
Abstract
Background:
Providing quality contraceptive counseling services is essential to support mothers in using modern contraceptives that meet their needs. However, the quality of service provision has not been evaluated in a study setting.
Objective:
This study aimed to assess the quality of contraceptive counseling using a service quality model in southern Ethiopia.
Design:
A facility-based cross-section study was conducted.
Methods:
The study was conducted from 15 May to 15 June 2021 at the public health facilities of Boloso Bombe Woreda in southern Ethiopia. In total, 391 clients were included using systematic sampling techniques. Data were collected using a structured service quality questionnaire, entered into EPI data version 3.1, and analyzed using SPSS version 25 for data analysis. The significant difference and correlation between the mean of a client’s perception and expectation were determined using the Wilcoxon’s sign test. The correlation between sociodemographic characteristics and the quality of counseling was tested using the Friedman’s test. A p value of <0.05 was taken as the criterion for statistical significance. Finally, the result was presented in a table and pie chart.
Results:
The study participants included 391 women of childbearing age attending family planning clinics, with a 96.6% response rate. Overall, the quality of advice was found to be low. Respondents’ ages (p < 0.001, χ2 = 385.00), number of living children (p < 0.001, χ2 = 381.04), marital status (p < 0.001, χ2 = 359.60), type of contraceptive method (p < 0.001, χ2 = 379.61), user type (p < 0.001, χ2 = 368.59), occupations (p < 0.001, χ2 = 379.00), and educational status (p < 0.001, χ2 = 371), 20) were statistically associated with the quality of counseling service.
Conclusion:
In all health facilities, the quality of contraceptive counseling services was low. Family planning users had high expectations of the contraceptive counseling service compared to that which they received.
Plain Language Summary
Maternal and neonatal mortality are current global problems, although there have been improvements over the last few decades. Providing quality family planning is among the most important approaches to preventing maternal and neonatal mortality. To achieve quality family planning services, we should provide quality counseling services. Improper counseling causes fear of side effects as well as rumors and misconceptions about contraceptive use. Most women have stopped using contraceptives. To address this problem, the quality of counseling services should be evaluated regularly. However, the quality of the counseling service had not been evaluated in the study area.
For this reason, we evaluated the quality of advice among family planning users, which we found to be low. In the study area, substandard contraceptive counseling leads to discontinuation of contraceptive services; change in methods, from the most effective to the least effective; unwanted pregnancies; and unsafe abortions. We suggest that all stakeholders should take effective and immediate action in this study area. This, in turn, would greatly improve contraceptive use, prevent unsafe abortions and unwanted pregnancies, prevent high fertility rates, and promote the health of mothers and their children.
Introduction
Contraceptive counseling is an ongoing face-to-face communication that takes place between family planning (FP) users and healthcare providers, helping clients to make decisions about the number of children they would like to have in the future. 1
Contraceptive advice is a woman’s right, which she must access when needed. The World Health Organization recommends quality contraceptive counseling services as rights-based FP services. Therefore, every healthcare provider has a responsibility to provide evidence-based information and to educate women about the effectiveness of the methods they use to prevent misinformed choices. 2
From a client’s perspective, quality of contraceptive counseling (QOCC) is a comparison between the client’s expectations of and perception after contraceptive counseling service. If clients’ expectations of the counseling service are higher than their perception of it, then the counseling quality is insufficient from their perspective, resulting in the clients not being able to meet their needs. Conversely, if the service provided exceeds clients’ expectations, the service is considered excellent, while the service quality is satisfactory if the clients’ expectations and perceptions match. Delivering quality contraceptive services to clients based on their expectations and interests is important for the success of healthcare organizations, and it is an essential step in providing quality counseling.3,4
Counseling service provision is critical to increasing service utilization and has a profound impact on economic situations.5 –7 The interaction between contraceptive counselors has a decisive influence on the QOCC services. It provides an opportunity for clients to assess and evaluate service quality; conversely, it provides healthcare providers with the ability to manage contraceptive counseling services. Globally, the prevalence of modern contraceptives among married women increased by only 2.1% over the past 20 years (2000–2019). This is due to several factors, including the low quality of contraceptive advice, limited access to FP services, provider bias, and fear or experience of side effects. 8 Low QOCC contributes to rumors about fears of side effects and misconceptions about contraceptive use.9,10
Evidence shows that in 21 of 52 developing countries, 20%–30% of women do not use FP methods because they fear side effects, health risks, and inconvenient methods. As such, 74 million unwanted pregnancies occur in these countries every year.11 –13 Owing to the lack of quality contraceptive counseling services and other related factors, 29% of women in sub-Saharan Africa experience unplanned pregnancies, with approximately 14 million unplanned pregnancies occurring each year. 14
In Ethiopia, the Ethiopian Demographic Health Survey (2016) reported that about 35% of respondents had stopped using contraceptives in the last 5 years. Of these, 18% of women discontinued the use of contraceptives for fear of side effects and other method-related health concerns. This report also showed that, despite concerted efforts to improve access to modern FP over the past decade, approximately 22% of women have not met their FP expectations. This could be due to substandard contraceptive counseling services. Although the Ethiopian government committed to achieving national modern contraceptive prevalence (55%) in 2015, the reported national modern contraceptive prevalence in 2019 was 41% service. The main problems in this challenge were poor quality contraceptive advice and provider- and user-related problems.15,16
To increase the quality of advice, advisors should not simply lecture their clients, but also ensure mutual understanding. Counselors should respect their clients and address their issues and concerns about contraception in a straightforward manner. To improve the quality of counseling, counselors should engage in effective communication, have adequate knowledge and skills, and have good attitude and behavior.1,17
Evidence indicates that some counselors use directive-counseling services that influence their clients’ decision-making. For this reason, the methods change from long-acting to short-acting methods and vice versa. Counselors with sufficient knowledge of long-acting methods advise their clients on them, while those with little knowledge might confuse the clients or advise them on short-acting methods. All of this affects the clients’ ability to make decisions, possibly affecting their contraceptive use. Therefore, healthcare providers need to be trained and updated. The quality of counseling does not depend solely on the counselors; it can be influenced by clients’ understanding and knowledge, their trust and respect for the counselors, their family members, and their spouses. These situations can make it difficult for them to choose and use FP methods.1,18,19
Previous experience with using an FP service may influence QOCC. New users are less likely to receive quality advice than are repeat users. Counselors should consider their clients’ prior exposure status. The Ministry of Health and other implementing partners generally have their own counseling tools, checklists, and guidelines for counseling services. However, there are no standard tools, although these instruments have a significant impact on improving the quality of counseling.11,20
Ideal counseling processes such as improved physical condition, wholesome interpersonal interaction, respectful caregiving, adequate contraceptive supply, easy access to and timely delivery of services, regular assessment of clients’ perceptions and expectations, and attitudes toward contraceptive services are important in improving patients’ quality of counseling outcomes. 21 To improve the use of effective contraceptive methods by women, all methods must be covered during counseling sessions. As such, this could have a significant impact on quality improvement, method choice, and client satisfaction with the service they receive.5,6,11,21
From the perspective of unmet contraceptive needs, the key approach to improving FP use continuity is to provide adequate FP counseling services. However, the QOCC in Ethiopia is currently low and varies from region to region. 22 In addition, no prior study has been conducted in this study area. Although some studies in Ethiopia have focused on the quality of contraceptive services, they did not capture the quality of counseling from the clients’ perspective.23,24 Therefore, using the quality of service model (SERVQUAL), this study aimed to assess the QOCC services from the perspective of clients using FP services in Boloso Bombe Woreda public health facilities.
Methods
Study design and setting
A cross-sectional study was conducted at Boloso Bombe Woreda public health facilities from 15 May to 15 June 2021. This Woreda is located in the Wolaita zone in southern Ethiopia, and it is 356 km away from the capital of Ethiopia, Addis Ababa. According to the 2020 Boloso Bombe Woreda Annual Baseline Report, the Woreda has a total population of 114,342 people. Of these, 57,400 are female, 26,642 are of childbearing age, and the remaining 56,942 are male. The Woreda has a primary hospital and three health centers. The study was conducted in all healthcare facilities. 25
Participants
The study population included randomly selected women of childbearing age who attended FP clinics in all Boloso Bombe Woreda public health facilities during the study period.
Inclusion and exclusion criteria
The study included selected women of childbearing age who sought the FP service during the data collection period. Those who used traditional methods and those who were unable to communicate (deaf people) were excluded from the study.
Study variables
In this study, the quality of contraceptive advice was a dependent variable and sociodemographic variables such as age, marital status, education level, user type, type of contraceptive methods, occupation, and number of surviving children were independent variables.
Sample size and sampling procedure
The sample size was calculated using a population proportion calculation formula, based on the following assumptions: 95% confidence interval (CI), 5% error rate, and 39.7% population proportion taken from the previous study. 22 The calculated minimum sample size for the study was 368. Considering the 10% non-response rate, the total sample for the study was 405. All public health facilities in Boloso Bombe Woreda were included in the study. The average monthly client flow to FP services for six consecutive months was determined as 1160. The final sample size (405) was proportionally allocated to these service centers by considering their monthly client flows. Finally, the participants were selected through systematic random sampling.
Measurements
The tangibility dimension relates to the appearance of physical facilities, healthcare providers, and communication materials. 26 Reliability relates to the ability of service providers to deliver the promised services accurately and consistently. 27 Responsiveness relates to a service provider’s desire to help a client and provide quick service. 5 Assurance relates to the knowledge and skills of a provider and their ability to instill trust and confidence. 27 Empathy relates to a counselor’s ability to provide caring and individualized attention to clients. 27 Perceptions (P) are referred to as the result of a client’s view of the service dimensions. 28 Expectations (E) are referred to as clients’ wants or desires regarding what they think a service provider should offer. 28 Expectations (E) are referred to as clients’ wants or desires regarding what they think a service provider should offer. 29
Each question had five options, rated from 1 (strongly disagree) to 5 (strongly agree). The counseling service quality-gap score for each dimension was calculated by subtracting the expectancy score from the perception score for that dimension. In each dimension, the question’s score was summed and its total was divided by the number of questions in that dimension. The total value for the quality of the counseling service was determined from the aggregation of all question scores, and the sum was divided by the total number of questions in the questionnaire; the total value for the quality of the counseling service was determined. It was recoded as follows:
TA: Average gap score for tangible items =
RL: Average gap score for reliability items =
RN: Average gap score for responsiveness items =
AS: Average gap score for assurance items =
EM: Average gap score for empathy items =
OSQ: Overall counseling service quality =
Tangibility dimension item 1 (TA1) is calculated by subtracting the client expectation on tangibility dimension item 1 (TA1E) from client perception on item 1 (TA1P), which is written as TA1 = TA1P – TA1E. The same is true for TA2, TA3, RL1, RL2, RN1, RN2, AS1, AS2, EM1, and EM2.18,27,28,30,31
High quality of counseling service—The resulting SERVQUAL score is positive when performance exceeds expectation (P > E). 32 Satisfactory quality of counseling service—SERVQUAL score is zero (E = P) when perceived (performed) counseling service is equal to expected counseling service. 29 Low quality of counseling service—When SERVQUAL score is negative (E > P), then the performance does not meet the client’s expectation. 29 In addition, a positive quality score for counseling service indicates that the counseling service provided exceeds the service recipient’s expectations, and a negative quality score indicates a quality gap. If the score is equal to zero, then there is no quality gap. 29
Statistical analysis
Data were collected using structured SERVQUAL and sociodemographic questionnaires. In this study, the reliability and validity of the questionnaire were examined. The Cronbach’s alpha was 0.934 and all items were valid. Data on the sociodemographic characteristics of the study populations were collected using a structured questionnaire. The SERVQUAL structured questionnaire assessed quality in counseling service in five dimensions: tangibility, reliability, responsiveness, assertiveness, and empathy (Table 1). In total, 22 statements were rated using a 5-point Likert-type scale, rated from 1 (strongly disagree) to 5 (strongly agree). The data were collected during the respondents’ entry and exit interviews. The questionnaires were completed in two ways. To assess the study participants’ expectations, the SERVQUAL questionnaire was completed by interviewing the participants before receiving services at the time of entry to the FP service room. An exit interview was conducted to complete a second SERVQUAL questionnaire and evaluate the participants’ perception of the services. Based on their communication skills with the clients, four BSc nurse professionals from each health facility were recruited for data collection. Two health officers were recruited as supervisors. The selected participants were informed by the data collector. Consent was obtained and data were collected from selected participants. During data collection, COVID-19 prevention techniques were applied.
Items under each dimension.

FP: family planning.
Of the questionnaires, 10% were pre-tested at the Kindo Koysha Woreda Camma health center before the actual data collection began. Further clarifications, relevance, and completeness of the instrument were then checked. The experts (two PhDs in philosophy) prepared the questionnaire in English, translated it into the local language (Wolaitato), and then translated it back into English to increase consistency. For 2 days, the study leader trained the data collectors and supervisors on instruments, data collection methods, ethical issues, and study goals. To ensure completeness and consistency, data collectors were closely supervised by supervisors during the data collection process. The study director monitored the correct implementation of the procedure and checked for completeness and logical consistency after data collection.
After checking the data for completeness and consistency, they were coded and entered into Epi Data 3.1. The data were exported to SPSS 25.0 for further analysis. A normality test was applied to determine the type of statistical analysis using the Kolmogorov–Smirnov test and histogram. Kolmogorov–Smirnov revealed that the p value of the data was 0.000, indicating that p < 0.05 and similarly the histogram showed that the data were skewed to the right. Both methods showed that the data were not normal. Therefore, the nonparametric tests were used to analyze the data. The median and the interquartile range (IQR) were determined for descriptive numerical variables. The Wilcoxon signed-rank test was used to compare median perception and expectation on another quality dimension, and the Friedman’s test was used to correlate the gap between the quality of counseling provision and respondents’ sociodemographic characteristics. A p value of <0.05 was taken as the criterion for statistical significance. Finally, the result was presented in a table and a pie chart.
Results
Sociodemographic characteristics of respondents
In total, this study’s participants included 391 women of childbearing age attending the FP Clinic, resulting in a 96.5% response rate. The mean age of the respondents was 29.0 years, with an IQR of 25–34 years. The majority of the respondents (58.3%) were between 15 and 30 years old and 112 (28.6%) had attended primary school. Regarding occupation, the majority of the participants, 235 (60%), were housewives. In this study, 227 (58.1%) participants had one to three children. The study also showed that 338 (86.4%) respondents were married. This study reported that the majority of the respondents (51.4%) received implant counseling, followed by injections (25.4%). Finally, 249 (61.6%) participants indicated that they were repeat users (Table 2).
Sociodemographic characteristics of the study participants at Bombe Woreda public health facilities in Wolaita zone, Ethiopia, 2021 (N = 391).

IUCD: intrauterine contraceptive device; ECM: emergency contraceptive methods.
Others—students, unemployed.
Others—widowed, divorced.
Contraceptive counseling service quality and its dimensions
This result indicates that the highest perception of the quality of contraceptive advice was observed in the dimension of tangibility (median value (IQR) = 3.25 (2.5–4.0)), followed by empathy (median value (IQR) = 2.20 (1.8–3.4)). Client perception assesses the remaining dimensions such as assurance (median (IQR) = 2.0 (2.5–4.0)), responsibility (median (IQR) = 2.0 (1.75–3.25)), and reliability (median (IQR) = 2.0 (1.6–3.6)), which were almost all the same and were registered as low (Table 3).
Dimension of the contraceptive counseling service quality median score for respondents’ perception and expectation at Bombe Woreda public health facilities, Ethiopia, 2021 (N = 391).

IQR: interquartile range.
With regard to expectation, the highest expectations for the quality of contraceptive advice were in terms of tangibility (median (IQR) = 5.0 (4.8–5.0)), reliability (median (IQR) = 5.0 (4.4–5.0)), responsiveness (median) observed (IQR) = 5.0 (4.25–5.0), and assurance (median (IQR) = 5.0 (4.25–5.0)); the lowest was empathy dimension (median (IQR) = 4.8 (4.4–5.0) (Table 2).
This study’s results showed that the counseling service that the clients received (perceived) was less than expected. The overall median difference in expectancy (median (IQR) = 4.73 (4.40–5.0)) and perception score (median (IQR) = 2.46 (2.07–3.09)) is presented in Figure 1.

Overall median score of the participants’ expectation and perception of the study participants.
The highest gap in counseling performance was related to reliability (median (IQR) = –3.25 (−4.0 to −1.75)) and the lowest gap in counseling performance was related to tangibility (median (IQR) = –1.75) (−2.25 to −0.75). The responsibility (median (IQR) = –2.52 (−3.25 to −1.5)), empathy (median (IQR) = –2.60 (−3.0 to −1.4)), and safety (median (IQR) = –2.50 (−3.25 to −1.0)) dimensions were classified accordingly (Table 3). This study reported that the overall QOCC service is low (SERVQUAL score = –2.27) and there was a negative gap in all dimensions of contraceptive counseling service (Table 4).
Overall gap score between the participants’ perception and their expectation at Boloso Bombe public health facilities, 2021 (N = 391).

The Wilcoxon signed-rank test found that compared to the expected score (median = 4.73, IQR = 4.4–5.0), the overall perception score (median = 2.46, IQR = 2.07–3.09) was significantly lower (p < 0.001, z = –16.3). The test also revealed that the perception score (median = 3.25, IQR = 2.5–4.0) of the tangibility dimension was significantly lower than the expected value (median = 5.0, IQR = 4.8–5.0, p < 0.001, z = –15.6). The perception value (median = 2.2, IQR = 1.8–3.4) of the empathy dimension was significantly lower than expected (median = 4.8, IQR = 4.4–5.0, p < 0.001, z = –15.8) (Table 3).
Association between overall service quality and sociodemographic characteristics
The Friedman’s test identified the association between sociodemographic variables and the overall QOCC services. While this test reveals general differences, it does not indicate which particular group is different from the other. All sociodemographic variables were shown as statistically associated with the overall quality of the counseling service. Respondent’s age (p < 0.001, χ2 = 385.00), number of living children (p < 0.001, χ2 = 381.04), marital status (p < 0.001, χ2 = 359.60), occupation (p < 0.001, χ2 = 379.00), type of contraceptive method counseled (p < 0.001, χ2 = 379.61), user type (p < 0.001, χ2 = 368.59), and educational status (p < 0.001, χ2 = 371.20) had a statistically significant correlation with the quality of counseling service (Table 5).
Association between sociodemographic characteristics and SERVQUAL score of the study population at Boloso Bombe public health facilities, 2021 (N = 391).

χ2: chi-square; df: degree of freedom.
Students, unemployed.
Divorced, widowed.
Friedman’s test (p < 0.001).
Comparing the quality of counseling service within each health facility
This study found that all healthcare facilities have negative gaps on all dimensions of service quality. Regarding the overall quality of counseling service, the quality of the QOCC was low in each healthcare facility: Bombe Primary Hospital (median = –2.38; IQR = –2.76 to −1.8), Zaba Health Center (median = –2.4; IQR = –2.8 to −2.11), Gammo Health Center (median = –2.37; IQR = –2.75 to −1.42), and Ose Health Center (median = –2.0; IQR = –2.4 to −0.95)) (Table 6).
Level of statistical features of contraceptive acceptors’ perception and expectation of counseling service quality in each facilities of Boloso Bombe Woreda, southern Ethiopia (N = 391).
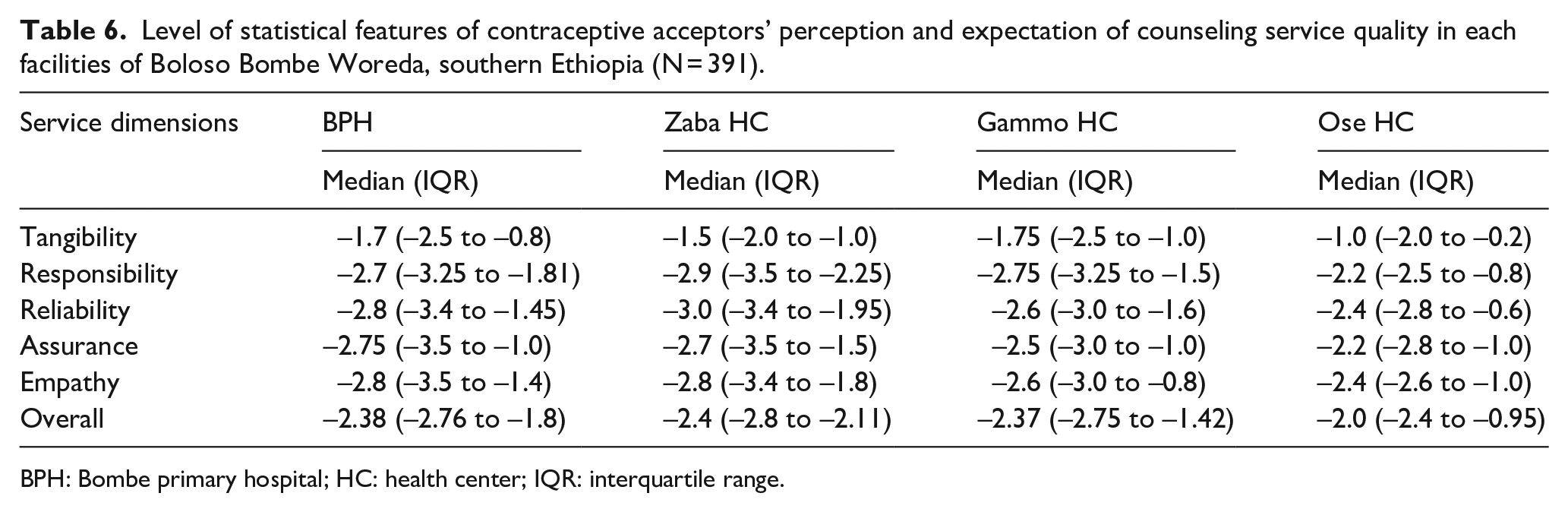
BPH: Bombe primary hospital; HC: health center; IQR: interquartile range.
Discussion
This study used the SERVQUAL model to assess the quality of counseling among contraceptive users. The model was built by Parasuraman et al., 33 who introduced five measurements/dimensions of service quality, such as tangibility, reliability, empathy, responsiveness, and assurance. The SERVQUAL scale is outstanding and is the most commonly used tool for assessing client preferences and their expectation of service quality. 34
According to this study, the overall quality of the counseling service was low (SERVQUAL score = –2.27). All quality dimensions of the counseling service had negative gaps. This indicates that the respondents’ expectation of contraceptive counseling was higher than their perception. Therefore, all Boloso Bombe public health institutions must pay particular attention to the quality of the counseling services provided and strive to provide quality counseling overall. This study was similar to the studies conducted in the different parts of the countries;7,29,32,35 however, it contradicted the studies conducted in Poland 24 and Nigeria. 36 A possible explanation for this inconsistency could be inequality in facility structure, provider training and experience, and sociodemographic characteristics. The purpose of the reliability dimension is to check that the counseling service is performed effectively and accurately. 30
The results of this study indicate that participants had very high expectations (mean score = 4.73) of the quality of counseling compared to their perception (mean score = 2.46). This suggests that clients expected twice as much quality of counseling as they perceived. This could be due to the modernization of the world, making it easier for clients to access health information from media, radio, and healthcare providers. In addition, the expansion and improvement of healthcare in Ethiopia can contribute to high expectations for healthcare services.
Reliability is the ability to deliver promised services effectively and accurately. 30 A reliable provider is one who continuously meets client requirements. Reliability also relates to a provider making an effort to solve a client’s problem, should one arise. The provider must be able to offer adequate service and satisfy the client’s right from the start. For planned interventions, the service provider must be able to deliver as required. 37 In this study, the highest advice quality gap was found in the dimension of reliability (median value = –3.25). This was consistent with the study conducted in Ghana, 27 Zanjan, 38 and Malaysia, 39 but not with the study conducted in Turkey, 40 Nigeria, 35 Golestan, 32 Poland, 24 and Iran. 4 The reason for the largest gap in reliability, as a distinct dimension, was that the counselor rarely promised, implicitly or explicitly, to do anything for FP users. As such, fulfillment of promises is an expectation remote from the client. 7 Therefore, healthcare providers should improve the reliability dimension, which is one of the most important areas that require special attention.
Specifically, healthcare facilities need to ensure that the equipment used meets client needs and is modern, even when staff are hygienic or pleasant and when the healthcare facility is attractive, which increases the quality of healthcare.34,37 This study found that the smallest gap in counseling service was related to the dimension of tangibility (median = –1.75), consistent with previous studies.27,36 This could be related to improving the establishment of health facilities, the organization of health education, and the quality of care in Ethiopia. As the dimension of tangibility has a significant impact on those seeking counseling, maintaining good physical health is crucial; 28 however, it still needs some improvements.
Regarding responsiveness, the service provider must be able to tell users what time they will be served or supported. The client needs to be served quickly and the hospital should respond to their requests as quickly as possible. 37 The study showed that the responsiveness dimension was observed as a negative gap (median = –2.52). This is consistent with the study conducted in Ghana. 27 Previous studies conducted in Sarawak 5 and Arak found that the highest gap in health care quality is related to the responsibility dimension. This could be explained by the service providers’ lack of interest in helping their clients and providing timely advisory services; they did not know exactly when to offer services to the user. However, findings from Poland showed a positive value. 37 The inconsistency could be explained by the fact that the provider offers fast and uninterrupted service, is always ready to deliver the service, and is cooperative with a user. Counselors are expected to work more on this dimension; otherwise, they risk abandoning and dissatisfying clients of FP services. This, in turn, leads to unwanted pregnancies or has a significant impact on the high birth rate.
The quality of healthcare services is influenced by the dimension of assurance, which encompasses the skills, knowledge, and confidence of healthcare providers in delivering services. 30 Therefore, healthcare providers should be careful when advising their clients. Healthcare workers are consistently well-mannered, they are well-trained to help clients in any situation, and clients feel comfortable communicating with service users. 37 The assurance concerns the behavior of the adviser that affects the trust of the service users. 34 The study found a negative gap (median = –2.5). This result is similar to studies conducted in Arak, 4 Mashhad, 28 and Sanandaj. 29 In contrast to this study, findings from Poland showed a positive mean value for this dimension. 24 This inconsistency could be explained by good knowledge of providers and trust and confidence in health professionals when delivering services. To provide quality advice, advisors should keep clients updated regarding the advancing health care services.
The empathy dimension indicates that every client deserves personal attention; they must experience consideration and kindness from the service provider; the service provider takes care of client needs and is aware of the clients’ interests. 37 The goal of this dimension is to pay attention to clients and respond to their requests. 30 Despite this, this study’s results showed a negative gap in the empathy dimension (median = –2.60). This is in line with the studies conducted in Mashhad 28 and Iran. 32 In contrast, cross-sectional studies from Poland 24 and Ghana 27 found a positive value in this dimension. This inconsistency could be explained by good knowledge of providers and trust and confidence in health professionals when delivering services. As counselors, every healthcare provider should be on behalf of the client. This plays an important role in improving the quality of counseling and client satisfaction.
The Wilcoxon signed-rank test revealed a statistically significant difference among all counseling service dimensions in terms of perception and expectation (p < 0.001, z = –16.3). Therefore, there was a gap between the FP attendants’ expectations and perception of the QOCC service in the facilities. In agreement with this study, evidence from Sanandaj, 29 Mashhad, 28 and Kermanshah 5 indicates that the difference between the mean score of perception and expectation for all dimensions and the overall mean score of expectation and perception was statistically significant (p < 0.05).
The Friedman’s test showed a statistically significant correlation between sociodemographic variables and the overall quality of the counseling service (p < 0.05). Thereafter, all sociodemographic variables were statistically significant with the overall quality of the counseling service. Respondent age (p < 0.001, χ2 = 385.00), number of living children (p < 0.001, χ2 = 381.04), marital status (p < 0.001, χ2 = 359.60), type of birth control method (p < 0.001, χ2 = 379.61), user type (p < 0.001, χ2 = 368.59), occupational status (p < 0.001, χ2 = 379.00), and educational level (p < 0.001, χ2 = 371.20) had a statistical significant correlation with service quality. Consistent with this study, a study conducted in Zahedan found a statistically significant association between respondents’ age and educational level and service quality (p < 0.05). 5 In contrast, findings from Mashhad 28 and Sanandaj 29 indicated no significant association between quality of service and sociodemographic variables (p > 0.05).
Some of the strengths of the study included the use of a strong sampling strategy and standard tool (SERVQUAL model) to assess counseling quality. In addition, because of the large sample size and the inclusion of all healthcare facilities, this study can be generalized to the entire population in the study area. One limitation of this study was using only patients’ perspectives to determine the quality of services provided. It is important to examine other providers’ perspectives on the quality of services because most patients do not fully understand the provider. Another limitation of this study was the use of a questionnaire to determine patients’ perceptions and expectations. Although the SERVQUAL questionnaire is valid and reliable, researchers cannot examine all dimensions of service quality with just one questionnaire. In this context, it is advisable to conduct some qualitative studies. Finally, data were collected before and after service delivery, which could lead to a social desirability bias. Therefore, future researchers should consider the observational data collection technique.
Conclusion
In general, the results show low quality of counseling service and negative gaps in all dimensions of counseling service quality in all health care facilities. This indicates that no healthcare facility included in this study met their clients’ expectations for the counseling service. All sociodemographic variables had a statistically significant connection with the quality of counseling. We found a negative gap in the dimensions of counseling service and recommended that counselors should provide counseling services when they promise to do so. As such, a provider should help clients to make informed decisions, provide appointment cards to the clients and let them know when they can return, ask the clients about their desire to have children and consistently be ready to help them in choosing the contraception method, and use visual materials to advise clients. The existing gap in the five dimensions of guidance service quality indicates that serious efforts are needed at all levels to improve the quality of guidance service. Therefore, in general, healthcare providers should improve the quality advice in every facility. In addition, other stakeholders, such as district health office, zonal, and regional health departments should supervise, monitor, and evaluate the quality of counseling in each health facility as well as organize training for the counselors.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231185407 – Supplemental material for Evaluating quality of contraceptive counseling using SERVQUAL model: A cross-sectional study in southern Ethiopia, 2021
Supplemental material, sj-docx-1-whe-10.1177_17455057231185407 for Evaluating quality of contraceptive counseling using SERVQUAL model: A cross-sectional study in southern Ethiopia, 2021 by Temesgen Geta Hardido, Tigistu Toru, Bizuayehu Atinafu Ataro and Tilahun Saol in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231185407 – Supplemental material for Evaluating quality of contraceptive counseling using SERVQUAL model: A cross-sectional study in southern Ethiopia, 2021
Supplemental material, sj-docx-2-whe-10.1177_17455057231185407 for Evaluating quality of contraceptive counseling using SERVQUAL model: A cross-sectional study in southern Ethiopia, 2021 by Temesgen Geta Hardido, Tigistu Toru, Bizuayehu Atinafu Ataro and Tilahun Saol in Women’s Health
Footnotes
Acknowledgements
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.