
Abstract
Purpose:
A descriptive qualitative study was conducted to explore perceptions and experiences related to pelvic health in the postpartum period among a cohort of women residing in communities with less than 50,000 residents.
Methods:
A semi-structured interview approach guided by the Theory of Planned Behavior was used. Postpartum individuals (<6 months since childbirth) were interviewed in the fall/winter of 2021–2022.
Results:
Specific to individuals’ attitudes toward pelvic health, women viewed Kegels as an important component to improving pelvic health but had a negative attitude toward their own pelvic health, often identifying their pelvic floor as “weak.” The subjective norms influencing a woman’s perception were typically, a positive influence by family/friends and the Internet, although the Internet was viewed as an insufficient resource. Healthcare providers were noted as an infrequent and ineffective resource for education and support in the postpartum period. Finally, women’s perceived behavioral control to manage their pelvic health was influenced by limited knowledge of pelvic health and time, and a desire for more education from their primary care provider and geographical barriers.
Conclusion:
Innovative strategies are needed to support postpartum women’s pelvic health within rural communities. Primary care providers may benefit from the development of “quick tips” by specialists, such as women’s health physical therapists, to optimize pelvic health discussions with their postpartum patients. Education interventions targeted toward postpartum women in rural communities should focus on strategies that address the geographic barriers identified while still providing individualized care. Options, such as webinars, telehealth, and text message interventions, could be considered.
Introduction
Pelvic floor disorders (PFDs) are a pervasive health issue that will affect one in four women in their lifetime. 1 PFDs may present as urinary or fecal incontinence, pelvic organ prolapse, sexual dysfunction, dyspareunia, or pelvic pain, among other presentations.2,3 Furthermore, it is estimated that the need for surgery related to PFDs will increase by 47% from 2010 to 2050, resulting in an associated increase in healthcare dollars spent. 1 The postpartum period leaves women especially vulnerable to experiencing PFDs due to the hormonal and physical changes associated with the perinatal period. Specifically, to prepare for childbirth, a woman experiences a widening pelvis and anterior tilt. These postural changes coupled with a gravid uterus can lead to a stretched or weakened pelvic floor. 4 The mode of delivery, the degree of perineal laceration, and previous pelvic floor muscle birth-related trauma can be correlated with an increased risk for certain types of PFD. 5
Despite the prevalence of PFDs, few affected women seek healthcare support or advice due to insecurity, embarrassment, lack of knowledge, or access issues.6,7 Furthermore, the majority of research on pelvic health perceptions/experiences has been conducted in urban settings leaving many unknown factors related to the perceptions of women residing in rural communities.7,8 A rural community is defined by the US Census Bureau as an entity that lies outside of metropolitan boundaries with those boundaries being defined as having a core county with one or more areas of 50,000 people and outlying counties tied to that core county. 9
It has been established that rural health disparities prevent women from getting adequate women’s health services, including comprehensive pelvic healthcare. While minimal research has explored barriers to seeking pelvic healthcare, research related to postpartum mental health found barriers for women in rural locations, including less access to women’s specialized healthcare providers, lower socioeconomic status, lack of educational opportunities, less health insurance coverage, limited childcare options, and lack of transportation.10,11 Lack of anonymity and stigma are also important barriers for women seeking out pelvic healthcare in rural communities, specifically in the postpartum time frame when self-reliance and hardiness from women are often the cultural expectation.11–13 More research is needed with postpartum women residing in rural communities to better understand how to support their self-management of their pelvic health to prevent and treat PFDs in the postpartum period.
Prior to the development of future interventions targeted at improving pelvic health in the postpartum period, a greater depth of understanding of the issue is required. The Theory of Planned Behavior (TPB) can support the prediction of engagement in health behaviors, such as engaging in pelvic floor muscle exercises or seeking treatment for pelvic floor dysfunction. The theory is broken down into three constructs: Attitudes toward the behavior, perceived behavioral control to engage in the behavior, and subjective norms related to the behavior. 14 Previous research related to TPB and pelvic health determined TPB variables that explained 53.1% of the variance in intention to engage in pelvic exercises during pregnancy. Furthermore, confidence in one’s ability to accurately partake in pelvic exercises predicted engagement. 15 To the researcher’s knowledge, TPB has not been used to explore the perceptions of postpartum women regarding their pelvic health or have investigations been specific to postpartum rural populations. Therefore, the purpose of this study was to explore perceptions and experiences related to pelvic health among postpartum women residing in rural communities.
Methods
Study design
This study employed a descriptive qualitative research design. Participation included completing an audio-recorded telephonic interview based on constructs of the TPB. Interviews took place in the Fall/Winter (2021–2022). This study was approved by a university-affiliated Institutional Review Board (Protocol # 2001886). The interview and survey measures reported in this study were deemed of minimal risk, and verbal assent was obtained prior to interview initiation. In addition, a cover letter was shared on the electronic survey and participants were asked to review study information and click enter if they wished to participate. Subjects were asked to complete a written consent form after the interview if they chose to enroll in a larger feasibility study related to pelvic health education. For the purposes of this research and future investigations, only those who enrolled in the subsequent feasibility study were included in this data analysis (n = 25).
Participants and recruitment
Participants were eligible to participate if they had given birth to a child in the last 6 months and resided in a community with ⩽ 50,000 residents and were at least 19 years of age, the age of adulthood in the state in which the study took place. Participants were excluded if they were not at least 19 years of age, did not live in a community with ⩽ 50,000 residents, or if they had not had a child in the last 6 months. The criteria of 6 months postpartum were selected as the postpartum period that has been termed as the “fourth stage of labor.” It consists of three continuous phases of healing. The acute (6–12 h), subacute (2–6 weeks), and the delayed postpartum period (up to 6 months). It is in the third and final phase that muscle tone and connective tissue are restored to their pre-pregnancy state. For this reason, the criteria of 6 months postpartum were selected. 16 Recruitment occurred via social media ads sent out by the sponsoring academic institution. Participants were directed to an eligibility link within the ad where postpartum status and geographic residence were confirmed. A total of 40 eligible participants were contacted with 10 being lost to follow-up (e.g. did not respond to initial contact) before 30 interviews were completed. Of those 30 individuals, 25 completed written consents to engage in a subsequent feasibility study. These 25 individuals were included in this analysis, so future data comparisons can be conducted.
Instruments
Once eligibility was confirmed, participants were directed to a demographic survey. The following sociodemographic information was obtained: age, age of the youngest child, number of vaginal deliveries, number of c-sections, race/ethnicity, highest level of education, occupation, household income, and time zone. Participants were also asked to complete two measures to assess their current pelvic health. These included the previously validated and reliable Pelvic Floor Disability Index (PFDI-20) and the Pelvic Floor Impact Questionnaire (PFIQ-7). 17 The PFDI-20 and PFIQ-7 measure the impact pelvic floor dysfunction has on an individual’s quality of life regarding symptoms related to the bladder or urine, bowel or rectum, and vagina or pelvis. The lower the score, the lesser effects the symptoms are having on the participant’s quality of life. 17
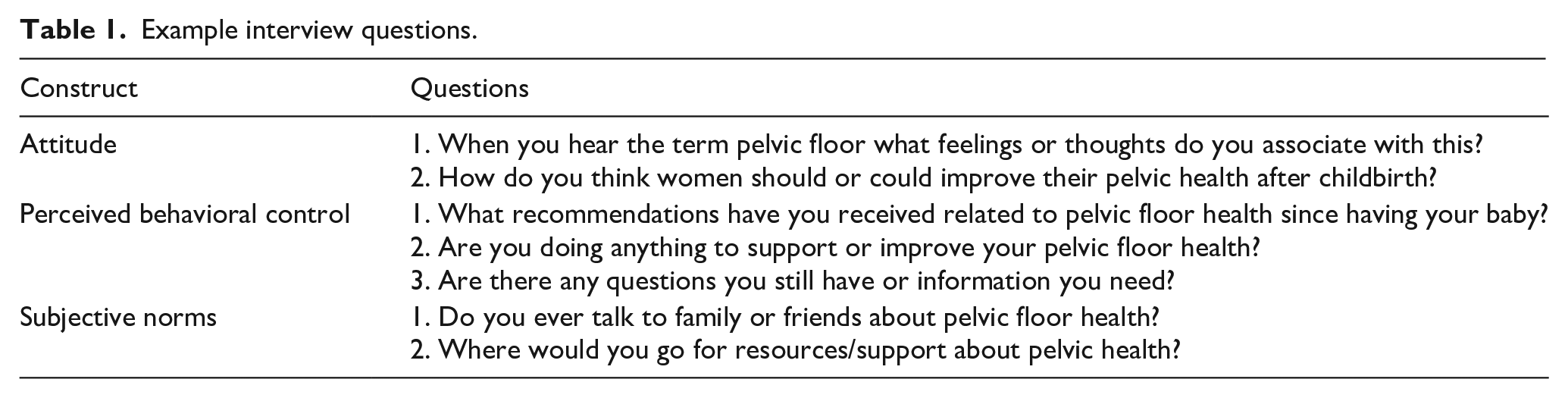
The interview guide was developed by a qualitative expert (PhD) in collaboration with two women’s health physical therapists. The interview guide was pilot-tested with two women who fit the eligibility criteria. Small wording changes were made to enhance clarity, and the guide was deemed complete. A total of 19 semi-structured interview questions were included. Example questions can be found below in Table 1.
Example interview questions.
Data collection
Participants were contacted via telephone by a female qualitative expert faculty member (PhD), and two trained female student researchers (BS, BS). Prior to initiation of the interview, participants were given a verbal description of the questions they would be asked (e.g. their personal experience and perceptions related to pelvic health). 6 They were also asked if they were alone or in an environment that allowed them to speak comfortably about the research topic. All participants verbally consented to continue the phone call and noted they were comfortable speaking at the time the interview took place. The semi-structured interview guide was used but participants were asked to expand or elaborate on their answers as needed. Interviews lasted approximately 30 min and participants received a US$25 gift card after the interview was completed.
Data analysis
Interviews were transcribed verbatim into a word document and uploaded into qualitative analysis software (NVivo 12). 18 After 15 of the interviews were completed, an informal open coding process was conducted by the primary investigator (K.S.). At this time, data saturation had not occurred and interviews continued. After 25 interviews were completed, data analysis by informal open coding took place again and saturation appeared to be achieved. The other researcher engaged in data analysis began their analysis at this time. An open coding, constant comparative method was employed for initial data analysis. 19 Raw transcript data were read multiple times independently by two investigators. Participant data were split into sections and compared to other participant responses for each question. Next, axial coding process was employed in which both researchers looked for connections between transcript sections and developed categories that connected the codes. At this point, researchers met to compare the categorical findings. Categories were assessed for similarities and collapsed between the two researchers until one codebook remained. Next, a selective categorical comparison was done independently where categories were compared to one another and a core category related to a TPB construct (e.g. attitudes, subjective norms, and perceived behavioral control) became the overarching theme with subsequent subthemes within it. Researchers met again to compare the categorical findings and discussed any discrepancies with a third qualitative researcher. Redundant codes were removed and discussions continued until consensus was met on the final themes among all three researchers.
This research met quality criteria in terms of its credibility, transferability, dependability, confirmability, and reflexivity. 20 Credibility was achieved by investigator triangulation in which three researchers were included in making coding, analysis, and interpretation decisions. 21 Transferability was used by engaging in thick description of the interviewee’s experiences. By having individuals’ complete survey measures that identify the current state of their pelvic health (PFDI-20 and PFIQ-7), one is better able to understand how an individual’s lived experience may be influencing their perceptions. 22 Dependability/confirmability was done by completing a meticulous record of the research process from start to finish. Finally, reflexivity was achieved by the researcher’s maintaining diaries in which they made a note of the implicit biases that might be influencing their data analyses. These were discussed openly among the researchers and each researcher examined one another’s codes to determine if these biases were seen in the coding structure.21,23
Results
Of the 25 women interviewed, on average, women had given birth 2.8 ± 1.1 months prior to the interview. However, 64% of women was identified as White/Caucasian followed by 28% of the women identifying as Black/African American. Participants in this study averaged a 125.5 ± 0.87 on the PFIQ-7 (out of 300) and a 146.2 ± 1.10 (out of 300) on the PFDI-20. See Table 2 for additional information.
Demographic information.
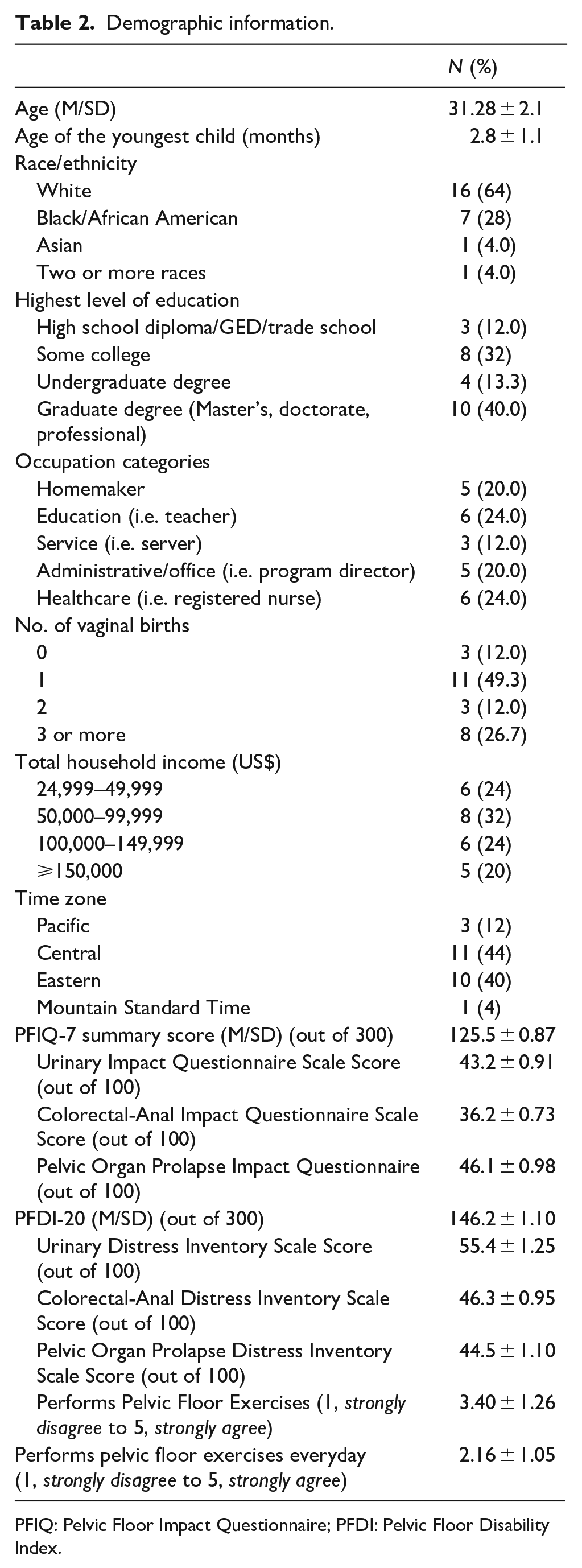
PFIQ: Pelvic Floor Impact Questionnaire; PFDI: Pelvic Floor Disability Index.
Thematic findings
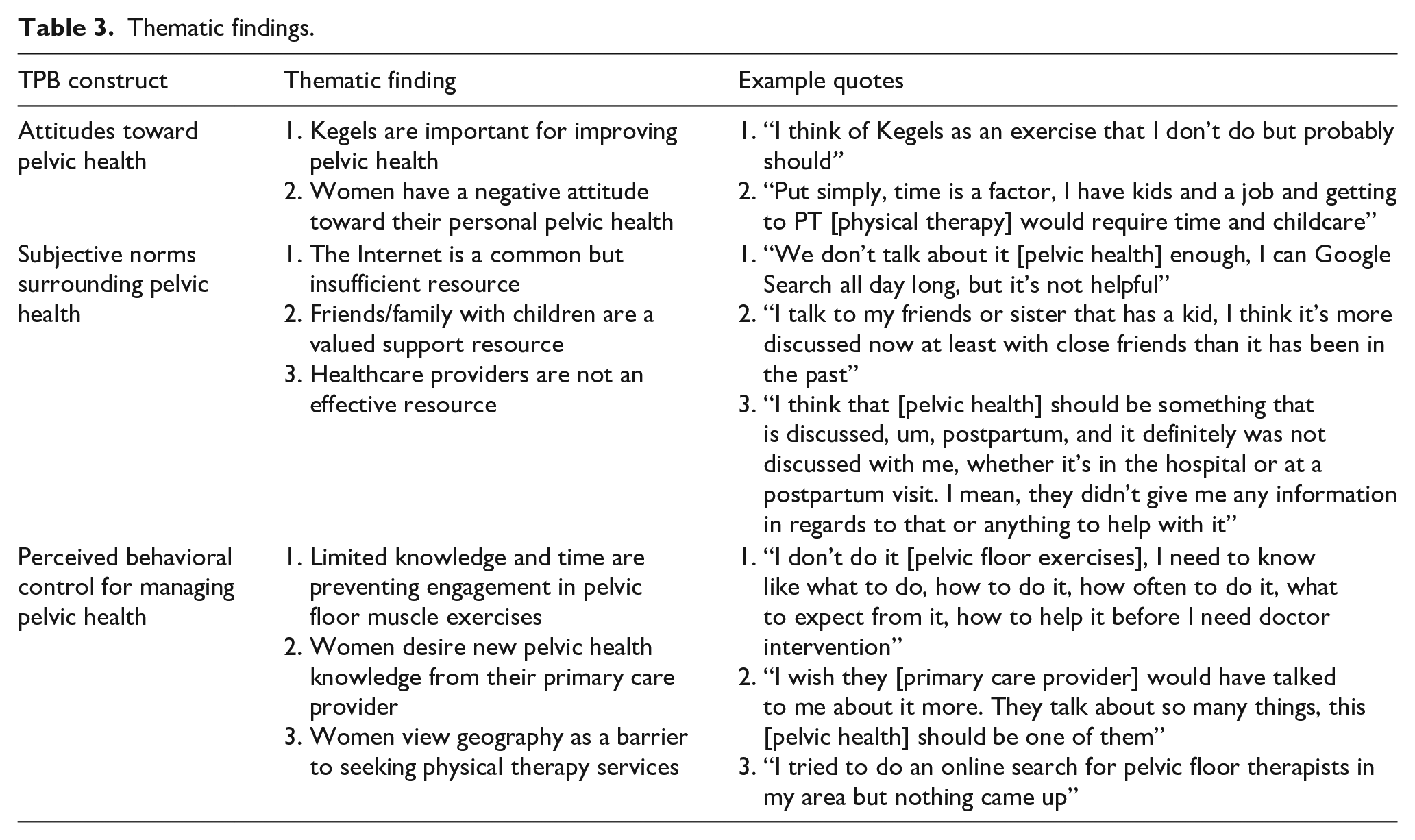
Table 3 identifies the themes and subthemes identified within the analysis. Additional details can be seen in the text below.
Thematic findings.
Attitude toward pelvic health in the first 6 months postpartum
The definition of attitude within the codebook included the degree to which a person has a positive or negative evaluation toward pelvic health. Within this theme, two subthemes are identified and discussed below.
Kegels are important for improving pelvic health
All women had heard of Kegel exercises and generally described them as the “activation of muscles.” Kegels were the most common reference when discussing ways to improve pelvic floor health (n = 22) and all women viewed them as a positive strategy for achieving pelvic floor muscle strengthening. For example, one mother said “I think of it as something I need to be doing more of because I know they’re important but I just don’t.”
Women have a negative attitude toward their personal pelvic health
The majority of women (n = 21) associated their current pelvic health with concerns related to weakness (n = 14), pain (n = 6), and worries for future pelvic health issues (n = 11). For example, one mother noted, I do have some concerns just because, you know, I’ve had 3 children. I guess the reason I have concern is because I’ve always heard from older women that the more children you have, you know, the more urine leakage that you might have later in life.
Within the realm of negative opinions, women also often spoke negatively about their ability to prioritize their self-care, and there was a general sentiment that their pelvic health was a low priority (n = 20).
Subjective norms surrounding pelvic health
Subjective norms were defined as the outside influencers who are impacting a mother’s perception of pelvic health. Within this theme, three subthemes were identified; additional details can be seen below.
The Internet is a common but insufficient resource
Participants commonly noted that they were using online resources to obtain pelvic health information after childbirth (n = 17). The most common information researched was related to pelvic floor exercises, symptom identification, and treatment options. Online resources included Google, Blogs, Facebook, and YouTube. One woman noted, “I didn’t get anything from a medical professional all of my information can from blogs that I’ve read.” Although the utilization of online resources was common, most women reported these were insufficient. Women noted a lack of confidence to engage in exercises they saw online (n = 8) or difficulty finding treatment options due to geographic barriers (n = 11). There was also a majority request for more individualized approaches to treatment (n = 16), and the online resources were described as “vague” or “general to all women” (n = 8).
Friends/family with children are a valued support resource
Many women noted that pelvic health discussions with family or friends had occurred but primarily with females who had also had children recently (n = 16). There was a general consensus that these discussions were valuable but should take place with intimate friends as there was still a societal taboo around the subject matter (n = 9). These discussions were deemed valuable because of the ability to commiserate with individuals having similar experiences (n = 12). For example, “so my best friend had a baby three months before me so our kids are three months apart. And we just talk about Kegels and just like how we are feeling.”
Healthcare providers are not an effective resource
Only one woman reported having their primary care provider bringing up pelvic health to them during pregnancy or postpartum without first prompting a discussion. This individual stated, “I had issues and they told me to go to a physical therapist but that just sounded odd, so I just read up on it and have learned from there.” However, few women prompted discussions related to pelvic health (n = 5). This is despite the fact that most women (n = 15) desired their provider to bring up these discussions. Only one woman reported a positive experience with the advice they received. They noted, I mentioned Kegels to my midwife and compared to my previous experience with a traditional OB my midwife point blank said, it would not be normal to experience urinary incontinence or other issues, even after multiple pregnancies and she would want to know right away and that she had a great contact for a physical therapist in our area.
Perceived behavioral control for managing pelvic health
Perceived behavioral control for managing pelvic health was defined as the perception of the difficulty to engage in pelvic floor supportive efforts, such as engaging in pelvic floor muscle strengthening or seeking support from a healthcare provider. Within these themes, three subthemes emerged; see additional details below.
Limited knowledge and time are preventing engagement in pelvic floor muscle exercises
Kegels were identified as the most commonly used pelvic muscle exercise although only half of the women reported at least weekly utilization. Most women had a desire to engage in pelvic floor muscle exercises to a greater degree than what they were doing currently (n = 20). This was especially true among those who self-reported experiencing a PFD or symptoms of a PFD (n = 10). However, these individuals often cited barriers, such as lack of knowledge (n = 5) or time (n = 5) as to why they were not engaging in pelvic floor muscle strengthening exercises to the degree they felt they should be.
Women desire new pelvic health-related knowledge from their primary care provider
Many women (n = 12) wanted their primary care provider, typically a family practitioner or midwife to educate them on their pelvic health. Most wanted exercise recommendations for strengthening (n = 8) and help identifying problematic symptoms (n = 4). For example, I guess my questions for them [primary care provider] would be like what are the best exercises to strengthen the pelvic floor? Is there anything I am currently doing that also helps? Are there any specific exercises that will help, or you know, not necessarily in addition to what I’m doing, but what I am already doing.
Women view geography as a barrier to seeking physical therapy services
Finally, women reported a geographic barrier to keeping them from seeking support from specialized healthcare, such as a physical therapist. Those who identified themselves as having symptoms of dysfunction (n = 4) and those without (n = 6) noted that geography was a limiting factor in accessing support from a physical therapist. Some (n = 2) noted long patient wait lists for nearby facilities or the closest available practitioner being more than 2 h away (n = 2).
Discussion
In this qualitative study, perceptions and experiences of pelvic health were examined within a cohort of postpartum women residing in communities with ⩽ 50,000 residents. Our findings provide important insights that should be considered prior to further intervention development. First, postpartum women perceive Kegels as a valuable exercise for improving pelvic floor health although only half of the participants reported engaging in Kegels regularly. Most women reported a desire to engage in Kegels to a greater degree. Importantly, Kegels may not always be the appropriate exercise based on the type of dysfunction a postpartum woman is experiencing. Ideally, a thorough evaluation of the postpartum woman by a pelvic health specialist would help determine if pelvic floor muscle strengthening is appropriate based on both subjective history and complaints, symptoms, and pelvic floor muscle palpation. However, as women have a negative attitude toward their personal pelvic health and put pelvic healthcare as a low priority, societal efforts are needed to improve maternal attitudes. To identify strategies to improve a woman’s attitude for managing their pelvic health, we should consider the overall experience of the postpartum mother. Postpartum women are typically given one 15-min postpartum healthcare visit 6 weeks after childbirth, despite a frequently lengthy list of complex health concerns. 24 Asking a mother to change her personal attitude about self-care in the postpartum period when her web of medical, social, and mental support is so limited is futile. While this study has uncovered the current state of maternal attitudes regarding pelvic health, the work needed to shift these attitudes cannot solely focus on the mother. It is not merely a need for greater education or resources but rather a complete cultural shift of enhanced support for a mother to be able to address her physical health in the postpartum period. To start this shift, sharing maternal perceptions of limited self-care with healthcare providers and changemakers is an appropriate first step. Furthermore, standards of care for postpartum mothers could include resources and referrals to a comprehensive healthcare team, including medical, rehabilitation, and mental health providers that can address the physical and emotional concerns related to pelvic health disorders.
There have been several interventions that have targeted pelvic health via mHealth (e.g. mobile applications) or online resources.25,26 Furthermore, our research team has determined that a one-time webinar can produce knowledge changes among postpartum women over a longitudinal period; however, a webinar did not change engagement in help-seeking behaviors or pelvic muscle exercise frequency. 18 However, our findings related to subjective norms within this study demonstrate that women frequently use online resources but find them inadequate. Concerns related to accurate engagement in muscle exercises and vague/general information were cited. This suggests that online resources can supplement support but may not be enough to improve self-management of pelvic health. Importantly, women do report engagement in discussions with female family/friends regarding pelvic health. Targeting avenues that focus on social support may be worthwhile, such as education interventions, that take place in parenting classes, exercise classes, play groups, or postpartum support classes (e.g. breastfeeding support groups).
Finally, related to perceived behavioral control, women report limited knowledge and time are preventing them from engaging in pelvic floor muscle exercises. Furthermore, women desire new pelvic health knowledge from their primary care provider. They would like these conversations to take place prior to experiencing symptoms of dysfunction and report a desire for individualized discussions and education targeted to their current state. However, given the limited time available to primary care providers during a 6-week postpartum follow-up appointment, it may not be feasible for physicians to have these individualized discussions and treatment prescriptions. 27 We propose two strategies to address this issue: (1) develop “quick tips” for assessing pelvic floor dysfunction during a postpartum, primary care visit. This would help primary care providers prioritize and optimize pelvic health conditions where a pelvic floor specialist or patient education resources may be beneficial. (2) Provide patients with cost-effective education materials to expand on discussions they had with their primary care provider. These may include webinars, text messages, and telehealth consultations. More research is needed to assess various education modalities among postpartum women in rural communities.
Limitations
This study is limited by its cross-sectional nature and the voluntary recruitment strategy that was used. The majority of participants identified as White and reported high levels of education. Participants may have self-selected to participate in this study via the sponsored social media ads due to interest in the subject matter. This may explain the large proportion of respondents that reported a graduate degree. Furthermore, although all women resided in communities with ⩽ 50,000 residents, it is unknown whether there are adequate healthcare services in the communities surrounding these participants. Finally, the utilization of the TPB in the data analysis process allowed researchers to better elucidate findings; however, since this theory was used directly and not through an emergent process, finding could differ when employing another data analysis technique in subsequent investigations. Further investigations employing additional analyses with a more diverse cohort that accounts for proximity of healthcare services based on geographic residence are warranted.
Conclusion
PFDs are common and can have devastating effects on a mother’s physical and psychological health. Women residing in rural communities experience additional barriers related to lack of access to specialized care for treating a PFD. Thus, it is pertinent that innovative strategies are employed with postpartum mothers to improve self-management of pelvic health prior to the occurrence of severe dysfunction. Our findings suggest women would benefit from an education intervention that targets time optimization, individualized care, peer support, and primary care provider support.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221122584 – Supplemental material for “We don’t talk about it enough”: Perceptions of pelvic health among postpartum women in rural communities
Supplemental material, sj-docx-1-whe-10.1177_17455057221122584 for “We don’t talk about it enough”: Perceptions of pelvic health among postpartum women in rural communities by Kailey Snyder, Elizabeth Mollard, Kari Bargstadt-Wilson and Julie Peterson in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221122584 – Supplemental material for “We don’t talk about it enough”: Perceptions of pelvic health among postpartum women in rural communities
Supplemental material, sj-docx-2-whe-10.1177_17455057221122584 for “We don’t talk about it enough”: Perceptions of pelvic health among postpartum women in rural communities by Kailey Snyder, Elizabeth Mollard, Kari Bargstadt-Wilson and Julie Peterson in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.