
Abstract
Background:
Vaccination serves as an efficient primary means of control for infectious diseases. However, in the case of the COVID-19 pandemic, pregnant women within the United States had the lowest rates of COVID-19 vaccination and reported the lowest intent to vaccinate.
Objectives:
To explore the decision-making process for COVID-19 vaccination for people pregnant during the pandemic.
Design:
A secondary analysis of data from a mixed-methods study that examined the impact of COVID-19 on experiences of prenatal care, birth support, and delivery in the Southern United States.
Methods:
This study used a descriptive phenomenological approach to thematically analyze in-depth interviews (n = 20) with adult women who were pregnant by January 2020 and had their prenatal care and delivery during the pandemic beginning in March 2020. The transcripts were de-identified, coded, and thematically analyzed to saturation to identify drivers of COVID-19 vaccine decision-making based on COVID-19 vaccination status and timing. Comparative analyses were conducted to assess differences in decision-making processes based on race/ethnicity and parity. Participants also completed a sociodemographic survey that included their COVID-19 vaccination status.
Results:
Two themes emerged, the weighing of parallel risks and priorities from different sources resulting in vaccine decisional conflict and the need to reconcile that conflict via multiple strategies. All participants weighed priorities and risks from multiple areas of their lives and described internal conflict around vaccination. Participants described tailoring decisions to household dynamics, reconciling public and private values around vaccination, and the impact of their identities on the decision-making process. While many described concerns over vaccine safety and fetal health, uniquely, many highlighted weighing the impact of prior pregnancy loss history, with some choosing other preventive measures like social distancing or mask-wearing, which they deemed less risky.
Conclusion:
Pregnant people make complex COVID-19 vaccination decisions, which must be considered in future vaccine messaging and advocacy for this group.
Introduction
In March 2020, the World Health Organization declared the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease 2019 (COVID-19)) outbreak a global pandemic. 1 Since the declaration of this emergency, mounting evidence shows that pregnant and recently pregnant people remain at risk of experiencing severe consequences from COVID-19.2 –4
Pregnancy coincides with marked cardio-pulmonary adaptations or changes in the immune system, heart, and lungs, resulting in greater adverse health outcomes from respiratory infections. 5 In 2022, there were 225,656 confirmed cases of COVID-19 among pregnant people in the United States resulting in 306 deaths.6,7 A global pooled data analysis of the consequences of COVID-19 infection from 12 countries highlighted that pregnant people had an eight times greater mortality rate than nonpregnant persons. In addition, post-infection, they were more likely to need intensive care admission and critical care intervention, including advanced respiratory support or mechanical ventilation. 8 Further nonmortality risks for pregnant people included dyspnea, low respiration rate, postpartum fever, pneumonia, and a cascade of negative psychosocial and mental health outcomes including increased stress, anxiety, and depression.9 –14
COVID-19 vaccination remains a top public health priority for pregnant people, with the Centers for Disease Control (CDC) recommending vaccination for pregnant and breastfeeding people. Despite evidence of both the safety and efficacy of the COVID-19 vaccine, rates of vaccination as of 2021 were remarkably low (<50%) for pregnant people and remain so. 15 Vaccination status in this population differs by socioeconomic status, educational status, and race/ethnicity, with the lowest vaccination rates being among non-Hispanic Black women, at 15.6%. 16 A 2022 systematic review of COVID-19 vaccination among pregnant people found that vaccination acceptance was lower among people of color, younger age, and lower educational attainment. 17 Pregnant people who had previously refused the influenza vaccine and those who lacked adequate provider counseling also had lower vaccination acceptance. 18 Pregnancy is a critical and abbreviated period for assessing risks to the health of the pregnant individual and fetus. Vaccine decision-making during pregnancy is complex, and pregnancy remains a key factor influencing vaccine hesitancy.19,20 An extensive body of work on vaccine decision-making surrounding other routine immunizations such as influenza and pertussis provides insights into the variety of interconnected factors pregnant people contemplate prior to uptake.21 –24
Recent data about COVID-19 vaccination among pregnant people are primarily quantitative and often highlight safety concerns. A survey of 387 Californians in December 2020 found 57% expressed COVID-19 vaccine hesitancy as vaccine rollout was occurring and 27% indicated no intention to vaccinate when they were eligible. 25 This study also found that low self-knowledge or not knowing enough about the vaccine was highly predictive of hesitancy to vaccinate. Another study conducted in early 2021 found that among 300 Turkish women, 63% expressed hypothetical refusal of future COVID-19 vaccination due to concerns about vaccine safety. 26 An online survey of 106 vaccine-hesitant parents and pregnant Australians found that vaccine decision-making was influenced by multiple factors including vaccine safety concerns, the sources of information accessed, and a previous negative immunization experience. 19 This study addressed attitudes toward all immunizations but highlighted how pregnant women had concerns regarding the COVID-19 vaccine, that was in development and testing at that time, that outweighed perceived risks of COVID-19-related morbidity and mortality. A survey of 300 pregnant women amid the COVID-19 vaccine rollout in Ireland found a bifurcated result, with around 1 (38%) of 3 of respondents agreeing they would receive a vaccine during pregnancy, while another 1 (36%) of 3 reported they were unlikely to, with the most common reason cited as concerns about safety for the fetus. 27 Another key factor cited in COVID-19 vaccine decision-making is the relationship between pregnant individuals and health workers, which is foundational to building trust in vaccination. A qualitative study in Kenya found that among 84 individuals, including pregnant women and health providers, vaccine safety was a top concern that eroded actual COVID-19 vaccination uptake among pregnant and lactating people. Health professionals interviewed in this study expressed similar concerns and myths to pregnant individuals, highlighting the need to develop a supportive and educated health workforce as a key player in the vaccine decision-making process for pregnant persons. 28
This study employs the precaution adoption process model (PAPM) and the theory of planned behavior (TPB) to understanding pregnant women’s decision-making process around COVID-19 vaccination, drawing from the work of Shapiro et al. 29 (see Figure 1). PAPM identifies six stages an individual might navigate as they make decisions to take precautionary action. We apply five stages in our study. These five stages include not having heard of COVID-19 vaccination (Stage 1, unaware of action), being ambivalent about vaccination (Stage 2, undecided), deciding not to take the COVID-19 vaccine (Stage 3, deciding not to act), deciding to take the COVID-19 vaccine (Stage 4, deciding to act), and having a COVID-19 vaccination (Stage 5, taking precautionary action).29,30 The TPB conceptualizes the individual-level belief structures and multiple predictors that influence decisions to carry out health behavior. 31 These influences include attitudes toward vaccination, belief in vaccination’s benefits relative to risk, and perceived control over behavior.31 –33 Currently, there is limited qualitative information available on COVID-19 vaccine decision-making among pregnant people that have applied PAPM or TPB. This study retrospectively examines vaccine decision-making for pregnant individuals residing in Georgia in the Southern United States with an emphasis on elucidating differences across key demographic characteristics.
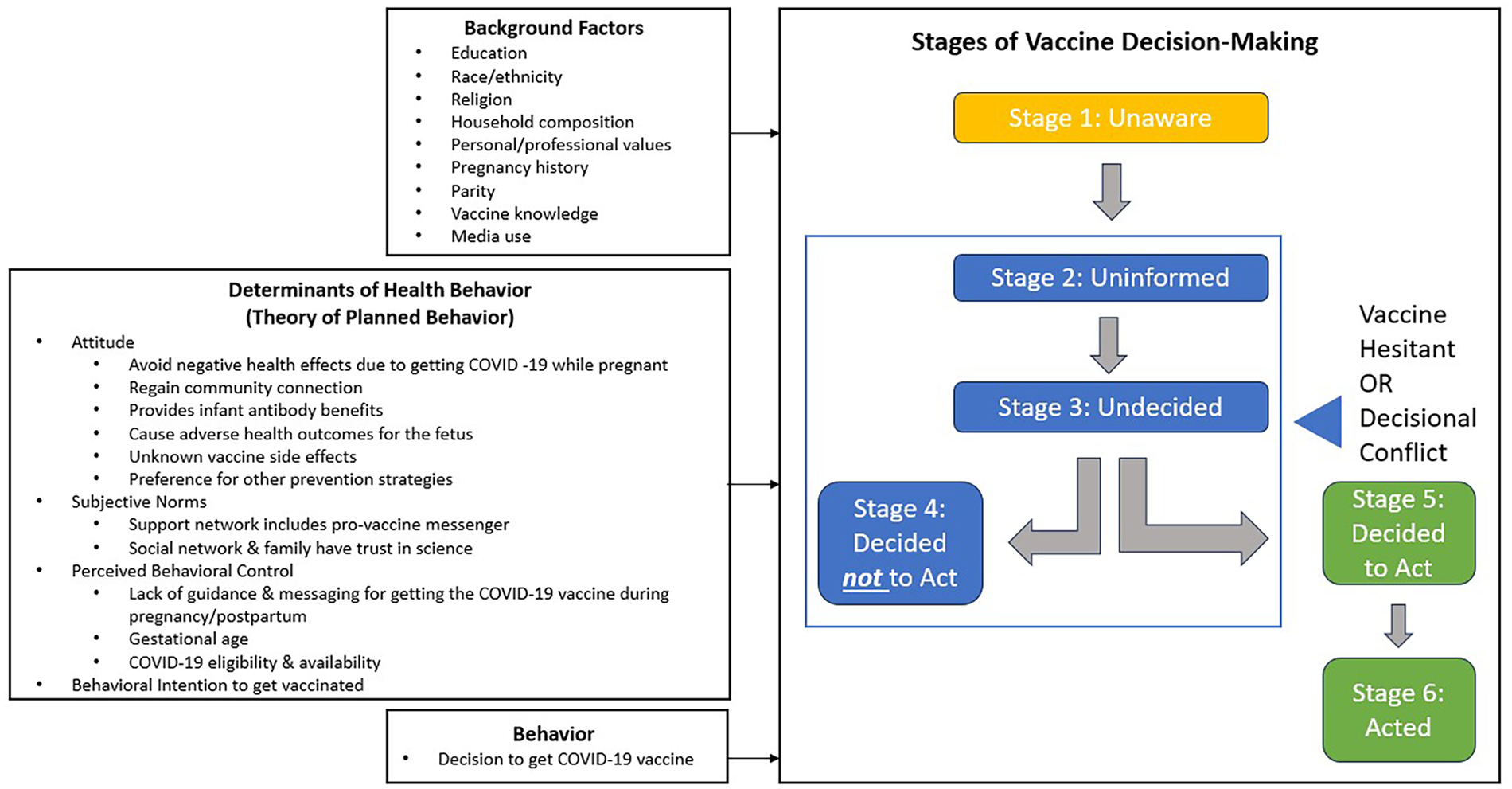
Conceptual model of the coronavirus disease 2019 vaccine decision-making process in pregnancy.
Methods
Study design
This is a secondary analysis of data from a cross-sectional, sequential mixed-methods study on the impact of COVID-19 on birth care and support among women who received prenatal and postpartum care during the COVID-19 pandemic prior to 2022 in Georgia.
Participant and recruitment
Participants (n = 20) were eligible to participate in the study if they were pregnant by January 2020 and delivered in Georgia after March 2020. All participants were enrolled from March to June 2022. Individuals pregnant with multiples or who did not receive any of their prenatal care in Georgia were excluded. Participants were purposively sampled to include diversity in parity and racial/ethnic identities, with a target of at least 40% of the sample identifying as a person of color. Study recruitment strategies included posting flyers in shared community spaces and distributing digital flyers through pregnancy-related social media groups, state-wide organizational listservs, and parent groups in the Metro Atlanta area. The study flyer listed the eligibility criteria and participation requirements alongside the questions “Did you have a pandemic baby?” and “Would you like to take part in a research study on how your prenatal care & birth was impacted by COVID-19?” Interested participants were asked to contact the study team via the email address provided on the flyer.
Data collection team and procedures
The study team consisted of principal investigators (PIs) Subasri Narasimhan, PhD, MPH, Leslie C.M. Johnson, PhD, MPH, and Research Assistants (RAs), Tahira L. Perry, MPH, Joi Henry, MPH, and India Stevenson, MPH(c). All individuals on the study team identify as female and women of color. One member of the study team was a first-time parent. The PIs have extensive experience in mixed-methods research and systematically trained both RAs in qualitative data collection and analysis.
Interested individuals (N = 22) emailed the study team with follow-up contact information to schedule an eligibility screening call. Of the 22 participants, 20 went on to participate, two were dropped due to nonresponse after three attempts via phone and email (91% response rate). Once screened, individuals who met the eligibility criteria (n = 20) were asked to provide written electronic consent and were then asked to complete a brief preinterview survey. During consent, RAs described the study motivations, goals, risks, and benefits. After completion of the consent process, the 18-question sociodemographic survey collected information on participant characteristics including age, gender, race/ethnicity, educational attainment, marital status, employment status, insurance coverage, as well as information on the number of household members, job loss during COVID-19, COVID-19 testing behaviors, COVID-19 medical history, COVID-19 vaccination status, vaccination timing, and pregnancy and childbirth history.
Individuals who provided written informed consent and completed the preinterview survey were then scheduled to complete a 1-hour online Zoom interview with no third parties present. Interviews were audio-recorded and transcribed verbatim using HappyScribe, an automatic transcription software. 34 Transcripts were then fidelity checked by a research team member and de-identified to ensure participant confidentiality. All audio recordings were deleted following transcription quality checks, and all interviewees were assigned a study identification number, which served to link study records while protecting the respondent’s identity.
The study (#00003607) was considered human subjects research but exempt from further review and approval by Emory University Institutional Review Board (IRB) under 45 CFR 46.104(d)(2)(iii) because the research only involved interactions involving the use of survey and interview procedures. However, researchers adhered to the ethical standards set by the World Medical Association Declaration of Helsinki 35 while performing the research. All participants provided written informed consent prior to data collection activities, and confidentiality procedures were implemented during study activities to ensure participant’s privacy was protected.
In-depth interview guide
The in-depth interview guide consisted of open-ended questions exploring four key areas: (1) the impact of COVID-19 on pregnancy support and birth experiences, (2) the differences in access to prenatal care between primiparous and multiparous women, (3) the perceived risk of COVID-19 and attitudes toward COVID-19 prevention strategies, and (4) the impact of the pandemic on women’s postpartum access to care and psychosocial health outcomes. Interview probes were included to examine vaccine decision-making. The interview guide was piloted and revised by SN during the first four interviews. SN and JH conducted all remaining participant interviews. Interviews on average lasted 66 min, with total times ranging from 52 to 87 min. All participants completed an 18-question sociodemographic survey with questions about an individual’s COVID-19 vaccination status and pregnancy history collected using REDCap. 36
Data analysis
This secondary analysis used a descriptive phenomenological approach to analyze narrative interview data that related to COVID-19 vaccine decision-making processes. 37 This approach involved seven iterative stages: (1) reading through all participant accounts multiple times to familiarize oneself with the data, (2) identifying significant statements (i.e. all accounts related to COVID-19 vaccination), (3) formulating meanings, (4) clustering themes, (5) developing an exhaustive description, (6) producing the fundamental structure, and (7) seeking verification of the fundamental structure.37,38
In this study, the phenomenon of interest was COVID-19 vaccine decision-making. Throughout the analysis process, three study team members generated memos to bracket assumptions and interpretations of the data through a practice of reflexivity. Dedoose was used for data management. 39 Coded data pertaining to vaccination, risk perception, decision-making, and types of support were used to facilitate stage 2 of the analytic process and were employed to reach thematic saturation, with 10% of data being double-coded to ensure consistency. Thick descriptions were developed for the identified themes and condensed down into summative statements that reflect essential elements of the vaccine decision-making process. Survey data on participants’ vaccination history and sociodemographic characteristics were used to verify how women’s lived experiences differed across groups (i.e. race/ethnicity, vaccination status, and prior adverse reproductive experience). Descriptive statistics of these quantitative data were generated to summarize the key sociodemographic characteristics and vaccination status of study participants. This article adheres to the Standards for Reporting Qualitative Research (SRQR) guidelines 40 (see Supplemental Material 1) and the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) (see Supplemental Material 2). 41
Results
Participant characteristics
Table 1 describes the participant characteristics of the sample. The mean age of the self-identified cis-gendered women interviewed was 35 years (R: 24–43 years). Most participants identified as White (60%, n = 12). The remainder of the participants identified as Black (30%, n = 6) and multiracial (White/Asian) (5%, n = 1). Only one participant (5%) identified as Hispanic/Latinx. A total of 60% of participants were primiparous, the reported pregnancy was their first live birth (n = 12), while 40% (n = 8) were multiparous, having had previous live births. Most participants (n = 17, 85%) held advanced degrees (i.e. master’s or doctoral degree) and were married (n = 19, 95%).
Demographic characteristics of participants.
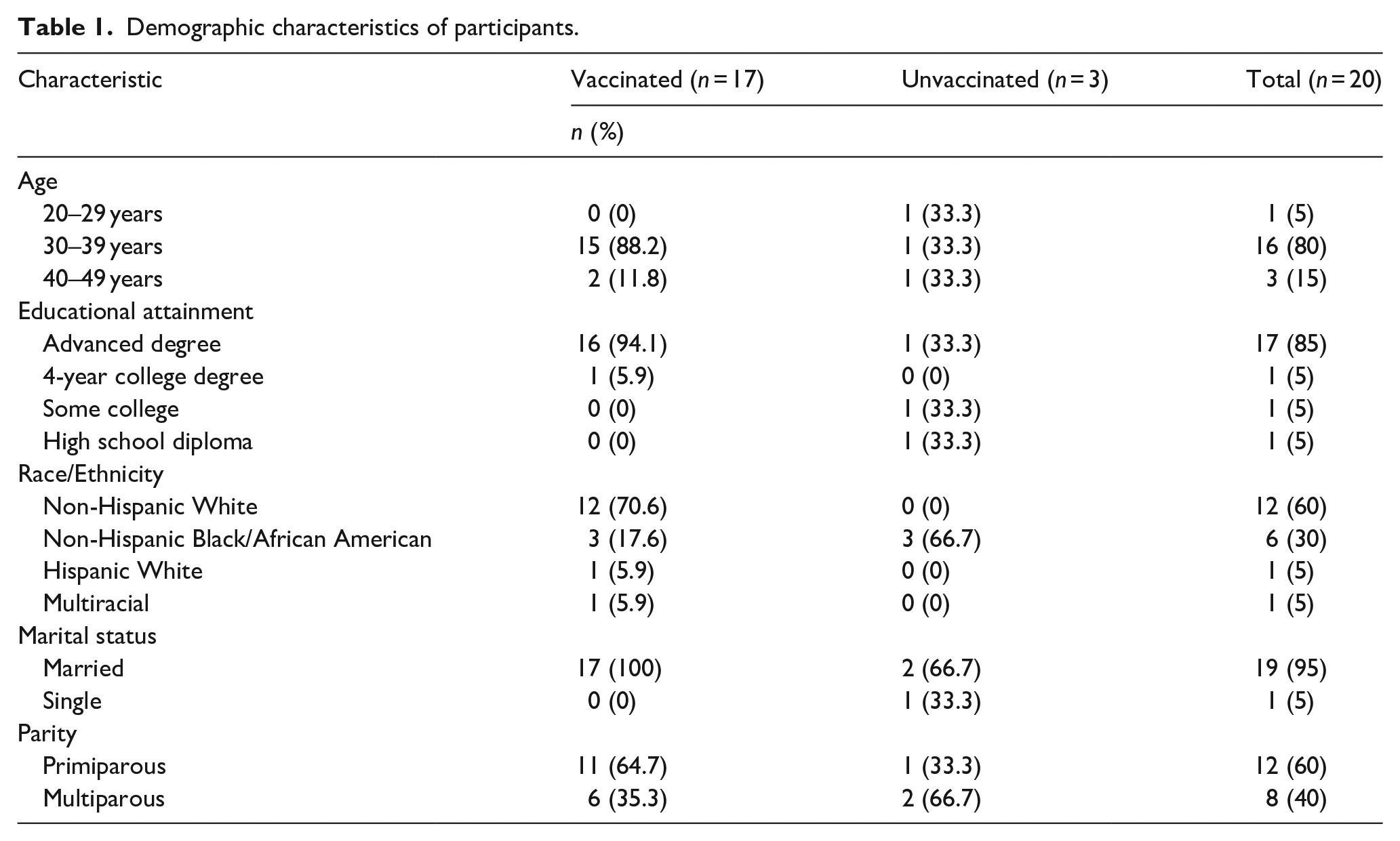
Most women (85%, n = 17) were fully vaccinated (i.e. received two primary vaccine doses of the Pfizer or Moderna vaccine or the single Johnson and Johnson vaccine), and of those women, all indicated receiving a COVID-19 booster. The remaining three women (15%) reported being unvaccinated (i.e. had not received a single COVID-19 vaccine dose). Finally, among vaccinated participants, 7 (41%) received the vaccine during pregnancy while 10 (59%) received vaccination postpartum. The 10 participants who received their first vaccination postpartum delivered between April 2020 and February 2021 when COVID-19 vaccines were unavailable. Two of the three unvaccinated participants had the option of getting the COVID-19 vaccine during pregnancy and chose not to, whereas the third gave birth prior to vaccine development.
Themes
The data were clustered around two themes, the weighing of parallel risks and priorities from multiple sources of decisional conflict and reconciling that conflict via multiple strategies.
Decisional conflict around COVID-19 vaccination involved weighing parallel risks and priorities, often resulting in a hesitancy to vaccinate while pregnant
All study participants began their vaccination decision-making process prenatally and described their need to weigh priorities and risks from multiple areas of their lives in tandem. The overlap of these priorities resulted in feelings of internal conflict around vaccination, resulting in a delay or refusal of vaccination for some participants. Thus, participants fell on a continuum, with a minority expressing no decisional conflict and a minority of people describing high levels of conflict, with most people falling in between these extremes.
Similar decisional conflicts existed among participants who ultimately became vaccinated and those who remained unvaccinated. Importantly, most participants were aware and concerned that their pregnancy made them more vulnerable to COVID-19 and subsequent adverse health outcomes, but how individuals arrived at their decision to vaccinate during pregnancy, delay to postpartum, or forgo vaccination altogether varied relative to how they weighed concerns relative to elements of the TPB, including household-specific dynamics, their prior experiences of negative reproductive health outcomes, and if vaccination aligned with their personal value system.
Moreover, there seemed to be differences in generational exposure to and trust in scientific processes, like vaccination. Participants with diverse backgrounds expressed differing action thresholds for COVID-19 research. For instance, participants with generational exposure to and trust in scientific knowledge, for example, coming from families of physicians or health professionals, described having lower thresholds for research-based evidence for vaccine safety, whereas participants without generational exposure to and trust in scientific knowledge expressed more vaccine hesitancy and needed extensive empirical proof of vaccine safety. In this sample, all Black participants described being a primary source of knowledge around vaccination for their extended families and peer networks.
Sources of conflict in vaccine decision-making
Household risk and priorities
Many interviewees described families as a primary factor contributing to risk concerns. Most participants were concerned with the possibility of family members exposing the household to COVID-19 and the possibility of being the person to expose their family members to the virus. The concern of outside exposure was especially prominent in households with children below the age of 5 who were unable to receive COVID-19 vaccination when the interviews were conducted, and who had the potential to be exposed to the virus in school or childcare settings. In addition, they weighed the presence of underlying conditions relative to the protectiveness of the vaccine for themselves. For example, a select few unvaccinated participants mentioned they feared how vaccine side effects might exacerbate underlying health conditions in themselves, making them unable to care for their children. A parent of three other children discussed that she relied heavily on herbal medicine because she feared the impact of COVID-19 vaccination on her asthma.
Between my husband and my little ones with asthma and myself with chronic bronchitis, just kind of not knowing [the possible vaccination side effects] (Non-Hispanic Black, 41 years old)
Participants who did not have other children in the household made similar determinations for themselves and their risk profiles based on the exposure of spouses or older family members.
Mismatch of public and private values and priorities
The majority of participants described their public and private priorities contributing to decisional uncertainty around vaccination. For most, their public stance on vaccination was supportive, with many being the conduit of knowledge or source of trust for vaccine information in their networks. However, their choices became more complicated when weighed within the context of pregnancy. One source of conflict for the majority was the focus of or messaging in their careers or jobs, which were often in health care, public health, or other closely related fields. These participants espoused vaccination publicly and they often supported vaccination in conversations with their peers and family, but their personal calculus during pregnancy was challenging. For example, many participants expressed working within the public health field and supporting the general concept of vaccination; however, they faced internal conflict when deciding whether to be vaccinated for COVID-19 while pregnant, due to lack of medical guidance, trusted information, and empirical studies about vaccination during pregnancy. Specifically, a public health practitioner explained the discordance between her professional and personal priorities,
I have this internal conflict given that I work for CDC, and I am pro-vaccine. They’re like, you need to take this vaccine. I’m like, okay, yes, no problem, no questions asked. I trust the science; I trust the medicine. And working with CDC, I try to promote vaccinations because I know they’re important. Yeah, but I’m torn about this one because looking at the data I read, first I need to do more research and actually look at the scientific articles and what has been written about it. (Non-Hispanic Black, 33 years old, primiparous)
For those who had COVID-19 vaccines available while pregnant and who worked in a medical or public health-related field, there was a pressure to uphold their public priorities while also deciding how to balance the health considerations of both parent and baby. Only one public health practitioner described how their religious beliefs determined their decision to forgo vaccination.
Prior experiences of negative reproductive health outcomes
Participants commonly described two domains of reproductive experience, concern over fetal anomaly and experience of prior pregnancy loss, as related to their vaccination decision-making. Many participants discussed concern that COVID-19 vaccination may lead to potential adverse health outcomes for their fetus. Specifically, some participants feared that the active ingredients in the vaccine might potentially impact fetal development or cause fetal abnormalities. Many times, the risk assessment was made more complex by individual’s professional identities, which were largely within the fields of public health and medicine. The internal conflict resulting from one’s professional identify being at odds with personal concerns regarding the potential unknown side effects of the vaccine was best captured by another Black participant in her late thirties who shared
As a person in public health, I was having an internal conflict with myself. Do I get this vaccine that they don’t know much about? How would it affect me in pregnancy? Will my baby have side effects from it? (Non-Hispanic, 38 years old, primiparous)
Participants who chose to get vaccinated emphasized that their concern over COVID-19 health effects while pregnant outweighed worries about vaccine side effects and safety; thus, they felt that not getting vaccinated put themselves and their baby at a greater risk for adverse health outcomes.
In addition, for some participants, past experiences of pregnancy loss reduced their threshold for fetal risk and influenced the timing of vaccination, resulting in some getting vaccinated as soon as they were eligible, some delaying vaccination to postpartum, or for one, choosing not to get vaccinated. A Hispanic participant in her early thirties shared how she had experienced a miscarriage just prior to the pandemic and how the heightened risk of maternal or fetal death and severe illness that could result from getting COVID-19 while pregnant led her to get vaccinated during pregnancy. Furthermore, the first-time parent recalls in her narrative, that vaccination afforded some relief from concerns around using appropriate infection control measures. When describing how the COVID-19 prevention messaging she received from her medical team, advice that seemed overwhelming and scary at the time, re-enforced her decision to get vaccinated as soon as eligible, she stated
I was so scared until I was fully vaccinated. When I went for my first appointment, I left there in tears. They were like, you have to double mask, you cannot leave the house, your husband has to double mask, you cannot get COVID while pregnant. We had just come out of that [COVID-19] spike, and there had been a lot of pregnant women who had died. I was as homebound as we could [be] at the end because the doctors again, even though I was vaccinated, were like, we have two women on ventilators right now who are pregnant. It’s very scary when it’s your first pregnancy . . . (Hispanic White, 33 years old, primiparous)
Another 36-year-old participant who had experienced multiple miscarriages prior to the pandemic and who was planning their pregnancy described how they timed their vaccination, which was available before they became pregnant, to avoid the possibility of pregnancy loss:
I was trying to be very thoughtful about when I can’t get my vaccinations based on kind of when I was going to be ovulating, when I might have implantation to get pregnant. I’m obviously too over-educated and thinking about how to get pregnant, but I was trying to time it so that I would get my second vaccination before theoretically, a pregnancy could implant just in case, because my main fear was, like, I would get a fever, and fever can be very dangerous for early pregnancy, not because I was concerned that COVID vaccination would be at all, like, bad for the fetus, but more just kind of the side effects [on the pregnancy]. (Non-Hispanic White, primiparous)
Weighing the different considerations was an emotional process, however, and ultimately led this participant to complete her vaccine series while pregnant and postpone getting a booster until after delivery when they felt the pregnancy would not be impacted and there would be the added benefit of passing antibodies to the baby while nursing. Every individual who experienced prior adverse reproductive health outcomes expressed a want to minimize health risks and maximize benefit to their baby, resulting in either the decision to vaccinate or forgo.
Concerns of fetal anomalies and pregnancy loss related to vaccination were more common in first-time parents and those who had experienced previous loss, both of whom had a more pronounced “fear of the unknown.” Internal conflict resulting from these concerns was exacerbated by the high levels of information access some participants had due to their professional expertise. One participant described how the process of navigating pregnancy for the first time was made more stressful by her and her spouse’s awareness of how vulnerable pregnant people are to COVID-19, stating
. . . we both worked for CDC [Centers for Disease Control], but he had been working on the pandemic response and so he was very aware of the ins and outs and of the data, the risks for pregnant women (Non-Hispanic Black, 33 years old, primiparous).
This individual went on to detail how she was unsure about whether she would have gotten the vaccine if it had been made available prior to her delivering her child, but that she received it soon after to allow for added antibody protection for her child through breastfeeding. These sentiments of concern about vaccinating during pregnancy, but also wanting to confer antibodies to infants, were mirrored by other women for whom vaccination was not available during pregnancy, most of whom received the vaccine as soon as eligible in the postpartum period.
A final important vaccination consideration was the likelihood of experiencing maternal mortality, which emerged among three participants, all Black women, one of whom remained unvaccinated. One 38-year-old Black participant who was vaccinated during pregnancy described the interplay between her racial identity, decision-making during pregnancy, and feelings of dismissal in clinical environments. Specifically, they mentioned feeling more comfortable with Black providers and/or doulas to truly care for their birthing experiences and outcomes.
They did know that there was a more likelihood of pregnant women dying. Couple that with being a Black woman and the complicating factors of that in the healthcare system while being pregnant, I was like, oh, God, here’s another thing for them to ignore . . . and luckily, my OB GYN is a Black guy, so I felt pretty safe with him and being able to tell him, don’t kill me, don’t let me die. (Non-Hispanic Black, primiparous)
These women described the salience of high rates of maternal mortality in the United States among Black women as an added stressor to the COVID-19 pandemic without prompting. In addition, these women mentioned how the experience of pregnancy as a Black woman is nuanced, impacting their pregnancy decision-making and vaccine considerations.
Decisional conflicts around vaccination arose across the majority of participants irrespective of their ultimate vaccination uptake. Furthermore, decisional conflict linked to weighing multiple levels of risk, including consideration of household dynamics, reconciling of public and private priorities, and weighing past negative reproductive health outcomes as well as current fetal considerations. Importantly, these influenced the timing of vaccination across different periods of pregnancy and postpartum or led a minority to forgo vaccination and use alternative infection control strategies.
Reconciling decisional conflict
Many respondents expressed their desire to reconcile decisional conflict around vaccination. Most employed several strategies, seeking additional public health information from data sources available to them (e.g. medical journals and CDC reports), consulting advice from medical professionals entrusted with their care, or seeking out guidance from public sources like social media. First, several participants described how they conducted independent research on the COVID-19 vaccine hoping to find data relevant to pregnant women, with those affiliated with public health and medical professions emphasizing the amount of time they spent seeking out the latest data or identifying individuals within their social networks who could weigh in as an expert and help interpret how they should respond to emerging information. For example, one individual with an advanced degree in public health shared
I knew the people who were on the community guidelines committee for CDC for COVID. For me, the [COVID-19 prevention] messaging was always directly from individuals I worked with and colleagues and friends that I had. And so, whenever [I was] considering something, in terms of, like, is this risky or what’s the latest evidence on this? Or what does epidemiology say? We would talk to our friends who are on the response team. (Non-Hispanic White, 36 years old, primiparous)
Individuals also consulted with their personal medical providers to reconcile their feelings of wanting to protect themselves and their fetus while still advocating for public health practices. Again, while most believed in the science and trusted infectious control policies, they also expressed reluctance to put their immediate families or their pregnancies at risk. A first-time parent who chose to get vaccinated while pregnant expressed frustration over the available guidance and its lack of utility in helping people decide whether to get vaccinated while pregnant, stating
I did research on my own, but at the time, there wasn’t any real research on COVID and pregnancy because they weren’t doing any trials for the vaccines on pregnant women. They didn’t know how COVID really affected pregnant women. (Non-Hispanic African American, 38 years old, primiparous)
Women acknowledged that the CDC vaccine recommendation for pregnant women was prominent and clear; however, most expressed that the lack of supporting evidence on vaccine safety, specific to pregnant women, contributed to hesitancy. Furthermore, the absence of appropriate vaccine messengers made decision-making around vaccination burdensome and complex with the onus on the pregnant individual to both gather appropriate evidence and sort through the rapidly changing guidelines.
Participants who worked in the health fields and/or had members of their support network (i.e. spouse/partner, family members, friends, and neighbors) and who were public health practitioners or clinicians were more likely to trust the safety of the COVID-19 vaccination protocol. Participants’ closer proximity to scientifically vetted health information made some feel like they had the self-efficacy to make informed decisions. The majority of respondents expressed how the ability to commune and discuss options with trusted members of their social networks eased the decision-making process. Specifically, a participant with one prior child mentioned her experiences with support and resource sharing within her own social networks. These experiences of sharing improved her comfort with vaccination and eased her concerns.
I’m very comfortable getting the COVID vaccination. I had no reservations for my spouse or parents, anyone in my friend group to receive it. Another layer of our family history is that I grew up in the [Atlanta] community where my neighbors are scientists and my friend group that graduated from [university] are scientists. A lot of them shared on social media research and excitement [for vaccinations]. A lot of my friends are healthcare providers. So, in my social media network, it was overwhelmingly excitement for vaccinations and sharing of precautions that we were taking to prevent the spread of COVID-19. (Non-Hispanic White, 34 years old, multiparous)
Within these conversations, most participants reported that there was no, or minimal stigma associated with COVID-19 vaccination discussions within their support network, in comparison with conversations with individuals outside their trusted social networks (i.e. coworkers and health care providers). Several study participants who solicited COVID-19 advice from their health providers and did not receive adequate help or guidance in their vaccine decision-making process. Many participants felt overwhelmed and dissuaded by the manner (i.e. frequency, tone, and source) in which information related to pregnancy and vaccination was delivered, a sentiment that was expressed by most participants of color. These experiences led to concerns about receiving the COVID-19 vaccine. One participant, who identified as African American, discussed how the COVID-19 messaging produced overwhelming pressure for vaccination which led to an aversion to vaccinate.
There’s a lot of things out here [and] some vaccines are not mandatory. You have your baby at the hospital. They ask you; do you want the hepatitis B vaccine? They don’t just take your baby and just start vaccinating your baby. They ask you, and there’s a lot of things that’s deadly for a baby. So, I feel like if you’re not forcing me to get those, I shouldn’t be forced to get anything else. I feel like it should just be my choice. When people force things, that’s when I get a little skeptical, like, why are you forcing it? If it was just a choice, I probably would have done it, but the way it got forced, it kind of pushed me away from it. (Non-Hispanic, 24 years old, primiparous)
Finally, participants described how they received information on vaccination through social media platforms and other online networks which provided an experiential component that might not be available from the pregnant person’s primary provider. For instance, one participant informed the interviewer that her decision to be vaccinated in pregnancy was reinforced by her network of pregnant women and providers on social media.
On social media, I saw people sharing things, providers, especially who said, I’m a provider and I’m a pregnant person. And I chose to get that vaccine for these reasons. And if you want to send me a private message and discuss your situation, I’m happy to talk with you. (Non-Hispanic White, 34 years old, primiparous)
Specifically, she spoke about how she would follow (on social media), a health provider who was also pregnant during COVID-19. This provider created content about the reason she received the COVID-19 vaccine and encouraged her followers to privately message her for advice and to discuss personal circumstances.
For some pregnant women, the rationale for COVID-19 vaccination was centered around the comparison between the COVID-19 vaccine and any other vaccines administered and encouraged during pregnancy. These participant’s approaches to making these decisions were rooted in communication with health professionals, including primary obstetric physicians and nurses. Of the participants that expressed receiving COVID-19 vaccine communication with their OB/GYN team, a minority described clear and informative advice regarding risks of pregnancy and COVID-19 vaccination. A participant with one other child expressed how the COVID-19 vaccine was no different to her than other interventions, including routine vaccinations, that were suggested during pregnancy.
To me, it was just like any other intervention you do during your pregnancy when you get your TDAP, or you do if you come back with Group B Strep and they’re going to give you penicillin immediately. I was going to get my flu vaccine anyways. It was like, let’s just do it right. (Non-Hispanic White, 32 years old, multiparous)
Participants described wanting to make an informed decision, but most felt they didn’t have the guidance and information needed to make a clear and confident decision based on their perceived risks, medical history, identities, and values system.
Discussion
Our study describes COVID-19 vaccine decision-making for pregnant people who were highly educated and informed about vaccination; we highlight the elements of decision-making that resulted in hesitation to uptake vaccination during pregnancy and elucidate how participants’ overlapping identities, including identifying as a person of color, a first-time parent, or having a past pregnancy loss influence vaccine decision-making.
Decisional conflict was common, with most participants expressing some level of concern or hesitancy around taking the COVID-19 vaccine while pregnant. This aligns with the broader literature on COVID-19 vaccine decision-making among pregnant people, with most participants in this study citing concerns over lack of guidance or possibilities of fetal loss or abnormalities. Many participants highlighted that at the time of decision, vaccination guidance and data excluded pregnant individuals which resulted in them feeling that safety data were inadequate. 29 Extensive research examining the perceptions of COVID-19 vaccine safety among pregnant women underscores that low trust in vaccine safety is due to the lack of relevant data,26,42 likely corresponding with the low vaccination rates for pregnant people in the United States. 43
As noted, the overall sample was highly educated about vaccination and most had some health background. However, not all Black participants in this sample had proximity to public health and clinical networks and were often the primary knowledge holders in their networks. They more often expressed a lack of decision-making support as well as differences in generational exposure to and trust in scientific processes, including vaccination. This study further underscores the need for additional research around the nuanced concerns of Black women, including considerations around maternal mortality, and why some may be less likely to receive the COVID-19 vaccination. This need continues to be highlighted through data underscoring the racial and ethnic disparities in COVID-19 vaccination in Black populations, which are rooted in ongoing legacies of medical mistrust, differential and poor treatment, and racism by the health system and system actors.44 –46 However, it is crucial to interpret this result with some caution, as our sample was small and did not reach saturation for distinct racial or ethnic groups.
In addition, this study underscores a more nuanced look at the reconciliation of personal and public values that pregnant people undertook, and their sometimes unsuccessful reliance on health workers to resolve these discrepancies. Only one other qualitative study among pregnant and lactating people in Kenya identified similar dynamics among individuals and health workers. 47 Future work should examine and understand hesitancy among health workers and the appropriate role of other types of vaccine messengers for pregnant people as women in this study felt messaging around vaccination often didn’t align with their values/needs and that their providers were inadequate in meeting their needs.
Furthermore, many people in this study highlighted concerns about how the vaccine would impact the fetus. This reason is commonly cited in the literature around COVID-19 vaccination and echoes results from a cross-sectional survey study on pregnant women’s COVID-19 vaccine refusal in three US cities. 48 Although several studies have attributed these findings to misperceptions or vaccine myths,49 –51 our data identified an important concern, prior experience of pregnancy loss, as possibly driving this fear for some individuals. Greater research should be done on the role of prior reproductive histories of pregnant people to further understand the individual-level calculus of fetal and maternal risks surrounding vaccination in pregnancy.
Our study also demonstrates strategies that people take to reconcile and decide vaccine action, contextualizing the complex process occurring when a person moves toward a decision to vaccinate and drawing greater attention to the heterogeneity of those who begin as vaccine undecided, especially among pregnant people in a high-income setting. Findings highlight that pregnant people who are vaccine hesitant are not completely forgoing prevention, rather they substitute vaccination for other prevention strategies, including social distancing and mask-wearing, which they deem to have less likelihood of a negative outcome. 19 The ability to have informative and resourceful communication within their trusted networks, particularly with health provider contact, seems to heighten the opportunity for vaccine acceptance for pregnant individuals.19,52 This concept seems to arise due to an extension of trust within social networks and point to the need for future work that considers the social support needs of pregnant people. Finally, we need better evidence of the direct impact of this decision-making process on maternal health.
Limitations and strengths
Our study should be considered with some limitations. Our sample had limited variation in educational attainment, professional training, and insurance status and it is likely saturation was not reached with regard to certain participant characteristics. Therefore, although we highlight important areas for future research, we make limited claims about the connection between certain individual characteristics and vaccine behavior. However, assert that this niche sample allowed for a deeper understanding of how vaccine decision-making may operate in those without significant resource constraints. In addition, the interview guide was not designed to focus on vaccination, nor were vaccines available at the time of pregnancy for all participants, so data were considered and reported within the context of vaccine availability.
The study’s strengths included a sample size appropriate to attain saturation on the topic of vaccination and deliberate sampling for important characteristics, including diversity in race/ethnicity, first-time parenthood, and prior negative reproductive health experiences. Thus, these data allowed insights into vaccine decision-making relative to these important factors. Furthermore, the sample drew from a state in the US Southeast, and data may be transferable to other states with similar policy or resource contexts.
Conclusion
Though the emergency of the COVID-19 pandemic has ended, pregnant individuals remain particularly likely to have adverse health outcomes from COVID-19 and adequate examination of their decision-making processes around vaccination is necessary. Even those who are highly educated and informed experience some level of decisional conflict stemming from the consideration of multiple, complex factors, including their own risk assessments based on intersectional identities, household dynamics, and the reconciliation of public and private values. Many individuals feel the guidance from data and health providers to be inadequate; thus, the results of this study reiterate the needs for more multisectoral and targeted approaches to help pregnant people make informed vaccine decisions.
Supplemental Material
sj-docx-2-whe-10.1177_17455057231218211 – Supplemental material for “I was having an internal conflict with myself.” COVID-19 vaccination decision-making processes among pregnant women
Supplemental material, sj-docx-2-whe-10.1177_17455057231218211 for “I was having an internal conflict with myself.” COVID-19 vaccination decision-making processes among pregnant women by Subasri Narasimhan, Tahira L Perry and Leslie CM Johnson in Women’s Health
Supplemental Material
sj-jpg-1-whe-10.1177_17455057231218211 – Supplemental material for “I was having an internal conflict with myself.” COVID-19 vaccination decision-making processes among pregnant women
Supplemental material, sj-jpg-1-whe-10.1177_17455057231218211 for “I was having an internal conflict with myself.” COVID-19 vaccination decision-making processes among pregnant women by Subasri Narasimhan, Tahira L Perry and Leslie CM Johnson in Women’s Health
Footnotes
Acknowledgements
The authors would like to thank the participants of this study, as well as Joi Henry and India Stevenson for their efforts and support of the project.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.