
Abstract
Background:
Multiple studies have demonstrated that pregnant and lactating people who use cannabis perceive a variety of benefits from that use, offering some explanation of why rates of use continue to increase.
Objectives:
The aim of this study was to explore pregnant and lactating people’s perceptions of the risks of cannabis use and understand what steps, if any, they take to mitigate these risks.
Design:
Qualitative description.
Methods:
We analyzed semi-structured interviews with 52 Canadians who made the decision to start, stop, or continue using cannabis during pregnancy or lactation between 2019 and 2021. Data collection iterated with analysis. We used a conventional (inductive) approach to content analysis.
Results:
Perception of risk was found to be an essential component of decision-making about cannabis use. We identified a cycle of “risk identification,” “management,” and “observation” of effects. First, the pregnant or lactating person assesses the risks and weighs them against the perceived benefits of cannabis use. Second, they take action to minimize risks, with some choosing abstinence. Others, often those who were using cannabis to manage symptoms, continued cannabis use but devised a variety of other risk mitigation strategies such as, decreasing the amount or frequency of their use, changing the form of cannabis, and strategically timing their use with caregiving responsibilities. The final stage of the cycle involves seeking information about whether or not the initial perceived risk has manifested after implementing mitigation strategies, through observations and clinical information about the pregnancy or child.
Conclusion:
Participants consistently engaged in deliberation about the risks and benefits associated with their perinatal cannabis use. Nearly all implemented strategies intended to minimize risk. Our results highlight the need for more research to inform clear public health messaging about risk mitigation to minimize the potential harms of perinatal cannabis use. This work informs clinicians about patient-perceived risks and mitigation strategies which could in turn help inform shared decision-making conversations.
Introduction
An increasing proportion of pregnant and lactating people in Canada report using cannabis since it was legalized for recreational use in 2018.1 –4 Clinical guidelines and public health messaging consistently advise against perinatal cannabis use due to a lack of evidence supporting safety and enduring concerns about the potential for negative fetal or infant health outcomes.5 –7 Multiple studies have described the benefits that pregnant people perceive from cannabis use, and these typically relate to managing symptoms of both pre-existing and pregnancy-related conditions, with additional mention of benefit related to pleasure, an improved sense of well-being, and stress management.8 –12 Less is known about the perceived benefits of cannabis use in lactation, and mentioned reasons are similar to those in pregnancy, with the exclusion of pregnancy-related conditions, such as the control nausea and vomiting associated with pregnancy.13 –17
Specifying the risks of cannabis use during pregnancy or lactation is more difficult. Risk refers to “the potential for harm,” and perceptions of risk during pregnancy and lactation are derived from the consideration of future potential outcomes.18,19 In pregnancy and lactation, considerations of risk include both potential harms to the pregnant or lactating person and to their fetus or infant, and potentially to other children or dependents under the care of the pregnant person. Risks to the pregnant or lactating person are similar to the general risks of cannabis consumption, and include respiratory and cardiovascular disorders,20,21 cannabis hyperemesis syndrome, 22 and mental health and substance use disorders.20,23 –25 Cannabis use during pregnancy may also be associated with an elevated risk of anemia. 26
Clinical evidence about the risks to the fetus or infant associated with perinatal cannabis use is still emerging.27,28 Current literature indicates an association between cannabis use and low birth weight,26,29 neurodevelopmental, executive functioning, and psychopathology problems in childhood 30 and a potential association with preterm birth. 31 This body of research is still evolving and more well-controlled studies are required.26,29 The existing clinical evidence mainly concerns smoked cannabis; there is little evidence available about how changing the form or composition of cannabis may impact clinical outcomes.
It is known that pregnant people are often concerned about the risk cannabis poses to their fetus,15,32 and also the risks associated with substituting or replacing cannabis with another substance they may deem more harmful.10 –12,33 –36 Currently, clinical guidelines advise that pregnant and lactating people avoid cannabis use.7,6,37,38 While abstinence may be an acceptable path to many who use cannabis, there is insufficient evidence to provide clinical guidance on effective techniques for risk reduction to those who are unwilling or unable to abstain.10 –12 This may result in a complex decision that is not a binary choice between complete abstinence and unchanged continuance, but rather a negotiation of perceived benefits against the uncertainty of future risk. To further understand how pregnant and lactating people perceive the risks of cannabis and what actions they employ to mitigate those risks, we conducted a qualitative study of the risk assessment and decision-making practices of pregnant and lactating people who use cannabis.
Methods
This is a secondary qualitative descriptive39,40 analysis of the data from a larger study exploring pregnant and lactating people’s decisions surrounding cannabis use.17,41 This study was conducted in Canada, where recreational and medical cannabis use is legal for those 19 years of age or older. Consolidated criteria for reporting qualitative research (COREQ) were used in the preparation of this article. 42
Theoretical lens
Van Loon’s 18 conceptualization of risk objects was used as a sensitizing concept. 19 Sensitizing concepts are theoretical ideas which inform the researchers’ thinking about the phenomenon under study. 43 Van Loon 18 describes the idea of the “virtual object,” something that is not a hypothetical outcome, but is real in the sense that it reflects reality—it has just yet to occur. The virtual object is a way of thinking through the relationship between perception and reflection, of what is real and what is ideal. In the context of pregnancy and lactation, virtual objects may include safe birth, a healthy child, and a happy expanded family.18,19 Perceptions of risk during pregnancy and lactation are derived from the pregnant person’s thinking about how their actions might positively or negatively affect “virtual objects” in the future.18,19 This theory helped us remain alert to the different types and targets of risk in our data, and the different potential futures that participants might be considering, fearing, or hoping for.
Eligibility and recruitment
People who made the decision to start, stop, or continue using cannabis during pregnancy or lactation in the past year were recruited to participate in this study. Eligible participants were at least 19 years of age, living in Canada, and able to communicate in English. Exclusion criteria included being 18 years of age or younger, not being pregnant or lactating within the past year, or not using cannabis either during pregnancy or lactation, or in the 3 months prior to becoming pregnant. 19 years of age was chosen as an inclusion criterion because that is the legal age for cannabis use in Canada. We started with a maximum variation approach to sampling, enrolling participants with as much variation as possible in their experiential and demographic features, and then moving to purposeful sampling to select participants who have particular experiential and demographic features of analytic relevance (e.g. reason for using cannabis).44,45 Participants were recruited from advertisements in prenatal clinics, social media, and snowball sampling in which existing participants were asked to share recruitment information with their potentially eligible contacts.
Data collection
Each participant completed one semi-structured interview over Zoom conference (video or phone) between November 2020 and March 2021. Interviews were chosen to permit confidentiality and in-depth exploration of individual experience and perception. Interviews were facilitated by one of four female interviewers trained in qualitative research employed as research assistants or the faculty principal investigator (A.P., J.P., M.V., and S.T.). Interviewers had no prior relationship with the participants. Personal goals and characteristics of the interviewer were not shared with participants. Interviews ranged from 12.5 to 67 min long, and field notes were taken after the interviews, when the discussion or circumstances prompted interviewer reflection. All interviews were recorded, transcribed verbatim, and were not reviewed by participants. We interviewed participants past the point of concept saturation, which we defined as new data not offering any new, theoretically relevant, insights. 46
The interview guide (see supplemental Appendix) was developed based on the findings from two recent systematic reviews,47,48 and the clinical and research expertise of the research team, which included a midwife, an obstetrician, and a family physician. Participants were asked about any worries they had about the effects cannabis could have on their child, and the strategies they employed to minimize risk during pregnancy and lactation.
Data analysis
Data analysis proceeded concurrently with data collection, with insights from initial data reflected for confirmation, elaboration, or refutation into future interviews in place of a formal member-checking exercise. The analysis of the interview transcripts was split between four researchers (A.P., J.P., M.V., and S.T.) who took part in an inductive approach to conventional content analysis, 49 the preferred analytic strategy in qualitative descriptive studies. 43 Initially, the transcripts were open-coded to identify the perceived risks of using cannabis during pregnancy and lactation, mitigation strategies, and methods of observation that participants discussed. After one round of coding, analytic insights were compared among the team, and a coding framework that integrated feedback from the rest of the team was created. This coding framework was then applied and progressively refined through further rounds of coding. This coding framework provided the concepts used to generate the “Perceive-Act-Observe” cycle described in the “Results” section. NVivo 13 software was used to manage data analysis. 50
Results
Overall, 52 pregnant or lactating people participated in this study, 51 identified as women and 1 person identified as non-binary. Participants were mostly white (69%) and Indigenous (13%), although represented diversity in age, educational attainment, and geography. Participant demographic information can be found in Table 1. At the time of the interview, 30 participants were currently pregnant and 22 were lactating. Of these 52 individuals, 31 had previous children and we encouraged them to draw on their experiences with those pregnancies and their most recent pregnancy. All participants used cannabis in the 3 months prior to pregnancy, and 30 continued to use cannabis during their most recent pregnancy. Of the 33 participants who discussed lactation, 28 used cannabis during this time.
Demographic data of participants.

Participants were asked to self-identify their race or ethnicity; no categories were imposed on this self-identification.
Responses here included opioid and controlled medications (e.g. gabapentin) both with and without a prescription, and methadone during pregnancy.
Nearly all participants believed that there was risk associated with cannabis use during pregnancy or lactation. Most participants reported taking action to mitigate these perceived risks, and some described the ways in which they observed their pregnancy or child for adverse outcomes. From these data, we developed a “Perceive-Act-Observe” cycle of stages (Figure 1) wherein the pregnant/lactating person (1) formed a perception of the risks associated with cannabis use; (2) developed a mitigation strategy and took action to lessen the likelihood of the perceived risks manifesting; and (3) observed their pregnancy or child to determine whether the risk they anticipated manifested. This cycle may be experienced several times throughout the perinatal period and across multiple pregnancies. Renewal of the cycle can be catalyzed by new information about risk, new observations, and new reproductive stages (e.g. giving birth, new pregnancy). Key findings, organized by stage, are available in Table 2.
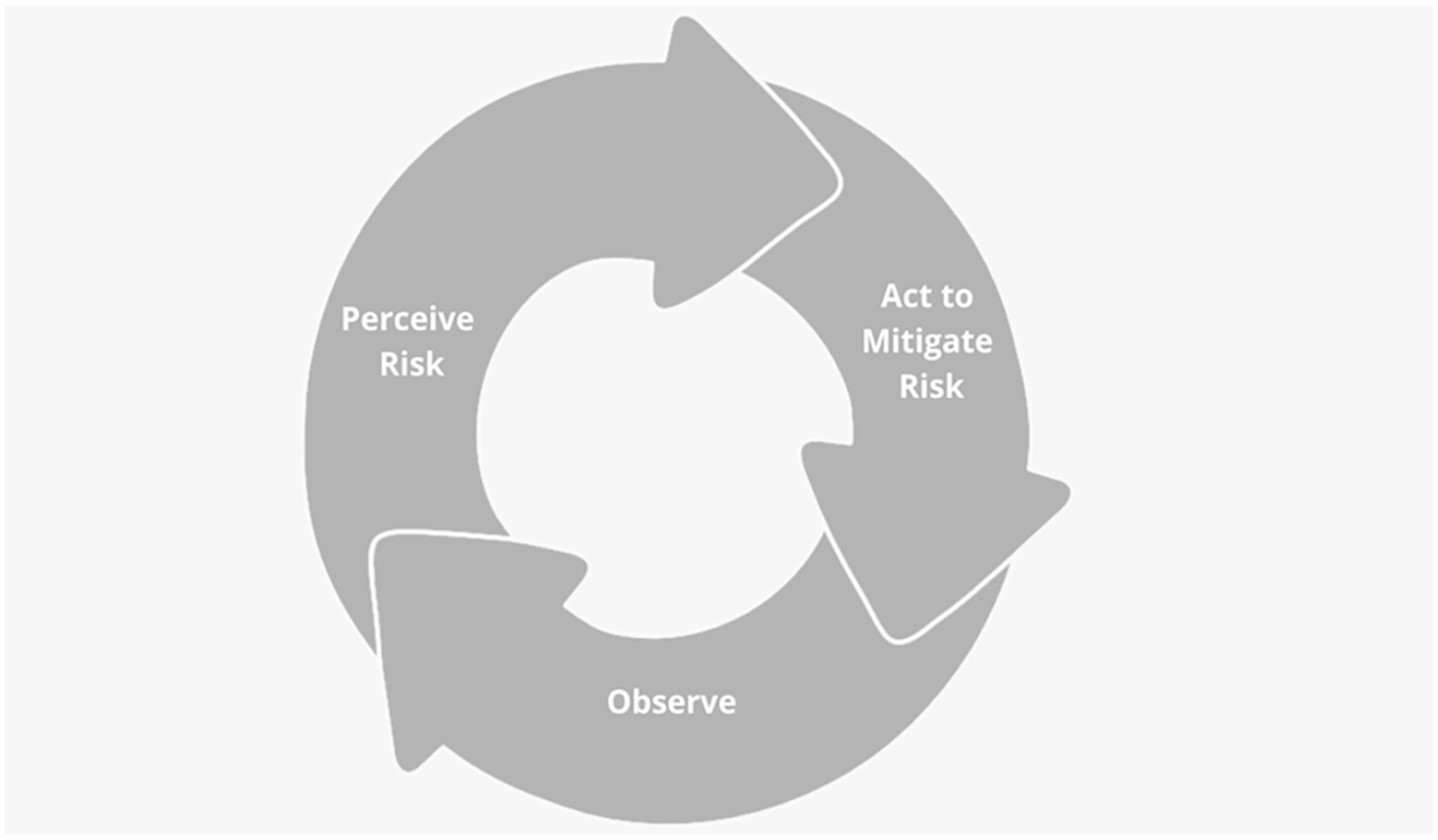
Perceive-Act-Observe cycle.
Summary of key findings about the Perceive-Act-Observe cycle with exemplar quotes.

Stage 1: perceive
Nearly all participants perceived that there were risks associated with using cannabis during both pregnancy and lactation, but few were able to articulate the specific nature of these risks. Participants also identified specific risks related to their own sobriety or state of alertness, and infant risks of exposure to secondhand cannabis smoke.
Perceptions of risk in pregnancy
While not all participants believed that cannabis consumption in pregnancy had any risk, the risks associated with cannabis use during pregnancy were commonly identified by participants, but often discussed in vague terms: “I didn’t use anything during pregnancy, because I wasn’t sure of the side effects, and I would hate for something to happen” (P35). Specific risks to their fetus or future child were occasionally identified explicitly. These specific risks included miscarriage or stillbirth, impeded lung development, low birth weight, premature birth, withdrawal symptoms in the infant, neurological, cognitive, and developmental issues, and impacts to their own or their child’s mental health.
Participants discussed risk that cannabis use during pregnancy could pose to themselves or their family members. This is illustrated by one participant who worried about the involvement of child protective services: “I wouldn’t want to risk losing my child or have [the] government involvement in my parenting” (P21). Participants also described secondary or indirect types of risk, such as when P48 discussed how cannabis use during pregnancy would cause her to experience severe anxiety due to the worry of potentially harming her child: “I felt very anxious, I felt very guilty, and the guilt overcame me to the point where I was like, you know what, I think it’s time to put the lighter down” (P48).
Perceptions of risk in lactation
Similar to pregnancy, participants expressed trepidation about risks related to cannabis use during lactation, although few specifics were provided about the nature of that risk. Participants were aware that cannabis could transfer through breastmilk: “I know that cannabinoids are fat soluble and especially when you’re breastfeeding [. . .] you know your breast milk is mostly fat, so if it’s going to come out anywhere it’s probably going to come out there” (P36). They had differing perspectives for the risk of cannabis being present in their breast milk; for some, simply knowing that cannabis is present in breast milk was enough to anticipate the potential for risks, catalyzing a move to the “Act” phase of the cycle, while others were curious about why the transfer of cannabis through breastmilk may pose a risk to the infant:
I saw [a study] that said there’s a small percentage of [cannabis] in breast milk for a long time, but what’s the bad side of that? There’s nothing that tells you like what’s the downside of that. I mean, it makes you sleepy—the baby’s got to be sleepy, it’s good for them. How does it do anything to them neurologically? (P42)
While risk associated with direct transmission was a common focus for participants, a less discussed, but still notable concern was the risks related to their child being exposed to second- or thirdhand cannabis smoke; within this, the risk of sudden infant death syndrome was a primary concern.
Some participants were not worried about cannabis use causing any direct harm to the child during lactation. Instead, they were concerned about the effect that using cannabis would have on their own sobriety or alertness and how this could indirectly affect their child’s health, as exemplified by P9 below:
There is always that little voice saying, “what if your son breaks a leg, and you need to drive to the hospital?” [. . .] That’s the thing that makes me want to be completely alert, and focused, and in my own senses to be with my son. (P9)
Stage 2: act
Risk mitigation strategies in pregnancy and lactation
While our participants highlighted an array of possible risks that could arise with cannabis use during pregnancy and lactation, many of them spoke to the benefits that they perceived from using cannabis. This led to entering a complex calculation of weighing risk and benefit to establish a mitigation strategy that would balance their own needs against potential risks to their child. Actions toward risk mitigation were present even in participants who stated that they did not perceive cannabis to pose any risk to themselves or their future child. A variety of mitigation strategies were described, including both cessation and harm reduction strategies to continue using while minimizing risk.
Cessation strategies
Among participants who decided to cease using cannabis during pregnancy, mitigating risk was the main justification given, as illustrated by P48, who wanted to do “everything that [they] could do in [their] power to make this the healthiest baby in the whole world” (P48). This view was most common among participants who used cannabis for pleasure before becoming pregnant, although was not limited to this group. Some participants who perceived a significant benefit to cannabis use were also motivated to cease their use due to potential risk.
During lactation, some participants decided to cease their use permanently or for the duration of the time they were lactating. Others discussed plans to resume using cannabis during lactation when their child was older (6 weeks to 3 months). Reasoning for this strategy included wanting to take the time to understand their child’s sleeping and feeding patterns, reducing their child’s exposure to chemicals, wanting to resume use after ending bedsharing, and worries about their infant being too small.
Harm reduction strategies
Participants highlighted a wide variety of harm reduction approaches to mitigate risk during pregnancy and lactation while continuing to use cannabis. Most commonly, participants reported employing harm reduction strategies when they perceived a therapeutic benefit from using cannabis. In both pregnancy and lactation, some participants discussed the importance of obtaining their cannabis from a trusted source to ensure optimal safety: “I mean if I don’t have any and my friend doesn’t have any, I go to the government shops and I buy there because I don’t trust anybody” (P1).
All participants who consumed cannabis during pregnancy reported reducing either the frequency or the amount of cannabis they consumed to mitigate risk: “I was smoking probably between three and four grams a day, and then I cut back to one gram because I was like, maybe I shouldn’t be giving this child so much marijuana” (P46). Strategies to mitigate risk varied among our participants. Changing the form or strain of cannabis that they were using was one strategy mentioned by some participants, but there was no consistency across participants in the forms of cannabis perceived to be safer. Others described mitigating risk by replacing smoked cannabis with oils, lotions, and bath bombs. Another strategy employed was to begin using cannabis products with higher cannabidiol (CBD) concentration, which participants understood to be the active cannabinoid associated with benefits and non-psychoactive properties: “I tend to go for the higher CBD strains now [. . .] to take the recreational aspect out of it and turn it more into the therapeutic aspect” (P41).
Participants described a variety of harm reduction strategies during lactation to mitigate risks to their child and themselves. Several participants reported strategically timing their use in relation to feeding and childcare needs. For example, using exclusively at night when their child was sleeping or ensuring their partner was ready to respond to any needs the child(ren) may have:
I use the CBD oil daily because it’s, it doesn’t have like any impairing effects. So, I’ll just use it in the morning and it kind of helps overall with general like aches and pains, but then anything that makes me like buzzed or high I will wait until you know after the kids are asleep. (P10)
Commonly, participants adopted consumption patterns to try to separate lactation and cannabis use, such as using cannabis right before or after they finished pumping or breastfeeding. The explanation offered for using cannabis right before pumping or feeding was that it would not have time to transfer to the breastmilk. Another strategy employed included using cannabis in a location in their home that was away from their child, washing their hands/body, and changing their clothes in an attempt to reduce the risk of their child coming into contact with cannabis. Participants described their partners partaking in these types of risk mitigation behaviors as well.
Stage 3: observe
The third part of the cycle describes how pregnant and lactating people gathered information about the health of their pregnancy or child to observe whether any risks manifested as a result of their cannabis use. In most cases, these observations catalyzed a renewal of the cycle.
Participants described approaching observation in a variety of ways, closely related to the types of risk they perceived, and the mitigation strategies they enacted. Participants who did not describe specific risks were likely to look for general indications of health. Not seeing any unusual or abnormal issues in their child was interpreted positively. This group tended to use relatively vague descriptors of their observations, describing their fetus or child as “okay,” “fine,” “smart,” “amazing,” “incredible,” and “healthy.” Participants who used these general conclusions also often admitted that they did not know what specific signs might indicate harm from cannabis use, as illustrated by P12: “I, honestly, have no way to find out what’s going on, but they’re both happy kids, healthy kids and no real issues, so [trails off]” (P12).
Participants who named specific types of risk were more likely to describe looking for specific symptoms or indicators of a problem. For this group, the absence of the symptom they had in mind indicated to them that their child was not affected by cannabis, as highlighted in this example from a participant who perceived asthma and preterm birth as the risks of cannabis use: “They say it causes asthma. My oldest daughter doesn’t have asthma. . . . Nobody was premature, everyone was overdue” (P43). While participants commonly relied on their own observations, others used information gathered from routine clinical appointments, particularly during pregnancy when it was difficult to make direct observations of their fetus: “After we went for the first ultrasound [. . .] he was right on track with growing” (P15).
Observation ceased at different points. Some participants stopped looking for the signs of harm related to cannabis after giving birth, or once they determined that the risk that they were concerned about did not manifest in their child. Other participants saw the process of observing their child after using cannabis as ongoing, due to the lack of information on the long-term effects:
I mean, my daughter is healthy and happy and by all measures kind of developing normally. But like I don’t- I imagine it won’t be until she’s like a fully grown adult that I will ever stop questioning whether or not that’s [cannabis use] had an impact. (P16)
Observations and perceptions of risk: continuing the cycle
The information obtained from observation was described as important for decision-making, and several participants demonstrated perceptions of risk that evolved over time. For example, participants who had used cannabis in previous pregnancies and did not observe detrimental effects described this as influential to their decision to use cannabis in their current and future pregnancies:
I noticed very little difference between the two kids, like the one that had cannabis exposure during breastfeeding, the one that doesn’t—they’re pretty much on par with each other. That’s kind of how I guess I got the confidence to go ahead with the decision [to use cannabis]. (P33)
Participants also, at times, made observations highlighting how the impact of their cannabis use on their pregnancy influenced their perceptions of risk during lactation:
I think that the harder choice would have been to use it during pregnancy. And I think at that point [after giving birth], I felt well you know I did it through my pregnancy, I have a beautiful healthy baby. I just kind of continued. (P41)
Discussion
This study examined 52 pregnant and lactating people’s perceptions of the risk associated with perinatal cannabis use. Most participants perceived that cannabis use posed some risk, direct or indirect, to their fetus or newborn. Despite the ubiquity of this concern, few were able to articulate specific risks of perinatal cannabis consumption. However, even without the identification of specific risks, all took some type of action to mitigate the possibility of harm caused by cannabis use. They then observed their pregnancy or child to monitor for the manifestation of perceived risks and adjusted their actions according to these observations.
Previous studies have found that most people who continue to use cannabis in pregnancy perceive little or no risk.10,32,51 –53 The ubiquity of risk perception in our sample is therefore striking, as very few participants indicated that they perceived “no risk” and even those who described this viewpoint still chose to employ risk mitigation strategies. There was a notable difference between the participants’ understanding of risk during pregnancy versus during lactation. Most participants discussed pregnancy-related harms, and fewer identified cannabis as posing a direct risk to a breastfed infant. This difference in understanding is reflective of the available clinical evidence, with numerous studies investigating specific risks during pregnancy, but limited research on risk during lactation.26 –28
Our study is also novel in its description of the risk mitigation strategies established by perinatal cannabis users. We could not identify any description of this type of harm reduction behavior in recent systematic reviews and other literature.3,48,54 In our study, most participants created behavioral strategies to mitigate risk, regardless of what types of risk they perceived. These strategies included ceasing use, or changing the timing, amount, dose, or form of cannabis used. Sometimes these strategies involved support and help from partners, which may be an important area for future research.
In the creation of these risk mitigation strategies, participants drew comparisons to harm reduction messaging about other substances, such as avoiding exposure to secondhand cigarette smoke by smoking outdoors, 55 or staging consumption of alcohol after breastfeeding, or pumping milk prior to alcohol intake to have available to feed the baby before drinking alcohol.56,57 Several remarked that they wished there was more information available to help them mitigate the risk of cannabis, similar to those which exist for substances, such as alcohol and cocaine.35,38,58,59 There is a gap in the literature to support these requests for information. We did not find any harm reduction guidelines in the literature to help mitigate the risk of perinatal cannabis use. Current recommendations emphasize cessation or substitution with few to no acknowledgements of the perceived benefits or reasons persons might use cannabis during pregnancy or lactation.37,38,60
Both perceived risk and mitigation strategies reflected the participants’ personal experiences, anecdotal evidence, and interpretations of science. Many participants drew on personal experiences and anecdotes when they described their perceptions of risk. This may not only reflect a lack of other forms of information and evidence but also demonstrate thoughtful deliberation about how to balance risk and benefit of cannabis use. Several studies have documented the perceived benefits of cannabis from the perspective of pregnant people,10 –12,34,36,61 –63 although there is little evidence about the perceived benefits of cannabis use during lactation.17,48 Further developing the evidence on motivations for cannabis use during lactation is an important area for future research. Our data indicate that pregnant and lactating people are likely to be receptive to clear information about risk as they were motivated to make significant behavioral change to mitigate the risk of their cannabis use. This resonates with the findings from other studies demonstrating that pregnancy is often a time when people are motivated to enact positive health-related behavior change.64 –66
While many participants discussed looking for signs that cannabis use was affecting the health or functioning of their pregnancy or infant, no participants mentioned observing or perceiving negative impacts of cannabis either in their current or previous pregnancy. This may represent confirmation bias, as all participants who continued to use cannabis during pregnancy or lactation expressed clear reasons and a strong desire to do so. Clinical evidence indicates that we may expect some prenatally exposed children to have a low birth weight, be born before term, or exhibit neurodevelopmental and behavioral challenges in childhood.26,29 –31 However, few participants were able to specify the risks they anticipated, and so they may not associate outcomes such as low birth weight with their cannabis use, especially if the child grew well after birth and was a typically developing infant. When participants reported not observing any impact, this may represent a focus on other aspects of pregnancy or infant development, such as a normal anatomical scan, positive reports from clinicians that the pregnancy is progressing well, typical weight gain after birth, or meeting expected infant development milestones.
Strengths and limitations
The open-ended nature of the interviews in this study was a strength, as was independence from participants’ perinatal health care providers and institutions, to whom they may be more reluctant to disclose stigmatized behaviors. This allowed for in-depth discussion of risk perception and strategies for mitigation. This might account for the differences in findings between this study and surveys of people who use cannabis during pregnancy and do not perceive risk to this use.10,32,51,52 However, interview-based studies are also prone to volunteer and social desirability bias. Our sample may overrepresent people who self-selected due to their thoughtful deliberation about cannabis use and perception of therapeutic benefit. Although qualitative research does not strive to achieve representation, understanding the particularities of the sample is important for considering the transferability of findings. Participants in this study were mostly white (69%), although this is similar to the general Canadian population, in which 70% identify as white. Among non-white participants, Indigenous persons were overrepresented in this study and other groups (e.g. South Asian, East Asian) were underrepresented.67 –69 Participants exhibited a range of education attainment, with 70% attaining “tertiary” education, defined as achieving a college or university degree. This is similar to the general Canadian population, where in 2022, 76% of women aged 25–34 years have achieved tertiary education. 70 The aim of qualitative research is not to provide evidence on clinical outcomes, and representative sampling is not employed. Accordingly, we did not systematically collect clinical data on outcomes of participant pregnancies, although many participants shared this information in the course of providing information about their experiences pertaining to decision-making about cannabis use. Where relevant, outcome information is incorporated in this way. In addition, interviews were only offered in English, excluding potential participants who do not speak this language. These results may not be readily transferable to groups with different educational attainment, linguistic backgrounds, or different ethnocultural traditions and understandings of pregnancy and parenthood. This study was also conducted in a socio-historical context where cannabis is legal and readily available through regulated retailers, and where substance use during pregnancy, while stigmatized, is not legally considered child abuse. Therefore, the findings may not be transferable to contexts where cannabis is criminalized or where fetuses are considered to have personhood rights.
Conclusion
This qualitative study of 52 people who made decisions about cannabis use during pregnancy or lactation indicates that cannabis use during the perinatal period is related to perceptions of important benefits from cannabis, despite the conflicting perception that cannabis use poses risks to the health of their fetus and child. When making decisions about perinatal cannabis use, many pregnant and lactating people resist a binary decision of abstinence versus continued use. Instead, they make changes to the frequency, amount, and form of cannabis they use to mitigate risk. These risk mitigation efforts are self-developed and point to the need for more research on specific risks of consuming cannabis during pregnancy and breastfeeding to inform evidence-based harm reduction strategies directly related to these specific risks. Prioritizing research in this area will determine whether other ways to minimize risk outside of abstinence are possible. This work may also provide clinicians with a greater understanding of patient-perceived risks and mitigation strategies which could in turn help inform shared decision-making conversations. Equipping clinicians with this knowledge may also lead to cannabis users being more comfortable with engaging in these discussions with their healthcare providers.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231202406 – Supplemental material for Pregnant and lactating people’s strategies to mitigate the risk of cannabis consumption
Supplemental material, sj-docx-1-whe-10.1177_17455057231202406 for Pregnant and lactating people’s strategies to mitigate the risk of cannabis consumption by Anuoluwa Popoola, Janelle Panday, Shipra Taneja, Devon Greyson, Sarah D. McDonald, Tejal Patel, Elizabeth Darling and Meredith Vanstone in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231202406 – Supplemental material for Pregnant and lactating people’s strategies to mitigate the risk of cannabis consumption
Supplemental material, sj-docx-2-whe-10.1177_17455057231202406 for Pregnant and lactating people’s strategies to mitigate the risk of cannabis consumption by Anuoluwa Popoola, Janelle Panday, Shipra Taneja, Devon Greyson, Sarah D. McDonald, Tejal Patel, Elizabeth Darling and Meredith Vanstone in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.