
Abstract
Background:
Less is understood about female’s nutrient intake’s impact on the severity of the menstrual cycle (MC) symptoms, which consequently interferes with their life quality.
Objectives:
The goal of this study is to look at the relationship between female nutrient consumption and the severity of MC symptoms to better understand how food affects women’s quality of life during their MCs.
Design:
To investigate this impact among healthy adult women, a self-administered, cross-sectional online questionnaire was obtained from 204 regularly menstruating women aged between 18 and 40.
Methods:
The questionnaire included questions on sociodemographic characteristics, a semi-food frequency questionnaire (FFQ), Arabic Premenstrual Syndrome Scale (A-PMS-S) for MC symptoms.
Results:
Results showed intake of polyunsaturated fatty acids (PUFAs) was associated with lower no to mild versus moderate to severe physical symptoms (odds ratio (OR): 0.71, 95% confidence interval (CI): 0.59–0.85; p < 0.001), psychological symptoms (OR: 0.87, 95% CI: 0.77–0.99; p < 0.05), and functioning symptoms (OR: 0.92, 95% CI: 0.83–1.02; p > 0.1). Thiamine prevented psychological symptoms (OR: 0.02, 95% CI: 0.02–0.02; p < 0.001), physiological symptoms (OR: 0.59, 95% CI: 0.58–0.60; p < 0.001), and functioning symptoms (OR: 0.47, 95% CI: 0.47–0.48; p < 0.001). Saturated fat, iron, and niacin intakes increased the risk of experiencing MC psychological symptoms.
Conclusion:
Our findings suggest that MC symptoms were correlated with some nutrient intake from food sources, which is considered an external controllable factor more than demographic characteristics. Therefore, women should be aware of the type of food consumed during their monthly MC phase.
Introduction
All women experience a monthly menstruation cycle (MC) during their reproductive lifespan, which is typically defined as 18–45 years of age. 1 The MC is considered a normal physiological process characterized by periodic and cyclic shedding of the presentational endometrium accompanied by bleeding from the vagina. 2 It is divided into two phases: the follicular phase (FP) defined as day one of the bleeding onset till day 14; 3 and the luteal phase (LP) defined from day 15 of the bleeding onset to day 28.4,5
The FP occurs when the ovaries prepare to release an egg and the uterine lining begins to thicken. 6 During the LP, the egg is discharged and the uterus prepares to accept a fertilized egg. 6 If the egg is not fertilized, the uterus sheds its lining and menstrual bleeding begins, signaling the start of a new MC. 6
Women experience various symptoms before and during the MC. Premenstrual symptoms, sometimes known as PMS (i.e. before the MC), are a collection of physical, emotional, and behavioral changes that occur in the days preceding the commencement of menstruation.7 –9 These symptoms are most common during the LP of the MC, which occurs after ovulation but before the commencement of menstrual bleeding.10,11 PMS can begin as early as 2 weeks before menstruation and normally ends when the MC begins.9,12,13 Menstrual symptoms (i.e. during the MC), on the contrary, are linked to the actual MC. 9 These symptoms often begin with the onset of the monthly period and remain throughout the duration of the bleeding, which usually lasts 2 to 7 days.
The experiences and symptoms during the MC are altered by many factors such as ethnicity or race, lifestyle behaviors (e.g. physical activity or smoking), and nutrient intake. 14 No to mild versus moderate to severe symptoms have a strong impact on women’s psychological state (e.g. mood swings, frustration, nervousness, uneasiness, aggression, sympathy, and thoughtlessness), physical state (e.g. pain in the body, exhaustion, restlessness), eating patterns (e.g. changes in food preferences, and sweet or salt food craving), social life, and on their general functioning. 15
Nutrient intake can have a great impact on the MC; 16 the MC symptoms on the other side significantly affect food and energy intakes. 17 The pathophysiology of MC involves an interaction of brain neurotransmitters, such as serotonin, with ovarian hormones.5,18 Thus, all nutrients involved in the neurotransmitter signals composition would affect the MC symptoms, such as B vitamins (i.e. thiamine, riboflavin, B6) and zinc. 18 Oxidative stress is markedly noticed during MC phase, which would explain the uncomfortable psychological and physiological senses. 19 Consequently, nutrients that are known to have anti-inflammatory and antioxidant functions would ease these symptoms, such as polyunsaturated fatty acids (PUFAs), vitamin C, and Mg. 14 Energy intake is greater in the premenstrual phase compared with the postmenstrual phase 20 due to neurochemical, hormonal, physiological, and psychological factors. Emotional eating day-to-day alteration was reported previously and explicated by the waves in estradiol and progesterone levels. 12
Associations between dietary intake and MC symptoms are often unstable due to potential effects on psychological, physiological, and biological functions.3,21 Previous studies have been limited by either small sample sizes or a lack of data on psychological and physiological symptoms coupled with diet composition macro- and micro-nutrient intakes.14,22,23 Moreover, among the Arabic world and mainly Islamic countries, puberty and menstruation have particular privacy practices regarding health practices. 14 The special attitude toward lifestyle patterns, physical activity, and religious practices may alert menstrual and premenstrual symptoms.24,25 Some women follow special ergogenic aids to deal with MC symptoms, such as the intake of supplements and analgesics, eating more healthy fresh food such as vegetables and fruits. 21
No previous studies have investigated the association between MC nutrient intake and lifestyle factors among women. Most studies focused on PMS among different levels of the women’s community, which addressed the seriousness of the major public health problem simplified by psychological, physiological, and functioning symptoms effect on professional and social functions. Limited or even no research was done to investigate the association of nutrient content of food composition during MC in Jordan. Hence, the novelty of our study is first to address the association between MC symptoms, nutrient intake, and lifestyle habits as potential risk factors among Jordanian women. We hypothesized that MC symptoms are altered by nutrient consumption from food sources and decreased by healthy lifestyles such as being physically active, nonsmokers, and having normal body mass index (BMI).
Materials and methods
Study design
A cross-sectional, observational study design was used in this research to examine the association between nutrient intake and the severity of MC symptoms among Jordanian women. The study tool was a self-administered valid questionnaire answered by a convenient participant sample from Jordan. The questionnaire included demographics, medical history, smoking status, sleeping pattern, the International Physical Activity Questionnaire–Short Form (IPAQ-SF), 26 and the MC symptoms using the validated scale A-PMS-S. 27 A semi-quantitative food frequency questionnaire (FFQ) was used to analyze dietary intake.
In order to enhance the study design and report, the STROBE-nut guidelines were followed by this study. STROBE-nut is an extension of the STROBE statement and stand for the Strengthening the Reporting of Observational Studies in Epidemiology—Nutritional Epidemiology (STROBE-nut): an extension of the STROBE statement.28,29
Instruments
The regularity of the main five food groups’ food consumption was estimated using the FFQ from our participants. Participants were asked during their current MC in particular how frequently, on average, they had consumed the 30 main food items in six classifications (rarely or never, one to three times/month, three to six times/week, one to two times/week, ⩾ two times/day, one time/day). Food photographs were used to standardize the serving size portion. The total daily energy intake, the micro-nutrients, and macro-nutrients mean during specific MC days were estimated by a standard scoring method of food frequency intake. This questionnaire has an excellent result (Cronbach’s alpha (α) = 0.90, McDonald’s omega (ω) = 0.92), and the validity is approved by the cross-correlation test addressed by the significant association of the translated questions.
Nutrition and fitness software (ESHA’s Food Processor® Nutrition Analysis software, version 10.1.1, Salem, OR, USA) was used to analyze the FFQ dietary intake and estimate the total average of daily energy and selected macro- and micro-nutrients intake.
The participants’ physical activity (PA) on their MC days was estimated using the IPAQ-SF, which is a validated measure for assessing PA among adults. This questionnaire assessed the duration and the frequency of the physical activity intensity and classified it into light, moderate, and vigorous. The A-PMS-S (Arabic Premenstrual Syndrome Survey) is a validated Arabic language scale 27 and used to evaluate the experience and severity of PMS symptoms among Jordanian women. The reliability of this scale is high (Cronbach’s alpha = 0.85). This study was used to evaluate the severity of symptoms of MC period days.
The A-PMS-S questionnaire contains 23 items, which are grouped into three parts: psychological, physical, and impairment of functioning. The scoring rates were as the follows:
“Zero” for no symptoms, “One” for mild symptoms, “Two” for moderate symptoms, and “Three” for severe symptoms.
Psychological symptoms consist of dispersed, futility, conscience feelings, nervousness/discomfort, affective labiality, increased sensitivity toward others, irritated feelings, easily getting angry, loss of interest, loss of focus, loss of control, and feeling exhausted. Physical symptoms include energy loss, feeling hungry, sweet/salt cravings, hypersomnia, insomnia, breast soreness, breast bump or weight gain, headache, backache, joint pain, and skin acne. Impairment of functioning symptoms disturb daily life practices, such as social withdrawal, career, or studying.
Participants took around 10–15 min to fill out the A-PMS-S questionnaire. The A-PMS-S is scored on a continuous score based on a mean value of the symptoms. The A-PMS-S was originally designed to measure the variety of physical and psychological symptoms in the days or weeks preceding menstruation (i.e. PMS). We acknowledge that while some premenstrual and menstrual symptoms overlap, they are distinct experiences.10,23,27 PMS symptoms often occur before menstruation and disappear once menstruation begins, whereas menstrual symptoms occur during menstruation. Thus, we modified the A-PMS-S to measure symptoms during the MC. Our modifications were based on the proffer suggesting that in general, menstrual-related diagnoses such as dysmenorrhea or PMS symptoms can be used to classify MC symptoms. 30 With permission from the A-PMS-S developers to better quantify MC symptoms, we have redesigned/modified the questionnaire. The original questionnaire was intended to assess the severity of physical and mental symptoms in the days preceding menstruation. However, we realized that many women had symptoms throughout their MC, not just during the premenstrual phase. As a result, we used the items in the questionnaire to encompass a broader time frame to include the MC.
Specifically, the original A-PMS-S included 23 items that asked about the presence and severity of symptoms experienced in the 2 weeks leading up to the menstrual period. These symptoms are commonly known as premenstrual symptoms or PMS. In this research, the time period that the questionnaire is focused on has been modified to be during the actual MC. This means that instead of asking about symptoms experienced leading up to the period, the questionnaire now asks about symptoms experienced during the period itself. This modification may allow for a more accurate assessment of the symptoms experienced by individuals during their MC. The 23 symptoms were as follows: (1) depressed mood; (2) hopelessness; (3) guilt feeling; (4) anxiety/worry; (5) affective labiality; (6) increased sensitivity; (7) feelings of anger; (8) easily tempered; (9) lack of interest; (10) difficulty concentrating; (11)lethargy/fatigue/decreased energy; (12) increased appetite; (13) craving for certain food; (14) hypersomnia; (15) insomnia; (16) loss of control; (17) feeling overwhelmed; (18) breast tenderness; (19) breast engorgement or weight gain; (20) headache; (21) muscle, joint, or back pain; (22) acne; and (23) symptoms interfering with functioning in relationships, or work, or school, or daily routine.
The basal metabolic rate (BMR) was computed for each subject depending on the participant age, weight, height, as per Institute of Medicine (IOM). 31
Study setting and participants
The data were collected consecutively between September and December 2021 using convenient self-selection adult sampling. The inclusion criteria were women between 18 and 45 years of age, able to read and write in Arabic and provide correct information, while the exclusion criteria were any female who did not meet the previous conditions. Participation was fully volunteering, and they were informed that they would withdraw from the study at any time.
Weight and height were self-addressed in this study. Several meta-analyses have found that self-reported weight, height, and BMI are highly correlated with measured values, with correlation coefficients ranging from 0.90 to 0.99.32 –34 Thus, while there may be some variability in the accuracy of self-reported anthropometric measurements depending on the population being studied and the methods used, overall, the evidence suggests that self-reported measures can be a valid and reliable alternative to measured values in many situations.32 –34
Using weight and height, the BMI (kg/m2) was calculated and classified according to the World Health Organization (WHO) categories of underweight (BMI less than 18.5), normal (BMI between 18.5 and 24.9), overweight (BMI between 25 and 29.9), or obese (BMI more than 30).
The estimated population of Jordan in 2021 is 10.3 million, with roughly 50% of the population being female. Of the 5 million women, it was projected that about 60%, that is, 3 million are childbearing women. Using one sample proportion with 95% confidence intervals (CIs; α), 7.5% margin of error (e), assuming 50% response rate (p), we estimated that 170 women are needed for our survey.
Sample size and power analysis
The sample size (n) is calculated according to the formula: n = z2 × p × (1 – p) / e2 where: z = 1.96 for a confidence level (α) of 95%, p = proportion (expressed as a decimal), e = margin of error. z = 1.96, p = 0.5, e = 0.075; n = 1.962 × 0.5 × (1 – 0.5) / 0.0752; n = 0.9604 / 0.0056 = 170.738. We aimed to include 200–250 participants.
Data were collected via an online questionnaire through immediate digital conversation using Google forms. The questionnaire used to be in the main despatcher via commercials on social media and instant messaging apps. Other recruitment techniques have been used, including word of mouth, work relationships, and authors’ connections. Moreover, members had been requested to share the hyperlink to the questionnaire with extra individuals who match the inclusion standards by using social media. All questions in our survey were in Arabic language and made as easy and comfortable as possible. All information had been saved in an impenetrable Google Drive, on hand solely to the principal investigator, and coded for the research team.
Statistical analysis
The data were analyzed by a statistical coding program (R version 4.1.3 (One Push-Up) was released on 10 March 2022), which is a programming for statistical computing and graphics supported by the R Core Team and the R Foundation for Statistical Computing. The value p < 0.05 was set as statistically significant. Preliminary data analysis data were cleaned by applying the following steps: removing duplicate or irrelevant participants, for example, age < 18 years; fixing structural errors, for example, reporting no MC by providing days for MC; filter undesirable outliers, for example, daily caloric intake > 6000 kilocalories; and handle missing data by replacing it with mean values. Data were tested for normality using Kolmogorov–Smirnov (K–S) and Shapiro–Wilk tests.
We encounter minimal missing data (nineteen occasions only) that was missing completely at random (MCAR). MCAR refers to missing data that are unrelated to the values of any observed or unobserved variables. This signifies that the missing data have nothing to do with the study participants’ characteristics or any other factors that could influence the study’s outcomes.
Descriptive statistics were used to summarize the findings. Continuous variables were given an arithmetic mean (M) and standard deviation (SD), while categorical variables were given counts and percentages.
Confirmatory factor analysis (CFA) was the statistical technique for investigating the underlying structure of a group of data of the modified A-PMS-S questionnaire. 35 Factor analysis was used in this context of ensuring that the psychometric properties of the questionnaire remained intact and that the modified A-PMS-S is a suitable tool for measuring MC symptoms. 35 In our CFA, we tested a pre-specified measurement model that outlines the hypothesized relationships between the observed variables and the underlying factors or constructs. 35 We used the original base model for the A-PMS-S questionnaire with three factors solution. Several fit indices were employed to assess the CFA model’s goodness of fit. Chi-square (χ²): was the statistical test that compares observed data to expected data given the model. 36 A non-significant chi-square score implies that the model fits the data well. 36 The Comparative Fit Index (CFI) was a measure of how well the hypothesized model fit compared to a null model. 37 A CFI value of 0.9 or higher is generally seen as indicating a good fit. 37 Root mean square error of approximation (RMSEA) was a measure of the disparity between the hypothesized model and the observed data that were corrected for the complexity of the model. 38 A score of less than 0.05 suggests a good fit, whereas 0.08 or more indicates a bad fit. Standardized root mean square residual (SRMR) is the average difference between the observed and anticipated covariance matrices. 38 An SRMR value less than 0.08 is generally seen as indicating a good fit. The Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC) were model fit measures that considered both the goodness of fit and the complexity of the model. AIC and BIC values that are lower suggest a better fit. 39
We also performed statistical analysis to assure the questionnaire’s internal consistency and reliability. We employed two common internal consistency measures: Cronbach’s alpha 40 and McDonald’s omega. 41 Cronbach’s alpha is a measure of a scale’s or questionnaire’s reliability. It determines how well each item in the questionnaire measures the same construct or idea. A high Cronbach’s alpha value (typically more than 0.7) suggests that the questionnaire items are consistent and dependable. 40 McDonald’s omega, such as Cronbach’s alpha, is a measure of internal consistency. It is, however, more suited for usage with more complicated models and can provide a more precise measure of reliability. 41 We conducted validation (i.e. CFA and internal consistency) on the entire sample of 204 women, which represented a diverse range of women with varying demographic characteristics. The percentage of the population on which the questionnaire was validated is, therefore, equivalent to the sample size used in our study.
To assess the strength and direction of the association between dietary intake (energy, macro- and micro-nutrients) and MC binomial logistic regression models were used. 42 The psychological, physical, and functioning symptoms of MC were recorded as a dichotomous outcome with no or mild symptoms in one category and moderate and severe symptoms in another category. The predictors were: Total Energy = Energy (kcal); Macro-nutrients = Protein (g); Cho (g); Fiber (g); Cholesterol (mg); Total fat (g); SFA (g); MUFA (g); PUFA (g); and Micro-nutrients (1) Minerals such as Ca (mg), Iron (mg), Mg (mg), Na (mg), Ph (mg), K (mg), Zinc (mg), and (2) Vitamins such as Niacin (mg), Thiamine (mg), Riboflavin (mg), Vit A retinol equivalent (RE), Vit B6 (mg), Vit C (mg). Regression models adjusted for age, BMI, and physical activity as potential confounders. Model selection was guided by the AIC and BIC measure model performance by accounting for model complexity. In both AIC and BIC, a term reflecting the fit of the model to data is combined with a term penalizing the model according to its number of parameters. Under the assumption that the “true model” is not among the candidates, AIC is asymptotically optimal for selecting the model with the least mean squared error. This assumption prevents BIC from being asymptotically optimal.
An analysis of network structures was performed using network analysis (NA) 43 as a set of integrated methods for depicting relations among actors and analyzing the structures that result from the recurrence of these relations. By analyzing the relationships among entities, better explanations of phenomena of objects can be found. The purpose of NA was to visualize the interrelationships between Macro-nutrients such as Protein (g), Cho (g), Fiber (g), Cholesterol (mg), Total fat (g), SFA (g), MUFA (g), PUFA (g); and Micro-nutrients (1) Minerals such as Ca (mg), Iron (mg), Mg (mg), Na (mg), Ph (mg), K (mg), Zinc (mg) and (2) Vitamins such as Niacin (mg), Thiamine (mg), Riboflavin (mg), Vit A (RE), Vit B6 (mg), Vit C (mg) and MC symptoms severity. Sparse correlation matrices were generated using the EBIClasso procedure. 44 Regularizing the model would essentially make it an alternative to the partial correlation matrix, accounting for all of the covariance and removing all residual covariance.
Results
Characteristics of the participants
A total of 204 Jordanian women participated and completed the A-PMS-S questionnaire. The mean participants’ age was 29.8 years, (averaged from 20 to 39 years).
Table 1 shows the sociodemographic, anthropometric, and general characteristics of the study participants. Eighty-five % were single and three–quarters were nonsmokers. Around 74% held an associated diploma/BSc certification. BMI mean was 24.23 ± 4.7 kg/cm2, which clarified that participants’ weight was distributed between the normal and overweight categories. The mean MC duration was 6 days, and the menarche onset was between 11 years to 14 years, with a mean of 13 years.
Participants’ sociodemographic characteristics and anthropometric measurements (n = 204).

SD: standard deviation; BMI: body mass index; MC: menstrual cycle.
Nearly half of the participants (52%, 49%, and 55%) suffered from no to mild versus moderate to severe physical, psychological, and functioning symptoms, respectively.
Psychological symptoms consist of dispersed, futility, conscience feelings, nervousness/discomfort, affective labiality, increased sensitivity toward others, irritated feelings, easily getting angry, loss of interest, loss of focus, loss of control, and feeling exhausted. Physical symptoms include loss of energy, feeling hungry, sweet/ salt cravings, hypersomnia, insomnia, breast soreness, breast bump or weight gain, headache, backache, joint pain, and skin acne.
Functioning symptoms include symptoms that disturb daily life practices, such as social life withdrawal, career, or studying.
The modified A-PMS-S tool appeared to have high psychometric properties in measuring MC symptoms. Specifically, internal consistency in terms of α and ω were both > 0.90. Results from CFA confirmed the factorial structure with CFI, Tucker–Lewis Index (TLI), Bentler–Bonett non-normed Fit Index (NNFI), Bentler–Bonett Normed Fit Index (NFI), Bollen’s Relative Fit Index (RFI), Bollen’s Incremental Fit Index (IFI), and Relative Noncentrality Index (RNI) all being > 0.90. Parsimony Normed Fit Index (PNFI) was 0.86.
Dietary intake
The mean of nutrients intake obtained from 30 common food items from FFQ is summarized in Table 2. The results of the FFQ were analyzed by using the multiple logistic regression analysis. The association between certain types of food items and psychological, physical, and functioning symptoms showed that PUFA and thiamine intakes were associated with lower risk of reporting no to mild versus moderate to severe physical, psychological, and functioning symptoms. Explanatory, PUFA showed a reasonable protective impact in decreasing the no to mild versus moderate to severe all three symptoms’ domains: physical symptoms (odds ratio (OR): 0.71, 95% CI: 0.59–0.85; p < 0.001), psychological symptoms (OR: 0.033, 95% CI: 0.77–0.99; p < 0.05) and functioning symptoms (OR: 0.92, 95% CI: 0.83–1.02; p = 0.101). In addition, thiamine showed a highly protective impact in all MC no to mild versus moderate to severe symptoms: psychological symptoms (OR: 0.02, 95% CI: 0.02–0.02; p < 0.001), physiological symptoms (OR: 0.59, 95% CI: 0.59–0.60; p < 0.001) and functioning symptoms (OR: 0.47, 95% CI: 0.47–0.48; p < 0.001).
Multiple regression analysis for energy and nutrients intakes and associations with MC psychological and physiological no to mild versus moderate to severe symptoms.

No to mild outcome variable is dichotomous = 0, versus moderate to severe symptoms = 1.
RDA: recommended dietary allowance; SD: standard deviation; OR: odds ratio; CI: confidence interval; SFA: saturated fatty acids; MUFA: monounsaturated fatty acids; PUFA: polyunsaturated fatty acids; Vit.: Vitamin; RE: retinol equivalents.
Nutritional goals for each age/sex group used in assessing adequacy of USDA Food Patterns at various calorie level.
Significant at p < 0.05.
Vitamin B riboflavin increased the risk of the psychological and functioning MC symptoms with a noticeable high OR addressed a very high risk of no to mild versus moderate to severe psychological symptoms (OR: 50.93, 95% CI: 50.61–51.26, p < 0.001) and functioning symptoms (OR: 10.9, 95% CI: 10.84–10.97, p < 0.001). On the contrary, vitamin B riboflavin decreases the risk for no to mild versus moderate to severe physiological symptoms with an OR of less than 0.50 (OR: 0.50, 95% CI: 0.49–0.50; p < 0.001). Similar results for zinc intake, which was associated with lower no to mild versus moderate to severe physiological symptoms (OR: 0.55, 95% CI: 0.51–0.59; p < 0.001), while increasing the risk of no to mild versus moderate to severe psychological symptoms ratio (OR: 1.44, 95% CI: 1.35–1.53; p < 0.001).
Vitamin B6 intake increases the risk of no to mild versus moderate to severe physiological symptoms (OR: 3.49, 95% CI: 3.44–3.55, p < 0.001); on the contrary, its intake decreases the no to mild versus moderate to severe of both psychological and functioning symptoms, respectively (OR: 0.79, 95% CI: 0.78–0.81; p < 0.001) and (OR: 0.47, 95% CI: 0.47–0.48; p < 0.001). A similar impact was addressed for the MUFA intake on increasing the physiological symptoms with an OR of (OR: 1.27, 95% CI: 0.96–1.68, p > 0.05), while protective from the psychological symptoms (OR: 0.86, 95% CI: 0.73–1.02; p > 0.05).
Saturated fat, iron, and niacin intakes increase the risk of experiencing the psychological symptoms of MC. No association was found between the energy kcal, carbohydrate, fiber, total fat, cholesterol, magnesium, phosphorus, calcium, sodium, potassium, vitamin A and vitamin C intakes with no to mild versus moderate to severe symptoms of both psychological, physiological, and functioning of the MC of the participants.
Recommended Daily Allowance (RDA) among our participants showed that among all nutrients, 45 only the intake of calcium and potassium were less than the RDA (intake 700 mg/day versus 1000 mg RDA, intake 4341 mg/day versus 4700 mg/day) according to their age and sex. Energy intake was higher by 1000 kcal for some participants. Carbohydrate and protein intakes were doubled (386 to 236 g intake versus 130 g RDA, 156 to 86 g intake versus 46 g RDA, respectively). Iron, Mg, Na, and K intakes were higher than RDA (42 mg intake versus 18 mg RDA, 506 mg intake versus 310 mg RDA, 2877 mg intake versus 2300 mg RDA, 1000 mg intake versus 700 mg RDA, respectively). Moreover, Niacin, Thiamine, Riboflavin, Vitamin A, Vitamin B6, and Vitamin C intake exceeded the RDA (23.9 mg intake versus 14 mg RDA, 1.4 mg intake versus 1.1 mg RDA, 1.7 mg intake versus 1.1 mg RDA, 953.3 RE intake versus 700 (RE) RDA, 2.7 mg intake versus 2.4 mg RDA, 121.6 mg intake versus 75 mg RDA, respectively).
The correlation between nutrient’s food composition is highlighted in Figure 1, which shows a positive correlation between blue lines and a negative correlation between red lines. The thickness of the lines presents the strength of the association (the thicker the lines, the greater the correlation). Protein as a macronutrient was positively correlated with iron and cholesterol intakes and also positively correlated with thiamine intake, but in a weaker bond. Carbohydrate’s intake was strongly positively associated with thiamine intake. Total fat was positively correlated with sodium, potassium, and zinc intakes. Moreover, vitamin B6 was strongly associated with fiber intake, which in turn was correlated with potassium in a positive way similar to vitamin A association with riboflavin. Furthermore, vitamin B6 was correlated with niacin intake, which correlated with thiamine, and then thiamine was correlated with protein, all in positive correlations. Vitamin C was correlated with potassium, which in turn was correlated with magnesium in a positive correlation. However, sodium is negatively correlated with the intake of zinc. Similarly, fiber is negatively correlated with the intake of vitamin C, which in turn is negatively correlated to calcium, and total fat is negatively associated with magnesium.
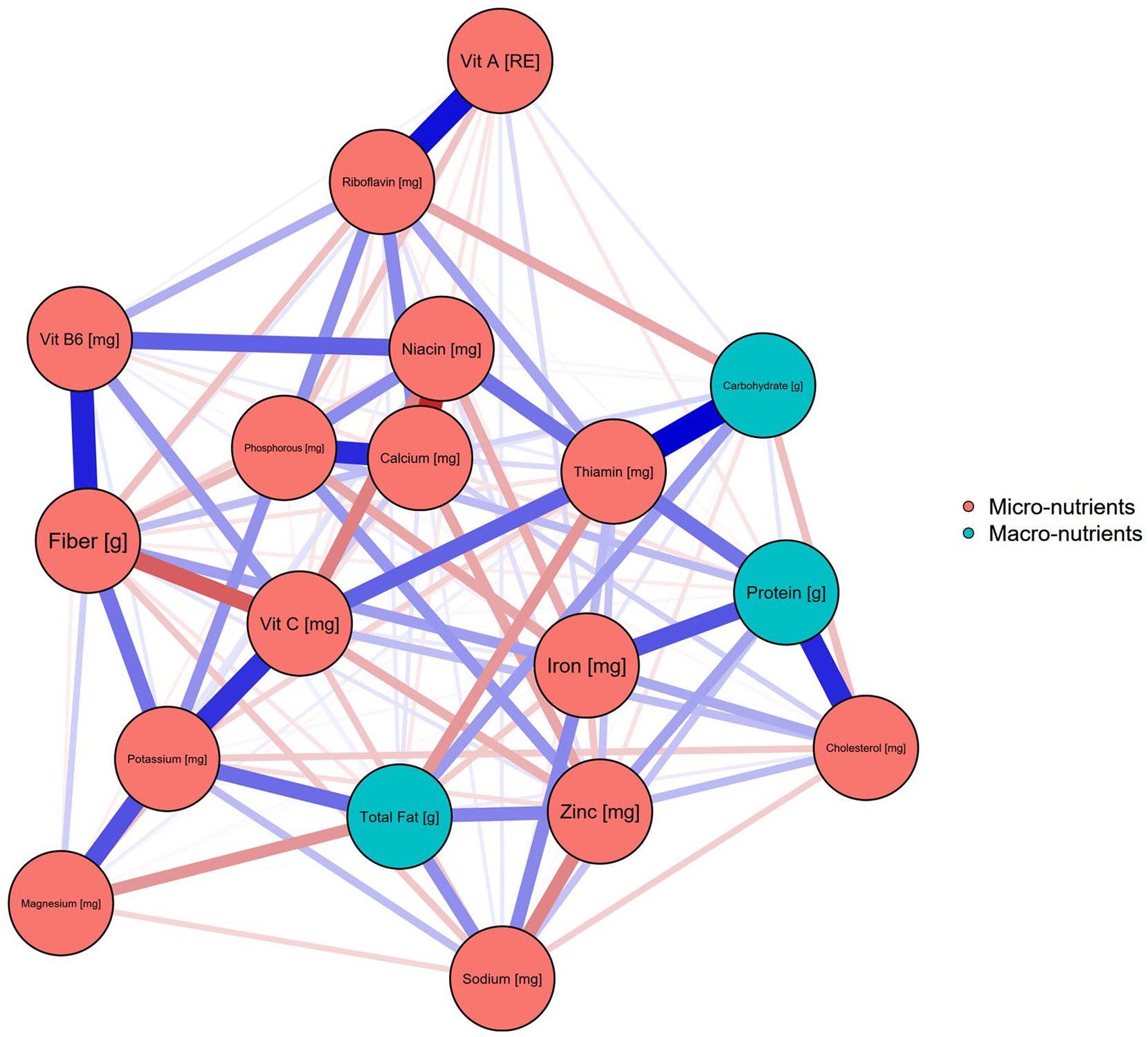
Network analysis of nutrient’s food composition and their impact on MC.
Association between descriptive data and nutrient intake with MC symptoms:
Using the independent samples t-test. There was no significant association between smoking status, BMI, physical activity, and marital status with nutrient intake toward MC symptoms. However, by using a one-way analysis of variance (ANOVA; Welch’s) test, marital status showed a significant association with consuming PUFA (p-value = 0.005). BMI showed significant associations (at p-value < 0.001) with nutrient intake and MC symptoms, such as sodium, potassium, zinc, magnesium, vitamin A, and vitamin C.
Discussion
Each menstruating female passes into a monthly reproductive cycle. 5 Several studies correlated MC symptoms with different life pattern factors.46 –48 Symptoms were more clarified and categorized as they took multiple expressions such as physiology pain (body pain, cramping, breast tenderness), psychological warning signs (i.e. mood swings, depression, anxiety), and functioning indicators that fluctuate in women’ life routine.27,49 A balanced diet plays an important role in overall health. Henceforward, female dietary patterns affect her cognition and emotions during her MC. 4 This study aimed to determine the correlation between nutrients consumed during MC and the severity of MC psychological, physiological, and functioning symptoms among Jordanian adult women.
To the best of our knowledge, and according to the accessible literature, this is the first research that examined MC symptoms’ correlation with variable dietary and lifestyle behaviors since the majority of previous research focused on PMS.14,48,50 Symptoms of MC significantly did not differ regarding the female’s educational level, physical activity, and BMI.
Remarkably, food intake varies during MC,3,15 energy intake was higher than the RDA among the participants (2000 to 3000 kcal versus 2000 kcal per day RDA) with no effect on the MC symptoms. In contrast, different results were shown in a UAE study where energy intake decreased and varied during the MC. 51 Nonetheless, our findings showed that daily energy and total macronutrient intake had no impact on menstrual symptoms (OR averaged from 0.88 to 1.01), with no significant differences. It is important to mention that macronutrient (protein and carbohydrate) intake in this study were over double the recommended dietary allowance RDA for their age (protein intake was 121 g ± 35.7 while RDA is 46 g/day, carbohydrate intake was 311.6 g ± 75.5 while RDA is 130 g), this might explain the indifferent effect of the macronutrients on the MC symptoms.
Our findings showed that whenever the intake of nutrients exceeds the RDA, the nutrients deactivate their impact on the MC symptoms. The metabolite’s precursors would explain it in vivo of those nutrients. Table 2 shows the exceeding amount of minerals related to meat (protein) intake such as Iron, Mg, Na, and K intakes were higher than RDA (42 mg intake versus 18 mg RDA, 506 mg intake versus 310 mg RDA, 2877 mg intake versus 2300 mg RDA, 1000 mg intake versus 700 mg RDA, respectively). The conflicting impact of zinc from food sources is shown in Table 2; it has a positive protective impact in decreasing no to mild versus moderate to severe physiological symptoms (OR: 0.55, 95% CI: 0.51–0.59; p < 0.001), while increasing the risk of no to mild versus moderate to severe psychological symptoms ratio (OR: 1.44, 95% CI: 1.35–1.53; p < 0.001). The Iranian study addressed the protective effect of long-term zinc supplementation for 12 weeks in improving physical and psychological symptoms. 20
On the contrary, Niacin intake was reported to be effective in relieving menstrual cramps.18,52 Niacin intake in our study doubled the RDA (24 versus 14 mg/day RDA) and negatively affected the MC’s motion symptoms (OR: 1.8, 95% CI: 1.47–2.21, p < 0.001). Niacin, with its role in synthesizing tryptophan, the precursor of serotonin, has a very important impact on the psychological symptoms among MC.53,54 Our study showed a negative correlation, which again might be explained by the high dose from the natural food source that would fluctuate the metabolite pathways.
Furthermore, it was addressed that the strength of menstrual pain, for example, was decreased by high consumption of fish, fruits, and fiber. 54 Interestingly, high fish intake enclosed healthy types of fatty acids such as PUFA. The protective impact of PUFA and fish oil on releasing the annoying symptoms of MC were addressed in many previous studies.55,56 Our study resulted with PUFA intake from daily food items being positively associated with decreasing the no to mild versus moderate to severe symptoms of all the three MC domains: physical symptoms (OR: 0.71, 95% CI: 0.59–0.85; p < 0.001), psychological symptoms (OR: 0.87, 95% CI: 0.77–0.99; p < 0.001), and functioning symptoms (OR: 0.92, 95% CI: 0.83–1.02; p > 0.101). Moreover, olive oil, one of the main sources of MUFA in Jordanian cuisine, showed a similar impact to protect from psychological symptoms (OR: 0.86, 95% CI: 0.73–1.02; p > 0.05). However, MUFA boosted the physiological symptoms (OR: 1.27, 95% CI: 0.96–1.68, p > 0.05). The well-known anti-inflammatory properties of the PUFA and MUFA would be the potential reason that protects from gynecological MC pains. 57 In addition, they sustain the production of the prostaglandin lipids groups through pathophysiological pathways, which are involved in dealing with infection and healing. Olive oil was shown to decrease blood loss during the MC, protecting against iron-deficiency anemia.58,59 On the contrary, SFA (the rich components in fast food and junk food sources) had a negative impact on psychological MC symptoms (OR: 1.33, 95% CI: 1.09–1.64; p 0.006) and on functioning MC symptoms (OR: 1.14, 95% CI: 1.00–1.30; p 0.048). Similar results were approved among Iranian women in 2018, which showed that high-fat meals (from junk food sources) increased the risk of MC pain. 60 For instance, it was assumed that symptoms such as breast swelling, tenderness, nodularity, and water retention due to the increased levels of estrogen have been associated with high fat intake, particularly SFA. 61
Oxidative stress heightens the negative impact on mood as it changes neurotransmitter secretion. In fact, during the MC, the antioxidant capacity declines, while the oxidative stress increases as a result, an imbalance of oxidant/antioxidant systems may be a cause or consequence of various stress symptoms. Hence, consuming dietary antioxidants has a positive impact on mood changes during the MC; for example, fruits and vegetables are foods high in fiber and antioxidants.4,14 However, our study showed no significant direct impact on fiber intake on the MC symptoms as shown in Table 2, while from Figure 1 (near here), fiber showed a strong positive connection with vitamin B6, which had a strong impact on MC symptoms. Vitamin B6 with vitamin C and fiber in Figure 1 showed a strong positive correlation. Vitamin C intake significantly differed (p < 0.05), although OR showed no impact on the psychological symptoms.
Vitamin B group are associated with gamma-aminobutyric acid (GABA), serotonin and dopamine neurotransmitter synthesis and the deficiency of each neurotransmitter is associated with some psychological symptoms. 61 Intake of vitamin B6 was close to the RDA (2.4 mg intake versus 2.7 mg/day RDA), thus it had an impact on the MC symptoms. It is well-addressed by studies that consuming 50 to 100 mg/day of vitamin B6 supplement would have a beneficial impact in managing pains and symptoms of the monthly cycle.62,63 Vitamin B6 in addition to thiamine, riboflavin, and niacin are cofactors in synthesizing serotonin and dopamine, the “happy neurotransmitters” chemicals that support nerve function and brain signals transmission. 63 In our study, B6 intake from food items had conflicting strong impacts on MC symptoms. From Table 2 (near here), vitamin B6 intake was associated with lower no to mild versus moderate to severe of both psychological and functioning symptoms (OR: 0.04, 95% CI: 0.04–0.04; p < 0.001; OR: 0.79, 95% CI: 0.78–0.81; p < 0.001, respectively), henceforth protecting the participant from being not effective in their daily routine. On the contrary, B6 intake did not protect from physiological symptoms, and it showed increase in the menstrual pain, headache, and so on (OR: 3.49, 95% CI: 3.44–3.55, p < 0.001). Most of the B6 studies, which recommend its intake to protect against the PMC/MC annoying symptoms focused on supplements 18 rather than B6 natural presence in food sources. This study is one of the primary studies, which assessed the impact of B6 intake from natural food sources. Fortunately, it has a strong positive impact on the psychological symptoms during the MC cycle as improved from our study. Consequently, B6 positively affected the psychological and functioning symptoms before and during the menstrual monthly cycle.
Finally, thiamine is important for the synthesis of serotonin and dopamine, which promote a joyful mood and prevent sadness, depression, and most of the psychological symptoms combined with the MC. 62 The findings of is study strongly the highly protective impact in all MC no to mild versus moderate to severe symptoms: psychological symptoms (OR: 0.02, 95% CI: 0.02–0.02; p < 0.001), physiological symptoms (OR: 0.59, 95% CI: 0.58–0.60; p < 0.001), and functioning symptoms (OR: 0.47, 95% CI: 0.47–0.48; p < 0.001). Thiamine has an important role in contracting muscles closely linked to the uterus where cycle cramps and pains occur. 64 In addition, riboflavin vitamin accelerated the psychological and functioning MC symptoms’ tone as observed from the high OR of the no to mild versus moderate to severe psychological symptoms (OR: 50.93, 95% CI: 50.61–51.26, p < 0.001) and functioning symptoms (OR: 10.9, 95% CI: 10.84–10.97, p < 0.001). Yet, vitamin B riboflavin was associated with lower risk of no to mild versus moderate to severe physiological symptoms with an OR less than 0.50 (OR: 0.50, 95% CI: 0.49–0.50; p < 0.001). Riboflavin is related conversely to estradiol secretion in vivo and promotes weight gain during the follicular cycle.23,65 Therefore, sufficient intake of vitamins and minerals through food intake seems to be critical to relieve or prevent MC symptoms. 33
Our study concludes the impact of food sources on the variant MC symptoms among Jordanian women. PUFA and thiamine influenced the three MC symptoms’ domains positively. However, other nutrients had a different impact on the symptoms in which they had a different impact on the MC symptoms domain. Some nutrients such as Mg, Na, K, calcium, fiber, and cholesterol had no impact. This study is the first to use the highly sophisticated protocol to analyze accurate network data from adult menstruating women.
Although many recent studies have been done regarding PMS, the association between nutrient intake and MC (FP) symptoms in particular is ambiguous. Indeed, our study has done so, giving it the power, uniqueness, and distinctiveness. It is one of the few rare studies that have examined and evaluated the impact of dietary habits and nutrient consumption on FP among Jordanian women resulting in a significant contribution. In addition, this study adds interesting, beneficial, and worthy knowledge to be considered to increase awareness among women regarding this issue encouraging them to adopt healthy and responsible strategies, thus alleviating or preventing symptoms development.
Strengths and limitations
The study has several strengths: This is one of the few studies to look into the effect of nutritional consumption on the severity of MC symptoms in healthy adult women. A self-administered, online questionnaire was employed in the study, allowing for a large sample size and simple data collection. The study assessed MC symptoms using a validated questionnaire, allowing for standardized quantification of symptom severity. The research adjusted for a number of potential confounding factors, including age, BMI, smoking status, and degree of physical exercise.
The study also has some limitations: The cross-sectional form of the study hinders establishing causation and limits our capacity to draw inferences regarding the direction of the observed relationships. The study relied on self-reported nutrient consumption via a semi-quantitative FFQ, which is susceptible to recall bias and may not include all relevant dietary components. The study only included healthy adult women aged 18 to 40, limiting the findings’ generalizability to other populations. The study did not account for the use of hormonal contraceptives, which may have an impact on MC symptoms. The study did not look at the effects of vitamin supplements or other non-dietary factors on MC symptoms.
Implications for practice
The study’s findings have crucial consequences for healthcare practitioners and women suffering from MC symptoms. The study findings can be used by healthcare practitioners to counsel women on the potential impact of nutrient intake from food sources on the severity of MC symptoms. Women, in particular, can be urged to consume more foods high in PUFAs and thiamine, while avoiding meals high in saturated fat, iron, and niacin. Women who have MC symptoms can benefit from the study findings by being more conscious of their food consumption during their monthly MC phase. Women may be able to minimize the intensity of their symptoms and improve their quality of life by making conscientious food choices. Women who are already using dietary supplements to manage their MC symptoms should contact with their healthcare physician to ensure they are taking the right nutrients. The study emphasizes the importance of a healthy and balanced diet in controlling MC symptoms, and healthcare practitioners should think about including nutritional counseling into their usual practice for women who have MC symptoms. However, further study is needed to determine causality and the best nutritional strategies for controlling MC symptoms.
Implications for future research
This study’s findings offer important insights into the potential impact of food consumption on the severity of MC symptoms in healthy adult women. However, more research is needed to build on these findings and address some of this study’s weaknesses.
Future research should employ a longitudinal design to establish causality and study the potential impact of nutrient intake changes on the incidence and severity of MC symptoms over time. This would help researchers better grasp the temporal association between dietary consumption and MC symptoms. To improve the accuracy of dietary evaluations and limit the possibility for recall bias, future studies should use objective measurements of nutrient consumption, such as biomarkers or food recalls. Future studies should include a more diversified sample of women of various ages, nationalities, and MC patterns. This would improve the findings’ generalizability and provide a better knowledge of the impact of food intake on MC symptoms in different groups. Future research should look at the effect of nutrient supplementation on MC symptoms, particularly for nutrients reported to be connected with symptom severity in this study.
Conclusion
The study’s findings imply that food consumption habits during the MC may have both preventive and aggravating effects on monthly MC symptoms. This suggests that certain foods or dietary habits may help alleviate or prevent MC symptoms, whereas others may aggravate or cause them. The findings of the study indicate that there may be a link between diet and menstrual health, and that paying attention to dietary choices during the MC may be key for controlling monthly discomfort.
As a result, food intake should be taken into consideration during MC. Initially, food rich in PUFA and thiamine are highly recommended during MC days for their protection against inconvenience-related symptoms, while food rich in SFA should be avoided to prevent emotional symptoms. Among women who suffer from MC psychological symptoms, avoiding food rich in riboflavin, niacin, and iron is recommended. Food intake should be controlled and managed carefully during MC days to improve the monthly female inconvenience experience. It is advised to provide health education for adult women about dietary habits and food intake as a protecting procedure to alleviate MC symptoms.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231185624 – Supplemental material for Menstrual cycle symptoms are associated with nutrient intake: Results from network analysis from an online survey
Supplemental material, sj-docx-1-whe-10.1177_17455057231185624 for Menstrual cycle symptoms are associated with nutrient intake: Results from network analysis from an online survey by Hadeel A. Ghazzawi, Omar Alhaj, Nicola Bragazzi, Lana Alnimer and Haitham Jahrami in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231185624 – Supplemental material for Menstrual cycle symptoms are associated with nutrient intake: Results from network analysis from an online survey
Supplemental material, sj-docx-2-whe-10.1177_17455057231185624 for Menstrual cycle symptoms are associated with nutrient intake: Results from network analysis from an online survey by Hadeel A. Ghazzawi, Omar Alhaj, Nicola Bragazzi, Lana Alnimer and Haitham Jahrami in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.