
Abstract
Objective:
This study was done to determine the overall estimate of decision-making autonomy on maternal health services and associated factors in low- and middle-income countries.
Method:
PubMed, Science Direct, Google Scholar, Scopus, and the Ethiopian University online library were searched. Data were extracted using Microsoft Excel and analyzed using STATA statistical software (version 14). Publication bias was checked by forest plot, Begg’s rank test, and Egger’s regression test. To look for heterogeneity, I2 was computed, and an overall estimated analysis was carried out. Subgroup analysis was done by country, year, and publication. Joanna Briggs Institute quality assessment tool was used to check the quality of each study. We carried out a leave-one-out sensitivity analysis.
Results:
Out of 1305 articles retrieved, 19 studies (with 104,871 study participants) met eligibility criteria and were included in this study. The pooled prevalence of women’s decision-making autonomy on maternal health services in low- and middle-income countries was 55.15% (95% confidence interval: 44.11–66.19; I2 = 98.6%, P < 0.001). Based on subgroup analysis, decision-making autonomy in maternal health services was the highest in Ethiopia at 61.36% (95% confidence interval: 50.58–72.15) and the lowest in Nigeria at 36.16% (95% confidence interval: 12.99–43.39). It was 32.16% (95% confidence interval: 32.72–39.60) and 60.18% (95% confidence interval: 47.92–72.44) before and after 2016, respectively. It was also 54.64% (95% confidence interval: 42.51–66.78) in published studies and 57.91% (95% confidence interval: 54.80–61.02) in unpublished studies. Age (adjusted odds ratio = 2.67; 95% confidence interval: (1.29–5.55), I2 = 90.1%), primary level of education (adjusted odds ratio = 1.75; 95% confidence interval: (1.39–2.21), I2 = 63.8%), secondary education level (adjusted odds ratio = 2.09; 95% confidence interval: (1.32–3.32), I2 = 87.8%), being urban resident (adjusted odds ratio = 1.80; 95% confidence interval: (1.22–2.66), I2 = 73%), and monthly income (adjusted odds ratio = 3.23; 95% confidence interval: (1.85–5.65), I2 = 97%) were positively associated with decision-making autonomy on maternal health service.
Conclusion:
Decision-making autonomy on maternal health services in low- and middle-income countries was low. Sociodemographic factors also influenced it. Educational accessibility and income generation should have been recommended, enabling women to decide for themselves.
Introduction
More than 50% of maternal and infant deaths still occur within the first day after birth, which is particularly high in low- and middle-income countries.1,2 According to reports, 800 women worldwide die every day as a result of complications related to pregnancy, and 99% of these deaths take place in low- and middle-income countries. 3 Low utilization of maternal health services in low- and middle-income countries has been associated to these poor maternal health outcomes. 4 Nearly two-thirds of maternal deaths worldwide are caused by unsafe abortion, hemorrhage, eclampsia, and obstructed labor, which are also the major causes of maternal mortality in middle-income countries. These deaths can be averted by providing women with the antenatal care, skilled birth attendant, and postnatal care that are considered to be important maternal healthcare services.5–7
Emergency obstetric care has also been suggested as a strategy that has significantly reduced maternal mortality rates worldwide since 1990. 8 These fall under the category of basic and comprehensive emergency obstetric care. Basic emergency obstetric care includes the removal of retained products, manual removal of the placenta, assisted vaginal delivery, and the administration of intravenous antibiotics, injectable anticonvulsants, and intravenous uterotonics. Blood transfusions and cesarean sections are part of comprehensive emergency obstetric care. 9
By 2030, the Sustainable Development Goals of the United Nations set a target for maternal mortality to reduce to less than 70 deaths per 100,000 live births and to ensure that all women have access to sexual and reproductive healthcare. 10 The World Health Organization also suggested that maternal health services could prevent the majority of maternal deaths. 11 The gender power relations have been explained in terms of a woman’s lack of access to and control over financial resources,12–15 lack of decision-making power,16,17 constrained gender norms,18,19 lack of “women-centered” reproductive health services,20–22 and disrespect and abuse of women by healthcare professionals during their pregnancies,23–25 all of which have had a negative impact on maternal health care services. Poor maternal health outcomes are a result of women’s limited decision-making capacity and gender power disparities that affect maternal health decisions and access to reproductive health services contributes to poor maternal health outcomes. 26
Women in low-income nations have little control over household finances and little say in medical decisions, despite an increase in women’s autonomy in maternal health care.27,28 Women’s autonomy is the capacity for women to make decisions about their health, freedom of movement, and financial management without seeking approval from others. 29 The ability of women to make their own health decisions is crucial for improving maternal and child health outcomes, and this ability is directly associated with the women’s household wealth child health outcomes.30,31 Women’s capacity to make independent healthcare decisions is a precondition for their opportunity to access maternal health care services.32–34 To improve mother and child health outcomes, women’s autonomy in making health care decisions is fundamental. 35
Several works of the literature revealed that women’s decision-making autonomy is positively associated with the use of maternal health services and improvement of maternal morbidity and mortality,27,29,36–43 In contrast to this, a study done on 31 Sub-Saharan African countries results revealed a weak relationship between women’s autonomy and the utilization of maternal healthcare services. 44 In addition to this, a study conducted in Bangladesh showed that women who either decided alone or jointly with their husbands were less likely to utilize maternal health services. 45
The prevalence of women’s autonomy in maternal health services has ranged from 21.9% in Ghana 43 to 82.4% in India. 46 There are no data on the proportion of women’s autonomy in decision making for maternal health services in low- and middle-income countries, despite the fact that various individual studies have reported this information at the national and district levels. In addition, the identified contributing factors differ between studies. Therefore, this study sought to determine the pooled prevalence of women’s decision-making autonomy on maternal health services and associated factors in low- and middle-income countries. The findings of this study will give clinicians and other stakeholders about the basic understanding that they need to participate in and support women’s engagement in choosing maternal health services.
Methods
Reporting
Using the standard PRISMA checklist guideline, this systematic review and meta-analysis study was conducted to determine the pooled prevalence of women’s decision-making autonomy on maternal health services and its associated factors in low- and middle-income countries. 47 (Supplementary 1.)
Search strategy
International online databases (Pub Med, Science Direct, Scopus, and Google Scholar) searched for articles on women’s decision-making autonomy in maternal health services. We also retrieved gray literature from Debre Behan University’s online research institutional repository. The search string was established using “AND” and “OR” Boolean operators. The following core search terms and phrases with Boolean operators were used to search related articles: (((((Decision making autonomy OR freedom of decision OR freedom of decision making OR autonomy of decision)) OR (“Decision-making autonomy” OR “clinical decision making” OR “decision making, clinical” OR “medical decision making” OR “decision making, medical”)) AND Maternal health service) OR (“Maternal health service” OR “maternal-child health service” OR “maternal health” OR “women’s health” OR “reproductive health service”)) AND (Low and middle- income countries). Search terms were based on the PICO principles to retrieve relevant articles through the databases mentioned above. The search period was from 1 February 2021 to 24 January 2022.
Outcome measurement
Women’s autonomy: It was measured using the three constructs of aspects of women’s autonomy: (a) the woman’s health care (healthcare autonomy), (b) major household purchases (economic autonomy), and (c) visits friends or family (movement autonomy)? A score of 1 was given if women could decide alone or together with husbands, whereas a score of zero (0) was given if a husband’s decision alone or by others. After all, women’s decision-making autonomy is equal to or above the mean categorized as having autonomy, whereas below the mean was categorized as having no autonomy.35,48
Women’s decision-making autonomy in maternal health care service: a woman is said to be autonomous when she decides independently or jointly to attend antenatal care, postnatal care, delivered at a health institution, choose a place to receive maternal health service (private or government health institutions), plan when to be pregnant, and plan to continue or stop using maternal health service. If a woman decided independently or jointly with her partner a score of 1 was provided, whereas a score of zero was given if a partner decided alone for the above six questions.49,50 Therefore, those women who decided independently or jointly with husbands to ⩾50% of the above questions were categorized as having decision-making autonomy, whereas those respondents who answered <50% of the questions were considered to demonstrate no decision-making autonomy.
Maternal health service: it was measured by the update of antenatal care, postnatal care, and institutional delivery service. 49
Timing of antenatal care visit: it was defined by asking the participants if they could attend the first antenatal care visit between 8 and 12 weeks of pregnancy, the second visit between 24 and 26 weeks, then third visit at 32nd week, and the fourth visit between 36 and 38 weeks of gestation. 50
Frequency of antenatal care visits: it was also defined if women visited the health institution at least 8 times during the time of pregnancy. 50
Frequency of postnatal visit: it was explained if the mothers attend a total of four postnatal visits. 51
Timing of postnatal care visit: it was assessed by if the mother attends the first visit on the first day (24 h), the second visit on day 3 (48–72 h), the third visit between 7 and 14 days, and the fourth visit at sixth week. 51
Eligibility criteria
Inclusion and exclusion criteria
In all studies that reported the prevalence of women’s decision-making autonomy on maternal health services as study participants, only English language articles, both published and unpublished studies, had full text available for search and took place in low- and middle-income countries were included in this meta-analysis. Those studies that reported duplicated sources, qualitative studies, and articles without full text were excluded from this systematic review and meta-analysis.
Quality assessment
The two authors (KA and NA) independently appraised the standard of the studies using the Joanna Briggs Institute (JBI) standardized quality appraisal checklist. 52 The third author (EA) handled any disagreement raised during the appraisal. Finally, an agreement was reached through a discussion between the authors. The critical analysis checklist has eight parameters with yes, no, unclear, and not appropriate options. The parameters involve the following questions:
Where were the criteria for inclusion in the sample clearly defined?
Were the study subjects and, therefore, the setting described in detail?
Was the exposure measured the result validly and reliably?
Were the main objective, and standard criteria used to measure the event?
Were confounding factors identified?
Were strategies to affect confounding factors stated?
Were the results measured honestly and dependably? and
Was the statistical analysis suitable? Studies were considered low risk when they scored 50% and above on the quality assessment indicators, as reported in Supplementary file 2.
Risk of bias assessment
Two authors (K.D.T. and N.E.S.) independently assessed included studies for risk of bias through a bias assessment tool developed by Hoy et al. 53 consisting of 10 items that assess four domains of bias and internal and external validities. Any argument during the assessment was resolved through a discussion led by the third author (N.A.G.). The first four items (items 1–4) evaluate the presence of selection bias, nonresponse bias, and external validity. The other six items (items 5–10) assess measuring the bias, analysis-related bias, and internal validity. Therefore, studies that received “yes” for eight or more of the ten questions were classified as “low risk of bias.” If studies that received “yes” for six to seven of the ten questions were classified as “moderate risk,” whereas studies that received “yes” for five or fewer of the ten questions were classified as “high risk” as reported in Supplementary file 3.
Data extraction
Two authors (E.A.L. and N.A.G.) independently extracted relevant data using the Microsoft Excel spreadsheet 2016. Any debate between the authors was resolved through a discussion led by a third author (K.A.G.). The data automation tool was not used due to this study’s absence of the paper form (manual data). The name of the first author, year of publication, study country, study setting, study design, the prevalence of women’s decision-making autonomy in maternal health service, sample size, different associated factors, and the quality of each paper was extracted.
Data analysis
After extracting all relevant findings in a Microsoft Excel spreadsheet, the data were exported to STATA software version 14 for analysis. The pooled prevalence of women’s decision-making autonomy was computed with 95% CI, whereas a log odds ratio was used to declare the statistical significance between associated factors and women’s decision-making autonomy. Publication bias was checked by funnel plot and more objectively through Begg’s and Egger’s regression tests, with P < 0.05 indicating potential publication bias. The presence of between-study heterogeneity was checked using the Cochrane Q statistic. This heterogeneity between studies was quantified using I2, in which a value of 0%, 25%, 50%, and 75% represented no, low, medium, and high heterogeneity, respectively. A forest plot was used to visually assess the presence of heterogeneity, which was presented at a high-level random-effect model used for analysis to estimate the overall prevalence of women’s decision-making autonomy on maternal health services. Subgroup analysis was done by study country, publication status (published versus unpublished), and year. Sensitivity analysis was executed to see the effect of a single study on the overall prevalence of the meta-analysis estimate. The study findings were presented in the form of text, tables, and figures.
Results
Search findings and study characteristics
One thousand three hundred five research articles were retrieved using an electronic search. Of these articles, 405 were expelled for duplication, and 830 studies were excluded after reviewing their titles and abstracts. At the qualification stage, 70 articles were completely approved and evaluated for eligibility. Finally, this systematic review and meta-analysis included 19 studies29,31–33,35,37,43,46,54–65 with 103,983 study participants (Figure 1).

A PRISMA diagrammatic presentation used to show the selection of studies. The inclusion criteria were variation of the title and abstracts, place of study (low- and middle-income countries), presence of full abstract, and reporting different results. Studies were excluded if they criteria were duplicated source, developed nations, unrelated research, case studies, and qualitative studies.
All of the included studies were cross-sectional. Sixteen studies were published, whereas three studies were unpublished. The lowest and highest prevalence of decision-making autonomy in maternal health services was 22% 43 and 82.4%, 46 respectively. The largest sample size was 32,698, 46 and the smallest was 327. 63 Using Joanna Briggs Institute (JBI) quality appraisal checklist, all studies assessed yielded low risk (Table 1).
Characteristics of the included studies in the systematic review and meta-analysis for the prevalence of women’s decision-making autonomy on maternal health service in low- and middle-income countries, 2022.

Meta-analysis
Women’s decision-making autonomy in low- and middle-income countries
The overall estimate of women’s decision-making autonomy on maternal health services is presented with a forest plot (Figure 2). Therefore, the random effect model revealed that pooled prevalence of women’s decision-making autonomy on maternal health services in low- and middle-income countries was 55.15% (95% confidence interval: 44.11–66.19; I2 = 98.6%, P < 0.001)

Forest plot for women’s decision-making autonomy on maternal health service with the height of the diamond is the overall effect size 55.15% while the width is the confidence interval at (95% CI: 44.11–66.19). The y-axis shows the standard error of each study while the x-axis shows the estimate of effect size of the each study. The vertical line denotes the no effect. The box represents the effect size of each study and the line across the box is the confidence interval of each study.
Leave-one-out sensitivity analysis
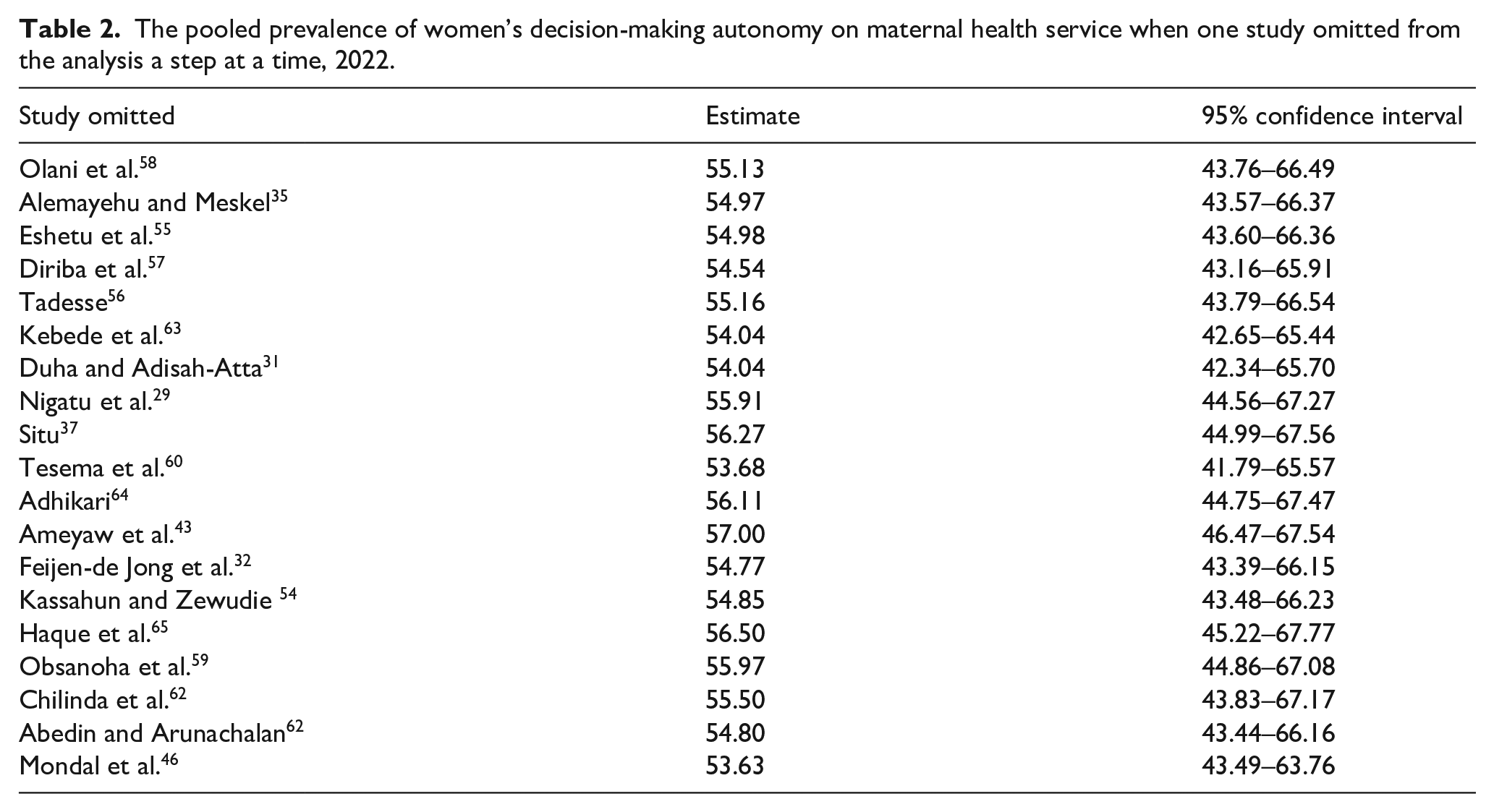
A leave-one-out sensitivity analysis was conducted to detect each study’s effect on the pooled prevalence of women’s decision-making autonomy on maternal health services by excluding one study at a time. The results random effect model reported that none of the omitted studies had shown a significant impact on the overall prevalence of women’s decision-making autonomy on maternal health service utilization (Table 2).
The pooled prevalence of women’s decision-making autonomy on maternal health service when one study omitted from the analysis a step at a time, 2022.
Subgroup analysis
We did subgroup analysis based on the presence of heterogeneity. In this study, the result of the Cochrane I2 statistic was 98.6%, P < 0.001, which indicated evidence of marked heterogeneity. Therefore, subgroup analysis was done by a country where studies were conducted, the status of publication (published versus unpublished), and study year. As a result, subgroup analysis based on country showed that the decision-making autonomy of women on maternal health services was the highest in Ethiopia (61.36%) and the lowest in Nigeria (31.19%) (Figure 3). The prevalence of decision-making autonomy based on the publication status of studies indicated that 54.64% in published articles and 55.14% in unpublished studies (Figure 4). Based on the publication year, the prevalence of maternal health service decision-making autonomy was 36.16% and 60.18% before and after 2016, respectively (Figure 5).

The forest plot displaying subgroup analysis based on the country where studies were done with the diamond represents the summary point estimate and the horizontal extremity of the diamond is the confidence interval at 95% (49.73%–73.38%). The standard error is plotted at the y-axis and the effect size plotted at x-axis. The squares represent the effect estimate of the individual studies and the horizontal lines indicate the confidence interval; the dimension of the square reflects the weight of each study.

The forest plot displaying subgroup analysis based on publication status of studies (published vs unpublished) with the height of the diamond is the overall effect size 54.64% (95% CI: 42.51–66.78) and 57.91% (95% CI: 54.80–61.02) for published studies and for unpublished studies, respectively. The y-axis shows the standard error of each study while the x-axis shows the estimate of effect size of the each study. The vertical line denotes the no effect. The square represents the effect size of each study and the line across the square is the confidence interval of each study.

Funnel plot showing displaying the subgroup analysis based on year of publication of studies. The pooled prevalence was 36.16% (32.72–39.60) and 60.18% (47.92–72.44) before 2016 and after 2016, respectively. The Y-axis is the standard error and the X-axis is the study result or effect size. The dotted diagonal lie of the funnel is the 95% confidence interval and the vertical. The vertical line is the line of no effect and dots are included studies reporting knowledge of kangaroo mother care.
Publication bias
The publication bias was checked subjectively through funnel plot visualization and objectively with Egger’s and Begg’s tests (P < 0.05). Therefore, the funnel plot shows the symmetrical distribution of studies (Figure 6). Moreover, both the Egger’s test (P = 0.243) and Begg’s test (P = 0.327) showed no publication bias in the studies.

Funnel plot showing symmetrical distribution of studies indicating absence of publication bias. The Y-axis is the standard error and the X-axis is the study result or effect size. The dotted diagonal lie of the funnel is the 95% confidence interval and the vertical. The vertical line is the line of no effect and dots are included studies reporting attitude of kangaroo mother care.
Factors associated with women’s decision-making autonomy in maternal health service
Seven variables were extracted to identify factors associated with women’s decision-making autonomy on maternal health service utilization among reproductive-age women in low- and middle-income countries. Of these, five variables (age, primary education, secondary education, being from urban, and wealth index) were significantly associated with women’s decision-making autonomy on maternal health service (Table 3). Among the socio-demographic characteristics of the respondents’ women whose age group above 35 was 2.7 times more likely autonomous to decide independently on maternal health service than those less than 20 years (OR = 2.67; 95% CI: 1.29–5.55), P = 0.008, I2: 90.1%; the heterogeneity test (P < 0.001) indicated no significant evidence of variation of heterogeneity across the studies, and Egger’s test reported no evidence of publication bias (P = 0.250). In addition, women who were at a primary level of education were 1.8 times more likely autonomous to decide independently on maternal health services than women with no education (OR = 1.75; 95% CI: 1.39–2.21), P < 0.001, I2 = 63.8%; the heterogeneity test (P = 0.097) showed evidence of variation across studies, and egger test reported no evidence of publication bias (P = 0.053). Women who were at a secondary level of education were also two times more likely autonomous to decide privately on maternal health services than women with no education (OR = 2.09; 95% CI: 1.32–3.32), P = 0.002, I2 = 87.8%; the heterogeneity test (P < 0.001) indicated no evidence of variation across studies, and Egger’s test showed no evidence of publication bias (P = 0.553).
Factors associated with women’s decision-making autonomy on maternal health service in low- and middle-income countries, 2022.

Those women from urban residents were two times more likely autonomous to decide themselves on maternal health services than rural women (OR = 2.09; 95% CI: 1.32–3.32), P = 0.003, I2 = 73%; the heterogeneity test (P = 0.298) showed evidence of variation across studies, and Egger’s test showed no evidence of publication bias (P = 0.071). Women whose monthly income greater than 5000ETB (Ethiopian Birr) were three times more likely autonomous to decide alone on maternal health service than women whose income was less than 1000 ETB (OR = 3.23; 95% CI: 1.85–5.65), P < 0.001, I2 = 97%; the heterogeneity test (P = 0.906) showed evidence of variation across studies, and Egger’s test showed no evidence of publication bias (P = 0.612).
Discussion
In undeveloped countries, the majority of women are given subordinate roles and excluded from all decision-making processes. 66 Especially in low- and middle-income nations, the Sustainable Development Goals by 2030, women’s empowerment, and gender inequality are seen as essential components for public health interventions. Therefore, this systematic review and meta-analysis study investigates women’s decision-making autonomy on maternal health services and associated factors in low- and middle-income countries.
In the current meta-analysis, the total estimate of decision-making autonomy for maternal health services in low- and middle-income countries was 55.16%. This result is congruent with research carried out in Iran (54.3%). 67 The presence of low socioeconomic group in the research area was a possible reason for the similarities.
This result is higher than the study conducted in Sub-Saharan African countries, where less than 20% of the population participated in maternal health service decision-making. 68 In contrast, the result of this study is lower than those of studies conducted in Canada (95.2%), 69 and low- and middle-income resource countries (61%). 70 This discrepancy might be attributed to existing sociodemographic conditions, the infrastructure of the healthcare system, and methodological variations (including study design). For instance, the low- and middle-income study, which was conducted on individuals 35 years of age and older, revealed that as a person gets older, their intention and participation in making their own decisions also increases. In Canada, the study also included mothers who were educated and capable of making their own decisions, which has a positive impact on maternal health service decision making
The subgroup analysis was done based on country, publication status of studies, and publication year. Ethiopia had the highest pooled prevalence of decision-making autonomy for maternal health services (61.36 %), while Nigeria reported the lowest frequency (31.19%). These differences are due to the number of studies, quality of papers, and the time gap between studies. The prevalence was higher after 2016 (60.18%) than before 2016 (55.15%). This variation might be because of the degree of concern given to the issue and the introduction of different policies and strategies targeting clinical and medical decision making. It was also no significant difference between published (54.64%) and unpublished studies (55.14%).
Women in our study who were 35 years or older had 2.7 times more autonomy to choose maternal health services than women who were under 20 years old (adjusted odds ratio (AOR) = 2.67; 95% CI: 1.29–5.55). This finding is consistent with a research conducted in Zambia, 71 which found that women above 30 were more willing to participate in decisions concerning their health. This might be brought on by older age, which increase the desire to make decisions freely, and by respect between couples, which promotes more private decision making.
Women with a primary education were 1.75 times more likely to decide maternal health services on their own than women without any education (AOR = 1.75; 95% CI: 1.39–2.21). Women with secondary education levels had also a higher chance of making decisions independently about maternal health services than women without a formal education (AOR = 2.09; 95% CI: 1.32–3.32). This finding is in agreement with research conducted in Sub-Saharan Africa. 72 These include the possibility that education increases women’s capability, decision-making knowledge, and self-confidence, which in turn improves women’s ability to make decisions about their health care and promote gender equality.
Compared with rural women, urban women had 1.8 times more autonomy to make their own decisions (AOR = 1.80; 95% CI: 1.22–2.66). These could be from urban women’s access to a variety of informational resources, particularly through television, radio, and other printable documents about reproductive rights and policy, which has a favorable impact on women’s decision making.
Our findings revealed that women with higher household monthly incomes were three times more likely to be autonomous compared with low-income women (AOR = 3.23; 95% CI: 1.85–5.65). This finding is supported by studies done in Zambia 82.4%45,71 and developing countries. 27 The possible explanation could be because economically sufficient women have access to mass media (i.e., television, radio, and magazine) and the chance to participate in various meetings than poor women; this could improve women’s engagement in making health care decisions.
This study utilized a random-effect model to manage a significant variation that resulted in between-study heterogeneity. We assessed leave-one-out sensitivity, and the results show that every study had no significant impact on the pooled good level of women’s decision-making autonomy on maternal health services. We assessed the possible variability source via subgroup analysis using the study country, publications, and year. The high heterogeneity might be due to differences in the sample populations, paper qualities, or sociocultural, ethnic, and regional differences.
Strength and limitations of the study
The study’s strength includes the use of a comprehensive electronic search strategy through a variety of datasets to determine the prevalence of women’s decision-making autonomy, the use of JBI-MAStARI appraisal, and access to gray literature. This study also had some limitations. These were the absence of a standard definition of decision-making autonomy to operationalize by the research team and might be researched bias on a cut of point. The absence of a similar previous study makes it challenging to compare this study’s findings. The study was limited only to the decision making of maternal health services (antenatal care, skilled birth delivery, and postnatal care) but did not address other sexual and reproductive health components.
Conclusion
In conclusion, this systematic review and meta-analysis reported that the pooled prevalence of women’s decision making in low- and middle-income countries was low. Besides, the pooled prevalence of women’s decision-making autonomy differed based on the study country, publication, and year. Age, primary level of education, a secondary level of education, being an urban resident, and monthly income were the determinant factors of women’s decision-making autonomy in low- and middle-income countries. Accordingly, it is better to have educational accessibility and income generation to improve women’s involvement in decision making.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221122618 – Supplemental material for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057221122618 for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis by Natnael Atnafu Gebeyehu, Kelemu Abebe Gelaw, Eyasu Alem Lake, Getachew Asmare Adela, Kirubel Dagnaw Tegegne and Nathan Estifanos Shewangashaw in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221122618 – Supplemental material for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057221122618 for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis by Natnael Atnafu Gebeyehu, Kelemu Abebe Gelaw, Eyasu Alem Lake, Getachew Asmare Adela, Kirubel Dagnaw Tegegne and Nathan Estifanos Shewangashaw in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057221122618 – Supplemental material for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis
Supplemental material, sj-docx-3-whe-10.1177_17455057221122618 for Women decision-making autonomy on maternal health service and associated factors in low- and middle-income countries: Systematic review and meta-analysis by Natnael Atnafu Gebeyehu, Kelemu Abebe Gelaw, Eyasu Alem Lake, Getachew Asmare Adela, Kirubel Dagnaw Tegegne and Nathan Estifanos Shewangashaw in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.