substantial gap in public education, healthcare services, and regulations on antibiotic dispensing without a prescription has created an important issue to tackle. Refugee camps have witnessed a tremendous rise in antibiotic use, exacerbating the problem of antibiotic resistance.9,10 In addition, despite prescribers generally having a good understanding of antimicrobial resistance in Jordanian camps, it has been shown that this knowledge is often inadequately considered in prescribing behaviors.10,11
Building on alarming menstrual challenges faced by Rohingya adolescent girls in refugee camps, where only 12% had basic menstrual hygiene knowledge, 17.82% used disposable sanitary pads, and 67% lacked healthcare access during menstruation,8,12 our study addresses the pressing women’s menstrual health concerns in refugee settings. Specifically, we aim to evaluate the association between unhygienic menstrual care, using the Menstrual Practice Needs Scale (MPNS-36), and the self-reported UTI and RTI symptoms in refugee camps in Jordan. The secondary aim is to understand the association between these self-reported symptoms and mental health, particularly depressive symptoms. Our hypothesis suggests that symptoms of urinary or reproductive tract infection (U/RTI) are linked to sociodemographic variables, poor menstrual hygiene habits, and elevated Patient Health Questionnaire-9 (PHQ-9) scores. The findings from this research will offer insights into the health risks that women encounter in refugee camps, particularly regarding UTIs and RTIs, as well as highlight how menstrual hygiene practices can exacerbate these risks in these marginalized areas.
Methods
Study design and setting
This cross-sectional study was conducted among women residing in refugee camps across Jordan between January and March 2023. We included participants from 10 United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) camps in Jordan that are officially recognized. We predominantly recruited women from Jerash, Talbieh, Baqa’a, Souf, and Jabal el-Hussein camps, each of which represents unique challenges. In a 2023 FaFo report, ⩾50% of Jerash camp residents were living below the national poverty line, and many were without health insurance, making it the most impoverished camp. Similar poverty and insurance issues were found in Talbieh camp. Despite being the largest, Baqa’a camp ranked the second in unemployment and the third in poverty. Souf camp also had unemployment issues, ranking the second in its household size and female unemployment. Finally, severe overcrowding and economic challenges were prevalent in Jabal el-Hussein camp. Our goal was to capture these various socioeconomic challenges and increase the generalizability of our findings by including multiple camps.
In accordance with the ethical guidelines, participants’ data were handled confidentially, as no personal identifying information was collected, and data access was limited to the research team. All participants were fully informed of the study purpose, the voluntary nature of participation, and the right to withdraw at any point. Ethical approval was obtained from the ethics committees of Jordan University Hospital, and the appropriate institutional review board (IRB) approved the study proposal (approval number 102023588; 5 January 2023). The study was conducted in compliance with the Declaration of Helsinki. Participants also consented by appending their signatures on the consent forms. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Guidelines were followed when preparing the manuscript.
Participants, sampling, and sample size
The study population involved women living in one of the 10 UNRWA registered camps, and convenience sampling technique was utilized. The eligibility criteria were adult females aged 18 years and older living in refugee camps and provided informed consent to participate. The exclusion criteria were women who had not had menstruation in the past 6 months, pregnant women, postmenopausal women, females younger than 18 years old, and those with three or more unanswered questions on the MPNS-36 questionnaire.13,14 Considering an 80% statistical power, a 95% confidence interval (CI), and a 5% margin of error, a minimum of 384 participants were required to achieve a statistically robust analysis. This calculation was based on the standard formula for sample size estimation in observational studies. 15 Using Epi Info and considering a 95% CI, and a 5% margin of error, a minimum of 384 participants were required to achieve a statistically robust analysis. 16
Data collection
Given the challenges associated with refugee camps’ accessibility and the strict security regulations, several data collection methods were employed to ensure sample representativeness. These included face-to-face interviews, where trained interviewers conducted in-person interviews to gather data directly from participants, ensuring a personal connection and understanding of responses. In addition, electronic questionnaires using Google Forms® distributed through online platforms, allowing for broader reach and convenience for participants. Also, we collaborated with women’s associations within the camps to distribute the survey to enhance engagement and participation. For illiterate participants, personalized interviews were conducted to ensure effective communication and explanation of the survey.
Initially, a pilot study was conducted with a convenience sample of 22 participants who met the inclusion criteria, and those were excluded from the main study. This pilot study aimed at assessing the clarity, comprehensibility, and cultural acceptability of the questionnaire items. In addition, Cronbach’s alpha was calculated to evaluate the internal consistency of the questionnaire. Participants were encouraged to provide feedback on the survey for further refinement. Notably, four questions related to menstrual practices were omitted since most participants misunderstood them and provided inconsistent responses.
Questionnaire development, variables, and data sources
The questionnaire employed in this study underwent a comprehensive validation process to ensure its accuracy and effectiveness as a data collection tool. An expert panel of consultant gynecologists at Jordan University Hospital and the research team assessed the questionnaire for face and content validity. The questions were meticulously designed to capture all essential data required to achieve the study objectives. The questionnaire comprised distinct sections, each serving a specific purpose in gathering comprehensive information. These included sections on sociodemographic variables, urinary and genital symptoms (U/RTI symptoms), menstrual hygiene practices, and depression symptoms.
Sociodemographic variables
In the first section, participants were asked about their age, marital status, place of residence, age at marriage, number of children, age at menarche, individual and paternal level of education, employment status, insurance type, monthly income amount, and last menstrual period. Then, two questions were adopted from a previous study to assess period poverty, and these questions were translated to Arabic and back-translated into English to validate the accuracy of the translations. The first question was: “In the past 12 months, have you struggled to afford menstrual products (such as sanitary pads or tampons)?” Participants who answered affirmatively were then asked: “Do you struggle to afford menstrual products every month?” Based on these questions, participants were categorized into three groups: those experiencing period poverty every month, those who experienced period poverty in the past year but not every month, and those who never experienced period poverty. 17
U/RTI symptoms
The survey also included a section assessing the urinary and genital symptoms experienced by the participants during the last 3 months. This section was developed based on an extensive literature review and a study by Ademas et al. 4 It incorporated seven binary (yes/no) questions for several symptoms, including burning micturition, vaginal discharge, genital itching, low back pain, lower abdominal pain, genital ulcers/lesions, and self-reported diagnosis of a urinary/genital infection. Based on the syndromic management of RTI recommended by the World Health Organization in low-income and limited resources areas,18,19 women with one or more positive symptoms were presumed to have an RTI. In addition, participants were asked about their use of antibiotics in the past 3 months to treat urinary or genital infections and whether it was prescribed by a physician or not. Participants were also asked to provide their opinion on the statement: “Antibiotic overuse and misuse are two main reasons for antibiotic resistance,” using a 5-point Likert-type scale ranging from strongly agree to strongly disagree.
Menstrual hygiene practices
The MPNS-36 was used to assess menstrual hygiene practices. 13 This 36-item validated instrument utilized a 4-point Likert-type scale (never, sometimes, often, always) to evaluate various aspects of menstrual hygiene, including material and home environment needs, transport and school environment needs, material reliability concerns, change and disposal insecurity, reuse needs, and reuse insecurity. 14 The English version of the MPNS-36 was translated and back-translated into Arabic by a bilingual healthcare professional. Reliability analysis using Cronbach’s alpha demonstrated internal consistency across the different subscales, as it was found to be 0.834 for material and home environment needs, 0.795 for transport and school environment needs, 0.865 for material reliability concerns, 0.856 for change and disposal insecurity, 0.924 for reuse needs, and 0.990 for reuse insecurity.
Depression symptoms
We also utilized the Arabic translation of the PHQ-9, 20 which is a validated depression screening tool composed of nine items that assess the frequency and severity of depression symptoms experienced over the past 2 weeks. Participants rated their symptoms on a 4-item scale: “not at all” (0), “several days” (1), “more than half of the days” (2), and “nearly every day” (3). The total score, ranging from 0 to 27, determined the level of depression, categorized as normal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), or severe (20–27). Its reliability was confirmed in the pilot study with a Cronbach’s alpha of 0.911, indicating its effectiveness in assessing depressive symptoms.
Statistical analysis
Basic parametric measures were used to describe our data, such as means ± standard deviations (SD) for numerical variables and count with percentages (n, %) for categorical variables. Simple logistic regression was performed to estimate odds ratios (ORs) and their CIs. This allowed us to assess the impact of different variables on the diagnosis of U/RTI). An independent t-test was conducted to compare the mean different scores on the diagnosis of U/RTI, and Cohen’s d was used to estimate the effect size of significant scores. Data were analyzed utilizing Python (version: 3.9.12) with Jupyterlab as an environment (version: 3.3.2). For data wrangling, we used NumPy and Pandas packages (versions: 1.21.5 and 1.4.2, respectively), while all statistical tests were applied using Pingouin (version: 0.5.3). Matplotlib and Seaborn were used for visualizing our data (versions: 3.6.0 and 0.11.2, respectively).
Results
A final cohort of 387 women who were residing in refugee camps in Jordan were included in the study. Their mean age was 33.16 ± 9.52. The participants were divided as follows: 264 (68.39%) married, 95 (24.61%) single, 18 (4.66%) divorced, and 9 (2.33%) widowed individuals. The average number of children per woman was 3.68, with a maximum of 11 children. Notably, only 15 (3.34%) women who were not single did not have any children. The mean monthly income was 318.30 ± 200.14 JoD. On average, a family comprised 5.82 ± 2.31 individuals, and each family earned an average of 65.14 ± 59.09 JoD monthly. The mean age of marriage for the subjects was 20.60 ± 4.33 years. Only 13 (3.36%) of the women in our sample had no formal education, while 278 (71.84%) had at least a secondary education. Regarding parental education, 88 (22.80%) women reported that their fathers had not finished elementary school, and 117 (30.23%) reported that their mothers had not completed elementary school. Table 1 summarizes the demographic features of the sample.
Sociodemographic and characteristics of the participants.

Tertiary education includes technical diploma, bachelor’s degree, master’s, or doctorate; monthly household income in JOD = Jordanian Dinar; 1 JOD = 1.41 USD.
In terms of health symptoms, when asked about experiencing symptoms of U/RTI in the last 3 months, most women (357 (92.25%)) stated that they experienced at least one symptom of the following: dysuria, vaginal discharge, itchiness of the genital region, lower back pain, and lower abdominal pain. However, only 141 (36.53%) women had a confirmed diagnosis. Among all the aforementioned symptoms, vaginal discharge had the highest OR for being diagnosed with a U/RTI, followed by dysuria (OR: 7.625 and 6.901, respectively; CI: 4.422–13.148 and 4.217–11.292, respectively; p-value: < 0.001 for both). All other symptoms had a significant positive OR for U/RTI diagnosis (p-value: <0.001 for all). The frequency of each symptom can be seen in Figure 1, while Table 2 describes the OR of being diagnosed with U/RTI and different symptoms.

Frequency of different urinary and genital infection symptoms among our sample.
Analysis of urinary and genital infection symptoms with urinary tract infection diagnosis.

Comparing age groups, women aged 40–49 years had significantly higher odds of U/RTI diagnosis compared to those aged 18–29 years (OR: 1.764, CI: 1.083–2.873, p-value: 0.023). In addition, women with monthly incomes above 401 JoD had significantly lower odds of U/RTI diagnosis compared to those with incomes below 101 JoD (l). Similarly, women with full-time employment had lower odds of U/RTI diagnosis compared to those unemployed (OR: 0.499, CI: 0.25–0.997, p-value: 0.049). Looking at age at marriage, number of children, and insurance, all did not reveal a statistically significant association with being diagnosed with a U/RTI.
On the other hand, education, the father’s education, and the mother’s education were all significant factors in being diagnosed with a U/RTI. Women with tertiary education have significantly lower odds of being diagnosed with a U/RTI compared to those without education (OR: 0.222, CI: 0.068–0.718, p-value: 0.012). Moreover, single women had significantly lower odds of U/RTI diagnosis compared to married women (OR: 0.328, CI: 0.188–0.574, p-value: < 0.001). Furthermore, women with delayed menstrual cycle (1–3 and 3–6 months) had higher odds of U/RTI diagnosis compared to women who had their last menstrual cycle in less than a month (OR: 3.065, 95% CI: 1.588–5.917, p-value: <0.001 and OR: 3.751, 95% CI: 1.227–11.466, p-value: 0.02, respectively). Table 1 summarizes the OR of U/RTI diagnosis and its associated p-values and CI for various variables.
Antibiotic use
Almost one-third (30.39%) of the population took antibiotics prescribed by a healthcare professional for urinary or genital infection in the last 3 months, while 49 (12.73%) women admitted taking antibiotics for urinary or genital infection without prescription. Moreover, 165 (42.64%) women strongly agreed, and 112 (28.94%) women agreed that taking antibiotics without a prescription could be harmful and increase antibiotic resistance in microorganisms; 60 (15.50%) stayed neutral toward that statement; 35 (9.04%) disagreed; and 15 (3.88%) strongly disagreed.
Menstrual practices and urinary/genital tract infection
More than two-thirds of the participants (n = 270, 69.77%) reported reusing menstrual products. Reusing menstrual products was associated with a significantly increased OR for U/RTI diagnosis (OR: 2.452, 95% CI: 1.497–4.015, p-value: <0.001). When asked if they face difficulties obtaining menstrual products, 211 (54.66%) women stated that they face yearly difficulties, and 161 (43.63%) reported facing these difficulties monthly. Difficulties in obtaining menstrual products in the past year and every month were both significant factors affecting U/RTI diagnosis (OR: 1.759; 95% CI: 1.149–2.693; p-value: 0.01 and OR: 1.989; CI: 1.295–3.057; p-value: 0.01, respectively). The mean overall MPNS-36 score for our sample was 1.92 ± 0.52, and Table 3 shows a detailed description of its subscales and their association with U/RTI diagnosis. The overall MPNS-36 scores were significantly lower in women diagnosed with a U/RTI in the last 3 months, with a p-value of 0.006 and an effect size of 0.296. Only the material and home needs and the change and disposal insecurity subscales exhibited similar significant associations with the diagnosis of U/RTI (p-value: 0.003 and 0.024, respectively). Figure 2 further illustrates the mean values of the menstrual practice needs subscales and the overall score according to urinary/genital tract infection.
MPNS-36, PHQ-9, and previous diagnosis of UTI.

Data were represented as mean ± SD. p-value was calculated using independent sample t-test and effect size was calculated using Cohen’s d.
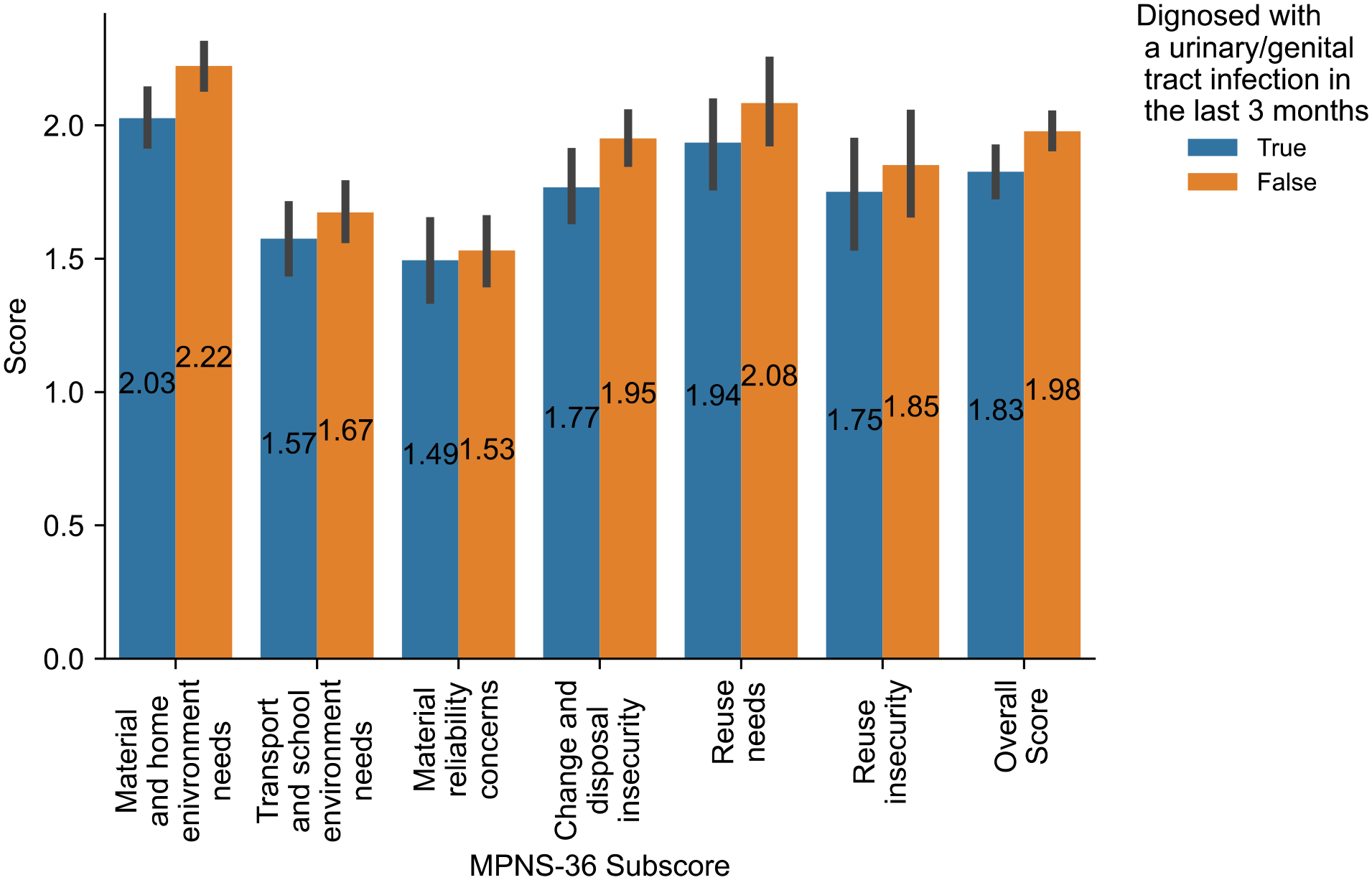
Mean value of menstrual practice needs subscales and urinary/genital tract infection.
PHQ-9
The overall mean PHQ-9 score for our sample was 10.77 ± 5.94. Women who experienced urinary/genital infection symptoms had significantly higher PHQ-9 scores (12.14 ± 5.87) compared to those who did not (9.99 ± 5.86) (p-value < 0.001). The relation between PHQ-9 and diagnosis with U/RTI is described further in Table 3. Figure 3 demonstrates the PHQ-9 depression severity and urinary/genital tract infection in the last 3 months.
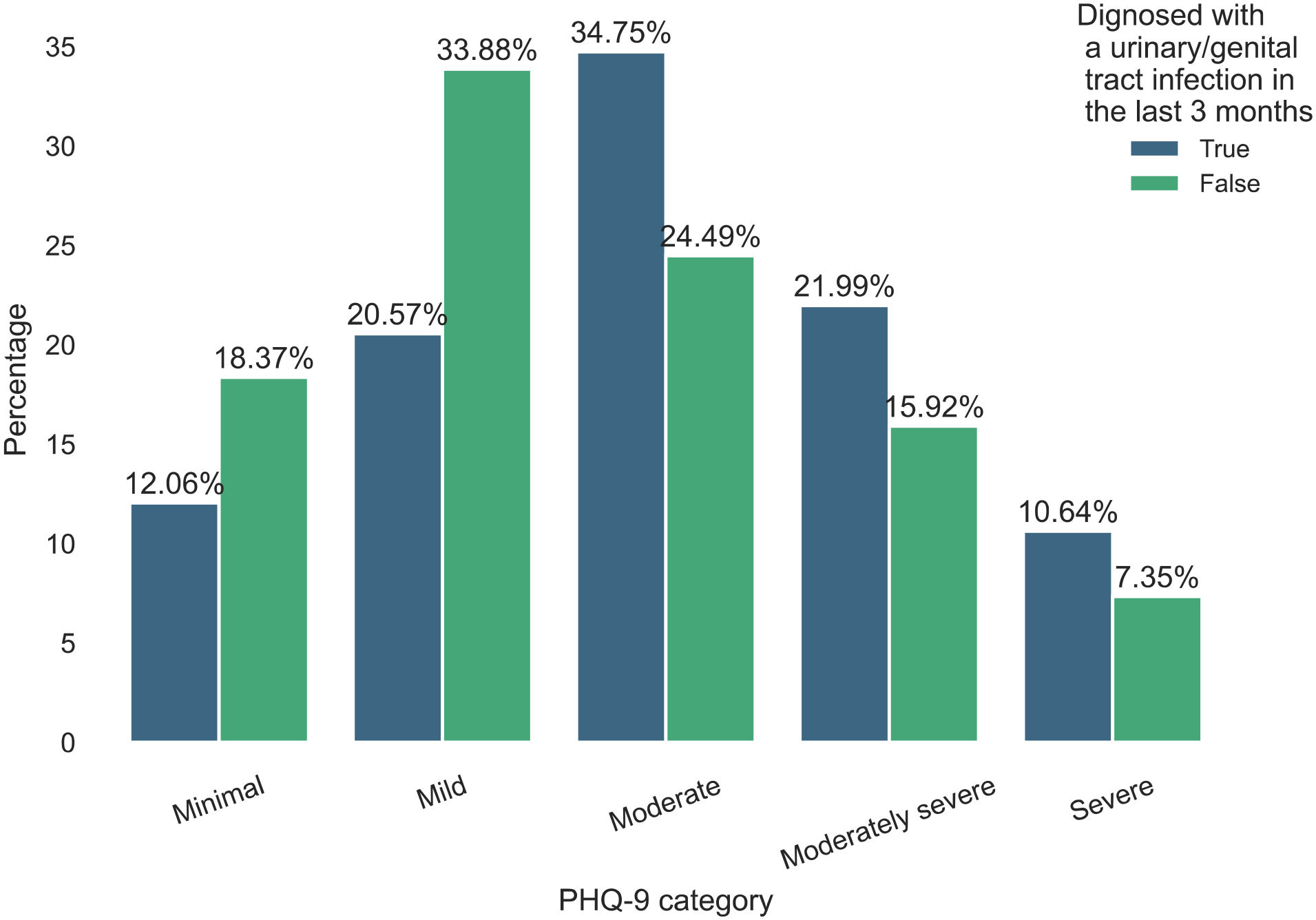
PHQ-9 depression severity and urinary/genital tract infection.
Discussion
The global burden of reproductive tract infections (RTIs) represents a significant public health challenge, with a notably higher prevalence in low-income settings. 21 Our study provides valuable insight into the self-reported prevalence of U/RTI and its associated factors among women residing in refugee camps in Jordan. More than 90% of refugee women reported U/RTI symptoms, and these symptoms were significantly associated with multiple sociodemographic and behavioral factors such as age, marital status, education level of the participants, and parents’ education level, employment status, family income, facing monthly and yearly problems in buying menstrual products, reusing materials, menstrual practices, and depressive symptoms. Indeed, women with U/RTI had significantly lower MPNS-36 scores and higher PHQ-9 scores.
Our study unveiled a high occurrence of U/RTI symptoms, as 92.25% of refugee women reported at least one symptom in the previous 3 months. The observed prevalence raises significant concern, particularly when compared to other geographic regions with similar low-income populations. In a study by Ademas et al., 4 they reported that 11% of women in urban Ethiopia had RTI symptoms in the year preceding their survey, similar to a study in Kerala, India (11.8%). 22 In contrast, a higher proportion of women (18%) reported experiencing symptoms of RTIs in a population-based study that utilized the District Level Household and Facility Survey (DLHS-3) in India. 23 A systematic review of community-based studies in India between 2000 and 2012 reported RTI prevalence rates varying from 11% to 72%. 24 Even in regions with different sociodemographic profiles, such as Hainan, China, around 20% of rural women reported at least one RTI symptom within the last 6 months. 25 This substantial difference in prevalence rates between our study and the previous literature underscores the severity of this issue within refugee camp settings. Notably, Khawaja et al. 5 studied women residing in low-income districts of Beirut, Lebanon while 42.7% of women resided in refugee camps and found that 42% of these women had at least one symptom of RTIs. A study conducted in Pakistan that examined a group of Afghan refugee women who sought medical care at basic health centers revealed that 76.7% of these women reported RTI symptoms. 6 Several challenges facing the displaced populations could potentially explain this high prevalence, including limited access to healthcare services, economic instability, poor sanitation, and overcrowding. 26
The diagnostic gap observed in our study, where less than half of the women with U/RTI symptoms had a confirmed diagnosis, necessitates a comprehensive investigation of the potential factors influencing health-seeking behaviors and healthcare accessibility among refugee women. Our finding is consistent with studies conducted in resource-constrained populations.27 –29 Several factors could elucidate this diagnostic discrepancy, including the overlapping nature of U/RTI symptoms with other health conditions, which could potentially delay seeking medical attention as women experiencing these symptoms could attribute them to other causes.30,31 Additional factors include the lack of comprehensive reproductive health education for women in vulnerable areas and the inadequate awareness of the necessity of early diagnosis and prompt management of U/RTI. 32 In addition, women with tertiary education were found to have significantly lower odds of diagnosis, which emphasizes the importance of health literacy and education on reproductive health. Verma et al. 33 also reported that women with higher educational status had a lower prevalence of RTI symptoms in urban and rural Delhi. Similarly, Bansal et al. 34 found a higher prevalence of RTIs among illiterate than literate women. Women with higher education were also previously reported to have higher treatment-seeking behaviors,33,35 which further stresses the importance of reproductive health education for U/RTI prevention and early detection. These results conform with previous research that found that disease prevention behavior is greatly affected by family income 36 and educational status.36 –38 Among Syrian refugees in Jordan, Alzoubi et al. 39 found low scores of health promotion behaviors. In 2014, Doocy et al. 40 highlighted the significant barriers to health-seeking among Syrian refugees in Jordan, primarily the cost (64.5% of households), along with barriers related to the perception of illness severity, lack of knowledge of where to access care, transportation difficulties, and other factors.
Our study identified several sociodemographic factors associated with U/RTI risk. Women between 40 and 49 years old had significantly higher odds of U/RTI diagnosis, as 44% of women in this age group had U/RTI symptoms, which aligns with previous research indicating an increased risk of U/RTIs with age.41,42 A potential explanation is that older women might have had a longer duration of sexual activity, thus increasing their exposure risk to infections. 42 Yet, other studies reported younger and primigravid women had a higher prevalence of infection,35,43 which could be attributed to differences in sexual behaviors, cultural factors, and health-seeking behaviors across populations. Furthermore, higher monthly income and full-time employment were associated with significantly lower U/RTI odds, highlighting the role of economic stability in health outcomes. These socioeconomic factors can influence healthcare-seeking behaviors, access to healthcare facilities, and the ability to afford preventive measures.
U/RTI burden in low-income settings could be attributed partially to poor MHM. 44 Our study revealed that more than two-thirds of refugee women reused menstrual products, which was associated with higher odds for U/RTI symptoms. Reusing materials is often due to economic constraints and limited access to sanitary products, as disposable materials are often too expensive for underprivileged populations.45,46 Indeed, around half the refugee women in our study reported financial difficulties in obtaining menstrual products monthly (43.6%) and during some months of the past year (54.7%). These challenges were found to be significantly associated with U/RTI diagnosis. In a prospective interventional cohort in Rwanda, vulvovaginal symptoms were significantly lower among adolescent females who used disposable pads, despite no significant change in positive urine cultures. 47
Women with U/RTI symptoms had significantly lower total MPNS-36 scores compared with participants who had no UTI diagnosis. In addition, the material and home needs subscale, which assesses the adequacy of materials and facilities for managing menstruation, had significant mean difference between participants’ previous diagnosis of UTI and those who had not. Women who reported difficulties accessing suitable materials and a conducive, hygienic environment for MHM were more likely to be diagnosed with U/RTIs. Similarly, in rural India, Baker et al. 48 reported that using latrines was associated with lower RTI symptoms compared to open defecation. Moreover, a lower mean in the change and disposal insecurity subscale, which focuses on discomfort or insecurity feelings associated with changing and disposing of menstrual materials, was associated with increased U/RTI symptoms. This elucidates that U/RTI prevention extends beyond hygienic materials availability to the perceived safety and convenience of utilizing them. In Odisha, India, changing menstrual absorbents outdoors increased the risk of bacterial vaginosis compared to using a private indoor place. 49 A qualitative study involving refugee women in Jordan and the West Bank revealed inadequate menstrual preparedness, primarily before menarche and this inadequacy was driven by practical issues like sanitary pad usage and hygiene practices, socio-cultural taboos, and variations in the timing of menstrual education. 50 Therefore, addressing the complex challenges of MHM in low-resource settings is essential to effectively reduce the burden of U/RTIs and enhance women’s reproductive health and well-being.
Our study yielded an average PHQ-9 score of 10.77 ± 5.94, and women who reported U/RTI symptoms had significantly higher PHQ-9 scores than women who did not report symptoms (12.14 ± 5.87 vs 9.99 ± 5.86, respectively). This finding highlights the interrelationship between physical health and mental well-being within the refugee community, consistent with prior studies in similar contexts.5,51 Among women in low-income neighborhoods in Lebanon using the General Health Questionnaire-12 (GHQ), mental distress was significantly associated with RTI symptoms. 5 Moreover, women seeking gynecology clinics for vaginal discharge in Pakistan were at a significantly higher risk of experiencing a common mental disorder when assessed by the General Health Questionnaire (GHQ-28) than those with other gynecological complaints. 52 Of note, vaginal discharge had the highest odds of being diagnosed with U/RTI among refugee women in our study, compared to other symptoms. Several factors may contribute to this association, as limited access to healthcare in refugee settings can lead to the persistence of symptoms, which in turn can contribute to depressive symptoms. Moreover, women who experience RTI symptoms may face cultural or societal stigma and feelings of shame, 29 which could further exacerbate depressive symptoms. Furthermore, depression can also influence health behaviors, as individuals with depressive symptoms may be less likely to seek medical care, 53 adhere to treatment regimens, 54 or practice good hygiene, 55 all of which can increase the risk of U/RTIs.
A notable proportion of refugee women reported using antibiotics for urinary or genital infections during the last 3 months, either prescribed by healthcare professionals or self-administered (30.39% and 12.73%, respectively), which has important public health implications. In a previous study conducted on refugees in Jordan, approximately half of the participants reported using antibiotics within the last 3 months. 11 Despite this, the percentage in our study appears more alarming, namely due to differences in study populations, as our sample comprised reproductive-aged females from the general refugee community, while the earlier study focused on refugees attending primary healthcare centers. Moreover, our study specifically inquired about antibiotics for urinary tract and genital infections, possibly underestimating the overall antibiotic usage for other infections. Given the previous results, public health campaigns are warranted to raise awareness about antibiotic misuse and self-prescription.
The main strength of our study is that it is the first in-depth study to tackle menstrual hygiene practices and their association with U/RTI symptoms among refugee women in the region. In addition, the research employed validated measurement tools, including the MPNS-36 and PHQ-9. Moreover, our study included a large and diverse sample of 387 refugee women from multiple camps in Jordan, enhancing the representativeness of our findings. Furthermore, developing a comprehensive data collection survey that covered sociodemographic factors, menstrual practices, mental health, and U/RTI symptoms facilitated a holistic analysis of U/RTIs and their associated factors. Nevertheless, our research is subject to certain limitations that should be taken into account during the interpretation of the results. We utilized a cross-sectional design, which limits our ability to establish causal relationships between variables. Also, we assessed U/RTI via self-reported symptoms without clinical examinations or laboratory investigations. This approach may not entirely reflect the actual prevalence of these infections, potentially introducing recall bias and variations in symptom reporting.
To address the burden of U/RTIs among refugee women, we advocate for a comprehensive approach. This includes reproductive health education, enhanced healthcare access, economic support, MHM initiatives, and mental health services. We recommend that future researchers prioritize several key dimensions to improve healthcare access and reproductive health outcomes among refugee women. We suggest employing qualitative and quantitative approaches to address the health-seeking behaviors and barriers to timely diagnosis among refugee women. In addition, we propose investigating the bidirectional relationship between mental health, U/RTI symptoms, and health-seeking behaviors to help improve refugees’ physical and psychosocial well-being. Finally, we suggest that prospective studies focus on developing and evaluating cost-effective, accessible, and sustainable reproductive health and MHM programs to reduce U/RTI risk in refugee and low-income communities.
Conclusion
In conclusion, an alarming self-reported occurrence of U/RTIs of 92.25% was observed among reproductive-age refugee women in Jordan in the 3 months before data collection. Several factors were associated with these self-reported symptoms, including age, marital status, education level of the participants, and parents’ education level, employment status, family income, facing monthly and yearly problems in buying menstrual products, reusing materials, menstrual practices measured by MPNS-36, and depressive symptoms measured by PHQ-9. Public health interventions are warranted to consider modifiable risk factors and reduce U/RTIs in underprivileged refugee communities.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241240920 – Supplemental material for Urinary and reproductive tract infection symptoms and menstrual hygiene practices in refugee camps in Jordan: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057241240920 for Urinary and reproductive tract infection symptoms and menstrual hygiene practices in refugee camps in Jordan: A cross-sectional study by Joud Al Karmi, Mohammad Ali Alshrouf, Tala A Haddad, Abdulrahman E Alhanbali, Neven Amer Raiq, Hadeel Ghanem, Omar Bassam Ibrahim, Tala Khamis and Nadia Muhaidat in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241240920 – Supplemental material for Urinary and reproductive tract infection symptoms and menstrual hygiene practices in refugee camps in Jordan: A cross-sectional study
Supplemental material, sj-docx-2-whe-10.1177_17455057241240920 for Urinary and reproductive tract infection symptoms and menstrual hygiene practices in refugee camps in Jordan: A cross-sectional study by Joud Al Karmi, Mohammad Ali Alshrouf, Tala A Haddad, Abdulrahman E Alhanbali, Neven Amer Raiq, Hadeel Ghanem, Omar Bassam Ibrahim, Tala Khamis and Nadia Muhaidat in Women’s Health
Footnotes
Acknowledgements
The authors express gratitude for the assistance provided by the governing bodies overseeing the camp, as well as the women who actively participated in our survey by dedicating their time and effort to convey their perspectives and concerns.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.