
Abstract
Background:
Although participation in paid work improves women’s quality of life and well-being, the health benefits decline for women with young children. Implementing family-friendly work conditions is one strategy for improving working women’s well-being, especially those with competing unpaid work responsibilities.
Objective:
This study investigated the extent to which accessibility and use of 11 specific family-friendly work conditions were associated with physical health, anxiety and depression in Malaysian women with young children.
Design:
A cross-sectional design using a retrospective self-complete, anonymous, online survey was conducted between March and October 2021.
Methods:
Women with a child aged 5 years or less (N = 190) completed an online survey measuring their exposure (availability and use) to 11 specific family-friendly work conditions, and their physical health, anxiety, and depression. The sample included women who were currently and recently working and with both formal and informal employment.
Results:
After accounting for potential confounders, women who used paid maternity leave have a lower likelihood of having anxiety symptoms.
Conclusion:
Future research is needed to extend the findings from this study by over-sampling women who are informally employed and not currently working. Policy creation and development processes, including research and decision-making, should be led by and inclusive of women. For example, research funding could be allocated to ‘lived experience’ research that privileges the co-design of research with consumers. Based on these findings, the extent to which family-friendly work conditions fulfill their intent to improve the well-being for working women requires further critique.
Introduction
Paid work participation and obtaining the associated resources can be enriching for women and improve their quality of life. 1 Paid employed women have better physical and mental health compared to unemployed women.2–4 However, increased paid work participation is associated with a decline in women’s physical and mental health, including increased sleep disturbance, alcohol use, depression, and psychological distress.5–9 Furthermore, the health benefits of paid work diminish when combined with care of young children. 10 The existing research demonstrates inconclusive evidence on the impact of paid work participation on women’s well-being, and negative impacts for women with young children.
Implementing family-friendly work conditions (FFWCs) is touted as one strategy for improving working women’s well-being and can be categorized into two key family policy expansion movements.11–14 The first movement classifies family policy expansion by appearing to give further government incentives for mothers to accept low wages in a service-based economy – promoting neoliberalism, with possible negative impacts on women’s well-being.14,15 The second movement advocates for working parents with young children in a more gender-friendly context, with family policy expansion works to partially liberate mothers from social reproduction-related tasks. 14 According to Ferragina, 14 the first movement dominates the second among 23 OECD (Organisation for Economic Co-operation and Development) countries (e.g. Australia, the United Kingdom, Denmark, and Switzerland). In Malaysia, FFWCs range from the promotion of flexible work hours and telework/work from home, provision of workplace creches, and a statutory requirement for maternity leave.16–18 The positioning of Malaysia in terms of family policy expansion movements described by Ferragina, 14 remains unclear.
There is some evidence for a positive association between flexible work arrangements and women’s perceived quality of life, work–life balance, and enrichment in Malaysia.19–22 Reliable associations between specific flexible work arrangements, such as staggered work hours and work from home as well as the benefits of other FFWCs (leave policies and childcare supports) about women’s physical and mental health in Malaysian women have not been established. Also, little is known on how the availability of FFWCs, or their utilization, may differentially affect women’s physical and mental health. Weale et al. 23 demonstrated inconsistent associations between FFWCs policy availability and their use on work–life balance across specific policy types. Each type of exposure to FFWCs may have its own unique benefits and/or risks for women’s physical and mental health, and the implementation gaps (i.e. whether availability or uptake is the limitation to promoting well-being) may differ across specific FFWCs. Therefore, understanding the potential impact of both the availability and use of specific FFWCs on well-being outcomes for women is critical for understanding the implications and value of FFWC policy initiatives.
The global literature establishing associations between specific FFWCs, and women’s physical and mental health originates in developed countries. This evidence may not be transferable to Malaysia’s cultural and economic contexts and is inconclusive regarding the benefits of FFWCs on women’s physical and mental health. Beneficial impacts of specific FFWCs (e.g. paid maternity and parental leave, provision of publicly funded childcare and reduced hours arrangements (e.g. part-time, job-share and term-time working arrangements)) on women’s mental health, level of stress, re-hospitalization, exercise and stress management and life satisfaction have been shown in Australia, Germany, Japan, the United States, and the United Kingdom.12,13,24–26 However, other specific FFWCs (i.e. additional 120 days of maternity leave, childcare subsidies, and work from home) have been associated with poorer health in the West Germany, the United States, and the United Kingdom, including increased susceptibility to symptoms consistent with anxiety, depression and parenting stress, and higher incidence of long-term sickness absence, job stress, burnout, somatic stress and sleep trouble.27–30 Studies in the United Kingdom and the United States have found that flexible work arrangements (i.e. part-time work, job sharing, flexitime, work from home, compressed work hours and school term-time contract) and paid maternity leave have no associations with self-rated health, long-term illness, life satisfaction or depressive symptoms among mothers.26,31 The global literature reveals inconsistencies in the patterns of influences between specific FFWCs and women’s well-being.
There are methodological limitations in the way knowledge about the impacts of FFWCs on women’s well-being is being established. Although specific FFWCs are likely to have distinct causal effects on women’s physical and mental health, studies have either created and depended on FFWCs indices that aggregate specific conditions as ‘a set’ with non-specific and broad definitions, or examined single specific FFWCs in isolation.19–22 FFWCs are rarely provided as a whole package, and specific FFWCs are likely to provide opportunities of varying value for enhancing women’s physical and mental health.
Systematic exclusion of women who are informally employed and not currently working introduces further bias into existing evidence. FFWCs are a fundamental right for all workers, regardless of gender, ethnicity, age, employment status, disability, or any other characteristics.32,33 Limiting research to formally employed and currently working women does not reflect ‘all women’s’ potential exposure to FFWCs, or their potentially varying influence on well-being. Absence from the formally employed population may have been affected by FFWCs availability and use itself, so that, restricting samples to those in the formal employment creates a sample selection bias towards those who are already potentially less negatively impacted by FFWCs. As a result, the benefits of FFWCs are likely to be over-stated and lead to biased decision-making about FFWC advancement or disinvestment. This trend can perpetuate the diminished visibility of informally employed and unemployed women to policymakers, and their inclusion in understanding associations between specific FFWCs and well-being is critical.
In summary, existing evidence has only established uncertain (in Malaysia) and equivocal (globally) associations between specific FFWCs and well-being among women; is biased by analyzing FFWCs as aggregate FFWCs indices or in isolation, and by excluding informally employed and not currently working women. Thus far, research has failed to differentiate between availability and utilization in exploring the associations between specific FFWCs and well-being, limiting our understanding of whether provision or uptake is the source of any benefits for women. This study aimed to determine the extent to which accessibility and use of specific FFWCs was associated with physical health, anxiety, and depression in an inclusive sample of Malaysian women with young children.
Methods
Study design
A cross-sectional design using a retrospective self-complete, anonymous, online survey was used to quantify women’s exposure to and use of eleven specific FFWCs, and their associations with well-being (physical health, depression, and anxiety). The online survey was available to complete in either English or Malay language (Supplementary Material 1). In preparing the article, we have followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Participants
To be eligible, participants had to be women who were Malaysian citizens residing in Malaysia, aged 15–64 years old, with at least one paid working experience in their life and at least one child aged 5 years or younger in their care at the time of participation.
Participants were recruited through one of three methods using purposive and snowball sampling, with self-selection for participation based on eligibility criteria (which was confirmed in the survey). The first method was distributing invitations consisting of study details (including eligibility criteria) and a link to the online survey through key organizations. These included invitations sent by email on behalf of the researchers to: 400 volunteers (both Malaysian and non-Malaysian, regardless of gender) in Women’s Aid Organization’s database; 800 women on TalentCorp Malaysia’s Career Comeback Programme Database of women seeking to recommence work after a career break and employees of the United Nations Development Fund. Invitations were sent to employees of the United Nations University International Institute for Global Health through a WhatsApp message. The second method of recruitment used online advertising methods to reach wider population samples in a cost-effective way and eliminate bias in geographical restrictions. 34 These included a paid Queensland University of Technology (QUT) Facebook Campaign Ad targeting the Malaysian population run from 15 to 28 April 2021, and a post, including study details and a link to the survey posted on the QUT School of Public Health and Social Work Facebook account. The ad included text, a headline, and a description of the study as well as a link to the survey.
The final method of recruitment was a panel online survey conducted by Malaysian provider Vase.ai, who were contracted to collect completed responses from 110 eligible women in their database for a total of AUD 2450. The English and Malay questionnaires and selected target audience profiles (i.e. 18–64 years, female, all states in Malaysia and Malay, Chinese, Bumi Sabah/Sarawak, Indian/Others race) were provided to the panel. The target audience profile based on age for this recruitment method was slightly inconsistent with the lower limit employed for this study overall, because the panel survey platform (Vase.ai) did not include participants < 18 years of age. The panel expert launched the questionnaire to participants who fit the selected profile in their database. Three quality control processes were conducted for responses. Two automated processes detected ‘straightliners’ (e.g. people who select option A for every question) and ‘speedsters’ (people who answer too quickly (e.g. 25% faster than the panel’s research team)). The third quality control process was manually conducted by panel’s data analyst (i.e. reviewing open-ended responses for acceptable words/sentences and excluding respondents with responses outside acceptable parameters).
Data collection
Data were collected via a self-complete online survey in March–October 2021. All participants were invited to participate in a prize draw for a chance to win one of 40 RM50 vouchers from Mydin Mohamed Holdings Berhad (a wholesale and retail company, with at least one store in every state that offers low-cost household products). Participants who accepted these invitations provided their information (i.e. name, phone number, email or residential address) through an external webpage not linked to their survey data to ensure anonymity and confidentiality.
Online survey
Participants could choose which language (Malay or English) they viewed and responded to survey items. The online survey included an information package with the study background and consent form to complete prior to survey commencement. The survey comprised five sections of questions: (1) screening items to determine eligibility, (2) current or recent (if not currently working) working information, including participation in paid work over the last 5 years (3) the availability and utilization of 11 specific FFWCs over the last 5 years, (4) physical and mental health and (5) questions to describe the sample, determine the representativeness and assess potential confounders of the associations being examined (e.g. age, marital status, educational background, number of children, elderly care and social support). Several items were designed specifically for this research and tested for usability or acceptability and face validity in a small sample of ten women before the items were finalized, given that no existing self-reported measures of FFWCs’ exposure and utilization existed.
After providing consent to participate and confirming eligibility on all screening items, participants proceeded to the subsequent survey items. Participants included in the study were women who confirmed their eligibility as Malaysian citizens residing in Malaysia, aged 15–64 years old, with at least one paid working experience in their life and at least one child aged 5 years and below in their care at the time of participation and who provided sufficient data for analyses (outlined further below and in Figure 1). On completion of the scurvey, women were given a more comprehensive project outline and personalized risk level associated with their scores on the Patient Health Questionnaire 15 (PHQ-15; ⩾1035, generalized anxiety disorder (GAD-7; scores ⩾ 1039 and Edinburgh Postnatal Depression Scale (EPDS; scores > 1241) as well as avenues through which they could seek support.

Participant exclusion and inclusion flowchart.
Measures
Dependent variables
Well-being was assessed separately for physical health, anxiety and depression (see Table 1).
Summary of variables.
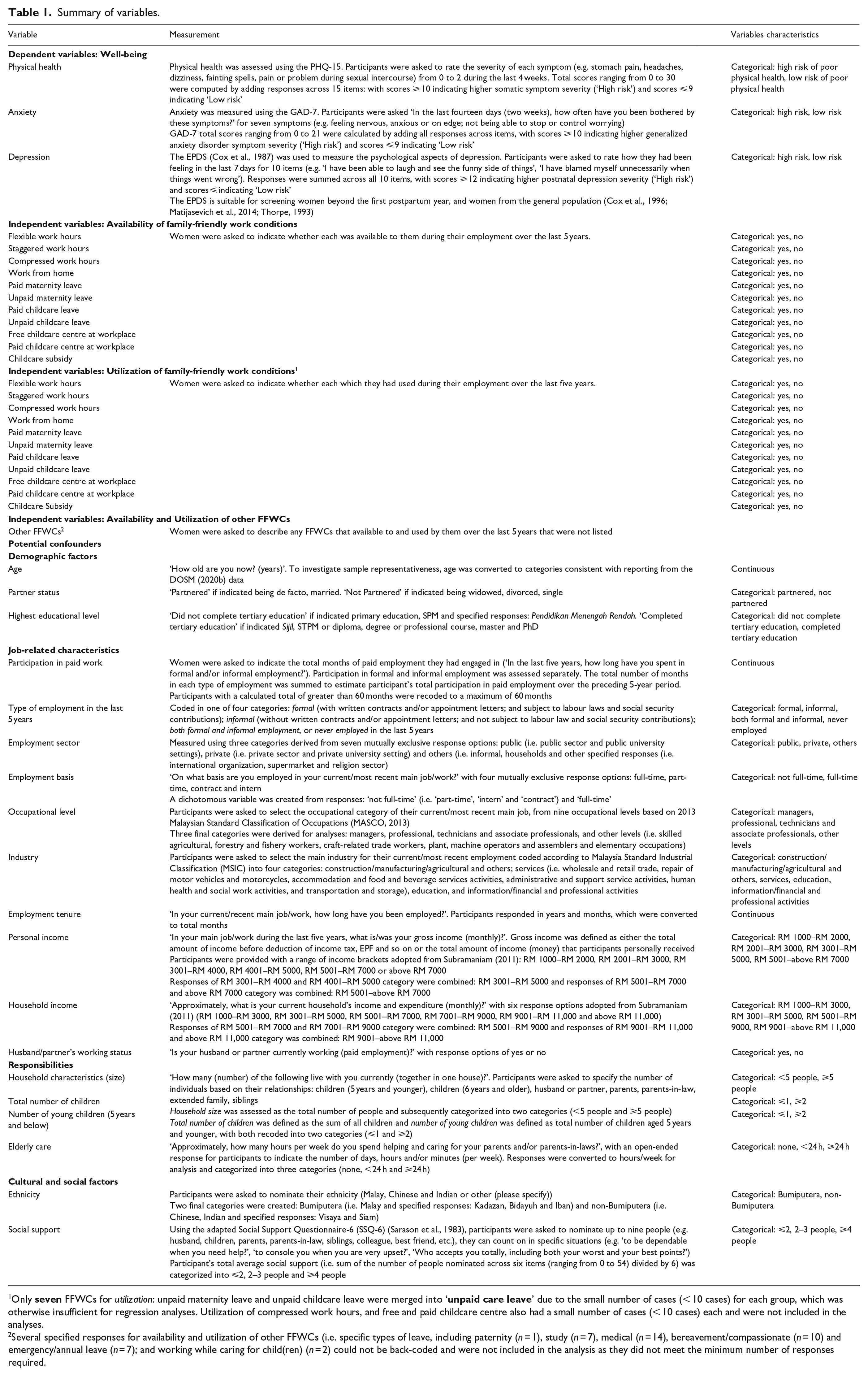
Only
Several specified responses for availability and utilization of other FFWCs (i.e. specific types of leave, including paternity (n = 1), study (n = 7), medical (n = 14), bereavement/compassionate (n = 10) and emergency/annual leave (n = 7); and working while caring for child(ren) (n = 2) could not be back-coded and were not included in the analysis as they did not meet the minimum number of responses required.
Physical health: The PHQ-15 was used to measure physical health. For 13 of the 15 items (e.g. stomach pain, headaches, dizziness, fainting spells, pain or problem during sexual intercourse), participants rated the severity of each symptom from 0 = (not bothered) to 2 = (bothered a lot) during the last 4 weeks. For two additional physical symptoms (‘feeling tired or having low energy’ and ‘trouble sleeping’), participants were asked: ‘In the last 4 weeks, how often have you been bothered by any of the following problems?’ with response options of 0 = (not at all), 1 = (several days) or 2 = (more than half the days or nearly every day). Total scores ranging from 0 to 30 were computed by adding all the responses across 15 items, with scores of ⩾10 and ⩽9 indicating high and low somatic symptom severity, respectively. Participants with scores of ⩾10 were informed about the associated level of risk for physical health following Kroenke et al.’s 35 study. The scale has good internal consistency (Cronbach’s α = .82). 36 Items were translated to the Malay language by academic staff of Universiti Sains Malaysia (English Language section) and a medical doctor checked and compared the Malay and English versions (Cronbach’s α = .94). Participants missing one or more responses to selected items were excluded from scale score calculation. 37
Anxiety: The GAD-7 comprising seven items (i.e. feeling nervous, anxious or on edge; not being able to stop or control worrying; worrying too much about different things; trouble relaxing; being so restless that it is hard to sit still; becoming easily annoyed or irritated; feeling afraid as if something awful might happen) was used to measure anxiety. Participants were asked ‘In the last fourteen days (two weeks), how often have you been bothered by these symptoms?’ on a four-point frequency scale from 0 ‘not at all’ to 3 ‘nearly every day’. 38 GAD-7 scores ranging from 0 to 21 were calculated by adding all responses across items, with scores of ⩾ 10 and ⩽ 9 indicating high and low generalized anxiety disorder symptom severity, respectively. Participants with scores of ⩾ 10 were informed about their associated level of risk for anxiety following Spitzer et al.’s 39 study. The GAD-7 has excellent internal consistency (Cronbach’s α = .92), 39 including the Malay version of GAD-7 version used in this research; 40 Cronbach’s α = .74). Participants missing one or more responses to items were excluded from the scale score calculation. 37
Depression: The EPDS 41 was employed to assess depressive symptoms. Participants rated how they had been feeling in the last 7 days from 0 (e.g. no, not at all) to 3 (e.g. yes, most of the time) for ten items (e.g. ‘I have been able to laugh and see the funny side of things’, ‘I have looked forward with enjoyment to things’, ‘I have blamed myself unnecessarily when things went wrong’, ‘I have felt scared or panicky for no very good reason’). Responses were summed across all ten items, with scores of ⩾12 and ⩽11 indicating high and low postnatal depression symptom severity, respectively. Participants with scores ⩾12 were informed about the associated level of risk for depression following Cox et al. 41 The EPDS scale has a good internal consistency, Cronbach’s α of .87, 41 including the Malay-translated EPDS (Cronbach’s α = .86). 42 The EPDS is suitable for screening women beyond the first postpartum year, and women from the general population.43–45 Respondents missing one or more responses to items were excluded from the scale score calculation. 37
Independent variables and potential confounders
All independent variables and potential confounders are described in Table 1.
Independent Variables: Exposure to 11 specific FFWCs was measured as both their availability and their use in the last 5 years. Drawing on previous literature, potential confounders of the association between exposure to FFWCs and well-being included demographic characteristics, job-related characteristics, unpaid work responsibilities and cultural and social factors.46–63
Statistical analysis
All analyses were performed using Statistical Programme for the Social Sciences (SPSS version 26), with significance set at p < .05. Chi-square goodness-of-fit tests were conducted to compare the sample against employed women population in the Malaysia Labour Force Survey 2021 and estimate representativeness. Logistic regression was used to assess associations between availability (referent group ‘not available)’ and use (referent ‘not used’) of specific FFWCs and well-being (i.e. physical health, anxiety and depression). Where physical health, anxiety or depression were significantly associated with availability and use of specific FFWCs (p < .1), multiple variable logistic regression modelling was used to determine whether any of the identified confounders affected the association. Potential confounders of the association between FFWCs exposure and well-being were included if they were significantly associated with the well-being indicator (p < .05) using binary logistic regression.
Results
Study sample
A total of 257 eligible responses were received (Figure 1). Of these, 27 women were excluded from the analyses of associations between FFWCs (availability and use) and well-being due to not having undertaken any paid work in the last 5 years and therefore missing data for exposure to FFWCs. A further 40 women were excluded due to missing data on one or more items assessing well-being, and 37 were excluded because they were missing data on potential confounders that had < 5% of cases with missing data (i.e. industry, employment tenure, age, partnered status, ethnicity, highest educational level, personal income, young children, total children, household size and household income), resulting in a sample of 153 women (59.5%) for analysis. Inclusion at each stage of the analyses is detailed in Figure 1. The final sample of 153 participants exceeded Green’s 64 recommendation for the minimum acceptable sample size (N ⩾ 104 + m (where m is the number of predictor variables) when investigating individual predictors. For this study, we accounted for 32 predictor variables (including potential confounder variables), calculating N ⩾ 136 as the minimum sample necessary to detect a moderate effect for multiple regression.
Participants were aged between 19 and 59 years (M = 32.93, SD = 7.02). Compared with the population of employed women in Malaysia 65 (see Table 2), the included sample over-represented women who were Bumiputera, managers or professionals/technicians and associate professionals, had completed tertiary education, and who worked in education or information/financial/professional activities industries. About a third (25.8%) earned RM3000–RM 5001 per month, 54.7% lived with ⩾2 children and 41.6% cared for elderly ⩾24 h per week (Table 2). Compared with those who were included in the analyses, participants who were excluded were less likely to experience depression (14.4%), followed by poor physical health (12.5%) and anxiety (7.7%).
Comparison of the included sample with the population of employed women in Malaysia.

p value < .001 **p value < .05. aLabour Force Survey, Malaysia 2021.
Preliminary analyses
Two potential confounders (age and employment tenure) contained several outliers. Since outliers were all within the range of valid values, they were retained and used as real data, with the exception of one outlier for age, 40 which was recoded to 40. The one outlier was recoded because Cook’s distance for multivariable logistic regression to predict anxiety exceeded one.
Identifying potential confounders
Variables were considered a potential confounders if there was a significant association (p < .05) with the dependent variable.
Physical health was not significantly associated with age, partner status, highest educational level, participation in paid work in the last 5 years, type of employment in the last 5 years, employment basis, employment sector, industry, employment basis, employment tenure, number of young children and total children who live together, household size, husband/partner’s employment status and social support nor ethnicity (see Table 3). There were statistically significant associations between physical health and some job-related characteristics, including occupational level (professionals, technicians and associate professionals: odds ratio (OR) = .49, p = .036, 95% confidence interval (CI) = .25, .95), employment sector (public sector: OR = .28, p = .046, 95% CI = .08, .98) and personal income (RM 5001–above RM 7000: OR = .35 p = .022, 95% CI = .14, .86). Among caregiving responsibilities, elderly care (< 24 h: OR = 2.58, p = .026, 95% CI = 1.12, 5.95) and household income (RM 9001-above RM 11,000: OR = .38, p = .037, 95% CI = .16, .94) were significantly associated with physical health. Both anxiety (OR = 11.41, p = .000, 95% CI = 3.73, 34.92) and depression (OR = 4.60, p = .000, 95% CI = 2.45, 8.64) were associated with physical health. Therefore, models for assessing the association between the availability and use of FFWCs and physical health included adjustment for occupational level, employment sector, personal income, elderly care, household income, anxiety, and depression.
Associations between potential confounder variables and physical health, anxiety and depression.

**p < .05, ***p < .001.
Reference groups: a–b ⩽ 1 child; c< 5 people; dnot working, enon-Bumiputera.
Anxiety
Anxiety was not significantly associated with the highest educational level, participation in paid work in the last 5 years, type of employment in the last 5 years, employment sector, employment basis, employment tenure, occupational level, industry, personal income, number of young children and total children, household size and income, husband/partner’s employment status, elderly care, social support nor ethnicity (see Table 3). Among demographic factors, anxiety was significantly negatively associated with age (OR = .90, p = .014, 95% CI = .83, .98) and partner status (OR = .09, p = .000, 95% CI = .03, .25). Physical health (OR = 11.41, p = .000, 95% CI = 3.73, 34.92) and depression (OR = 56.82, p = .000, 95% CI = 7.48, 431.78) were positively significantly associated with anxiety. Therefore, models for assessing the association between the availability and use of FFWCs and anxiety included adjustment for age, partner status, physical health, and depression.
Depression was not significantly associated with the highest educational level, participation in paid work in the last 5 years, type of employment in the last 5 years, employment sector, employment basis, employment tenure, occupational level, industry, number of young children, and total children who live together, household size and income, husband/partner’s employment status, elderly care, ethnicity nor social support (see Table 3). There was a significant association between depression and demographic factors, including age (OR = .96, p = .050, 95% CI = .91, 1.00) and partner status (OR = .32, p = .023, 95% CI = .12, .85). There was only one significant association between depression and job-related characteristics: personal income (RM 5001–above RM 7000: OR = .39, p = .038, 95% CI = .16, .95). Physical health (OR = 4.60, p = .000, 95% CI = 2.45, 8.64) and anxiety (OR = 56.82, p = .000, 95% CI = 7.48, 431.78) were positively significantly associated with depression. Therefore, models for assessing the association between the availability and use of FFWCs and depression included adjustment for age, partner status, personal income, physical health, and anxiety.
Associations between exposure to FFWCs and well-being
Availability of specific FFWCs
The most available FFWC reported by women was paid maternity leave (86.3%), followed by staggered work hours (63.7%) and flexible work hours (39.5%). The least available FFWC was compressed work hours (6.3%), followed by free childcare centre (6.8%) and childcare subsidy (10.0%) (see Table 4).
Associations between availability of specific family-friendly work conditions, physical health, anxiety and depression (n = 190).
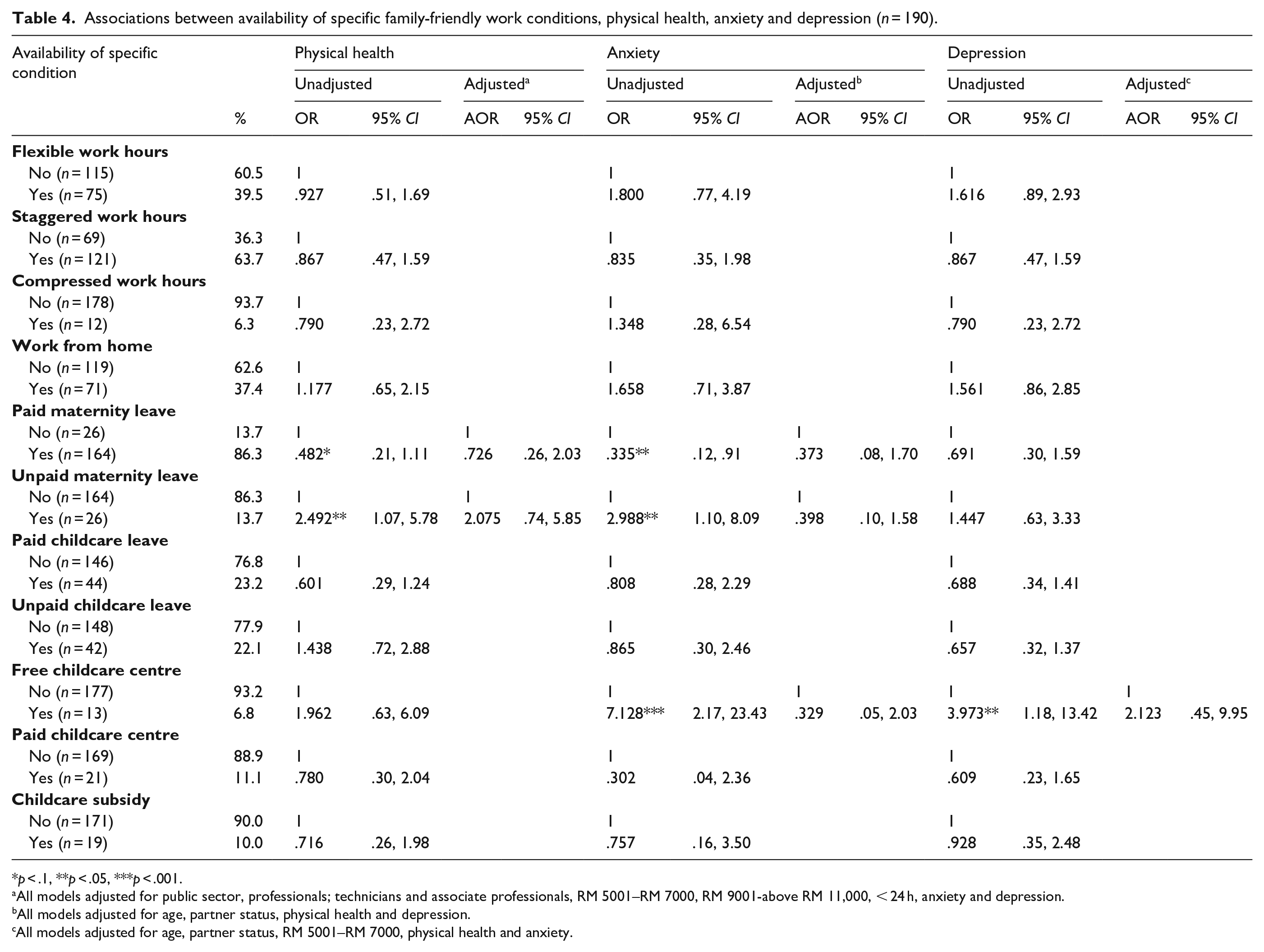
p < .1, **p < .05, ***p < .001.
All models adjusted for public sector, professionals; technicians and associate professionals, RM 5001–RM 7000, RM 9001-above RM 11,000, < 24 h, anxiety and depression.
All models adjusted for age, partner status, physical health and depression.
All models adjusted for age, partner status, RM 5001–RM 7000, physical health and anxiety.
Physical health
There were significant associations between availability of both paid and unpaid maternity leave, and participants’ physical health (see Table 4). These associations were no longer significant after adjustment for potential confounders. Among the included potential confounders, women who worked in the public sector had lower odds of poor physical health (paid maternity leave: adjusted odds ratio (AOR) = .44, 95% CI = .19, 1.03, unpaid maternity leave: AOR = .43, 95% CI = .18, 1.00). In contrast, women who cared for elderly (paid maternity leave: AOR = 2.04, 95% CI = .96, 4.37, unpaid maternity leave: AOR = 2.03, 95% CI = .94, 4.36), and had anxiety (paid maternity leave: AOR = 5.53, 95% CI = 1.37, 22.33, unpaid maternity leave: AOR = 5.17, 95% CI = 1.28, 20.82) and depression (paid maternity leave: AOR = 3.38, 95% CI = 1. 57, 7.26, unpaid maternity leave: AOR = 3.42, 95% CI = 1.58, 7.40), had higher odds of poor physical health. The adjusted model accounted for approximately 31.6% (paid maternity leave) and 32.5% (unpaid maternity leave) of the variance in physical health.
Anxiety
Availability of paid maternity leave, unpaid maternity leave and free childcare centre were significantly associated with anxiety (see Table 4). After adjusting for potential confounders, there was no longer significant association between availability of paid maternity leave, unpaid maternity leave and free childcare leave with anxiety. Women who were partnered had lower odds of experiencing anxiety in the adjusted models (paid maternity leave: AOR = .10 95%CI = .02, .56, unpaid maternity leave: AOR = .09, 95% CI = .02, .49, free childcare centre: AOR = .10, 95% CI = .02, .53). Higher odds of experiencing anxiety were observed for women who had poor physical health (paid maternity leave: AOR = 6.30, 95% CI = 1.60, 24.81, unpaid maternity leave: AOR = 6.03, 95% CI = 1.50, 24.29, free childcare centre: AOR = 6.57, 95% CI = 1.63, 26.50) and depression
Depression
Availability of free childcare centre was significantly associated with depression (see Table 4). After adjusting for potential confounders, these associations were no longer significant (see Table 4). Women who had poor physical health were more likely than those who did not have poor physical health to experience depression (AOR = 2.96, 95% CI = 1.45, 6.05) and anxiety (AOR = 30.91, 95% CI = 3.66, 261.28). The adjusted model accounted for approximately 34.5% of the variance in depression.
Use of specific FFWCs
The most used FFWCs reported were paid maternity leave (58.9%), followed by staggered work hours (33.7%), as well as work from home and flexible work hours (31.1% for each category). Least-used FFWCs were unpaid childcare leave (5.3%), childcare subsidy (5.8%), and paid childcare leave (11.6%) (see Table 5).
Associations between utilization of specific family-friendly work conditions, physical health, anxiety and depression (n = 190).
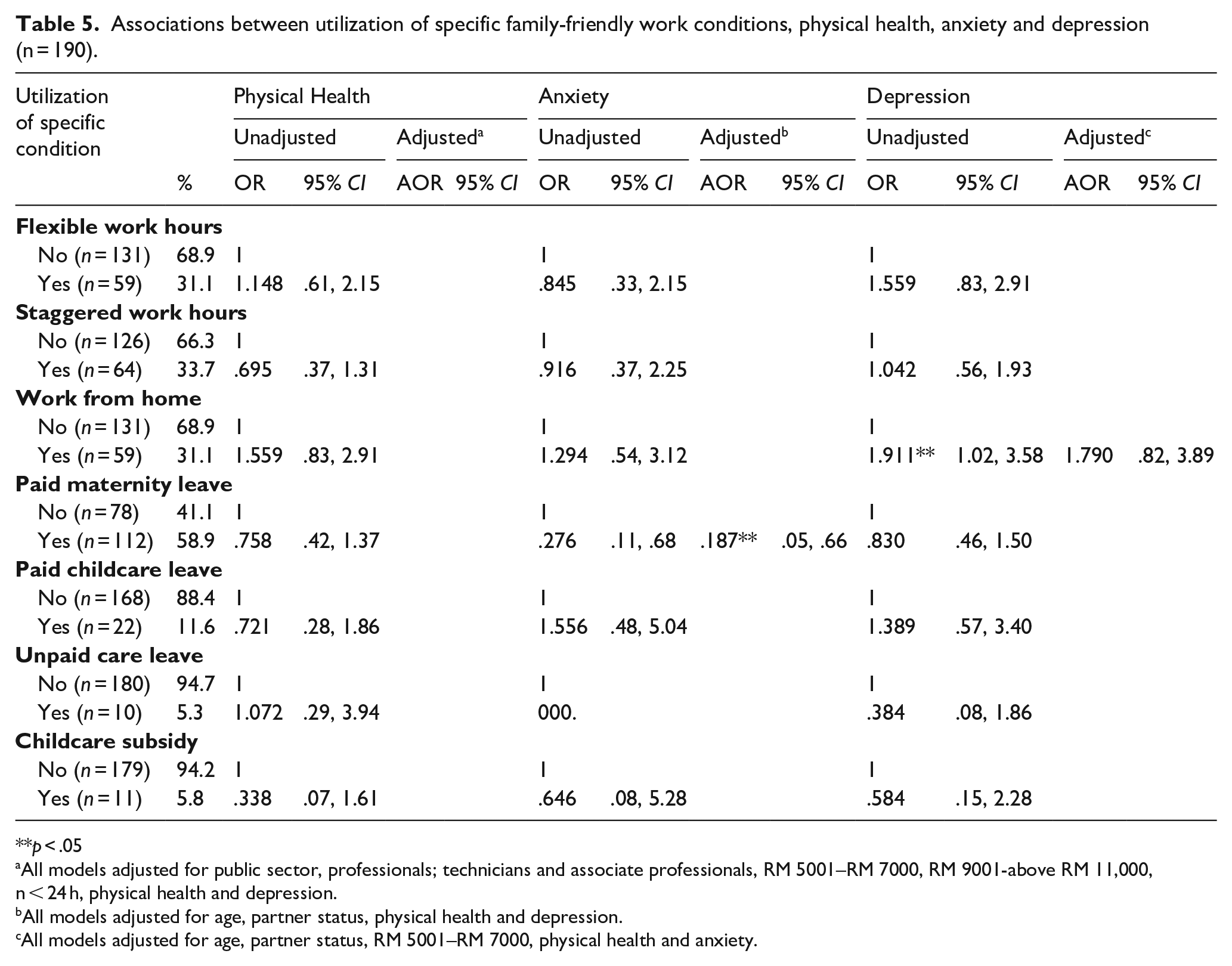
p < .05
All models adjusted for public sector, professionals; technicians and associate professionals, RM 5001–RM 7000, RM 9001-above RM 11,000, n < 24 h, physical health and depression.
All models adjusted for age, partner status, physical health and depression.
All models adjusted for age, partner status, RM 5001–RM 7000, physical health and anxiety.
Physical health
There were no associations between utilization of any specific FFWCs and physical health.
Anxiety
Only use of paid maternity leave was significantly associated with anxiety. After adjusting for confounders (see Table 4), use of paid maternity leave was associated with significantly lower odds of anxiety (AOR = .187, 95% CI = .05, .66). The adjusted model accounted for approximately 60% of the variance in anxiety. Women who were partnered had lower odds of experiencing anxiety in the adjusted models (AOR = .08 95% CI = .01, .52). Higher odds of experiencing anxiety were observed for women who had poor physical health (AOR = 6.75, 95% CI = 1.66, 27.54) and depression (AOR = 40.28, 95% CI = 4.50, 360.70).
Depression
Use of work from home was significantly associated with higher odds of depression. After adjusting for confounders, this association was no longer significant (see Table 5). Women were more likely to experience depression if they had poor physical health (AOR = 2.76, 95% CI = 1.33, 5.73) and anxiety (AOR = 31.88, 95% CI = 3.75, 270.75). The adjusted model accounted for approximately 35.2% of the variance in depression.
Discussion
This study sought to examine how women’s access and use of FFWCs was associated with several measures of well-being, including physical health, anxiety and depression. Availability and use of all FFWCs neither enhanced nor worsened physical health and depression in women, consistent with earlier research.26,31 Of 11 FFWCs, only utilization of paid maternity leave was associated with anxiety. These unanticipated findings, while preliminary, suggests that using paid maternity leave may reduce the likelihood of experiencing anxiety. Our findings add to the literature on the possible outcomes of paid maternity leave for women’s well-being. 26 Women who used paid maternity leave had lower likelihood of anxiety compared to women who did not use paid maternity leave. Some women (13.7% women) reported not having had access to paid maternity leave despite it being a statutory work condition), 18 which aligned with findings from other research in Malaysia. 66 More research is needed to further investigate disparities in access to paid maternity leave.
Our findings also revealed other factors (potential confounders: demographic factors, job-related characteristics, unpaid work responsibilities, and cultural and social factors) that influenced ’women’s well-being. These potential confounders had varying effects on ’women’s well-being. Women who worked in the public sector had lower odds of poor physical health. Existing study discovered that Saudi women who work in the public sector were more likely to be overweight/obese. 67 Our result indicates that the influence of women’s employment sector on their well-being varied according to the measured well-being indicator. Our finding that women who cared for the elderly had higher odds of poor physical health was consistent with other studies.68,69 In addition, women who were partnered had lower likelihood of having anxiety, consistent with Fadzil et al.’s 70 Our findings contribute to the international and national literature on the impact of the employment sector, elderly care, and partner status on women’s well-well-being.67–70 Our fully adjusted models found that depression, anxiety, and physical health were all significantly related. Women who experienced anxiety, for example, were more likely to have poor physical health and anxiety, and women who experienced depression were more likely to have anxiety and poor physical health. These findings emphasize the importance of developing and implementing new ‘FFWCs’ that protect women’s overall physical and mental health, and that improving one outcome, such as anxiety, may improve other outcomes (depression and physical health).
The overall value of FFWCs for women’s well-being, or at least for general physical health, anxiety, and depression, was generally unsupported. This may reflect the implementation of FFWCs in Malaysia as an attempt to modernize policy to encourage women’s paid work participation. 71 Paid maternity leave, staggered work hours and flexible work hours were the most commonly available work conditions for women. Paid maternity leave was used most by women, followed by staggered work hours, work from home and flexible work hours. Women had less access to and use of childcare centres (both paid and free), possibly due to the Malaysian systems that maintain traditional values and family constructions, where families are held accountable for their member’s welfare.72,73 Considering Ferragina’s 14 analyses of two key family policy expansion movements, these findings may suggest Malaysia’s positioning within the first movement characterized by family policy expansion as another tool to promote neoliberalism rather than the second movement to support working parents with young children in a more gender-friendly context. 14 Future research is needed for more in-depth assessment of the genuine underlying intention of implementing FFWCs, and stigma, attitudes and regulations associated with FFWCs in Malaysia to ensure that FFWCs are beneficial for women and do not reinforce traditional roles and neoliberalist ideals.
Strengths, limitation and future research directions
This paper measured women’s well-being, where other researchers in Malaysia have consistently measured women’s perceived quality of life, work–life balance and enrichment.19–22 We analyzed self-reported data from a sample of Malaysian women with young children, who over-represented the population of working women in Malaysia in terms of living strata, ethnicity, educational background, occupational level, personal income, and responsibilities (children and elderly care). Women with higher social advantages (e.g. completed tertiary education, lived in urban areas, who were Bumiputera, and managers or professionals/technicians and associate professionals and have children) have better well-being compared to women who are less advantaged,33,56,74–76 whereas, women with lower income and elder care have worse well-being.47,77 Notably, although our study intentionally included women who were not currently working (n = 36), we were only able to compare our sample to the population of working women to assess generalizability. Nevertheless, our findings may be more transferable to higher socially advantaged groups of women within Malaysia. Our study is unable to offer firm conclusions about FFWCs exposure (both availability and utilization) and the impacts of FFWCs on women from under-represented groups, who are likely to be those with fewer resources to begin with. Ferragina 14 concludes that FFWCs expansion does not automatically result in enhancing or diminishing outcomes for an entire population or specifically the lower class, highlighting the complexities of implementing policy within multicultural and varied social class contexts where equity is of concern. Future research detailing these complexities with larger and representative population samples and over-sampling of women from specific subgroups is needed to ensure broader generalizability and confirm or refute the preliminary findings reported here. In addition, our study did not assess sociodemographic factors (e.g. age, marital status, level of education, number of children, elderly care, and social support) as potential mediator and/or moderator variables in the relationship between availability and utilization of FFWCs and women’s physical health, anxiety and depression. Existing research78–80 found sociodemographic factors, such as social support mediated the relationship between COVID-19 stressful experience and acute stress disorder, that household income mediated marital status effects on depressive symptoms and that educational level could mediate the Mediterranean diet’s protective effect. Future research is recommended to examine sociodemographic factors as mediating or moderating variables to better understand the mechanisms between availability and utilization of FFWCs and women’s well-being.
Our study included women in informal employment in the sample, as well as a measure of informal employment participation, in assessing the impact of work conditions on women’s well-being. This is the first study that has attempted to examine the impacts of specific FFWCs on the well-being among informally employed and currently not working women and acknowledge the existence of these women in paid work participation. There were 548.9 thousand informally employed in the population in 2019, who have rights to FFWCs. Of the 38 women who were informally employed in our sample, 20 were also formally employed. While the inclusion of not currently employed and informally employed women in the sample represents a more inclusive way forward for research in this area, women in these sub-populations should be over-sampled or purposively sampled in future research so that the differential exposure to FFWCs and its impact can be better understood in these groups.
Conclusion
The overall value of FFWCs for women’s well-being, particularly physical health, anxiety, and depression is generally unsupported. Paid maternity leave (used by 58.9% of the sample) was the only FFWCs for which use was associated with any well-being outcomes, particularly anxiety. Findings from this study point out the need for greater attention in analyzing the availability and utilization of FFWCs in-depth. Without assessing the real intention of provision of FFWCs, stigmas, attitudes, and regulations associated with FFWCs, these work conditions appear non-beneficial to women’s well-being in Malaysia. One practical implication of this study arises from the demonstrated need for policy creation and development processes, including research and decision-making, to be led by and inclusive of women. For example, research funding could be allocated to ‘lived experience’ research that privileges the co-design of research and policy creation with consumers. In addition, women should be empowered to make choices and exercise their agency about how they prefer to participate in and complete their work that enhances their well-being. Finally, providing employer-based mental health support to the women, such as free monthly sessions with a counselor or psychologist, is recommended.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241233113 – Supplemental material for Family-friendly work conditions and well-being among Malaysian women
Supplemental material, sj-docx-1-whe-10.1177_17455057241233113 for Family-friendly work conditions and well-being among Malaysian women by Nadirah Mat Pozian, Yvette D Miller and Jenni Mays in Women's Health
Footnotes
Acknowledgements
The authors would like to express their gratitude to all participants who participated in this study and to the TalentCorp Malaysia, United Nations Development Fund, Women’s Aid Organization and the United Nations University International Institute for Global Health for their support and help in recruitment.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.