
Abstract
Background:
Emotion dysregulation is increasingly recognized as highly prevalent and impairing in autistic individuals. Yet, a large majority of studies have considered emotion dysregulation in youth only, and most of them did not consider sex differences in emotion dysregulation manifestation.
Objectives:
In the present study, we aim to investigate sex differences relative to emotion dysregulation in autistic adults without intellectual disability as well as its relationship with different factors potentially involved in emotion dysregulation (e.g. camouflaging, alexithymia, suicidality, quality of life). Self-reported emotion dysregulation will be assessed in autistic adults but also in females with borderline personality disorder, given that emotion dysregulation is particularly enhanced in this population.
Design:
Cross-sectional, prospective, controlled.
Methods:
Twenty-eight autistic females, 22 autistic males and 24 females with borderline personality disorder were recruited from a dialectical behavior therapy program waiting list. They completed several self-report questionnaires measuring emotion dysregulation, alexithymia, suicidality, quality of life, camouflaging borderline symptoms and autism severity.
Results:
Most emotion dysregulation subscale scores and alexithymia scores were heightened in autistic females compared to females with borderline personality disorder and, to a lesser extent, compared to autistic males. Independently of borderline personality disorder symptoms, emotion dysregulation was related to alexithymia and poorer psychological health in autistic females, whereas it was mostly related to autism severity, poorer physical health and living conditions in autistic males.
Conclusion:
Our results suggest that emotion dysregulation is a major difficulty of autistic adults without intellectual disability eligible for dialectical behavior therapy, and this is especially the case for autistic females. There seem to be different sex-specific factors involved in emotion dysregulation found in autistic adults, which highlight the need to target-specific domains (e.g. alexithymia) in the treatment of emotion dysregulation in autistic females. ClinicalTrials.gov Identifier: NCT04737707 https://clinicaltrials.gov/ct2/show/NCT04737707
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by early-onset social communication abnormalities and repetitive, stereotyped behaviors.1,2 The prevalence rate of ASD is approximately 1% worldwide, with a higher prevalence in males than females (in this article, we will use the terms “females” and “males” and not “men” and “women,” since our focus is on sex differences and not gender 3 ). 4 However, the male-to-female ratio in ASD has shown a consistent decrease over the last years. As an example, in a recent systematic review update from 2022, the median male-to-female ratio was estimated at 4:2, 4 whereas a systematic review published 5 years prior reported a male-to-female ratio at 4:1. 5 The higher rates of ASD among males reflect sex differences likely to be involved in its etiology but also in potential biases in clinical assessment and diagnoses.4,6,7
Recent research has highlighted a number of reasons for the underdiagnoses of autistic females. Most of them refer to “male-centric” aspects of diagnosis such as females having more socially appropriate special interests than males, or overall higher levels of social skills.6,8,9 In addition to neurocognitive and behavioral aspects, 10 cultural factors may also contribute to sex-based differences in ASD as there are greater expectations for females to engage in adaptive social behaviors. 11 This may, in turn, be involved in the enhanced use of compensatory behaviors to mitigate social challenges and mask autistic symptoms in autistic females.12–14 Indeed, while both autistic males and females without intellectual disability may hide or mask their symptoms to meet everyday social requirements and “look normal,” this has been reported to be more common in females than in males.13,15,16 The term camouflaging has been used in ASD to refer to the process by which individuals with ASD hide or mask symptoms that may be viewed as socially unacceptable and/or artificially perform social behaviors considered more acceptable.12,13
While short-term consequences of camouflaging might include decreased feelings of loneliness, a number of negative long-term consequences of camouflaging on mental health have been described. 17 In particular, increased self-reported camouflaging in autistic people without intellectual disability has been associated with higher depression and/or anxiety symptoms, but also increased suicidality, especially in females.17–21 Irrespective of camouflaging, however, autistic females have been reported to present more frequently with affective symptoms and suicidal behaviors,22,23 which has been mainly associated with elevated levels of emotion dysregulation (ED).24–29 Nevertheless, to our knowledge, the relationship between camouflaging and ED per se has not been investigated in autistic adults.
ED is defined as a deficit in adaptive and efficient emotion regulation that interferes with appropriate goal-directed behavior. 28 ED is a core symptom dimension found in a number of psychiatric and neurodevelopmental disorders, such as Attention Deficit Hyperactivity Disorder (ADHD), mood disorders and borderline personality disorder (BPD).30,31 Although ED is not considered to be disorder-specific, BPD is typically seen as the prototypical presentation of ED. 1 In addition to ED, BPD is characterized by a persistent pattern of unstable relationships and self-concept, associated with pronounced impulsive and self-harming behaviors. 1 ED in BPD is characterized by affective instability, uncontrolled anger and impulsive self-harming behaviors which are considered to be a maladaptive way of emotion regulation.31,32 Interestingly, using self-report and parent-report measures of ED, similar manifestations of ED have been described in youth and adults with ASD compared to typically developing (TD) individuals25,33–35 and youth with ADHD. 36 This, along with the growing awareness of the specific presentation of ASD in female adults, has increased the interest in the overlap between ASD and BPD, although research comparing ED in ASD and BPD is lacking. 37 In addition to the aforementioned manifestations described in BPD, ED in autism has been significantly linked to alexithymia38,39 and anxiety,25,40 both dimensions being particularly related to the core dyad of autistic symptoms.
Although ED is increasingly recognized as highly prevalent and impairing in autistic individuals, 41 a large majority of studies have considered ED in children and adolescents28,41–43 or autistic individuals with intellectual disability, 40 and most of them focused on males 43 or did not consider sex differences in ED manifestation. 44 Yet, in typically developing individuals, sex differences in emotion regulation abilities are well-known, as females are less likely to use adaptive strategies to regulate negative emotions compared to males. 45 This, in turn, is thought to be involved in the higher prevalence of depression, anxiety, BPD and eating disorders in females. 46
Irrespective of gender and sex differences, very few studies have investigated ED in autistic adults without intellectual disability. In one early study, Samson et al. 39 compared the scores of young adults diagnosed with ASD without intellectual disability to that of their TD peers on the Toronto Alexithymia Scale 47 and the Emotion Regulation Questionnaire. 48 The authors found that autistic adults had significantly more difficulties in both emotion labeling (i.e. alexithymia) and the use of effective emotion regulation strategies compared to TD individuals. In another study using self-report questionnaires, 49 the authors found that autistic participants used more maladaptive emotion regulation strategies (i.e. other-blame) and less adaptive strategies (i.e. reappraisal) compared to TD individuals. These results are consistent with those found by Cai et al. 50 using experience sampling methodology. The authors found that the use of maladaptive emotion regulation strategies (e.g. other-blame) significantly increased negative mood in autistic adults. Overall, despite the lack of studies focusing on ED in autistic adults, these results suggest that, akin to research conducted in autistic youth, ED is significantly increased in autistic adults compared to TD individuals, on the one hand, and that it has a significant impact on well-being, on the other hand.
Regarding the effect of sex on ED, research in autistic adults is lacking and only a few studies have been conducted in children and adolescents.44,51,52 The results of these studies converge in showing that ED is more severe in autistic girls than boys, a finding that is in line with those reported in TD children. 45 For instance, in the only study that focused on sex differences in ED in autistic individuals, Wieckowski et al. 44 reported in an inpatient ASD children and adolescent sample that ED was significantly increased in females compared to males. Moreover, the authors reported that, beyond sex, increased age and higher verbal ability were also associated with higher ED scores. This is all the truer for adult autistic females without intellectual disability, given that camouflaging has been reported to be more common in females than males, as well as mood and anxiety symptoms and suicidal behaviors.23,53 However, probably due to the underrepresentation of females in the research conducted in autistic adults without intellectual disability, gender and sex differences relative to ED in this population as well as its relationships with psychological dimensions and overall well-being have not been investigated thus far.
In the present study, we aim to investigate sex differences relative to ED in autistic adults without intellectual disability as well as its relationship with different factors potentially involved in ED in ASD (e.g. camouflaging, alexithymia, suicidality, quality of life). To do so, self-reported ED will be assessed in male and female autistic adults without intellectual disability, but also in females with BPD, given that ED is particularly enhanced in this population. We hypothesize that self-reported ED will be increased in autistic females compared to autistic males, and, in both groups, ED will be decreased compared to females with BPD. Moreover, we expect camouflaging, alexithymia, suicidality and measures of well-being (e.g. quality of life) to be associated with ED in both ASD groups independently of borderline personality traits.
Methods
Participants
The data used in this study were collected from 2019 to 2022 at the Psychiatric Unit of the University Hospital of Strasbourg, as part of a larger study on ED and dialectical behavior therapy (DBT). 54 Participants were enrolled because they presented with self-reported ED and were eligible for DBT. There were 85 participants originally recruited, with various primary conditions, that is, ASD, BPD, bipolar disorder (BD), ADHD and eating disorders. Given the goals of the study, we focused on a subset of emotionally dysregulated participants (N = 74), excluding patients with disorders other than ASD or BPD. Due to the small sample size of males with BPD in our study (N = 7), only females with BPD were included in the analysis. The final sample of 74 participants was categorized into three groups: women with a diagnosis of ASD (ASDf; N = 28; age, M = 29.51, SD = 8.01), men with a diagnosis of ASD (ASDm; N = 22; age, M = 31.64, SD = 10.85), and female patients with BPD (BPDf, N = 24; age, M = 27.50, SD = 7.16). Individuals with ASD did not present with BPD, and vice versa, with the exception of three individuals. These three individuals with ASD + BPD were included in the ASD group. However, other co-occurring disorders were observed in both groups (see Table 1). 55 Autistic participants completed all the self-report questionnaires, while participants with BPD completed all the questionnaires with the exception of the AQ, the CAT-Q, the BSS and the WHOQOL-BREF. Participants did not receive any financial incentive to participate in the study. Nevertheless, after they completed the questionnaires, they benefited from DBT, an empirically validated treatment for ED. 56 The current study is the preliminary step for a randomized controlled trial (RCT) on DBT being conducted as part of MEC’s PhD project that was approved by the regional ethics committee of the East of France (No. SI 21.01.21.41923). Therefore, because participants were included as part of another study, the calculation of the sample size was based on assumptions on the distributions of the DERS score made from the data from a pilot study conducted by our team. 27 A sample of 48 autistic participants was needed to demonstrate a decrease of at least 10 points of the score at mid-therapy compared to the baseline with a power of 95% and a decrease of at least 15 points post-therapy and at 6-month follow-up compared to baseline with a power of 91%.
Socio-demographic characteristics and health status.

Significant values are expressed in bold.
ADHD: attention deficit and/or hyperactivity disorder; ASD: Autism spectrum disorder; BD: bipolar disorder; BPD: borderline personality disorder; DSM: diagnostic and statistical manual of mental disorders; SD: standard deviation.
Missing data for n = 1.
Missing data for n = 2.
Missing data for n = 6.
Missing data for n = 4.
Measures
The Difficulties in Emotion Regulation Scale (DERS) 57 is a widely used 36-item self-report scale assessing ED. Items are grouped into six subscales: (a) nonacceptance of emotional responses (Non-acceptance; “When I’m upset, I feel guilty for feeling that way”); (b) difficulties in engaging in goal-directed behaviors when experiencing negative emotions (Goals; “When I’m upset, I have difficulty getting work done”); (c) impulse control difficulties when distressed (Impulse; “When I’m upset, I lose control over my behavior”); (d) lack of emotional awareness (Awareness; “I am attentive to my feelings”—reversed item) (e) limited access to effective emotion regulation strategies (Strategies; “When I’m upset, I believe that I’ll end up feeling very depressed”); and lack of emotional clarity (Clarity; “I have no idea how I am feeling”). Each item is scored on a Likert-type scale ranging from 1 (almost never) to 5 (almost always). Higher scores indicate greater impairment in emotion regulation. The current study used the French version of the DERS. 58 The DERS has been validated in ASD. 59
The Borderline Symptom List-Short Version 60 (BSL-23) is a 23-item self-report measure assessing BPD symptoms. In addition to the DSM BPD diagnostic criteria, items evaluate self-criticism, self-disgust, helplessness, loneliness and mistrust, with a total of 25 statements. Scores on each item range from 0 to 4 (the sum of the total score is divided by 23), and higher total scores indicate increased BPD symptom severity. Kleindienst et al. 61 defined six degrees of impairment: 0–0.3, none/law; 0.3–0.7, mild; 0.7–1.7, moderate; 1.7–2.7, high; 2.7–3.5, very high; and 3.5–4 extremely high. The BSL-23 has been validated in French. 62
The Beck Depression Inventory-2nd edition 63 (BDI) is one of the most widely used tools for assessing depression severity. This self-report questionnaire comprises 21 items with Likert-type scale responses ranging from 0 (not at all) to 3 (severely). Interpretation of scores recommend the following guidelines: 0–9, minimal depression; 10–16, mild depression; 17–29, moderate depression; 30–63, severe level of depression. The French version of the BDI has been found to be valid and reliable. 64
The Beck Anxiety Inventory 65 (BAI) is a 21-item self-report measure of somatic and cognitive anxiety symptoms. Participants score each item on a Likert-type scale ranging from 0 (not at all) to 3 (severely). The French version of the BAI has been validated in French. 66
The General Alexithymia Factor Score 67 (GAFS-8) is a subset of eight items of the Toronto Alexithymia Scale 47 developed to assess difficulty in identifying and describing emotions (alexithymia) in individuals on the autism spectrum. Items are scored on a five-point Likert-type scale (1 = strongly disagree; 5 = strongly agree). For the current study, the total score of the GAFS-8 was calculated by referring to the sum of responses to the items: 1, 2, 6, 9, 11, 12, 13 and 14 indicated in the French version of the TAS-20. 68
The Autism Spectrum Quotient 69 (AQ) is a self-report questionnaire designed to assess autistic traits. The 50 items reflect difficulties related to social and communication skills, imagination, attention to detail and attention-switching. Each score was grouped into one of two categories: yes (definitely agree or slightly agree); and no (slightly disagree or definitely disagree), with a value of 1 or 0. The sum of the scores was calculated across all questions, resulting in a total score ranging from 0 to 50. Higher total scores indicate higher levels of autistic-like traits. The French version of the AQ was validated by Lepage et al. 55
The Camouflaging Autistic Traits Questionnaire 70 (CAT-Q) is a self-report questionnaire of social camouflaging strategies in adults. The 25 statements relate to a three-factor structure consisting of the following strategies: (a) compensatory behaviors in social situations (Compensation, e.g. “When I am interacting with someone, I deliberately copy their body language or facial expressions”), (b) hiding autistic-like characteristics (Masking, e.g. “I adjust my body language or facial expressions so that I appear interested by the person I am interacting with”) and (c) attempting to fit in with others (Assimilation, e.g. “In social situations, I feel like I’m performing rather than being myself”). Items are scored on a 7-point Likert-type scale ranging from “strongly disagree” 1 to “strongly agree.” 7 The total CAT-Q score can range from 25 to 175, with higher values indicating increased use of camouflaging behavior. In this study, we used the French translation of the CAT-Q, whose psychometric properties are being assessed in a study led by our team.
The Beck Scale for Suicide Ideation 71 (BSS) is a 21-item clinician-rated scale evaluating suicidal thinking and intent. Each statement is scored on a three-point scale (from 0 to 2). Individuals are instructed to select the statement considered most applicable to them. The total score ranges from 0 to 38, with a higher score reflecting higher suicide risk. The BSS is validated in French. 72
The Abbreviated World Health Organization Quality of Life Questionnaire73,74 (WHOQOL-BREF) is a 26-item short version of the WHOQOL-100, 73 which provides a brief and adequate assessment of the following quality of life domains: (a) physical health, (b) psychological health, (c) social relationships, and (d) environment (e.g. financial resources, physical safety, home environment, transport). Items refer to the previous 2 weeks, participants respond on a 1–5 Likert-type scale, with higher scores indicating better quality of life. The mean score for each domain was multiplied by 4 and transformed into a 0–100 scale to enable comparisons with the scores used in the WHOQOL-100. 73
Procedure
After providing written informed consent, participants were requested to complete a brief form for socio-demographic variables, together with self-report questionnaires. The psychiatric status of participants was evaluated either by a clinical psychologist or a psychiatrist, based on the DSM-5 criteria. Prior to their recruitment, autistic participants had received a diagnosis of ASD, supported by the ADI-R and the ADOS-2. In addition, Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV) was administered to verify the absence of intellectual disability. In our sample, IQ scores were superior to 80 in autistic participants. Among the entire sample (N = 74), 29 participants (39%) presented one comorbid secondary disorder, 16 (22%) presented two comorbidities and 2 patients (3%) had three comorbidities. Detailed demographic information is found in Table 1. Our study followed the STROBE guidelines.
Statistical analysis
For this cross-sectional study, socio-demographic comparisons were performed between the three groups—ASDf, ASDm and BPDf corresponding, respectively, autistic female adults, autistic male adults and female patients with BPD—on the basis of chi-square (χ2) test for nominal variables. One-way analyses of variance (ANOVAs) were conducted to assess between-group differences in continuous variables. For these analyses, the significance level was set at p < 0.05 and was corrected using the Bonferroni post hoc procedure, controlling for multiple comparisons. Independent sample t-tests were performed to compare the mean scores between ASDf and ASDm on autism-related characteristics (e.g. AQ and CAT-Q) and quality of life (i.e. WHOQOL-BREF). Bonferroni adjustment for multiple comparisons was used. The Pearson coefficient was calculated to determine the correlations and partial correlations (controlling for borderline symptoms) between ED, clinical dimensions and well-being measures in the ASD groups. The listwise deletion method was used in the case of missing data. Statistical analyses were performed using SPSS Version 25 (IBM SPSS Statistics for Windows, Version 25.0.; Armonk, NY: IBM Corp).
Results
Socio-demographic characteristics
Table 1 summarizes the socio-demographic characteristics of the three groups. There were no differences between ASDf, ASDm and BPDf with respect to age distribution (F = 1.30, df = 2, p = 0.280), age at diagnosis (t = 0.42, df = 47, p = 0.966), professional (χ2 = 0.207, df = 4, p = 0.207) or marital (χ2 = 0.342, df = 4, p = 4.506) status. However, ASDf had higher educational levels (χ2 = 13.040, df = 6, p = 0.042), with 15 of them (54%) having completed at least a bachelor’s degree, compared to 4 ASDm (18%) and 4 BPDf (18%). In addition, there was a significant difference in the living situation status between subjects, as ASDf: n = 4 (14%) and BPDf: n = 1 (4%) were less likely to live with their parents, when compared to ASDm: n = 11 (50%). Moreover, ASDf had significantly more somatic disorders compared to ASDm. No other differences were found between groups in terms of health and socio-demographic characteristics.
Emotion dysregulation scores between groups
The three groups did not differ on the total score of the DERS (F = 1.98, p = 0.146; Table 2), but ASDf tended to have significantly higher scores compared to ASDm with a moderate effect size (t = 1.96, p = 0.056, d = 0.56); Table 3). On the subscale level, compared to BPDf, ASDf had significantly higher scores on the “nonacceptance,” “goals” and “strategies” subscales of the DERS (respectively, F = 7.24, p = 0.001, F = 5.18, p = 0.001, F = 34.46, p < 0.001). By contrast, BPDf had significantly higher scores on the “clarity” DERS subscale compared to both ASDf and ASDm (F = 42.81, i < 0.001). On the “impulse” and “awareness” DERS subscales, there were no differences between groups (F = 0.88, p = 0.420, F = 0.1.41, p = 0.252, respectively). Results were unchanged when patients presenting with ASD and co-occurring BPD were excluded from the analyses (N = 3).
Differences between groups on the DERS, the BSL, the BDI, the BAI and the GAFS-8.

Significant values are expressed in bold; p values refer to the ANOVA results.
BAI: Beck anxiety inventory; BDI: Beck depression inventory; BSL: borderline symptom list; GAFS-8: general alexithymia factor score; DERS: difficulties in emotion regulation scale; SD: standard deviation.
Significant values of post hoc comparisons including the three groups.
Differences between autistic groups on the self-report questionnaires.

AQ: autism spectrum quotient; BAI: Beck anxiety inventory; BDI: Beck depression inventory; BSL: borderline symptom list; BSS: Beck scale for suicide ideation; CAT-Q: camouflaging of autistic traits questionnaire; DERS: difficulties in emotion regulation scale; GAFS-8: general alexithymia factor score; SD: standard deviation; WHOQ: World Health Organization Quality. Significant values (p < 0.05) are expressed in bold.
Psychological and well-being dimensions
Regarding other psychological dimensions, ASDm had significantly fewer depressive symptoms compared to BPDf and ASDf (F = 3.15, p = 0.049), whereas alexithymia scores were lower in BPDf compared to ASDf (F = 7.75, p < 0.001). Compared to ASDm, ASDf had significantly higher scores on the CAT-Q (camouflaging) “assimilation” subscale (t = 2.32, p = 0.024) and on the AQ “communication” subscale (t = 2.03, p = 0.048). In other words, autistic females reported having greater communication difficulties and making more efforts to fit in compared to autistic males. In terms of quality of life, ASDf report having poorer physical health compared to ASDm (t = −2.17, p = 0.035). Results on other measures (borderline personality traits, suicidality and anxiety) were similar between groups (see Tables 2 and 3 for detailed results).
Correlation analyses
Results of correlation and partial correlation analyses are reported in Tables 4 and 5. In ASDf, DERS total score was positively correlated to increased depressive, borderline and anxiety symptoms, but also alexithymia score. In ASDf, greater ED was associated with poorer psychological health. In ASDm, a slightly different pattern was found as elevated ED score, measured by the DERS, was associated with increased suicidality, depressive scores, borderline symptoms and anxiety symptoms, but not with alexithymia. Regarding quality of life, higher levels of ED were related to poorer physical health and quality of the environment in ASDm. When controlling for borderline symptoms, higher ED scores remained significantly associated with increased alexithymia and anxiety symptoms in ASDf. In contrast, in ASDm, ED was related to increased autistic traits, and decreased quality of life in two domains: poorer physical health and environment.
Correlation matrix per group.
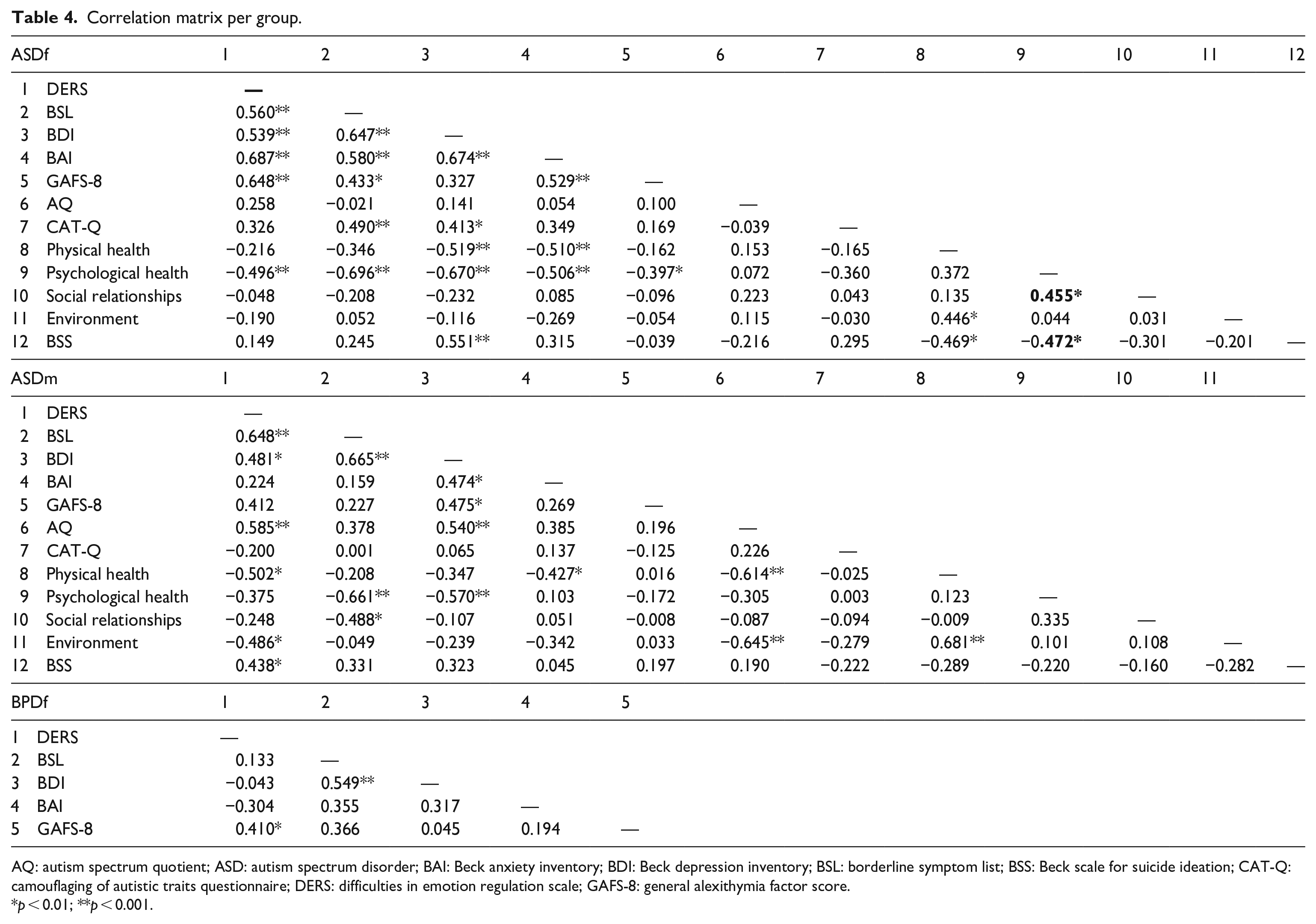
AQ: autism spectrum quotient; ASD: autism spectrum disorder; BAI: Beck anxiety inventory; BDI: Beck depression inventory; BSL: borderline symptom list; BSS: Beck scale for suicide ideation; CAT-Q: camouflaging of autistic traits questionnaire; DERS: difficulties in emotion regulation scale; GAFS-8: general alexithymia factor score.
p < 0.01; **p < 0.001.
Partial correlation between clinical measures and DERS, controlling for borderline symptoms.

AQ: autism spectrum quotient; BAI: Beck anxiety inventory; BDI: Beck depression inventory; BSS: Beck scale for suicide ideation; CATQ: camouflaging of autistic traits questionnaire; GAFS-8: general alexithymia factor score.
p < 0.01; **p < 0.001.
Discussion
The aim of the present study was to assess sex differences relative to ED in autistic adults in comparison to a control group of females with BPD. First of all, contrary to our predictions, female autistic adults presented with ED scores that were either higher (3 of the 6 subscales of the DERS) or comparable to that of females with BPD (with the exception of the “clarity” subscale of the DERS). In autistic males, however, ED scores were overall similar to those of females with BPD and tended to be lower compared to autistic females. This suggests that ED is particularly heightened in autistic females compared to autistic males, but also, surprisingly, compared to females with BPD. Moreover, we found that ED was mainly associated with alexithymia and psychological difficulties in autistic females, whereas in autistic males, ED was associated with the severity of autism, suicidal ideation as well as physical and environmental difficulties. Overall, these results suggest that ED is a major difficulty for autistic adults without intellectual disability, and this is all the more the case for autistic females.
Our results are consistent with previous research which found that ED was particularly marked in autistic adults without intellectual disability compared to TD individuals.39,49 Strikingly, our results suggest that many facets of ED are also particularly marked in autistic adults, especially females, compared to people with BPD. 75 More specifically, we found that the “nonacceptance,” “goals” and “strategies” subscale scores of the DERS were significantly elevated compared to BPDf. Although discrepant findings have been reported in the literature, probably due to the variety of methods used to measure ED, 76 these results are inconsistent with a number of studies which found that, although ED is not disorder-specific, higher DERS scores were specifically related to BPD. However, with the exception of one study 75 which focused on emotion regulation strategies used during interpersonal situations, none of these studies focused on the difference between BPD and ASD. As an example, in a study conducted on adolescents, the DERS total score, and the “impulse” and “strategies” subscale scores in particular, were found to be higher in inpatients with BPD compared to controls with other psychiatric disorders. 76 In another study conducted in adults with BPD and major depressive disorder (MDD), 77 the authors found that ED was significantly associated with BPD, as DERS scores were significantly increased in patients with BPD + MDD, compared to the group with MDD and healthy controls. Interestingly, in this study, only three DERS subscale scores did not differ between BPD + MDD and MDD groups: that is, “nonacceptance,” “goals” and “awareness.” This might suggest that nonacceptance of emotional responses and the interference of emotions with goal-directed behaviors are equally involved in ED in BPD and MDD.
By comparison, in our study, we found that “non-acceptance,” “goals,” but also “strategies” scores were significantly heightened in our sample of ASDf compared to BPDf. While these results are supportive of ED being particularly present in autistic females, 44 they also suggest that, compared to BPDf, ED is even more characterized by the non-acceptance of emotions, the lack of effective strategies to regulate them, and it highly interferes with goal-directed behaviors. Interestingly, these dimensions have been linked to a number of psychiatric disorders in nonautistic and autistic individuals (e.g. generalized anxiety disorder, depression, eating disorders).43,77-79 This supports the idea of ED as a transdiagnostic factor involved in the emergence and the maintenance of psychological difficulties independently of BPD comorbidity. 43 Consistent with these findings, in our study, we found that increased ED scores were related to poorer psychological health in autistic females, but not in autistic males. Relatedly, compared to autistic males, autistic females presented with increased self-reported communication difficulties, camouflaging and depressive symptoms compared to autistic males, a finding consistent with those from previous studies.17,80,81 Given the relationship between ED and psychopathology in people with disorders other than ASD, 56 but also in children and adults with ASD,40,41 it is likely that ED might play a role in the diminished psychological well-being reported by autistic females. Indeed, since ED is elevated in autistic children and seems to be a predisposing factor for a number of psychological difficulties in adulthood, 43 it is possible that ED might be a predisposing factor for depression, especially in autistic female adults. However, it is also possible that there is a reciprocal relationship between ED, depression and diminished psychological well-being in autistic females.
Contrary to our predictions, we did not find any links between ED and self-reported camouflaging in ASDf and ASDm. However, consistent with one previous study by Hull et al., 16 the score on the “assimilation” subscale of the CAT-Q was higher in ASDf compared to ASDm. The “assimilation” subscale of CAT-Q taps into the behavioral strategies people use to better fit in with others (e.g. forcing oneself to interact by pretending or putting a performance). 70 Interestingly, “assimilation” has been found to mediate the relationship between autistic traits, thwarted belongingness and lifetime suicidality, 82 suggesting its key role in the interpersonal difficulties (e.g. feelings that social interactions are not natural or genuine and one has to pretend to fit in) and overall well-being in ASD. In our study, camouflaging was associated with increased borderline symptoms (and to a lesser extent with depressive symptoms), but not ED, in autistic females only. It is therefore likely that, rather than ED per se, in autistic females, camouflaging is more directly related to other symptoms of BPD, for example, the feeling of alienation due to interpersonal difficulties. It should be noted, however, that in the latest version of the International Classification of Diseases, 11th Revision (ICD-11), disturbances in the functioning of aspects of the self and/or problems in interpersonal functioning are the main diagnostic requirement shared by personality disorders, irrespective of the associated trait domain specifiers and the addition or not of the Borderline pattern. 2 This increasingly dimensional approach to personality disorders points to the need for investigating the specificities of ED, but also the functioning of the self and the social relationships, in ASD compared to personality disorders as a whole, through the use of instruments other than the BSL-23. 83
When BPD symptoms were controlled for, we found that heightened alexithymia and anxiety symptoms remained highly correlated with ED in autistic females but not in autistic males. Elevated anxiety scores, as measured by the BAI, have been associated with hyperarousal in a number of disorders. 84 Our results thus suggest that ED in autistic females is characterized by increased arousal/reactivity than it is in autistic males, consistent with Wieckowski et al.’s 44 results in autistic youth. Regarding alexithymia, while two recent meta-analyses have highlighted that alexithymia is particularly heightened in autistic people85,86 none have considered the effects of sex on this ability. Our results suggest that self-reported alexithymia is significantly increased in autistic females compared to females with BPD, even though alexithymia is also particularly heightened in the latter population. 87 These results contrast with the higher “clarity” scores of the DERS found in BPDf compared to ASD, suggesting that female participants with BPD have more difficulties understanding and labeling their emotions than autistic adults. As a matter of fact, these results may not be contradictory since alexithymia encompasses not only the identification of one’s own emotions, but also describing them, external oriented thinking and constricted imaginal processes. 88 It is therefore possible that the latter dimensions, which are more related to social relationships, are particularly impacted in autistic females. Interestingly, in our study, in both BPDf and ASDf, ED was associated with alexithymia, which has been linked to interpersonal and mentalizing difficulties, but also emotion processing abnormalities in both disorders.87,89–93
Our study is the first to show that alexithymia is particularly heightened in autistic females compared to females with BPD, on the one hand, and that it is associated with ED in autistic females, but not autistic males, on the other hand. The results concur with the growing awareness of the overlap between behavioral (e.g. interpersonal difficulties) and cognitive (e.g. theory of mind peculiarities) aspects of BPD and ASD without intellectual disability. 37 However, very few studies thus far have directly compared core dimensions potentially involved in this overlap. Since many facets of ED and alexithymia are more pronounced in female autistic adults compared to female patients with BPD, clinicians should consider these dimensions when designing tailored interventions for autistic females.90,94 This is particularly important given the relationship between alexithymia, ED, social difficulties and mental health in autistic adults, especially women.85,92
In autistic males, it is noteworthy that ED scores were mostly similar to those of BPDf and tended to be lower than those found in autistic females. Moreover, while ED in autistic females is particularly linked to alexithymia and poorer psychological health, in autistic males, ED was found to be related to the severity of autism, poorer physical health, increased suicidal ideation and environmental living conditions. While these results are consistent with the higher percentage of ASDm participants living with their parents compared to ASDf, they contrast with the fact that the ASDf group presented with more physical conditions than the ASDm group in our study. 95 These findings likely reflect challenges which are related to sex differences in ASD and might be differentially linked to ED in females and males. Taken together, these results suggest that ED is associated with alexithymia, poorer psychological health and probably more interpersonal difficulties in autistic females, whereas, in autistic males, autism severity (at the clinical and functional levels) seems to be particularly linked to ED. Based on these findings, it is likely that therapeutic interventions for ED in autistic females should target preferentially alexithymia and social relationships while in autistic males, and it should target the severity of autism and its functional impact on independent living.
Our study has a number of limitations. First, our participants were enrolled because they presented with self-reported ED and were eligible for DBT; hence, it is possible that our results cannot be generalized more broadly to all autistic adults without intellectual disability. However, ED has been reported to be particularly heightened in other samples of autistic youth and adults41,81 suggesting that these results are not limited to a specific sample of autistic individuals. Moreover, our control group (BPDf) also had self-reported ED and were eligible for DBT and, despite this, ASDf presented with overall greater ED and alexithymia compared to BPDf and ASDm. Second, because of the aforementioned selection bias (i.e. participants were enrolled as part of another study), the sample size is relatively small. Future studies should include larger samples of autistic adults and people with BPD recruited from the general population, to determine whether our results can be generalized more broadly. Third, in our study, we focused on sex differences, and it is likely that gender differences might also be involved in ED. 16 Future studies should investigate ED in gender-diverse autistic individuals, given the specific challenges they might encounter (e.g. camouflaging, discrimination, mental health) and their specific needs. Fourth, in our study, we focused on ED in ASD compared to BPD, based on the more categorical approach of the DSM-5 compared to the latest version of the ICD. Given that ED is also found in other subtypes of personality disorders (e.g. Kassee et al. 95 ), and that anankastic, detached and narcissistic trait dimensions have been found to be associated with ASD96–98 future studies should focus on the specificities of ED in ASD compared to other personality subtypes. Finally, we did not assess post-traumatic stress disorder symptoms, which are highly prevalent in BPDf and ASDf,31,95 although they are related to ED. 31 Future studies should consider the relationship between childhood adversity, trauma and ED in autistic adults, especially in females.
Conclusion
Our study is the first to show that ED is particularly marked in autistic females compared to autistic males eligible for DBT (i.e. presenting with self-harming behaviors and/or suicidal behaviors), but also female patients with BPD. Given the relationship between ED, self-harm, suicidality and overall well-being and quality of life, 27 it is of the utmost importance to better understand the determinants and manifestations of ED in autistic individuals, including sex and gender-related specificities, to tailor pertinent and individualized treatments.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231174763 – Supplemental material for Emotion dysregulation is heightened in autistic females: A comparison with autistic males and borderline personality disorder
Supplemental material, sj-docx-1-whe-10.1177_17455057231174763 for Emotion dysregulation is heightened in autistic females: A comparison with autistic males and borderline personality disorder by Luisa Weiner, Madalina Elena Costache, Doha Bemmouna, Juliette Rabot, Sébastien Weibel, Marine Dubreucq, Julien Dubreucq and Romain Coutelle in Women's Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.