
Abstract
Polycystic ovary syndrome is a common reproductive endocrine condition that affects women of fertile age and is characterized by three main features, including hyperandrogenism, chronic anovulation, and polycystic ovaries. In addition, half of women with polycystic ovary syndrome have insulin resistance, and obesity or overweight, type 2 diabetes, hypertension, and hyperlipidemia are the most common metabolic abnormalities affecting (30%) women with polycystic ovary syndrome. Weight loss is regarded as the first-line treatment as it can potentially improve polycystic ovary syndrome parameters (androgen levels, menstrual cyclicity, lipid and glucose metabolism). However, achieving and maintaining weight loss can be challenging, and pharmacological agents could be essential to achieve optimal glycemic control and improve the endocrine disturbance associated with polycystic ovary syndrome. Glucagon-like peptide-1 receptor agonist has been demonstrated as monotherapy or in combination with metformin for managing obesity and insulin resistance associated with polycystic ovary syndrome. Yet, its effect on endocrine and metabolic parameters remains elusive, and further research is needed to close the gap. The aim is to evaluate the efficacy of glucagon-like peptide-1 receptor agonist monotherapy and/or a combined treatment between glucagon-like peptide-1 receptor agonist and metformin for improving anthropometric measurements, endocrine and metabolic parameters in lean and obese women with polycystic ovary syndrome. A systematic review of longitudinal cohort studies was conducted across databases including Ovid Medline, PubMed Central, and Cochrane Library between 2015 and 2022. Eligible studies included participants with polycystic ovary syndrome diagnosed according to the 2003 Rotterdam or the 1990 National Institutes of Health criteria. A total of eight studies including 486 patients with polycystic ovary syndrome were analyzed. The mean age was between 18 and 45 years with mean follow-up period between 12 and 32 weeks. In all these studies, results were comparable for the reduction in body mass index, waist circumference, fat mass, and visceral fat mass; however, it was more in combination therapy versus comparator. In conclusion, glucagon-like peptide-1 receptor agonists effectively reduce body weight and improve some of the endocrine and metabolic parameters of polycystic ovary syndrome. A combined treatment with glucagon-like peptide-1 receptor agonist and metformin had significant effects on weight loss and favorable results on endocrine and metabolic parameters, yet further research is needed to discover the long-term safety of combined therapy in women diagnosed with polycystic ovary syndrome and obesity or overweight.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is the most prevailing reproductive endocrine condition affecting women in their reproductive years, accounting for 10%–20% of all cases.1 –4 Approximately 50%–70% of women diagnosed with PCOS display pathophysiological changes and clinical manifestations, including insulin resistance, Luteinizing Hormone (LH)/Follicle-Stimulating Hormone (FSH) secretion disorder, metabolic abnormalities, and an increased risk of subfertility, diabetes mellitus, metabolic syndrome, and cardiovascular diseases. 5 Furthermore, established guidelines for classifying and managing PCOS include Rotterdam, Androgen Excess Society, and the National Institutes of Health (NIH). However, based on international evidence, Rotterdam 2003 criteria have been advocated as the main diagnostic guideline, which identifies the syndrome as the presence of any two out of the following criteria: (1) oligo-anovulation, (2) clinical or biochemical hyperandrogenism, (3) polycystic ovaries on ultrasound.6-8
PCOS is often underlined by insulin resistance in which 70% of obese/overweight patients with PCOS have decreased insulin sensitivity. 9 Further studies have shown that the first-line treatment of PCOS is weight loss and lifestyle modifications due to their potential to improve the endocrine and metabolic profile of these patients; however, it is challenging for patients because of their weight regain.10 –13 Therefore, pharmacological agents could be essential to achieve optimal glycemic control and to improve the endocrine disturbance associated with PCOS. Metformin is frequently used in women with PCOS and insulin resistance as it reduces hepatic glucose production and improves insulin sensitivity in addition to its glucose-lowering effect 14 . Metformin in combination with an oral contraceptive pill (OCP) is recommended as a secondary treatment in certain PCOS guidelines, as it improves insulin resistance and reduces hyperandrogenism and the clinical severity of the syndrome; however, its effect on weight loss is frequently unsatisfactory to patients.15,16 Thus, the identification of innovative, safe, and effective pharmacological-anti-obesity agents must be addressed for the improvement of fertility.
Glucagon-like peptide-1 receptor agonist (GLP-1 RA) is an incretin hormone that shares a similar effect with incretin mimetic. 17 Over the past decade, the incretin modulator has been introduced as a novel treatment for obesity and type 2 diabetes mellitus,4,18,19 as it promotes insulin biosynthesis and improves insulin resistance without causing hypoglycemia. 20 It is also associated with significant weight reduction due to its ability to regulate energy expenditure and delayed gastric emptying. In addition, it has a safe cardiovascular and renal outcome.18,17,19,20 Long-acting liraglutide and short-acting exenatide have recently been demonstrated for the management of PCOS,21 –28 as it has significant effect on weight reduction and favorable outcomes on metabolic and endocrine parameters. In addition, some studies revealed that a combination of GLP-1 RA and Metformin (MET) had the potential to improve menstrual cyclicity, insulin sensitivity, glucose metabolism, and anthropometric measurements.22,23,27,28 However, the effect of these medications on the endocrine parameters of PCOS still needs to be discovered, with a considerable gap in the available data.
The systematic review aims to highlight research conducted during the past 5 years and evaluating the efficacy of GLP-1 RA compared with metformin and/or a combined treatment between liraglutide or exenatide and metformin for improving anthropometric measurements, endocrine and metabolic parameters in lean and obese women with PCOS. It is important to note that this study will focus only on metformin and GLP-1 RA and will not include the other medications for PCOS and weight loss.
Methods
References
Search strategy and databases
Comprehensive exploration criteria combining medical subject headings, Mesh Subheadings, and relevant text words were used to screen the database as appropriate. These terms included: PCOS, ovary syndrome, polycystic syndrome, polycystic ovary, polycystic ovary disease, hyperandrogenic anovulation, Leventhal syndrome, GLP-1 RA, exenatide, lixisenatide, liraglutide, albiglutide, dulaglutide, and randomized controlled trial (RCT) or controlled clinical trial (CCT).
The search was restricted to human studies published from 2015 to 2022 in English language. Electronic databases including Ovid Medline, PubMed Central, and Cochrane Library were searched on 15 November 2022 (updated: 10 June 2023). In addition, all the selected articles were uploaded to endnotes for automatic deduplication screening and reference management. Furthermore, references from included studies were also analyzed for more relevant articles.
Inclusion criteria
The selection of articles for this systematic review was guided by the Participant, Intervention, Comparison, Outcome, and Study Type (PICOS) framework.
Participants: Females aged 18 and above with a diagnosis of PCOS. We included articles that used Rotterdam, NIH, or NICHD criteria for diagnosing PCOS.
Intervention(s): GLP-1 RA.
Comparison: Compared with metformin or placebo.
Outcomes: Changes in anthropometric measurements, insulin resistance, hyperandrogenism, and metabolic and endocrine parameters.
Study design: RCT studies, such as randomized open-label trials, prospective randomized trials, double-blind controlled trials, and single-blind controlled trials.
Exclusion criteria
Study design: Systematic review, meta-analysis, and animal studies were excluded.
Participants: Postmenopausal period, pregnant women, and women with a diagnosis of diabetes mellitus or cardiovascular disease (CVD) and chronic kidney disease (CKD).
Intervention: GLP-1 RA versus dietary interventions or if GLP-1 RA or metformin were with other treatments were excluded.
Study selection and risk-of-bias assessment
Screening of articles on abstracts and the full text was carried out by one independent reviewer (S.B.) to identify eligible studies. Discrepancies were resolved through consensus or by a second reviewer (R.B.). The methodological quality of included studies was assessed by two independent reviewers (S.B. and R.B.) on individual criteria related to external validity (methodology, inclusion/exclusion criteria, and appropriateness of measured outcomes) and internal validity (detection, selection and reporting bias, confounding, statistical analyses, and study power). Risk-of-bias assessment was resolved through discussion between reviewers to reach a consensus.
Data analysis
Information was collected on general details (authors, reference/source, year of publication, and setting), participants (anthropometric measurements, hyperandrogenism, intervention, and endocrine and metabolic parameters.), and results (point estimates and measures of variability/effect). Due to the large number of outcomes, these data were extracted manually using Microsoft Excel. A narrative description of results is presented according to each outcome category.
Results
Search results
A total of 403 articles were selected from the search as illustrated in Figure 1. Following that we excluded 303 duplicates, 29 studies were excluded based on abstracts, and an additional 63 studies were excluded based on full-text assessment. Ultimately, eight studies satisfied our inclusion criteria.

PRISMA flowchart and selection of studies.
Characteristics of included studies
The features of the selected articles are outlined in Table 1. One study is comparing metformin versus liraglutide, two studies comparing combination treatment of metformin and liraglutide versus liraglutide, two studies comparing between liraglutide and placebo, one study comparing between exenatide and metformin, and one study comparing combination exenatide and metformin versus metformin. These studies were conducted in women with PCOS aged between 18 and 45 years. The mean follow-up time ranged between 12 and 32 weeks.
Characteristics of included studies.

BMI: body mass index; BID: twice a day; QD: every day; TID: 3 times daily; QW: once a week; OD: once daily; NIH: National Institutes of Health; RCT: randomized controlled trial; NICHD: National Institute of Child Health and Human Development.
Changes in anthropometrics, and endocrine and metabolic parameters
The role of GLP-1 RAs has been evaluated in several small studies either alone or in combination with metformin in overweight/obese women with PCOS. Table 2 provides a summary of clinical studies that assessed the weight-reducing effects of GLP-1 RAs as one of their outcomes.
A summary of clinical studies with anthropometric outcomes.
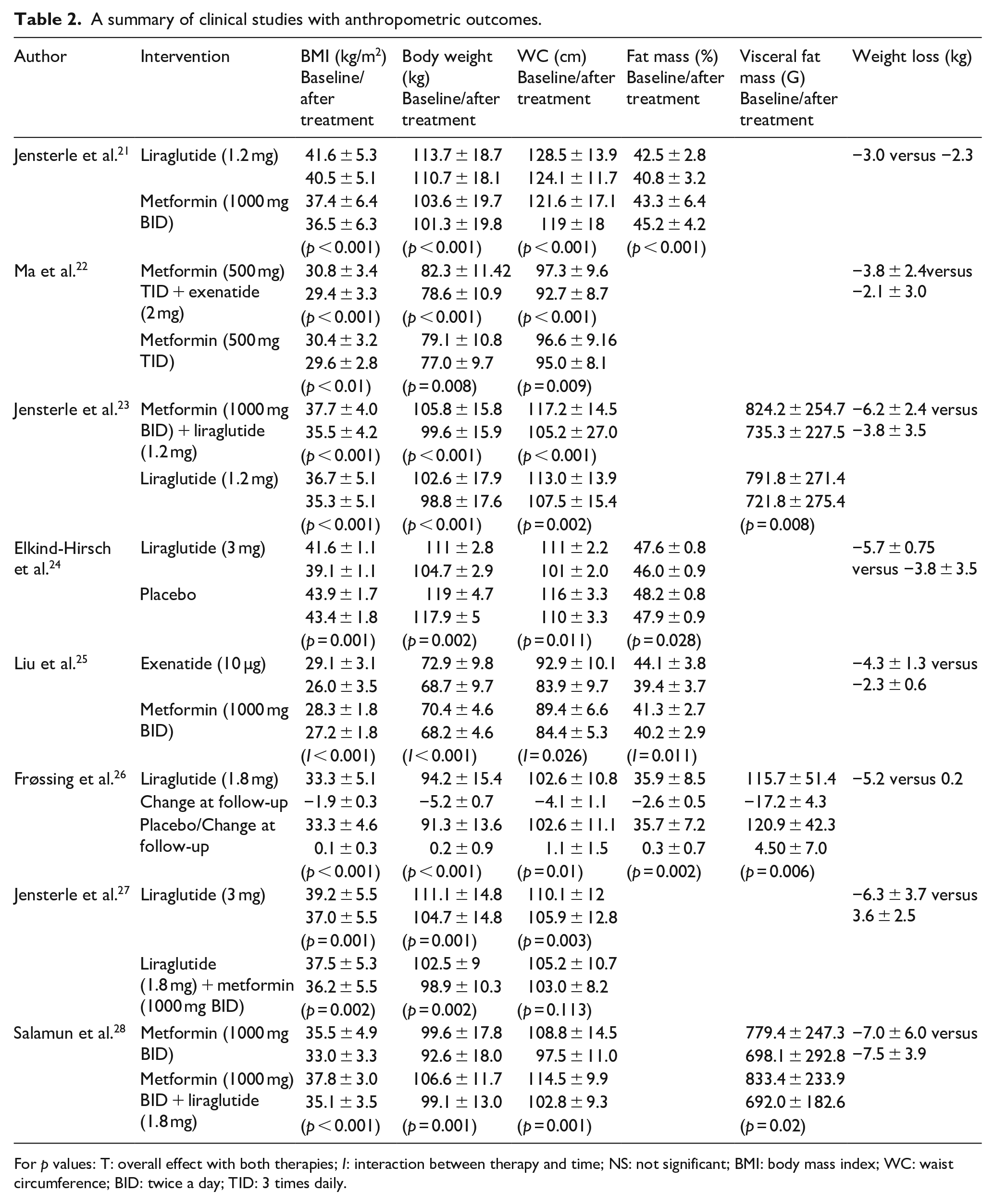
For p values: T: overall effect with both therapies; I: interaction between therapy and time; NS: not significant; BMI: body mass index; WC: waist circumference; BID: twice a day; TID: 3 times daily.
In all these studies, results were comparable for the reduction in body mass index (BMI), waist circumference (WC), fat mass, and visceral fat mass. One study showed that WC reduced by 4.63 ± 4.4 cm (combination group) versus 1.72 ± 3.07 cm (metformin-only group). 22 On the contrary, Jensterle et al. 27 showed that WC in the liraglutide group exhibited a greater reduction compared with the combination group. Four studies showed weight reduction in nearly 5%. It was seen in 59.1% in the combination group (liraglutide and metformin) versus 42.9% of patients in the liraglutide-only group. 23 It was also seen in about 69.2% in combination group (liraglutide and metformin) versus 57.1% metformin-only group. 28 One study showed similar achievement in 55% and 14% of participants in the liraglutide and placebo groups, respectively. 26 In addition, 47% of patients achieved more than 5% weight loss with exenatide therapy within the initial 12 weeks, contrasting with the metformin group where a similar weight loss was not observed. Notably, the reduction in WC was more pronounced in patients treated with exenatide compared with those on metformin. 25
Table 3 summarizes the endocrine parameters in women with PCOS. Five studies showed the reduction in total testosterone (TT) with improvement in Sex Hormone Binding Globulin (SHBG) levels. This was more with GLP-1 RA versus comparator. Three studies looked at menstrual cycle frequency, and two of these studies showed improvement.
Endocrine parameters.

For p values: T: overall effect with both therapies; I: interaction between therapy and time; NS: not significant; BID: twice a day; TID: 3 times daily.
Information on the metabolic effects evaluating the impact of GLP-1 RA on different metabolites in women with PCOS is summarized in Table 4. Out of eight studies, seven studies showed the reduction in Homeostatic Model Assessment for Insulin Resistance (HOMA-IR)-a measure of insulin resistance with GLP-1 RA either alone or in combination versus its comparator and it reached statistical significance in four of them. Frøssing et al.’s study was the only study that didn’t show any discernible difference between treatment groups were observed concerning markers of insulin resistance. Fasting total, High density Lipoprotein (HDL) and Low density Lipoprotein (LDL) cholesterol, and triglycerides (TG) did not change much in these studies.
Metabolic outcomes.

BID: twice a day; NS: not significant; TID: 3 times daily; BID: twice a day.
Discussion
The systematic review identified 8 RCTs or CCTs encompassing 486 overweight/obese women with PCOS. These trials evaluated the impact of GLP-1 RA alone or in combination with metformin on anthropometrics, and metabolic and endocrine parameters. In all these studies, with mean follow-up of 12–32 weeks’ duration, results were comparable for reduction in BMI, WC, fat mass, and visceral fat mass. Hence, liraglutide was more effective in decreasing body weight, BMI, and WC than metformin, indicating the potential superiority of GLP-1 RAs, particularly liraglutide, over metformin in these specific physical parameters. 21 Jensterle et al. 21 showed weight loss of 3 kg versus 2.3 kg with liraglutide compared with metformin. Frossing et al. 26 compared liraglutide (3 mg) with placebo and showed weight loss of 5.2 kg versus 0.2 kg with 4.1 cm versus 1.1 cm reduction in WC. Elkind Hirch et al. 24 showed the reduction in 5.7 kg versus 3.8 kg comparing liraglutide (3 mg) versus placebo. Another study comparing exenatide to metformin found that both treatments resulted in weight loss, but exenatide significantly affected body weight and BMI. About 47% of patients in exenatide group lost >5% of their initial body weight and body mass compared with the metformin group. 25
Combination therapy of metformin and liraglutide was shown to be more effective. Jensterle et al. 23 showed that combining liraglutide (1.2 mg) and metformin versus liraglutide (1.2 mg) only gave significantly more weight loss (6.2 kg versus 3.5 kg) and reduction in WC (p ⩽ 0.001). Another trial by same author showed that liraglutide (3 mg/day) was more effective in reducing BMI and WC. 27 On the contrary, Salamun et al. 28 demonstrated reduction in weight, BMI, and WC in both arms.
Two studies showed that weight loss of more than 5% was seen in liraglutide and metformin versus liraglutide-only group, 23 and also with combination group (liraglutide and metformin) versus metformin-only group. 28
Frossing et al. 26 showed similar achievement in 55% and 14% of patients in the liraglutide and placebo arms, respectively.
Overall, several studies demonstrated that a combination of GLP-1 RA and metformin has superior effects on weight loss. This is probably due to each treatment’s complementary mechanism of action, with GLP-1 RA promoting satiety, decreased food intake, and weight loss. 17 At the same time, metformin enhances insulin sensitivity and reduces hepatic glucose uptake. 14 For example, a study by Liu et al. reported that the combination treatment resulted in significantly more extensive weight loss than liraglutide alone (6.2 kg versus 3.8 kg). 25
In addition to weight loss and the other anthropometric changes, GLP-1 RA and metformin were evaluated regarding endocrine and metabolic parameters of PCOS. Several studies showed that GLP-1 RA had a superior effect on metformin in improving lipid profile, blood pressure, and insulin sensitivity in women diagnosed with PCOS and obesity or overweight. Jensterle et al. 23 showed that HOMA IR reduced in both arms but liraglutide (1.2 mg) was superior to combination therapy. In 2021, Ma et al. 22 showed significant reduction in TG and improvement in HDL.
Different studies noted varying effects of GLP-1 RA and metformin monotherapies on LH, TT, FSH, SHBG levels, and menstrual cyclicity while some studies indicated the superiority of metformin to GLP-1 RA, other trials have found that a combination treatment has a neutral effect. Jensterle et al. 23 compared combination treatment of metformin and 1.2 mg liraglutide versus 1.2 mg liraglutide showed improvement in SHBG and reduction in TT with combination therapy. Elkind-Hirsch et al. 24 showed that liraglutide (3 mg) improved the menstrual cyclicity and reduction in TT. In contrast, a study by Liu et al. 25 showed that exenatide and metformin both enhanced the level of TT with no significant difference; however, exenatide was found to be more effective than metformin in terms of improving menstrual cyclicity, pregnancy rate, and the level of High-sensitive C-reactive protein (HsCRP). Three studies investigated the use of combined treatment with GLP-1 RA and metformin; results showed that a combined treatment had a promising effect on metabolic and endocrine parameters compared with the individual administration of either medication.
The strength of this systematic review is that it is a comprehensive review including all studies that focused on anthropometrics, endocrine, and metabolic parameters as outcomes in patients with PCOS. The primary limitation lies in the selection of studies with short duration of follow-up and the number of participants in the studies. Another limitation is that all studies didn’t include all the anthropometrics, and endocrine and metabolic parameters.
Conclusion
GLP-1 RA and metformin have emerged as a promising intervention for PCOS, with ongoing database surrounding their comparative effectiveness. Several studies highlighted the potential superiority of GLP-1 RAs, particularly liraglutide, over metformin in reducing body weight, BMI, and WCs. These physical improvements indicate a potential impact for GLP-1 RAs in managing the metabolic outcomes of PCOS. Given that insulin resistance stands as the primary driver for metabolic and endocrine dysfunction in PCOS, the therapeutic advantages of GLP-1 agonist therapy in this population appear logical.
Although the primary effect of GLP-1 is not to stimulate insulin secretion, these agonists may indirectly enhance insulin sensitivity through their weight-reducing effects. This dual mechanism of action positions GLP-1 RAs as potentially advantageous in tackling the intricate interplay of factors contributing to PCOS. By not only addressing physical metrics but also potentially influencing insulin sensitivity, GLP-1 RAs present a multifaceted approach to managing the complexities of PCOS. On the contrary, several articles revealed that the combination treatment of GLP-1 RA and metformin has demonstrated promising results enhancing metabolic and endocrine parameters compared with monotherapy. In conclusion, GLP-1 RAs, especially liraglutide, exhibit potential superiority over metformin in addressing physical and metabolic aspects of PCOS. However, further research is needed to determine the optimal treatment approach and ultimately discover the long-term safety of combined therapy in women with PCOS and obesity.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241234530 – Supplemental material for A systematic review of GLP-1 on anthropometrics, metabolic and endocrine parameters in patients with PCOS
Supplemental material, sj-docx-1-whe-10.1177_17455057241234530 for A systematic review of GLP-1 on anthropometrics, metabolic and endocrine parameters in patients with PCOS by Salwa Bader, Rahila Bhatti, Bashair Mussa and Salah Abusanana in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.