
Abstract
Maternal mortality is rising in the USA. The pregnancy-related maternal mortality ratio increased from 10/100,000 to 17/100,000 live births from the 1990s to 2012. A large proportion of maternal deaths are preventable. This review highlights a national approach to reduce maternal death and morbidity and discusses multiple efforts to reduce maternal morbidity, death and improve obstetric safety. These efforts include communication and collaboration between all stake holders involved in perinatal health, creation of national bundles addressing key maternal care areas such as hemorrhage management, call for all obstetric hospitals to review and analyze all cases of severe maternal morbidity, and access to contraception. Implementation of interventions based on these efforts is a national imperative to improve obstetric safety.
Keywords
Maternal mortality in the USA, after a dramatic fall from 900s/100,000 live births in the early 1900s, largely due to the advent of antibiotics, plateaued at 8–10/100,000 from 1980 until the late 1990s at which point maternal mortality rose [1–4]. Worldwide between 1990 and 2013 maternal mortality decreased in nearly every country, except the USA, where it increased by 1.7% [5]. In a country that spends more on healthcare dollars than most countries this rise is particularly unacceptable. Understanding the causes of these deaths as well as the preventable factors has become a national imperative.
Historical perspective of US maternal mortality
Historically and internationally maternal mortality was measured using the maternal mortality ratio defined as any maternal death during pregnancy or up to 6 weeks postpartum per 100,000 live births and this remains the World Health Organization metric. However, in an attempt to capture and analyze more pregnancy-related deaths, in 1987 the Centers for Disease Control and Prevention with the American College of Obstetricians and Gynecologists created the Pregnancy-Related Mortality Surveillance System [6,7]. For this system, the pregnancy-related maternal mortality ratio was developed and defined as maternal death within 1 year of pregnancy from pregnancy-related complications per 100,000 live births. Deaths were considered pregnancy related if they were deemed due to complications of pregnancy, a chain of events initiated by pregnancy, or pregnancy aggravation of an already existing disease or event [7]. The purpose of this change in focus was to collect data on more pregnancy-related deaths and better understand and ultimately reduce such deaths in the USA. In 1990s the pregnancy-related maternal mortality ratio was 10/100,000 live births and in 2012 it is 17/100,000. This translates into approximately 600 deaths per year in the USA. Fortunately, the actual number of deaths is a small number, however this low number makes it difficult to meaningfully study the etiology and preventability of the deaths and hence develop interventions to reduce maternal mortality. However, we do know some basic facts. The top three causes of maternal death have been consistently hemorrhage, hypertensive disease and thrombosis until recently when cardiovascular disease has become a leading cause of maternal death [1,8] (Figure 1; modified from [1]). We know that there is a persistent and disturbing disparity in maternal morbidity and mortality with African American women having a fourfold higher mortality compared with Caucasian or Asian or Hispanic women [1,9]. And, we know that a large proportion of maternal deaths are likely preventable [10–13]. Further, we know that preventability is related to causes of death. For example, 93% deaths due to hemorrhage, 60% deaths due to hypertension and 40% deaths from cardiovascular disease were deemed preventable [10]. Although interesting and important, these descriptive characteristics are neither new information nor have they led to a reduction in maternal deaths.
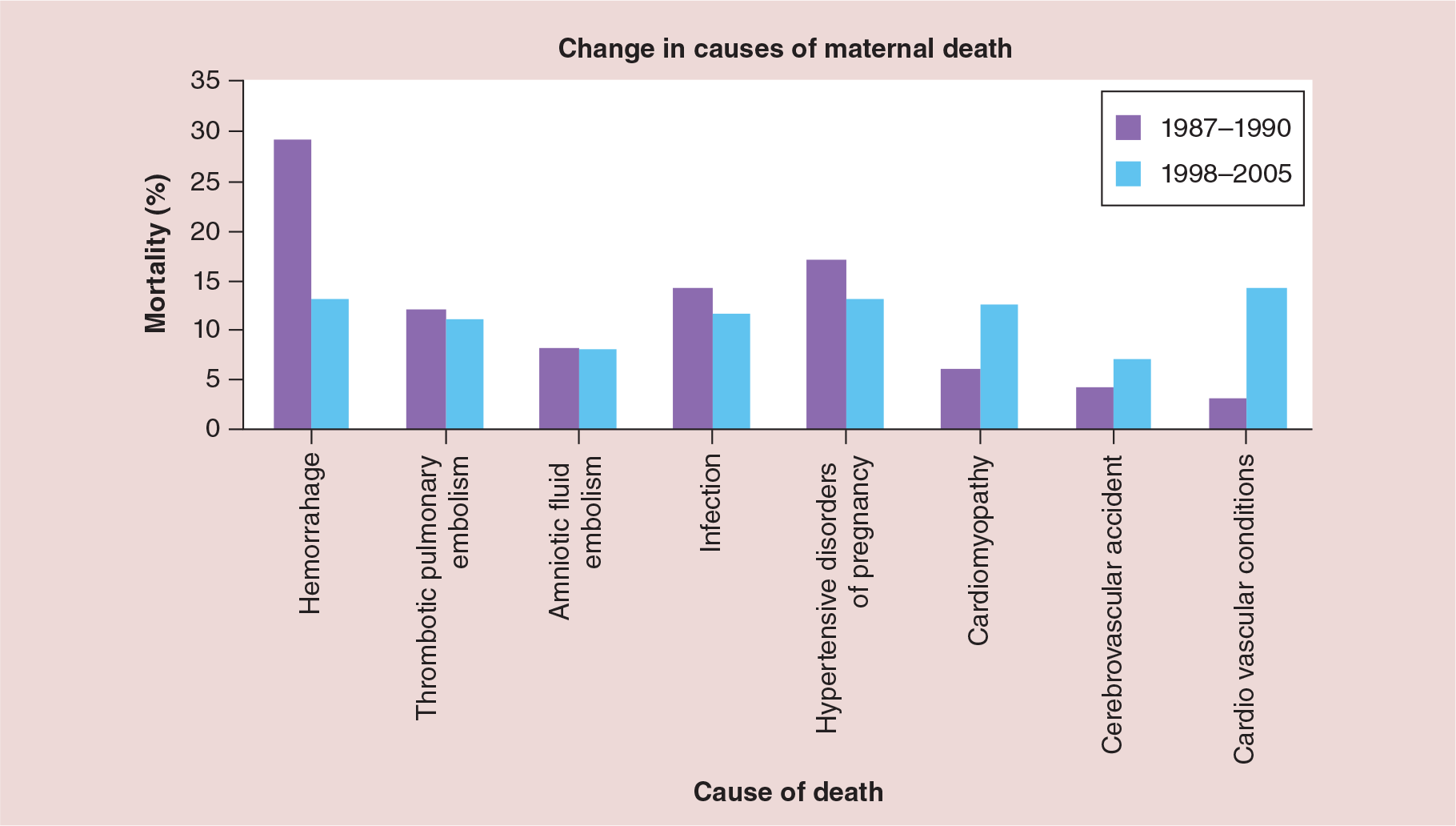
Change in causes of maternal death.
Approach to prevention of maternal mortality: severe maternal morbidity
To better understand how to reduce maternal death, it is important to consider death in the context of a continuum of maternal health from wellness to morbidity to severe morbidity to death [14]. Presumably, women who die move through this continuum, and thus the question is, can progression from wellness to severe maternal morbidity to death be reduced to result in improved maternal outcomes. It is well accepted that far more women have severe morbidity than die in pregnancy. In fact, several studies have estimated that severe maternal morbidity may occur at a rate of 0.5–1.3% of pregnancies accounting for up to 50,000 women per year in the USA [15,16]. Severe maternal morbidity was identified by using ICD-9 codes including codes for acute renal failure, cardiac arrest, sepsis, shock, disseminated intravascular coagulation, myocardial infarction, transfusion, ventilation, pulmonary edema and eclampsia. More evidence that severe maternal morbidity is on the continuum to maternal death is that in conjunction with an increase in maternal death in the USA, severe maternal morbidity has also increased between 1998 and 2011 from 0.6% deliveries to 1.6% [16]. If women with severe maternal morbidity have similar characteristics as women who die, then evaluating women with severe morbidity to understand their disease process, presence of preventable factors and outcomes should result in data useful in reducing morbidity and progression to death.
Early studies used the concept of near miss to define women that were extremely sick but did not die and asked whether these women had similar characteristics to those who died [17,18]. Intensive care unit (ICU) admission or transfusion of four or more units of blood had a high sensitivity and specificity for identifying women with near-miss morbidity [17,19]. In one study 40% of maternal deaths and 45% of near-miss cases had preventable factors compared with only 17% of cases with less morbidity (p = 0.01), supporting the concept that there is a continuum between very sick women and women who died [14]. As with maternal deaths, provider and system preventable factors were far more common than patient preventable factors in women with near-miss morbidity [13,14]. These data are important because they begin to focus our attention in areas to be studied which could ultimately improve maternal outcomes.
Characterizing preventable maternal morbidity & mortality
Attempts to address preventability or opportunities to alter outcome in women with severe maternal morbidity have been modeled after maternal death reviews and have focused on provider, system and patient factors and asked the question would the morbidity have been less or outcome improved if some aspect of care had been different. Specific areas identified that potentially negatively affected outcomes included delayed diagnosis, delayed treatment, failure to identify high risk, incomplete/inappropriate treatment, system issues are communication, documentation, equipment, protocols and medication [20,21]. Although, the CDC has recommended since 2001 that all maternal deaths in the USA should be reviewed in order to evaluate medical and nonmedical causes, analyze and interpret findings and then act on the results still today not all states have maternal mortality committees [22,23]. In contrast, The United Kingdom has consistently reviewed all maternal deaths and, based on interpretation of their data, mandated routine thrombotic risk assessment of all pregnant women with recommendations that resulted in postpartum heparin prophylaxis for most women delivering by cesarean, to reduce thromboembolic deaths [24–26].
Specific steps to reduce maternal mortality & morbidity
The coalescence of the awareness of increasing maternal mortality and severe morbidity, acceptance that a high percentage of maternal morbidity and mortality is likely preventable, recognition that other countries were decreasing their maternal mortality, patient safety principals and that meaningful assessment of care must be multidisciplinary and focused on system as well as provider factors, resulted in a national call to seriously address maternal care and outcomes. Two recent pivotal papers made the call to action: “Put the M (maternal) back into MFM (maternal fetal medicine)” [27,28]. These calls to action stimulated multiple multidisciplinary, inclusive activities which resulted in the efforts listed below intended to improve maternal care and reduce severe maternal morbidity and mortality.
Communication and collaboration between all stake holders involved in perinatal health.
– Multiple national organizations were represented at meetings held in 2012–2013 to build consensus around improving maternal care and outcomes. These meetings resulted in alignment to reduce maternal morbidity and mortality and The National Partnership for Maternal Safety and the Council on Patient Safety in Women's Healthcare were created to bring together organizations interested in maternal outcomes [28,29]. The breadth of participants in the Council of Patient Safety in Women's Healthcare is impressive and currently includes American College of Obstetrics and Gynecology (ACOG), Society for Maternal Fetal Medicine, American College of Nurse Midwives, Association of Women's Health, Obstetric, and Neonatal Nurses, Society of Obstetric Anesthesia and Perinatology, National Association of Nurse Practitioners in Women's Health and Academy of Family Physicians. The full listing is on their website for the Council on Patient Safety in Women's Healthcare [30]. The website contains educational items, bundles, forms for severe maternal morbidity review and other updates are ongoing national efforts to reduce maternal morbidity.
Creation of national guidelines or bundles addressing key maternal care areas.
– Although ACOG for years has provided practice bulletins, committee opinions on obstetric care and health, these have not consistently been multidisciplinary nor specific guidelines. Maternal care is complex and often multiple disciplines are involved not only in high-risk care but also in low-risk care. Thus, the broad inclusion of multidisciplinary providers is crucial to developing consensus around the development of patient safety bundles [28]. The initial bundles in various stages of production focused on areas associated with maternal death and morbidity include obstetric hemorrhage, severe hypertension and venous thromboembolism prevention in pregnancy. Each bundle was or is being developed with a multidisciplinary team representing multiple organizations. The bundle concept is to facilitate the ability of providers to reliably provide the best care was derived from the Institute for Healthcare Improvement [31] and each bundle is written to allow individual site modification if desired. Currently, the hemorrhage bundle is available to be downloaded from this website [30]. As more bundles are created they will be made available to the public at this website. The belief that implementation of national bundles will improve maternal outcomes is supported by data that sentinel events were decreased after the implementation of an obstetric safety program that included obstetric team training, specific protocols and efforts at clear communication and chain of command [32].
Call to review and analyze all cases of severe maternal morbidity.
– Following the model of reviewing all maternal deaths, each facility that provides obstetric care should review all their cases of severe maternal morbidity to determine if there are areas for improvement in care. It was recommended that all pregnant or recently postpartum women who received four or more units of blood or who were admitted to an ICU should be reviewed. As noted above these characteristics will identify most women with severe morbidity [33]. The purpose of reviewing cases of severe maternal morbidity is to determine if there were opportunities for improvement in care that could potentially reduce morbidity. Key steps to begin the process to review these cases include creating a confidential multidisciplinary maternal morbidity review committee that focuses on whether there are opportunities to improve outcome [34]. The primary data should be abstracted from the chart focused on the specific morbidity such as eclampsia, severe postpartum hemorrhage or disseminated intravascular coagulation, and then details of the care around the morbidity presented to the committee for discussion and assessment. Abstraction and assessment forms including instructions as to their use are available for anyone to download on this website [30]. The committee should focus on systems and if opportunities for improvement in care are identified mechanisms in-place to facilitate change. The culture of the committee should be nonjudgmental. Finally, data should be trended and analyzed eventually.
Research.
– It is critical that as new efforts are developed to understand maternal morbidity that research efforts are ongoing. These efforts include prospective trials such as those undertaken by the NICHD-funded MFMU network that currently includes 14 hospitals which create and participate in clinical trials about obstetric care and outcomes [35]. In addition, as more reviews of severe maternal morbidity are undertaken it will be critical to determine if heightened review and if data analyzed from such reviews can be shown to reduce maternal morbidity.
Contraception.
– Unplanned pregnancies may represent a significant proportion of pregnancies that ultimately have severe maternal morbidity. Therefore, easy access to desired contraception and family planning services must be maintained.
Educational enhancements for American Board of Obstetrics and Gynecology Maternal–Fetal Medicine Fellowship training.
– Maternal–Fetal Medicine Fellowship training requirements were changed to increase the proportion of time spent focused on maternal care and disease including increased requirement for critical care experience.
Conclusion & future perspective
Several major factors have changed dramatically in the last 20 years which undoubtedly affect maternal morbidity and mortality. Obesity has increased with now 36% of women over age 19 meeting criteria for obesity [36]. The mean maternal age during pregnancy has significantly increased with 3% of pregnancies now in women over 40, and the birth rate for women aged 40–44 has increased 2% per year since 2000 [37]. The cesarean delivery rate in the USA is now 33% as compared with 19.7% in 1996 [38]. However, of these factors only advancing maternal age has been shown to have an increased association with maternal mortality with women in their 40s having a mortality ratio 4–5-fold higher than women in their 20s [1]. Therefore, better research is needed to explore the likely deleterious impact of these factors on pregnancy outcomes and how to reduce that impact. In addition, better epidemiologic data about individual deaths and severe morbidities would be very beneficial to understanding how to reduce death and morbidity. Unfortunately, possibly due to lack of a universal healthcare system in the USA, potential fear of medical legal risk for any poor outcome and lack of dedicated resources, obtaining detailed accurate information per case has been difficult. It is hoped that eventually the severe maternal morbidity forms could be collected at the regional and national level in a patient safety organization format and thus analyzed to obtain more specific data to inform efforts to reduce maternal morbidity and mortality.
Another area to address is hospital levels of maternal care. Although there are required levels of care designations for neonatal hospital care and the call for maternal hospital levels of care was made in the 1970s, there are still no requirements for maternal levels of care designation. The concept is that the best maternal outcomes would occur when the level of hospital care for a mother matches her specific need for care. The potential importance of designating clear levels of maternal care for improving maternal outcomes has been noted [39,40]. For example a mother with a known placenta accreta who will likely have a hysterectomy at the time of delivery and require a large amount of blood should be delivered at a hospital that has the providers and system needs to manage massive hemorrhage and its inherent complications such as ventilation ICU care and extended surgical needs. Pertinent to this example, maternal mortality from peripartum hysterectomy was 71% lower in high volume sites compared with low volume sites suggesting better care [40]. The concept of designation and utilization of maternal levels of care is an area that needs further exploration and development in the future. The importance of this topic was just highlighed by a call to implement maternal levels of care supported by multidisciplinary national organizations including ACOG, the Society for Maternal Fetal Medicine, American College of Nurse-Midwives, Association of Women's Health, Obstetric and Neonatal Nurses, American Association of Birth Centers, and Commission for the Accreditation of Birth Centers [41]. Finally, disparities in maternal outcomes are woefully understudied and clearly should be a focus of future research.
US maternal severe morbidity and mortality must decrease. Finally, essentially all the healthcare organizations that are focused on maternal health are aligned in these efforts. The recognition that a substantial proportion of severe morbidity and mortality is preventable, and with the better understanding of the causes of morbidity, the multidisciplinary work to focus on systems of care, develop bundles to guide care, and continue to research focused on maternal care and outcomes should result in reduced morbidity and mortality. These efforts will take the commitment of all providers of obstetric care, the healthcare institutions, public health institutions and the public to successfully make obstetric care safer.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Maternal mortality in the USA has increased since the 1990s.
Large proportion of these deaths are likely preventable.
Maternal death likely has followed a progression from severe maternal morbidity.
Severe morbidity is far more common than maternal mortality.
Excellent markers of severe morbidity are transfusion of four or more units of blood and or intensive care unit admission in peripartum women.
Identifying and reviewing all severe morbidities is likely to yield data to direct interventions to reduce morbidity and mortality.
Morbidity review should focus on provider, system and patient factors to determine if outcome could be improved if some aspect of care had been different.
Six specific recommendations are made to reduce morbidity and mortality including gaining multidisciplinary agreement to reduce mortality, creating national bundles to address specific obstetric problems associated with morbidity and death, and reviewing all maternal severe morbidities and mortalities.
Investigation focused on the impact of maternal age, ethnicity and race, obesity, and cesarean delivery rate on maternal morbidity and death is called for.
Reducing US maternal mortality and morbidity will take the commitment of all providers of obstetric care, the healthcare institutions, public health institutions and the public to be successful.