
Abstract
Background:
The World Health Organization recommends companionship as a critical element of respectful maternity care. However, there is paucity of literature regarding women’s attitudes, related factors, and barriers of implementation in Saudi Arabia.
Objective:
This study aimed to assess women’s attitudes toward birth companionship during labor and delivery, related factors, and barriers of implementing labor companionship in Saudi Arabia.
Design/Methods:
This study was carried out in Al Ahsa, Saudi Arabia, using a cross-sectional design. The data collection took place over a period of approximately 6 months, specifically from 16 August 2021 to 20 February 2022. A total of 418 women who had given birth at three governmental hospitals and three private hospitals in Al Ahsa participated in the survey. The study included women between the ages of 18 and 49 years who had delivered during the study period.
Results:
The study revealed that while around 82.8% of mothers expressed a desire for companionship during labor, only 43.2% actually had a labor companion present during delivery. The primary obstacle to labor companionship reported by 21.5% of respondents was hospital policies. Other barriers identified included husbands’ fear of being present during labor (4.7%) and limited availability of time for companionship (3.8%).
Conclusion:
The study concludes that birth companionship is highly desired by women in the study area. However, various physical, emotional, and institutional barriers, such as hospital policies and regulations, impede its implementation. Addressing these barriers and promoting supportive policies are essential to facilitate the provision of birth companionship and improve the childbirth experience for women in Al Ahsa.
Introduction
Birth companionship is recommended by the World Health Organization (WHO) for a positive childbirth experience. It is also emphasized that women are prepared early for support during the prenatal period. 1 While the number of women giving birth in hospitals has increased globally between 2003 and 2013, 2 challenges remain in terms of retaining, ensuring equity, preserving dignity, and delivering quality care for mothers. 3
According to the WHO, neonatal mortality in Saudi Arabia dropped from 22 per 1000 live births in 1990 to 7 in 2016. A national survey involving 10,931 ever-married women in Saudi Arabia revealed a reduction in the infant mortality rate from 29 to 20 deaths per 1000 live births between 1994 and 2004. 4 In 2023, the maternal mortality rate saw an 11.11% decline from 2019, standing 16 per 100,000. 5
In Saudi Arabia, most governmental hospitals lack clear policies permitting the presence of a supportive companion during childbirth, and due to staff shortages, one-to-one nursing care is rarely provided. This results in laboring women being left alone for intermittent periods, especially in the first stage of labor. 6
By providing emotional and social support, birth companions can help women navigate the physical and emotional challenges of labor and delivery, reduce the need for medical interventions, and enhance the overall childbirth experience for mothers and their families. 7 Supportive care from a woman’s social network is crucial in this context. 8
As part of the continuum of respectful maternity care, the WHO suggests that women be offered the option to have a companion who can offer emotional and social support throughout labor and delivery, thereby enhancing birth outcomes. 9 Several studies have demonstrated the positive impact of ongoing support on the health outcomes of both mothers and babies.10,11 Continuous support can be particularly valuable in circumstances where women may not have the decision to have a companion during the birthing process. 12
A birth companion can support the mother emotionally and physically resulting in fewer medical interventions and improved birth outcomes.10 –12 It is crucial to respect women’s desires and aspirations for birth companions throughout the delivery process while also acknowledging the benefits of continuous support in all birth settings to improve the experience of labor for both mothers and newborns.10,13
According to the WHO (2018), birth companions are essential in supporting women during labor and delivery. 14 They offer emotional, social, and practical assistance, alleviating the workload of healthcare providers, particularly in understaffed facilities, and contributing to positive birth outcomes. 15 Research indicates that constant support during labor, whether from a birth companion or a healthcare professional, enhances women’s overall birthing experience and improves the likelihood of positive outcomes for both mothers and newborns. However, in instances where healthcare professionals are absent or unavailable, some women have expressed feelings of helplessness during labor and delivery. 16
Ongoing support throughout labor and delivery can be provided by trained birth companions, such as doulas or individuals chosen from the woman’s social network. 10 It is recommended to incorporate this practice into maternal health guidelines to improve maternal healthcare and promote positive delivery experiences globally, especially in nations with low and moderate incomes, such as those in sub-Saharan Africa.10,17 Healthcare professionals should prioritize supporting women’s desires for birth companionship and ensuring its availability during childbirth. 13
Childbirth is a significant existential life event and women value a positive birth experience. The WHO recognizes a “positive childbirth experience” as a crucial goal for all laboring women.14,18,19 Previous studies have identified several factors associated with a positive birth experience, including women’s prenatal expectations,20,21 having a normal vaginal birth,22,23 and using non-pharmacological pain-relief methods. 24 Other important factors include the ability to communicate birth preferences in advance 25 and receive support from the midwife. 10
The WHO (2020) has emphasized the significance of healthcare services in reducing maternal, neonatal, and child mortality rates.26,27 Moreover, women who are continuously supported during labor are more likely to experience a spontaneous vaginal birth, have shorter labor, give birth to a baby with a high 5-min Apgar score, and are less likely to report negative ratings about their childbirth experience. 10
Conducting research on women’s attitudes and beliefs regarding birth companionship can provide valuable insights into delivering high-quality maternal healthcare services. This study intends to raise the standards of maternal healthcare services and lower mother and infant death rates in Saudi Arabia by examining the use of companionship during childbirth and finding associated features. The findings of the current study can be applied to create policies and initiatives that are sensitive to the needs and preferences of women, leading to improved patient-centered care during childbirth. This initiative to improve maternal healthcare services aligns with the global health agenda of achieving universal health coverage and promoting sustainable development. 28
Methods
Study design
This cross-sectional study was conducted in Al Ahsa city between 16 August 2021 and 20 February 2022. The city has 10 governmental hospitals and 10 private hospitals with delivery rooms and maternal care units. For this study, three governmental hospitals (Maternal and Child Health Hospital, King Faisal General Hospital, and Al-Omran Hospital) and three private hospitals (Al Mousa Hospital, Al-Obaid Hospital, and Al-Maneea Hospital) were selected.
MCH Hospital is a government public hospital specializing in healthcare and therapeutic services for Maternity and Children. The Maternity and Children Hospital—Al Ahsa, with a 450-bed capacity, is a specialized healthcare facility within the governorate. It offers round-the-clock, high-quality integrated health services in the fields of obstetrics, gynecology, and pediatrics. This hospital has successfully conducted numerous complex and rare operations.
Women who had given birth during the specified study period and were between 18 and 50 years old were included. Women with serious health issues, language barriers, and cognitive impairments were excluded.
Sample size
The study employed a multistage sampling process to select health facilities. The hospitals in Al Ahsa were divided into two strata: governmental and private, and further divided into the districts of Al Hofuf, Al Mubarraz, and villages. One exception was made for the city’s largest hospital, MCH, which served as the referral hospital and was included in the study without applying the sampling technique. From each sector, three hospitals were randomly selected. The allocation of samples to health facilities considered the number of women who had given birth at each facility in the 2 months preceding the data collection period.
The study population comprised all mothers who delivered a baby at the selected health facilities in Al Ahsa during the designated study period.
A single population proportion calculation was used to calculate the sample size, considering a 95% confidence level, a 0.05 margin of error. An additional 10% non-response rate was accounted for, resulting in a total sample size of 418 individuals.
The sample was proportionally distributed among health facilities considering the number of women who gave birth at each hospital. The sample size was divided equally between governmental hospitals (209) and private hospitals (209) due to similar admission volumes.
The sampling process used a systematic random sampling technique. The researchers first selected the hospitals, then calculated the interval between participants based on monthly number of women who gave birth in those health facilities and the previously calculated sample size. The first participant was selected through a lottery system, and subsequently, every fifth participant from governmental and every third woman from private hospitals were included in the study, using a sampling interval of five and three which was determined by dividing the entire population size by the desired sample size.
Data collection
Survey was distributed to all participants to gather information about their preferences, contributing factors, and barriers in relation to labor companionship.
Questionnaire development
A structured questionnaire was developed for data collection. The survey was created by adapting information from various sources of literature and research studies.1,17 It was designed to gather relevant data related to labor companionship and factors associated with it.
Pilot study
The questionnaire underwent validation through a pilot study involving 22 participants who were selected from Al Ahsa public health facilities. The purpose of the pilot study was to assess the suitability and clarity of the questionnaire. Pre-tests were also conducted to ensure that the language used in the questionnaire was understandable and appropriate for the study population.
Reliability
The Cronbach’s alpha coefficient (Cronbach’s alpha) was used in this study to measure the instrument’s reliability (0.80).
Study instruments
The questionnaire consisted of two sections.
Background data
The first section collected background information about the participants, including their age, marital status, parity (number of previous births), education level, literacy, employment status, household wealth, type of hospital they attended, attendance at antenatal visits, pregnancy and labor complications, and their perception of crowding in the delivery rooms.
Birth companionship
The second section focused on gathering information related to the availability and type of birth companionship. This section included questions about whether continuous support during labor and delivery was allowed, the participants’ desire for companionship during labor, delivery, and postpartum, and their preferred type of support person. The questionnaire assessed the type and availability of the companion, their relationship to the woman, and the participants’ desire for continuous support during labor, delivery, and after delivery. Overall, the questionnaire was designed to capture relevant data regarding labor companionship and factors associated with it, providing insights into the participants’ preferences and experiences.
Ethical considerations
The study was approved from the ethical research board at King Fahd Hospital “IRB KFHH” number 22-Ep-2021 on 15 August 2021. Informed consent and written permission from the women were obtained after explaining the aim and objectives of the study. It was ensured that respondents’ confidentiality and anonymity were maintained. In addition, data were securely stored and only accessible to authorized statisticians, further ensuring data security and privacy.
Statistical analysis
The study data were analyzed using IBM SPSS software. Frequencies and percentages (n (%)) were used for categorical variables, while mean and standard deviation were used for quantitative variables. The chi-square test was used to determine the association between different variables, and statistical significance was established at a p-value of less than 0.05.
Results
The demographic characteristics of the respondents are shown in Table 1. The study included a total of 418 participants. It was found that nearly half of the participants, 174 (41.6%), belonged to the 29–39 years of age group. Most of the participants, 391 (93.1%), were married. Around 34.9% (146 participants) reported having delivered more than three babies. Among the participants, 261 (62.4%) had a higher education. The number of unemployed participants was 261 (62.4%). Government hospitals were the setting for labor in 209 (50%) cases. A total of 70 (16.7%) participants experienced pregnancy complications during their last pregnancy. Furthermore, 93 respondents (22.2%) faced complications during their delivery. Notably, in 234 (56%) of the cases, healthcare providers did not explain companionship as a right to the patients.
The demographic characteristics of the study participants.

SD: standard deviation.
Regarding companionship as shown in Table 2, the majority of respondents, 351 (84%), reported having a companion from home to the healthcare facility. Out of these cases, 266 (63.6%) were accompanied by their husbands. For 212 respondents (50.7%), their companions remained with them during the first stage of labor. During the second stage of labor until the end of delivery, 170 respondents (40.7%) had someone by their side. In the third stage of labor, 160 respondents (38.3%) had companions with them. Furthermore, 352 respondents (84.2%) expressed their desire to have a companion during the first stage of labor, and 335 (80.1%) indicated a preference for a companion during the second stage of labor.
Companionship and preferences.

Figure 1 illustrates the rates of companionship among participants during labor and delivery. On average, 43.2% of participants reported having a labor companion. Specifically, companionship was achieved during the first stage of labor in 50.7% of cases, during the second stage in 40.7% of cases, and during the third stage in only 38.3% of cases.
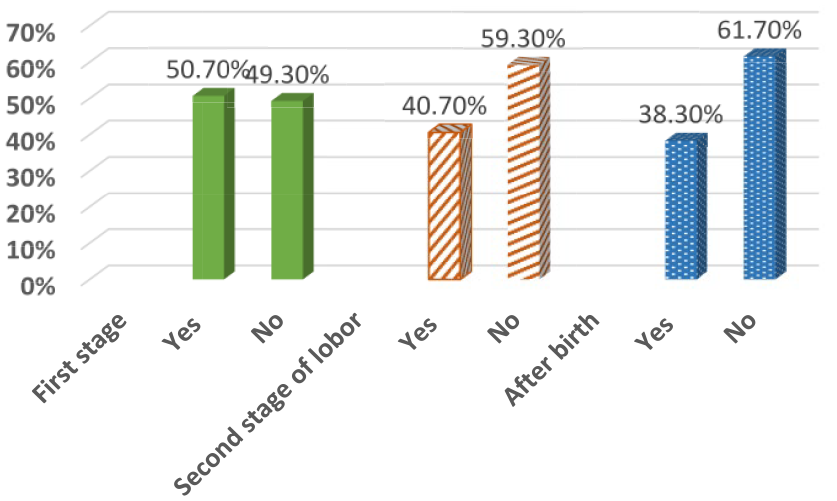
The prevalence of labor companionship stayed among participants.
Figure 2 depicts the prevalence of women’s desire for companionship during labor. According to the participants, approximately 82.8% of mothers expressed a desire for companionship. Specifically, during the first stage of labor, 84.2% of participants wanted a companion. In the second stage, 80.1% expressed a desire for companionship. During the third stage, nearly 84% of participants desired a companion.

The prevalence of desire for labor companionship among women in Saudi Arabia.
Table 3 presents the significance of companionship during labor and its associated barriers. The table reveals that 84% of participants found it helpful to have a partner during childbirth and labor. Among the women surveyed, 34.2% reported that companionship during labor provided them with social, moral, and psychological support. In addition, 32.3% perceived companionship as a means of alleviating pain during labor. For 14.8% of respondents, companionship during labor fulfilled their physical needs.
Importance of companionship during labor and childbirth: reasons and barriers.
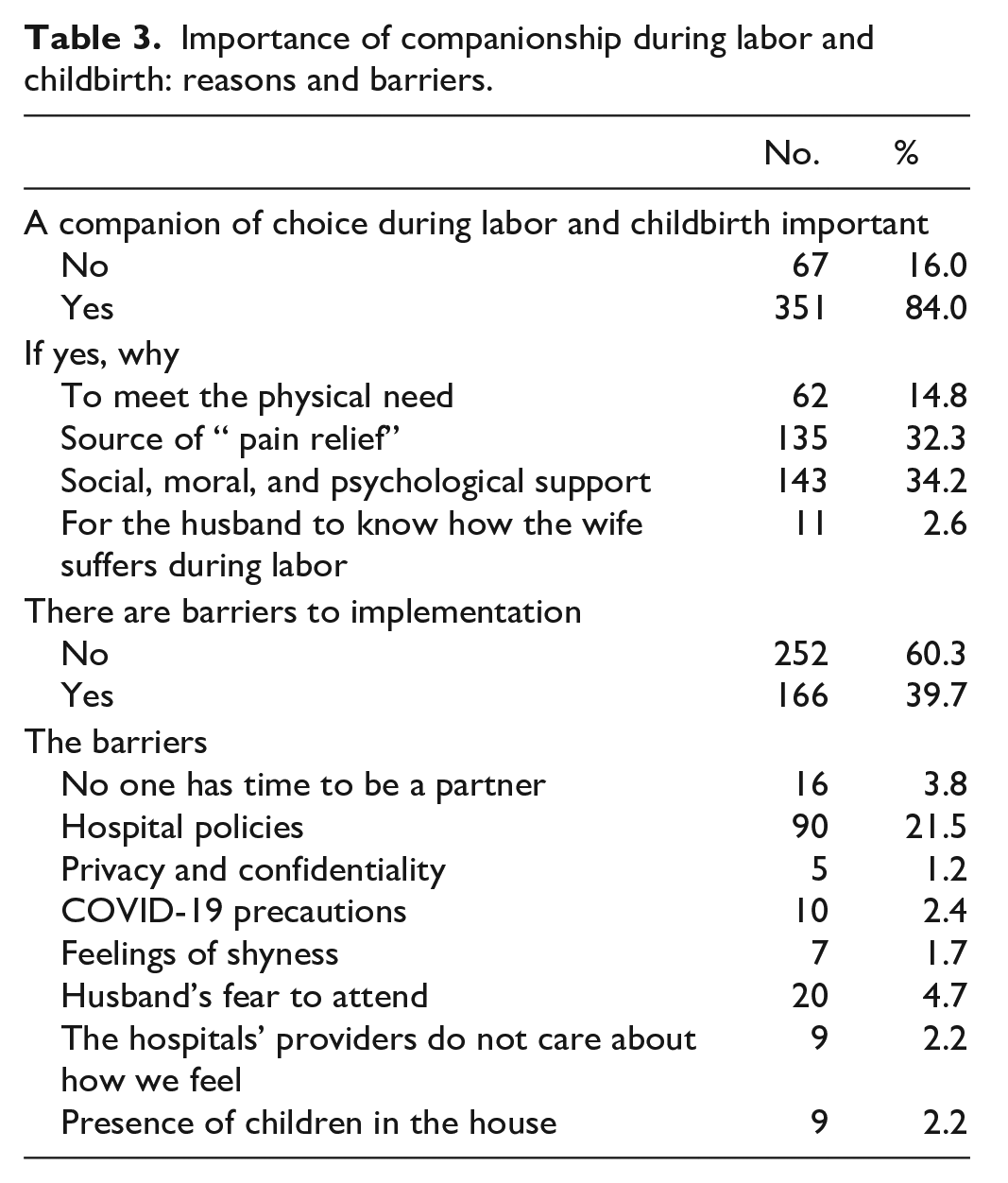
The table also highlights the barriers encountered in implementing companionship during labor. Approximately 39.7% of participants reported facing barriers. Among them, 2.6% expressed a desire for companionship during labor to educate their husbands about the woman’s labor experience. Hospital policies were identified as the primary barrier by 21.5% of respondents. In contrast, 4.7% considered their husbands’ fear of being present during labor as a hindrance. In addition, 3.8% perceived a lack of time as a barrier to having a companion during labor.
Table 4 displays the correlation between women’s desire for a companion during labor, delivery, and postpartum and their personal characteristics. The table reveals that there is a statistically significant relationship between several variables and the participants’ desire for companionship during labor. These variables include age, the number of previous births, educational level, and the place of labor. However, no significant associations were found between marital status, occupation, pregnancy, labor complications, and the desire for companionship.
Relation between studied women desire a companion during labor, delivery, and postpartum and their personal data.

Percentage calculated by row.
Statistically significant at 0.05.
Statistically significant at 0.01.
Discussion
The objective of the study was to assess women’s attitudes, prevalence, related factors, and perceived barriers of birth companionship in a city in Saudi Arabia. Our findings show that majority (82.8%) and only 43.2% had a labor companion present during delivery. The primary obstacle to labor companionship reported was hospital policies. Other barriers identified included husbands’ fear of being present during labor and limited availability of time for companionship.
In Saudi Arabia, the maternal mortality ratio stands at 17 deaths per 100,000 live births. 29 The WHO recommends the inclusion of a chosen companion during delivery as a crucial component of high-quality and compassionate maternity care (WHO b., 2016). 27 This practice offers emotional, practical, and informational support to women, enhancing their childbirth experience. 30 According to a Brazilian study, the presence of a companion of the woman’s choice improved her satisfaction with birth. 31 However, not all women who desire a labor companion have access to one, particularly in low-resource settings. 32 Offering assessment and support to mothers during early labor has the potential to decrease the need for epidural anesthesia, facilitate labor progression, and improve maternal satisfaction. 33 According to the WHO (2017), companionship is crucial for providing women with respectful and high-quality maternity care. Having a companion during labor increases satisfaction and provides a sense of control and assurance for women. 34 The WHO (2018) recognizes the importance of offering both physical and emotional support during labor to ensure a positive birthing experience and improve outcomes for mothers and newborns. 14 Women who receive doula support often develop strong relationships with their doulas through regular meetings before delivery, which helps establish rapport and clarify expectations. 35
In our study, a significant number of women expressed their preference for having a companion during labor and childbirth, although their preference decreased after delivery. This finding aligns with a previous study conducted in Nigeria, which indicated that women preferred the companionship of their husbands during labor and delivery. 36 The need for the presence of the companion in the current study was reported by many of the participants. Some women needed their companions to feel stronger which is similar to the findings of a study on the emotional journey of labor, where women described entering a “zone” of timelessness and letting go of control. 37
This is also confirmed by a qualitative interview study, which revealed that birth companions attended to both the physical and emotional needs of women during labor process. However, the study emphasizes the significance of considering the unique needs of each women and suggests that additional training for birth companions would improve their role and help address any potential shortcoming during childbirth. 38
Furthermore, a meta-analysis conducted by Bohren et al. 10 in 2017 demonstrated that having a birth companion and continuous presence during labor have a positive impact on birth outcomes, reducing the likelihood of medical interventions and enhancing the overall experience for women.
However, these findings differ from previous studies conducted in Kenya and Ghana, where only a small percentage of women expressed a desire for a partner as a companion during childbirth.17,39 Furthermore, Afulani et al. 17 found that women’s preferences for having a companion varied depending on the stages of labor and delivery. Most women desired companionship during the first stage of labor but not necessarily at the time of delivery. While the presence of a companion is important, these findings might inform the need to assess the individual needs of women during childbirth.
Women in our study cited various justifications for desiring a companion, with the primary motivation being to receive social, moral, and psychological support. Interestingly, the desire for the husband to witness the labor experience ranked lower among the reasons provided. However, the primary reason for seeking a companion during labor and delivery is for physical support, while emotional support and the husband’s understanding of the woman’s pain are considered less significant.
The main barrier reported by the majority of participants in our study was related to hospital policies that restrict the presence of companions during labor and childbirth. According to WHO (2019), the introduction of labor companionship can be complex and requires restructuring of services and involvement of multiple stakeholders. It is vital to prioritize women’s desires and privacy in determining who is present during labor and delivery. 34 In contrast, previous studies identified overcrowding and privacy issues as the primary barriers to having birth companions.17,39
In addition, another study found that cultural attitudes about the impact of a partner’s presence during delivery and concerns about a potential loss of sexual attraction were among the worries expressed by women regarding their partners being present during birth. 17
Challenges arise when considering that not all women have a preference for a labor companion, and this can be influenced by various factors, such as sociodemographic characteristics and financial considerations. Our study revealed that younger and more educated women, those delivering in private hospitals, and those with more birth complications were more inclined to seek a companion during labor, delivery, and postpartum. This finding is aligned with a study carried out by Afulani (2018) which revealed that women with higher socioeconomic status and higher level of education were more inclined to choose their partners as companions during labor and delivery compared to women with lower socioeconomic status. 17 Another study conducted in Nigeria reported that the majority of women (86%) opted for their husbands as their labor companions, possibly due to the inclusion of women with a higher socioeconomic status. 35
Limitation
First, the data relied solely on self-reporting, which may introduce potential biases and limitations. Second, the research was conducted exclusively in the Al Ahsa district, raising concerns about the generalizability of the findings to other women and caregivers in Saudi Arabia. Moreover, our study did not address all barriers related to birth companionship, including overcrowding, mistrust and lack of confidence in companions, familial influences, distance to the facility, and economic status. Therefore, further research study is needed to address those barriers.
However, In spite of these limitations, this research significantly contributes to the understanding of social support in settings with limited resources. It represents one of the most extensive and thorough studies on childbirth assistance in Saudi Arabia, providing valuable insights into this topic.
Conclusion
The study findings indicate that women generally desire birth companionship, although their preferences may vary during the different stages of labor and delivery. While most women prefer companionship during labor, their preference may decrease during the actual delivery. However, it is concerning that many women do not receive continuous support throughout the entire process of labor and delivery. Addressing this issue requires interventions at multiple levels, including individual, companion, and healthcare provider levels, and changes to the health system and hospital policies. Various barriers, such as physical and emotional discomfort, privacy concerns, and regulatory restrictions, can hinder the provision of labor companionship.
In light of these findings, several recommendations can be made. First, it is important to educate women during their antenatal care about the advantages and benefits of having a birth companion to prepare them for labor and delivery. This can help increase their awareness and understanding of the support available to them. Second, healthcare providers should actively promote and support the idea of labor companionship to ensure that women have access to this form of support during childbirth. Their involvement is crucial in facilitating the implementation of labor companionship.
Further research is also needed to explore the attitudes of birth companions and husbands toward providing support during childbirth. Understanding their perspectives can help identify strategies to enhance their involvement and ensure effective support for women in labor. In addition, conducting qualitative research can provide a deeper understanding of women’s experiences and the factors that influence their decisions regarding birth companionship.
It is also recommended to investigate the long-term impact of birth companionship on maternal and neonatal health outcomes. This can provide valuable insights into the potential benefits and advantages of having a birth companion throughout the entire childbirth process.
Finally, conducting similar studies in different regions of the country would be beneficial to gain a more comprehensive understanding of the use of labor companionship during childbirth and to identify any regional variations or specific challenges that may exist.
By implementing these recommendations, we can work toward promoting birth companionship as a standard practice, which in turn can have a significant positive impact on maternal and neonatal health outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231224553 – Supplemental material for Women’s attitudes, prevalence, related factors, and perceived barriers of birth companionship in Saudi Arabia
Supplemental material, sj-docx-1-whe-10.1177_17455057231224553 for Women’s attitudes, prevalence, related factors, and perceived barriers of birth companionship in Saudi Arabia by Ola Mousa, Basma Salameh, Mohammed Alqahtani, Maryshela David, Aishah A Almefarfesh, Duaa Al Duhilan, Asmaa Saber Ghaly, Nourah Alsadaan, Fadia Ahmed Abdelkader Reshia and Zainab Mohammad Ahmad Alsandal in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231224553 – Supplemental material for Women’s attitudes, prevalence, related factors, and perceived barriers of birth companionship in Saudi Arabia
Supplemental material, sj-docx-2-whe-10.1177_17455057231224553 for Women’s attitudes, prevalence, related factors, and perceived barriers of birth companionship in Saudi Arabia by Ola Mousa, Basma Salameh, Mohammed Alqahtani, Maryshela David, Aishah A Almefarfesh, Duaa Al Duhilan, Asmaa Saber Ghaly, Nourah Alsadaan, Fadia Ahmed Abdelkader Reshia and Zainab Mohammad Ahmad Alsandal in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.