
Abstract
PURPOSE:
Parenting a child with special health care needs (SHCN) is often stressful. This study aimed to measure and compare stress among mothers of children with (a) Autism Spectrum Disorder (ASD) - ASD group, (b) Developmental delay without ASD group, (c) SHCN without developmental delay group, and (d) Typically developing group. To assess factors associated with maternal stress in children with developmental disorders.
METHODS:
A cross-sectional analytical study was performed with children aged 2–12 years and their mothers. The study population was classified into four groups as defined above help of detailed history, developmental & behavioral assessments, psychological assessments, and Child Special Health Care Needs Screener (CSHCN). Parental Stress Scale (PSS) Questionnaire was administered. The main outcome measurement was the PSS and various factors affecting it.
RESULTS:
The mothers of the ASD group reported a high stress score (50.4±11.4) compared to SHCN without developmental delay group (38.2±8.8) and the Typically developing group (22.3±3.3) (p < 0.05) and higher but not significant stress than Developmental delay without ASD group (45.3±9.6, p > 0.05). Maladaptive behavioral issues and irregular interventions were the factors contributing to higher parental stress in the ASD group (p < 0.05). A moderate positive correlation was observed in rewarding and challenging scores of PSS among mothers of the ASD group, Developmental delay without ASD group, and SHCN without developmental delay group.
CONCLUSION:
Mothers of the ASD group perceived higher stress as compared to SHCN without developmental delay group and Typically developing group. Evaluation of stress and stressors is crucial for holistic management of ASD.
Introduction
Parenting is the process of understanding the physical, emotional, psychosocial, and intellectual development of a child from infancy to adulthood, and not just the biological relationship between parent and child [1]. Each parent, irrespective of their child’s characteristics, socioeconomic status, or other experiences, has parenting stress to some extent [2]. Parenting stress is defined as “a set of processes leading to aversive physiological and psychological reactions arising while parents attempt to adapt to the demands of parenthood.” This definition suggests that parenting stress involves parent and child factors, which invariably affect the parent-child relationship [2]. By definition, these feelings arise directly from the parenting role. This definition suggests that parenting stress involves parent factors as well as child factors. Looking at this, parent-child relationships can also be invariably affected by parenting stress.
Development is an essential aspect of childhood that harbingers the future of an individual. A developmental disorder affects both the child and the family. The stress of rearing a child with a developmental disorder can create a difficult home environment with stressful parent-child relationships. In the United States of America (USA), the prevalence of Autism Spectrum Disorder (ASD) has increased from 1 in 68 to 1 in 54 children in the last two decades [3]. The prevalence of ASD is reported to be as high as 1 in 65 in India [4]. The essential features of Autism Spectrum Disorder (ASD) are persistent impairment in reciprocal social communication and interaction and restricted, repetitive patterns of behavior or interests [5]. Maladaptive behavior like temper tantrums, aggression, and self-injurious behavior are often present in children with ASD. Sensory issues and self-adaptive skills (an ability that makes a child live independently) make routine care difficult to handle, along with the core deficits of ASD [6]. These maladaptive behavior, sensory issues, and self-adaptive skills, along with the core deficits of ASD, are some of the reasons for parental stress in families raising a child with ASD [6]. Also, unclear prognosis, maladaptive behavior, and low self-adaptive skills in the child add to the stress [7]. Parents of children suffering from chronic illnesses have varying levels of stress at the time of diagnosis, during the transition, during acute exacerbations of the illness, and during repeated hospitalizations [8, 9].
Studying distress among parents of children with ASD and other developmental disorders is vital. It is crucial to keep parents’ mental health in good shape for good care of children. An in-depth study of the same can give an insight into the factors responsible for the stress these parents experience. Once the reasons are identified, the issues can then be addressed as they can be medical, social, psychological, or personal. This area is underexplored in countries like India [10, 11]. In India, society still stigmatizes these disabilities. There is also no structured or designed referral system or recommendations, along with a lack of trained professionals in the field of developmental and behavioral pediatrics. The lack of insurance coverage for these interventions overwhelms many parents. Attempts to integrate and create an inclusive environment for their children are quite challenging in India [10]. Moreover, it is not very clear how the stress of a parent of a child with ASD stands in comparison to those with special health care needs like developmental delays, other neurological disabilities, and children with chronic illness. These comparisons can help understand the challenges parents go through. Studies are performed on parental stress in children with ASD in developed countries. However, the data from Lower Middle-Income Countries (LMIC), like India, is very limited. Considering the cultural differences and experiences, it needs to be explored.
Thus, the objectives of this study were; (1) To measure and compare the stress among mothers of children with (a) ASD, (b) Special health care needs (SHCN), including developmental, emotional, or behavioral problems other than ASD (children with other developmental problems), (c) SHCN without developmental problems and (d) Typically developing children without SHCN; (2) To assess the factors associated with maternal stress in children with developmental disorders in India.
Methods
A cross-sectional study was conducted from April 2018 to October 2018 at the Child Development and Guidance Clinic division of a tertiary care pediatric unit on parents of children from the age of 2–12 years. The project was approved by the Institutional Ethical Committee. Written informed consent was obtained from the mothers. Those having pre-existing mental health or other chronic illnesses were excluded to remove the confounding bias of over-reporting. Only those mothers who were able to read, understand, and write were included in the study (as shown in Fig. 1)
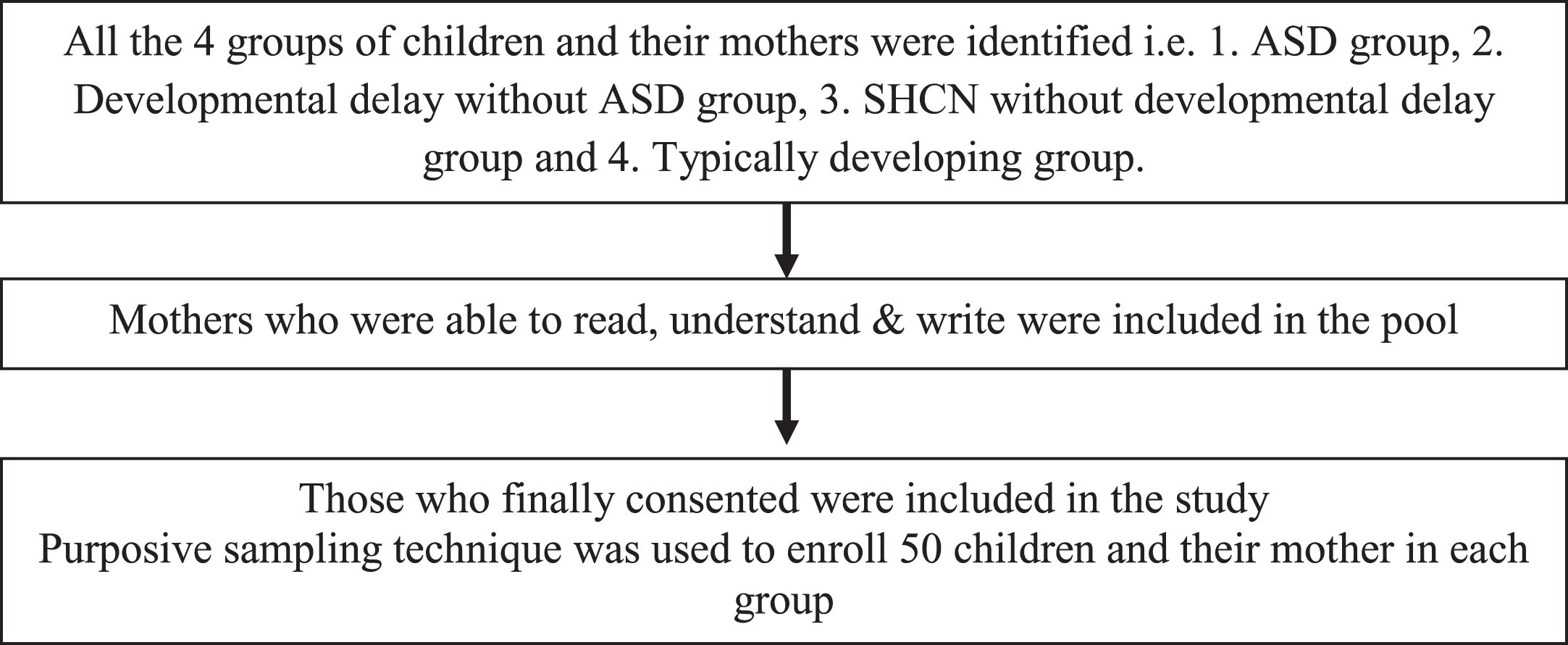
Case selection and enrolment in the study.
The study population was divided into four groups classified below ASD group: Children with ASD, diagnosed by validated tools, including INCLEN (INCLEN Diagnostic Tool for Autism Spectrum Disorder). INDT-ASD, which is an indigenously developed tool for the assessment of Indian children with ASD. This tool has been developed by the INCLEN group in India, and it is used by mental health professionals and pediatricians. It consists of two main areas. The first includes questions related to domains-social interaction & communication, and the second involves restricted interests with the concerns about sensory issues added with the onset in the early developmental period. It relates to scoring as well as arriving at a diagnostic classification [12, 13] based on the diagnostic criteria of DSM-5. Developmental delay without ASD group: SHCN with developmental problems other than Autism, SHCN without developmental disorders group: SHCN without developmental problems and having chronic illnesses like Type 1 Diabetes Mellitus or hemato-oncological disorders, Typically developing group: Children without SHCN, with typical development.
Procedure
Detailed history and demographic data, including age, gender, type of family (nuclear or joint), birth order, total siblings, and the modified Kuppuswamy method of socioeconomic classification [14] were noted. The modified Kuppuswamy scale is used to measure socio-economic status (SES) in urban and peri-urban communities. It is based on a composite score consisting of the education and occupation of the head of the family along with monthly income of the family. The study population is classified into high, middle, and low SES [14].
Before commencing the study, the PSS questionnaire was translated into the local language (Marathi) and back-translated into English. Internal reliability was tested using the test-retest reliability method on ten parents within five days (r = 0.78 and p = 0.034).
Measures
A Parental Stress Scale Questionnaire (PSS) [15] was administered to all the mothers, as in India, usually, the mother is the primary caretaker. It provides a measure of the positive (rewarding) and negative (challenging), ‘stressful’ aspects of parenting. It is an 18-item self-report scale. Items represent rewarding (e.g. emotional benefits, personal development) and challenging (demands on resources, restrictions) themes of parenthood. It is a 5-point Likert scale (disagree to agree). To compute the total score, the rewarding questions were scored reversely (Hence, it is important to understand that low rewarding scores mean parents are more positive about their child). The item scores were then summed up with a final score in a range of 18–90. Hence, a final low score signifies a low level of stress, and a high score signifies a high level of stress.
Groups 2, 3 & 4 were assessed with the CSHCN (Child Special Health Care Needs) Screener [16].
CSHCN is a screener to identify children with chronic physical, developmental, behavioral, or emotional conditions and also requires other health-related services beyond those generally required by children [16].
The CHSCN screener questionnaire includes questions on five health care consequences: (1) need/use prescription medications (except vitamins); (2) need/use more medical, mental health, and education services than most same-aged children; (3) limited/prevented inability to do things than most same-aged children; (4) need/get special therapy such as physical, occupational, or speech; (5) have any kind of emotional, developmental, or behavioral problem for which treatment or counseling is needed. A child was classified as having SHCN [16] if the parents acknowledged any of the five health care consequences and two follow-up questions: whether the consequence was because of a medical, behavioral, or other health condition and whether that condition lasted for 12 months.
Other psychological assessments were used in the study to tailor the needs of a child with developmental and behavioral disorders. All groups were chosen with the purposive sample method, therefore all were equal in number at 50.
In the ASD group INDT-ASD/ ISAA, the Vineland Social Maturity Scale (VSMS) [17], for the evaluation of social and adaptive functions or social maturity of the child, SQ was performed (a score < = 70 was considered deficit). Behavioral assessment was done with the help of the Child Behavioral Check List (CBCL) [18], 113 item questionnaire to assess behavior and emotional problems in children. In the Developmental delay without ASD group: VSMS and CBCL were used.
A delayed speech and language diagnosis was given by a speech and language pathologist after evaluation. A child was considered to be receiving regular interventions if they attended at least one hour per day per week of structured interventions for one year [19]. Comorbidities of seizure disorder, sleep disturbances, and dysmorphism were evaluated based on a detailed history and evaluation.
Statistical analysis
All data were entered in Microsoft Excel 2016 and analyzed using IBM SPSS25. The mean and standard deviation were used to express the data. An appropriate statistical test was performed, including ANOVA, to compare the parental stress among different groups and an unpaired student’s T-test was used to study factors affecting stress among parents. Spearman’s correlation analysis was performed on the rewarding and challenging scores of PSS in each group. The p-value <0.05 was considered significant.
Results
A total of 200 children and their mothers (126 boys and 74 girls) were enrolled and analyzed in the study, 50 in each group. The mean age of the study population was 5.4±2.1 yrs. The basic demographic data of all four groups are shown in Table 1. There was no statistical difference observed in any of the groups because of any of the demographic or socio-cultural data.
Demographic data of the study, mean composite PSS score, rewarding and challenging scores with SD scoring in the comparison groups (*ANOVA test p < 0.05)
Demographic data of the study, mean composite PSS score, rewarding and challenging scores with SD scoring in the comparison groups (*ANOVA test p < 0.05)
On ANOVA analysis, the PSS score was significantly different between the groups (p = 0.0001). Post-hoc analysis revealed that the ASD group had a higher stress score as compared to other groups (p = 0.0001) except for the Developmental delay without the ASD group (p = 0.203). The Developmental delay without ASD group had higher stress scores as compared to the SHCN without developmental delay group (p = 0.004) & the Typically developing group (p = 0.0001). The SHCN without developmental delay group had higher stress scores than the Typically developing group (p = 0.0001) (Fig. 2).
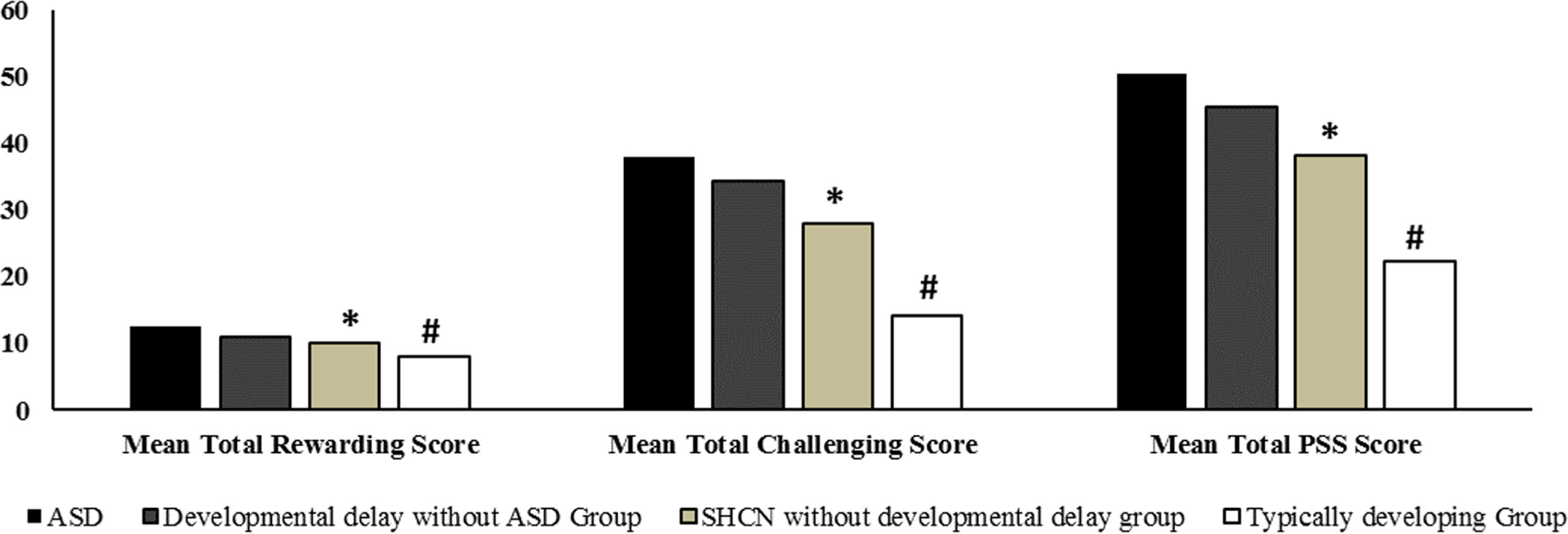
Comparative mean PSS, rewarding and challenging scores in different groups with its significance; (*p < 0.001 when comparing all the groups individually with SHCN without developmental delay group, #p < 0.001 when comparing all the groups individually with Typically developing group).
The mean challenging scores were in the following order: ASD group > Developmental delay without ASD group > SHCN without developmental delay group > Typically developing group. In the ASD group and Developmental delay without ASD group, mothers reported majorly increased stress due to: worry whether doing enough for the child; caring for the child takes more time and energy; being overwhelmed by the responsibility of being a parent. In SHCN without developmental delay group, concern about financial burden was higher. The challenging scores of different items observed in the four groups were statistically different from one another (Table 2). The mean rewarding scores were in the following order: ASD group<Developmental delay without ASD group<SHCN without developmental delay group<Typically developing group. The majority of the mothers affirmatively reported doing everything for the child; closeness with the child; enjoying spending time with the child, and the child being an important source of affection. The scoring observed in all these questions from the four groups was not statistically different from each other (Table 2).
Mean PSS score with respect to the rewarding and challenging questions of the scale. Expressed as Mean±SD
There was a moderate positive correlation observed in the rewarding and challenging scores of PSS of the ASD group (R = 0.473, p = 0.008). This implies that if the rewarding score was low, there is a high likelihood of challenging scores also being low (please note that the rewarding questions are to be scored in a reversed way, so the mothers who are having a more challenging theme of motherhood about their children are having a less rewarding theme of motherhood towards them). Similar correlations were found in the developmental delay without ASD group (R = 0.411, p = 0.024) and the SHCN without developmental delay group (R = 0.421, p = 0.026), but not in the Typically developing group (R = 0.249, p = 0.185) (Table 3).
Correlation Analysis of Rewarding and Challenging Scores of PSS among all the groups
Among the ASD group, behavioral issues were observed in 42 (84%) children, whereas 8 (16%) had no behavioral issues. Maternal stress in children with ASD group was higher in those with behavioral issues as compared to those who did not have behavioral issues (p = 0.039). In the ASD group, mothers whose children were on regular interventions had a lower PSS score as compared to those who were not on regular interventions (p = 0.012) (Fig. 3a and 3b). There was no difference observed in the PSS in the ASD group for inadequate social maturity of child (VSMS score < = 70), delayed speech, presence of co-morbidities along with ASD, and different duration of illness in the children (p = 0.343).
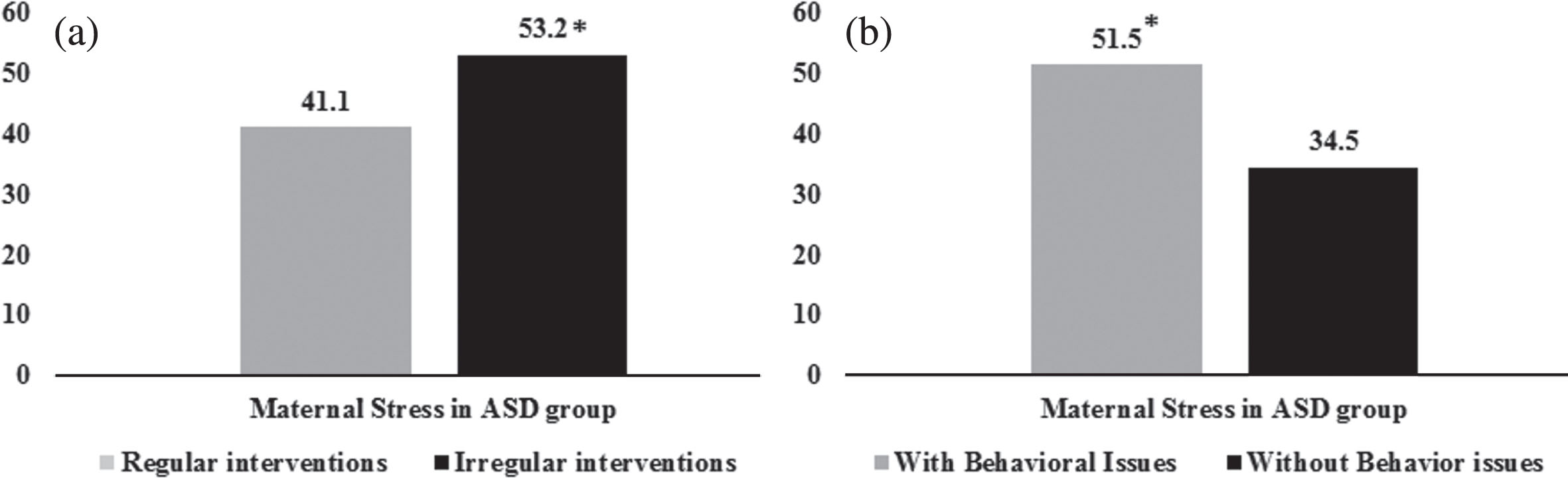
(a) Maternal Stress in children with ASD for behavioral issues in children (*p < 0.05). (b) Maternal Stress in children with ASD for regularity of interventions (*p < 0.05).
Among children with other developmental disorders with SHCN, no statistical differences were observed in PSS on the grounds of maladaptive behavior in the child (p = 0.664) or inadequate VSMS score < = 70 (p = 0.202).
The results show higher stress among mothers of children with SHCN as compared to other children without SHCN. Among all four groups, the ASD group reported higher stress. This higher maternal stress among the ASD group was associated with behavioral issues and irregular interventions among children. The strength of this study is the focus on the rewarding aspect of the mother-child relationship helping in making a ‘family-centered approach’ for interventions. The study of rewarding and challenging aspects of the mother-child relationship, maternal stress, and stressors was attempted. Further, four different groups- three groups belong to a variety of disorders reflecting maternal stress in different situations, and a typically developing children group serves as a control in the Indian setting were studied. The need to conduct such studies in India, where disability is neglected by society and mothers are overwhelmed without essential support systems was already highlighted. The limitations are a modest sample size, though four broad groups were attempted to be covered. Parental stress of only mothers was reported in the study, considering them as the primary caretaker of the child in India. Parenting styles, resilience, and more details on parents could have been obtained. This observation is from a single center. Similar reports from other Indian centers might help to support these observations.
The mean PSS in another study using the same tool [11], where the parents of children with ASD, Specific Learning disabilities, and children without any psychiatric disorder were analyzed, had scores similar to those in this study. The mean score was significantly higher in parents of children with ASD than in the other two groups. Similar observations were also made from studies worldwide [11, 21]. It is reported that parents of children with Autism were more likely to score in the high aggravation range (55%) than parents of children with developmental problems other than ASD (44%), followed by those with SHCN without developmental problems (12%), and least by parents of children without SHCN (11%) [22]. The reasons for higher stress observed in the ASD group are possibly due to unique challenges related to the characteristics of such children as compared to other developmental disabilities. ASD, which is considered an invisible disability without any physical impairment, leads to significant distress in families [7]. Higher levels of distress are reported in the presence of problem behaviors and impaired adaptive functioning-commonly observed in other developmental disabilities but are observed at a higher degree in children with ASDs [7]. Maternal stress in Developmental delay without ASD group may be due to maladaptive behavior, lower self-care and adaptive skills, emotional disturbances in children, and the need for specialized care [23].
The rewarding aspects reveal the pleasant and rewarding experience felt by the mother, which was seen in 90% of mothers in the ASD group. From the observations, it seems that despite substantial stress, mothers do report a rewarding perception of their relationship with their children. These findings are consistent with previous observations [24, 25]. This aspect of parenthood can help guide coping strategies and offer support to the parents. However, mothers in the ASD group were less optimistic about the future and their role and less satisfied as parents, which have been previously reported [24, 26]. Mothers in India are not only the primary caregivers for their children but also the entire family and household chores. Due to such overwhelming responsibilities, they are probably affected a lot.
In the ASD group and the Developmental delay without ASD group, mothers reported higher stress mainly due to: worry about doing enough for the child; caring for the child requiring more time and energy; responsibility of parenthood. These findings are in line with the previously reported studies [22, 26]. However, in the SHCN without developmental delay group, the concern of financial burden was higher, and, with an uncertainty of the illness course, concerns about the prognosis or complications related to illness were sources of maternal stress [8, 9]. This may be due to the lack of insurance coverage for the above illnesses. The positive correlation between rewarding and challenging PSS scores may be due to strong negative emotions interfering with the motivational aspects of parenting and the cognitive appraisal of caregivers. Hence, mothers perceive their children less positively or suppress their positive emotions towards them [27].
In the ASD group, the mean PSS observed among those having behavioral issues was significantly higher than children without them. It has been suggested that maternal stress increases with behavioral issues in children with ASD [20, 21]. Also, it is reported that a child’s behavior is the most important predictor of parental stress [7]. The vicious cycle of a child’s behavior leads to parental stress, and the inappropriate reactions of parents reinforce the development and persistence of behavior problems, which in turn elevates parental stress [28]. Mean PSS in the ASD group with irregular interventions was higher. This may be due to the lack of availability or not seeking professional support, either formal (interventions by therapists and professionals) or informal (social or family support), leading to elevated parental stress and affecting the overall child’s functioning [29]. There was no difference reported in PSS with inadequate social maturity of the child, delayed speech, presence of co-morbidities along with ASD, and different duration of illness in the children, which is consistent with the previously reported findings [30, 31].
No differences were observed in stress among mothers in the Developmental delay without ASD group with the presence of maladaptive behavior or inadequate adaptive skills of a child. There is conflicting evidence on whether a child’s poor adaptive skills lead to increased parental stress [30, 32]. The findings of the study could be attributed to the fact that the majority of children with developmental delay who did not have ASD were receiving regular interventions and cognitive evaluations from their caregivers. The children fulfilling CSHCN criteria (condition lasting for at least 12 months) were only included in the group, so it will be difficult to comment on parental stress due to maladaptive behavior at the time of diagnosis.
Conclusion
Mothers of children with a developmental or behavioral disorder, ASD in particular, perceive higher stress as compared to mothers of children without the developmental disorder. The combination of maladaptive behavior in the child and irregularity in follow-up for evidence-based interventions contributes to elevated stress in mothers of children with ASD. Despite substantial stress in mothers of children with ASD, they report a rewarding mother-child relationship. Evaluation of stress and stressors in mothers of children with developmental disorders is vital. Steps towards improving maternal stress could also enhance their capacity to provide adequate care for their children and might lead to better outcomes for the whole family. The study is very crucial for LMIC like India due to certain reasons. In India, the priority is given to acute illnesses over chronic neurodevelopmental disorders. A heterogeneous population of doctors serves these children, therefore lacking proficiency to cater to their special needs. Also, the lack of insurance coverage for families with children with neurodevelopmental disorders and limited awareness among parents and society are hurdles in executing the optimum standard of care for developmental disorders. There is unmet need to give optimum care to families with SHCN in India. It may be provided through a multidisciplinary standard of care in management and reinforcing parental support.
Footnotes
Acknowledgments
We are thankful to the children and their mothers who participated in the study
Conflict of interest
The authors have no conflict of interest to report
Funding
No funding was received for the study