
Abstract
Background:
Severe maternal morbidity and mortality are increasing in the United States with continued healthcare disparities among Non-Hispanic Black women. However, there is sparse data on the disparities of severe maternal morbidity and mortality by race/ethnicity as it relates to community type.
Objective:
To determine whether residing in rural communities increases the racial/ethnic disparities in severe maternal morbidity and mortality.
Design:
This study is a cross-sectional analysis of women admitted for delivery from 2015 to 2020. A total of 204,140 adults who self-identified as women, were admitted for delivery, who resided in Maryland, and were between the ages 15 and 54 were included in our analysis. Community type was defined as either rural or urban.
Methods:
A multivariable logistic regression, which included an interaction term between race/ethnicity and community type, was used to assess the effect of community type on the relationship between race/ethnicity and severe maternal morbidity and mortality. Data were obtained from the Maryland Health Service Cost Review Commission database. The primary outcome was a composite, binary variable of severe maternal morbidity and mortality. Exposures of interest were residence in either rural or urban counties in Maryland and race/ethnicity.
Results:
Our study found that after adjusting for confounders, odds of severe maternal morbidity and mortality were 65% higher in Non-Hispanic Black women (odds ratio 1.65, 95% confidence interval: 1.46–1.88, p < 0.001) and 54% higher in Non-Hispanic Asian women (odds ratio 1.54, 95% confidence interval: 1.24–1.90, p < 0.001) compared to Non-Hispanic White women. The interaction term used to determine whether community type modified the relationship between race/ethnicity and severe maternal morbidity and mortality was not statistically significant for any race/ethnicity (Non-Hispanic Black women, p = 0.60; Non-Hispanic Asian women, p = 0.91; Hispanic women, p = 0.15; Other/Unknown race/ethnicity, p = 0.54).
Conclusion:
Although our study confirmed the known disparities in maternal outcomes by race/ethnicity, we found that residing in rural communities did not increase racial/ethnic disparities.
Introduction
Maternal mortality in high resource countries has been declining yet continues to rise in the United States. 1 In 2019, 754 women died of maternal causes and that number rose to 861 in 2020. 2 When compared to high-income countries, in 2020, the maternal mortality ratio in the United States was 23.8 per 100,000 live births, whereas it was 12 in other high-income countries. 3 In addition to the higher incidence of maternal mortality, there is also notable disparities between races/ethnicities when looking at maternal mortality in the United States. Data from 2007 to 2016 in the United States show that Non-Hispanic Black and American Indian/Alaska Native women experienced higher incidences of pregnancy-related mortality than other racial/ethnic groups. 4 Studies have shown that patients of a racial/ethnic group other than Non-Hispanic White are also more likely to deliver at hospitals with higher rates of adverse maternal outcomes, and to receive lower quality of care than Non-Hispanic White patients at the same institution.5–7 Although the rise in maternal mortality can be partially attributed to an increased prevalence of pre-existing co-morbid conditions and older maternal age, disparities by race/ethnicity are also influenced by access to quality care, implicit bias, and systemic racism.1,4,8 According to the National Institutes of Health, implicit bias is defined as “a form of bias that occurs automatically and unintentionally, that nevertheless affects judgments, decisions, and behaviors.” 9 Systemic racism is a form of racism that is well ingrained into systems, such as healthcare systems, policies and laws that allow for practices to “perpetuate widespread unfair treatment and oppression of people of color, with adverse health consequences.” 10
When addressing the issue of maternal mortality, it is equally important to consider severe maternal morbidity (SMM) as they are considered “near miss” events and are among the leading causes of maternal mortality. 11 SMM is defined by the Centers for Disease Control and Prevention (CDC) as “unexpected outcomes of labor and delivery that result in significant short- or long-term consequences to a woman’s health” and can be described using 21 indicators or diagnoses. 12 Unfortunately, in addition to higher odds of mortality, Non-Hispanic Black women also have increased odds of SMM. 13
In addition to race/ethnicity, research has shown that differences in healthcare between geographic areas have been associated with higher SMM and mortality.14,15 Women residing in rural communities have limited access to healthcare due to the need to travel long distances to seek obstetric care and ongoing diminishment of the healthcare workforce. 15 In Maryland, the number of physicians per 10,000 rural county inhabitants can be as low as nearly 2, namely in St. Mary’s county. 16 In addition, women of color who live in rural communities are also subject to food insecurity, poverty, inadequate transportation, and implicit bias, among other social determinants of health.8,14 These differences in social determinants of health and the decreased access to healthcare may help to explain the increased risk of SMM and mortality in rural settings.14,15 One study demonstrated that indigenous women in the United States living in rural communities had a higher relative risk of SMM and mortality when compared to those residing in urban communities. 14 However, there are still limited studies that explore the effect that community type has on the racial/ethnic disparities seen in SMM and mortality. The objective of this study is to confirm the existence of racial/ethnic disparities in SMM and mortality and we hypothesize that residing in rural areas increases the racial/ethnic disparities seen in SMM and mortality. With this observation, public health and clinical interventions can be tailored to reducing SMM and mortality among specific racial/ethnic groups in different residential communities.
Methods
Study design
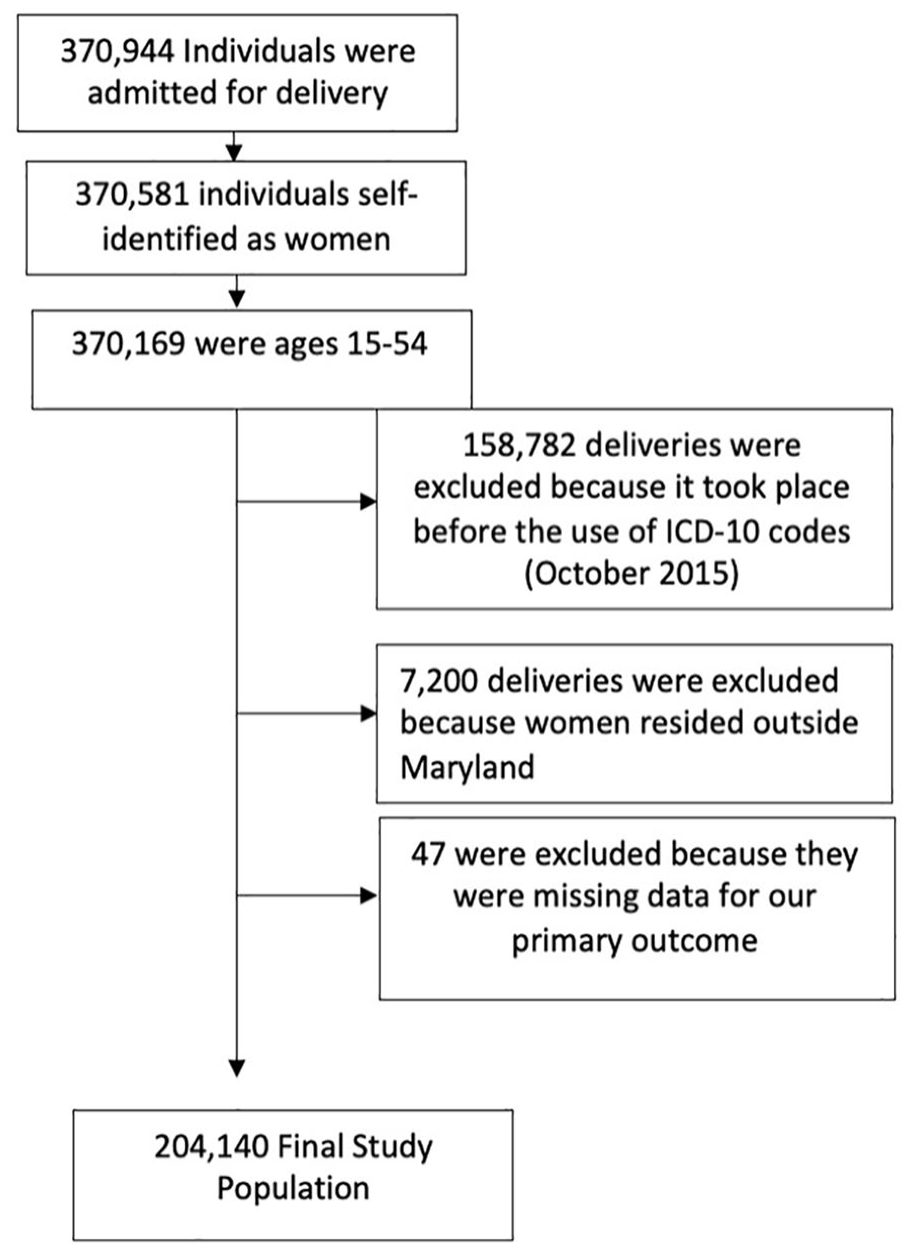
We performed a cross-sectional analysis on hospital delivery records gathered through the Maryland Health Service Cost Review Commission (HSCRC) from October 2015 to June 2020. The Maryland HSCRC is a database created to improve the quality of health and healthcare, and to reduce the cost of care for residents of Maryland. 17 In Maryland, out-of-hospital deliveries only accounted for about 2.5% of all births. 18 Our analysis therefore accounted for the majority of deliveries occurring in Maryland during that time period. Deliveries that took place prior to October 2015, before International Classification of Disease, the Tenth Edition, Clinical Modification codes (ICD-10) became available, were excluded. 19 Of those individuals who were admitted for in-hospital delivery, we included 204,140 residents of Maryland from the ages of 15 to 54 years. Ages 0–14 and 55 and above were excluded due to being outside the age of biological fecundity and outside of the age recommended for the use of obstetrics ICD-10 codes (see Figure 1). 12 Given that most current data and study findings are on women, adults who self-identified as women were included in this study. This is not to exclude individuals other than self-identifying women who this subject matter may affect, but to simply provide consistency with current data. This study was reviewed by the Johns Hopkins School of Medicine Institutional Review Board (IRB) and was classified as exempt from continuing IRB review under the DHHS regulation 45 CFR 46.101(b)(4), which allows exemption for publicly available data or data that are de-identified in some manner. A waiver of consent was granted based on the following criteria: the study involves very minimal risk to human subjects, the waiver will not have an adverse effect on subjects, and this study could not be conducted without the waiver. The IRB number is IRB00082345. This study also utilized The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.
Study population.
Race/ethnicity was our main predictor and was defined within the database based on self-reported information. 17 Multi-racial as well as races/ethnicities other than Non-Hispanic White, Non-Hispanic Black, Non-Hispanic Asian, and Hispanic were included in an Other/Unknown category to ensure that most patients were captured.
Community type was used to determine effect modification. It was a binary variable defined by counties. Rural communities were defined based on 18 jurisdiction recognized by the State of Maryland and defined by the Rural Maryland Council as counties that “share common characteristics that set them apart from their suburban and urban counterparts, such as geographic isolation, lack of transportation, and lack of access to and availability of health care.” 20 The counties were: Allegany, Calvert, Caroline, Carroll, Cecil, Charles, Dorchester, Frederick, Garrett, Harford, Kent, Queen Anne’s, Somerset, St. Mary’s, Talbot, Washington, Wicomico, and Worcester. The remaining counties were deemed urban communities, which included suburban areas as well. 20
The main outcome of interest was a binary, composite variable comprising indicators (or defining diagnoses) that are classified as SMM and also included mortality. SMM was defined according to criteria established by the CDC and the variables were generated by using recommended ICD-10 codes. It is defined as having any of the following 21 indicators in the peripartum period: acute myocardial infarction, aneurysm, acute renal failure, adult respiratory distress syndrome, amniotic fluid embolism, blood products transfusion, cardiac arrest/ventricular fibrillation, conversion of cardiac rhythm, disseminated intravascular coagulation (DIC), eclampsia, heart failure/arrest during surgery/procedure, puerperal cerebrovascular disorders, pulmonary edema/acute heart failure, severe anesthesia complications, sepsis, shock, sickle cell disease with crisis, air and thrombotic embolism, hysterectomy, temporary tracheostomy, and ventilation. 12 The peripartum period in our study, given the information provided by the database, was the time in which the woman was hospitalized. This could include any length of time in the antepartum, intrapartum, and postpartum period. Because the units of blood transfused were not included in the database, blood transfusion was excluded as one of our indicators of SMM, hence 20 indicators. Some data have shown routine transfusion of one unit of blood preventatively, whereas two units or more may be used in the case of a postpartum hemorrhage—defined by American College of Obstetrics and Gynecology as a blood loss of one liter or more or clinical signs of hypovolemia. The exclusion of blood transfusion is to avoid over estimation of SMM and some data have also begun to report SMM with and without blood transfusion as a result.21,22 Mortality, another component of our composite variable, was defined by patient disposition at discharge.
Covariates
Age was included in the database as a categorical variable binned in 5-year intervals. Primary payers were defined by the Maryland HSCRC as Medicaid, Private, Self-Pay, and Other—which included Medicare. Comorbidities and cesarean delivery were identified and included as covariates as they were identified as increasing the risk of SMM and mortality a priori. 23 The comorbidities included the following: diabetes, hypertension, obesity, chronic respiratory disease, chronic renal disease, chronic heart disease, HIV/AIDS, substance use disorder (i.e. tobacco use and substance abuse disorders), depression, hypertensive disorders of pregnancy (which includes preeclampsia and gestational hypertension), and gestational diabetes. The diagnosis and procedure codes used to define these covariates were based on the multiple sources: the codes used to generate Elixhauser Comorbidity Index scores, a study looking at hypertensive disorders of pregnancy by Fingar et al., 24 a study by Admon et al. 25 looking at comorbidities in pregnancy, Current Procedural Terminology (CPT) codes and ICD10Data.com—to find ICD-10 or convert ICD-9 codes.26–28
Statistical analysis
We performed descriptive analyses on our categorical demographic and clinical characteristics data. Pearson’s chi-square or Fisher’s exact tests were used to assess unadjusted differences by race/ethnicity for categorical covariates. Based on Centers of Medicare and Medicaid Services (CMS), any value between 1 and 10 were not reported in order to ensure confidentiality. 29
Multivariable logistic regression models were used to assess the effect of community type on the relationship between race/ethnicity and the binary outcome of having at least one indicator of SMM and/or mortality. Our first and main model used race/ethnicity as the primary predictor to assess disparities in SMM and/or mortality when comparing races/ethnicities to non-Hispanic White women—reference group. To test whether any of the racial/ethnic disparities in SMM and/or mortality varied by community type, we ran two additional models that were modifications of our main model: one was a stratification of the main model by community type—in order to provide odds ratios (ORs) of SMM and/or mortality comparing each race/ethnic group to Non-Hispanic White women in urban communities and ORs of SMM and/or mortality comparing each race/ethnic group to Non-Hispanic White women in rural communities—and another model added an interaction term (race/ethnicity and community type) to our main model —to assess whether community type serves as an effect modifier. The interaction model included race/ethnicity, community type, and their interaction. All models were adjusted for using the aforementioned confounding variables (i.e. age category, payer, comorbidities, cesarean delivery).23–27 Measures of association were expressed as OR, as mentioned. We used an alpha level of 0.05 for both bivariate descriptive analyses as well as all logistic regression models, including the interaction term. All data, except the post hoc power analysis, were analyzed using Stata version 15.1 (StataCorp, College Station, TX). Post hoc power analysis was conducted using ClinCalc Statistical software (version © 2023- ClinCalc LLC, clincalc.com). 30
Results
This study included 204,140 women from Maryland who were admitted for delivery from October 2015 to June 2020. Non-Hispanic White women made up 41%, Non-Hispanic Black women made up 27%, Non-Hispanic Asian women made up 7%, Hispanic women were 19%, and women of Other/Unknown races/ethnicities made up 5% of the women in our study (see Table 1). Most women who were seen for delivery ranged from ages 20 to 34 (74%, see Table 1), with Non-Hispanic Asian women having the largest percentage of women in the 30–34 age range (42%, see Table 1). Non-Hispanic White and Non-Hispanic Asian women mainly had private insurance as their primary payer (72% and 74%, respectively, see Table 1), whereas the majority of Hispanic and Non-Hispanic Black women used Medicaid as their primary payer (73% and 53%, respectively, see Table 1). Of all racial/ethnic groups, Non-Hispanic Black women had the highest prevalence of pre-existing diabetes, pre-existing hypertension, obesity, HIV/AIDS, chronic respiratory disease, and pre-eclampsia (see Table 1), Non-Hispanic Asian women had the highest prevalence of gestational diabetes (17%, see Table 1). Non-Hispanic White women had the highest prevalence of tobacco users and those with substance use disorders (13% and 4%, respectively, see Table 1). Depression was also most prevalent among Non-Hispanic White women (7%, see Table 1). Finally, Non-Hispanic Black women had the highest incidence of cesarean section deliveries compared to all racial/ethnic groups (37%, see Table 1).
Demographics and clinical characteristics by race/ethnicity.

In compliance with Center of Medicare and Medicaid Services (CMS) cell size suppression policy, values in certain cells were too low to report, hence the absence of value(s) in certain cells.
Women who had at least one indicator of SMM or mortality made up 0.8% (1575) of our study population. Given the low incidence of certain indicators of SMM and mortality, multiple values in certain categories were not reported. Non-Hispanic Black women had a high proportion of the overall incidence of the indicators that were reported, namely DIC, acute renal failure, and shock (see Table 2). The three indicators of SMM with the highest incidence were DIC, eclampsia, and acute renal failure (n = 325, n = 309, n = 285, respectively, see Table 2). The total in-hospital maternal deaths were less than 11 and were, therefore, not reported.
Clinical characteristics by race/ethnicity.

In compliance with Center of Medicare and Medicaid Services (CMS) cell size suppression policy, values in certain cells were too low to report, hence the absence of value(s) in certain cells.
The main logistic regression model, unadjusted, shows a higher OR of SMM and/or mortality among Non-Hispanic Black women (OR 1.89, 95% confidence interval (CI): 1.68–2.13, p < 0.001, see Table 3) when compared to non-Hispanic White women. In addition, there is a higher OR of SMM and/or mortality, when unadjusted, among Non-Hispanic Asian women (OR 1.24, 95% CI: 1.01–1.53, p = 0.04, see Table 3), when compared to non-Hispanic White women. After adjusting for demographic factors and clinical characteristics, Non-Hispanic Black and Non-Hispanic Asian women had higher odds of SMM and/or mortality than Non-Hispanic White women (OR 1.65, 95% CI: 1.46–1.88, p < 0.001, and OR 1.54, 95% CI: 1.24–1.90, p < 0.001, respectively; see Table 3). In this adjusted model, the covariates that were statistically significant were ages 25–29 and 30–34, Other payer type, pre-existing diabetes, pre-existing hypertension, hypertension of pregnancy, depression, substance use, cesarean section, chronic renal disease, and chronic respiratory disease. When looking at whether or not community type modified the OR of SMM and/or mortality in non-White racial/ethnic groups compared to non-Hispanic White women, the p-values for our interaction term in the adjusted interaction model were greater than 0.05 and was therefore not statistically significant. (Non-Hispanic Black women, p = 0.60; Non-Hispanic Asian women, p = 0.91; Hispanic women, p = 0.15; Other/Unknown race/ethnicity, p = 0.54, see Table 3).
Odds ratios of severe maternal morbidity and mortality by race/ethnicity by community type.

Adjusted models were adjusted for age, insurance payer, pre-existing diabetes, pre-existing hypertension, gestational diabetes, hypertensive disorders of pregnancy, obesity, cesarean section, substance use disorder, tobacco use, depression, chronic renal disease, chronic respiratory disease, chronic heart disease, and HIV/AIDs.
OR: odds ratio; CI: confidence interval.
Discussion
Principal findings
Given that there are known relationships between both rural communities and race/ethnicity with maternal outcomes, we designed this study to investigate if residing in rural communities increased the racial/ethnic disparities in SMM and mortality in Maryland. Our study showed that though there was a significantly higher odds of SMM and mortality for Non-Hispanic Black and Non-Hispanic Asian women when compared to Non-Hispanic White women, residing in rural communities did not increase the racial/ethnic disparity. Regardless of known and perceived barriers that may exist when living in a rural community, race/ethnicity plays a major role in SMM and mortality as seen in previous studies.4,11,13,14,31–36
Findings in the context of existing literature
Although the increased odds of SMM and mortality among Non-Hispanic Black women is well-established, our study also adds to the minimal but growing data that show increased odds of SMM and mortality among Non-Hispanic Asian women when compared to Non-Hispanic White women. Parchem et al. designed a study looking at both adverse neonatal and maternal outcomes. The study found an increased relative risk of admission to intensive care unit (ICU), uterine rupture, and unplanned hysterectomy when comparing Non-Hispanic Asian women to Non-Hispanic White women. 34 Another study by Siddiqui et al. 35 shows that despite adjusting for factors known to increase maternal mortality, Non-Hispanic Asian American and Pacific Islander women had higher odds of maternal mortality during hospitalization. Finally, a study conducted by Wagner et al. 36 showed an increased relative risk of adverse maternal outcomes among specific Non-Hispanic Asian ethnic subgroups when compared to Non-Hispanic White women. Our study shows that community type, largely differing in access to care, does not modify the relationship between race/ethnicity and adverse maternal outcomes. In order to rectify such disparity, more research is needed to investigate the nuances that explain the differences in outcomes between and within racial/ethnic groups.
To address racial disparities in adverse maternal outcomes, Hill et al. 33 recommends exploring the social conditions that may differ between Non-Hispanic Black women, for example, and their Non-Hispanic White counterparts. In addition to addressing poverty, access to prenatal care, and optimizing health before and between pregnancies, the authors suggest addressing racial inequity through implicit bias trainings and diversifying the healthcare workforce to further address existing structural racism. 33
In our cohort, most women who identified as racial/ethnic minorities also used Medicaid as their primary insurance payer. Medicaid coverage, however, typically ends 60 days postpartum and does not factor in the required follow-up for those with SMM at delivery or readmission. 37 In a report by the CDC looking at pregnancy-related death from 2011 to 2015, it was noted that a greater incidence of maternal deaths among Non-Hispanic Black women occurred in the 43–365 days after delivery when compared to the incidence of death among Non-Hispanic White women in that same time period. 34 The option—for which Maryland has opted into—to expand postpartum care for up to 12 months under Medicaid through The American Rescue Plan Act of 2021 may, therefore, help to reduce SMM and mortality occurring in the first year after delivery.37,38 This initiative is a step in the right direction toward not only reducing overall maternal mortality, but also reducing racial disparities seen in adverse maternal outcomes.
In a post hoc analysis, we ran a logistic regression model looking at community type as a main predictor with the main outcome of interest remaining SMM and mortality, however the ORs were not statistically significant.
Strengths and limitations
Our study encompasses a diverse population in the state of Maryland, however, it may not be generalizable to other states or to the United States as a whole. Although 54% of live births in Maryland from 2010 to 2017 were that of Non-Hispanic White women, more than 50% of women who died of pregnancy-related causes were Non-Hispanic Black women and 28% were Non-Hispanic White women. 39 This discordance is stark and required exploration. Finally, our analysis uses a large database and accounts for SMM, race/ethnicity, and community type; a subject matter that has been minimally studied.
In terms of limitations, our study only looked at in-hospital mortality based on the HSCRC data availability, which was an inherent limitation, and therefore we could not examine mortality within 12 months of delivery. Second, our study used ICD-10 codes, which resulted in the exclusion of patients in the database prior to October 2015. 19 Second, given the use of data that include Medicare and Medicaid patients in the setting of a rare outcome, values were not able to be reported without jeopardizing the confidentiality of patient information. Third, using county as a means of distinguishing community type was a drawback considering that counties are heterogeneous in their distribution of residential populations. In addition, Maryland HSCRC is a smaller database as compared to national databases, as a result a post hoc power analysis was conducted and only showed a power level of 100% when comparing SMM and mortality in Non-Hispanic Black women to Non-Hispanic White women. However, the power level when comparing Non-Hispanic Asian, Hispanic, and women of Other/Unknown race/ethnicities to non-Hispanic White women was 54%, 37%, and 8%, respectively. Our analysis is, therefore, likely underpowered given the smaller sample size as the cohort was broken down into racial/ethnic groups. We especially had a small incidence of mortality, however, given that SMM often is the cause of maternal mortality, it was not excluded from our analysis, similar to the small incidences of certain indicators of SMM. Future studies using a larger database may be better suited to determine if the disparity in SMM and mortality increases when one resides in a rural community when compared to urban communities. Finally, our database did not include data about those who may have previously resided in a rural community and moved to an urban county or vice versa.
Conclusion
In our study, we demonstrate disparity in SMM and mortality by race/ethnicity among women who were seen for delivery in Maryland; however, this relationship was not modified by community type, as noted by the statistically insignificant p-values. Non-Hispanic Asian and Non-Hispanic Black women showed an increased odds of SMM and mortality when compared to Non-Hispanic White women. Seeing as access to care or the lack thereof—defined by residing in either urban or rural communities—does not statistically significantly change the racial/ethnic disparity seen in SMM and mortality, extensive research is needed to fully understand and resolve the very well-known disparity. In addition, given that there are 21 indicators of morbidity, research looking into the association between race/ethnicity and individual indicators of SMM is imperative for being able to effectively create targeted policy and hospital protocols to reduce the overall odds of adverse outcomes by race/ethnicity.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231189556 – Supplemental material for The association between severe maternal morbidity and mortality and race/ethnicity with community type in Maryland
Supplemental material, sj-docx-1-whe-10.1177_17455057231189556 for The association between severe maternal morbidity and mortality and race/ethnicity with community type in Maryland by Lorene NEA Cudjoe, Joseph K Canner, Shari M Lawson and Arthur Jason Vaught in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231189556 – Supplemental material for The association between severe maternal morbidity and mortality and race/ethnicity with community type in Maryland
Supplemental material, sj-docx-2-whe-10.1177_17455057231189556 for The association between severe maternal morbidity and mortality and race/ethnicity with community type in Maryland by Lorene NEA Cudjoe, Joseph K Canner, Shari M Lawson and Arthur Jason Vaught in Women's Health
Footnotes
Acknowledgements
We thank the entire Johns Hopkins Surgical Outcomes Research (JSCOR) program, namely all who were in the 2020–2021 cohort as well as Drs. Elliot Haut and Caitlin Hicks. We would also like to thank Dr. Saifuddin Ahmed and Mrs. Shannon Murphy for all their assistance and support.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.