
Abstract
Background:
Although the overall rate of adherence to postpartum glucose screening is low (less than 50%), the geographical disparities, rural versus urban, in postpartum glucose screening rates for women with gestational diabetes are relatively unknown.
Objectives:
The purpose of this study was to compare postpartum glucose screening rates between women living in rural versus urban areas. Secondarily, this study evaluated the impact of transfer of maternity care on adherence to postpartum care and glucose screening rates in women with gestational diabetes mellitus.
Design:
Through retrospective chart review, data were collected from records with a diagnosis of gestational diabetes between January 2015 and October 2020.
Methods:
Subjects were classified as urban or rural residents. The following data were collected: number of prenatal and postpartum care visits, number of prenatal and postpartum glucose testing, infant birthweight, maternal complications, and demographic data, including race, age, and insurance status.
Results:
Our final sample consisted of 82 women classified as urban and 67 classified as rural. Overall, the number of postpartum glucose tests was lower in the rural group (M = 0.30), compared to the urban group (M = 0.52) and demonstrated statistically significant differences with Poisson regression (coefficient 0.56, Wald chi-square = 4.59, p = 0.03). Women from rural areas, who were referred and transferred maternity care to the Regional Perinatal Health Care Center, had the lowest average postpartum visits (M = 1.00) and postpartum glucose tests (M = 0.22) compared to the women from urban areas who were transferred from other providers with mean postpartum visits (M = 1.46) and mean postpartum glucose tests (M = 0.29).
Conclusions:
Rural women received lower postpartum glucose screening than those residing in urban areas. This finding illustrates greater disparities among rural women seeking postpartum care. Larger prospective studies are warranted to examine contributing factors, such as continuity of care and the transition from postpartum care to primary care. The remaining significant need is for healthcare providers to facilitate preventive care following pregnancy, including timely glucose screening and detection of women at high risk for developing type 2 diabetes, especially among rural populations.
Introduction
Along with the global trends of obesity and diabetes, gestational diabetes mellitus (GDM) is a public health issue that carries a significant risk for adverse health outcomes in both maternal and infant health. In 2020, the National Vital Statistics Survey reported that the rate of GDM in the United States rose 30% from 2016, from 6% to 7.8%, and is currently estimated at 8.3%. 1 The reported prevalence rates of GDM vary greatly according to the data source, from 6.9% up to 22.4% in North America.2,3 Women diagnosed with GDM during their second or third trimester of pregnancy are seven times more likely to develop type 2 diabetes mellitus (T2DM) within 10 years postpartum.4,5 Other risk factors for developing T2DM, such as ethnicity, race, maternal body mass index, maternal age, and family history, have been well studied and documented. 6
Routine postpartum follow-up and standard of care according to the American College of Obstetrics and Gynecology (ACOG) and American Diabetes Association (ADA) state that women diagnosed with GDM during pregnancy should receive 2-h glucose tolerance testing at 4–12 weeks postpartum.7,8 Yet, States continue to report suboptimal rates of postpartum diabetes screening even after the National Diabetes Education Program put out a call to action in 2012, and the Society for Maternal-Fetal Medicine Special Statement urged providers to improve postpartum glucose screening for women with GDM. 9 Strikingly, less than half of women with GDM report being tested for T2DM postpartum.10–12 Similar trends are being reported worldwide in countries such as the United Kingdom, Korea, Canada, and Brazil. 13
Geographical disparities
Current literature demonstrates that geographical disparities in postpartum glucose screening exist; however, the disparity between rural and urban populations has not been well studied. Geographic location has been shown to be a strong predictor of postpartum glucose screening practices, with the Western U.S. being found most likely to receive postpartum screening within 12 weeks postpartum (36%) compared to lower rates in the Northeast (19%) and South (18%). 10 GDM rates have been found to vary by state of residence, with a high of 12.6% in Alaska to a low of 4.7% in Mississippi. 1 On the global scale, those living in a socially deprived area are less likely to seek postnatal testing. 14 There is insufficient current evidence to conclude that disparities in postpartum glucose testing exist specifically between rural and urban populations, as conflicting results published by Hale et al. found no significant differences between the two groups. 15
Transfer of care
The transfer of maternity care and resulting disruption to continuity of care can be a significant problem affecting the receipt of postpartum glucose screening for women with GDM. Transfer of maternity care disproportionally affects rural women, mainly due to the dwindling supply of obstetrical delivery services in these areas. Currently, more than one-third of U.S. counties are maternity care deserts, with no access to obstetric care or obstetrical (OB) providers. 16
In 2019, ACOG established guidelines for risk-appropriate levels of maternity care to improve maternal outcomes. 17 These guidelines also delineated a set of conditions or complications that warrant consultation or consideration for transfer of maternity care. Transfer of maternity care to another provider or healthcare facility may occur during the prenatal period as indicated for high-risk pregnancies, such as those with GDM. Transfer of maternity care to another healthcare facility, otherwise known as interhospital transfer, can also occur before or after delivery for life-threatening maternal and/or infant complications. According to Kozhimannil et al., there are known disparities in the interhospital transfer of maternity care among rural women, who are transferred more often compared to urban women, and Black and Native American women are transferred more than White women. 18 Moreover, severe morbidity and mortality (SMM) are associated with interhospital transfer of maternity care, and SMM rates are higher among rural residents compared to urban residents. 18 The overall rate of interhospital transfer, before or after infant delivery, is approximately 0.4%–2%; however, the rate of transfer for prenatal or postpartum care to another healthcare provider is relatively unknown.18,19
Current data depict GDM and postpartum glucose screening rates as state averages or regional differences, but there is no current analysis of specific geographical county-level differences, that is, rural versus urban residents, within states regarding postpartum glucose screening rates. Identifying women earlier, particularly in rural or underserved communities, who are at risk for developing T2DM postpartum, could inform postpartum lifestyle interventions sooner, which have proven to facilitate weight loss and improve markers of insulin resistance. 20
The purpose of this study was to compare the geographical disparities, urban versus rural, in postpartum care for women with GDM. Secondarily, this study evaluated the impact of transfer of maternity care on adherence to postpartum care and glucose screening rates in women with GDM.
Methods
A retrospective patient chart review was completed with the retrieval of subjects with the following inclusion criteria: diagnosis with GDM and pregnancy between January 2015 and October 2020, age 18 and older, and delivery at the Level IV Regional Perinatal Healthcare Center in the Southeastern United States. The following electronic medical records were excluded from the chart review: women under the age of 18, those with a previous diagnosis of type 1 or type 2 diabetes, and having no prenatal care or delivery at the institution. Four hundred ninety charts were reviewed for eligibility criteria, and duplicates were excluded. Charts were reviewed until the calculated sample size of 152 charts was attained. However, to ensure an adequate sample size with rural address classification and other covariates, 428 subjects were reviewed for initial analysis as outlined in the flowchart (see Figure 1). Charts that met eligibility criteria were then classified as rural or urban residence. The sample size was calculated based on the following parameter specifications: (a) Total sample size = 152; missing data adjustment = 20%, which is arbitrary; (b) allocation ratio = 1; (c) effect size = 0.5; (d) alpha error probability = 0.05; (e) power = 0.80.
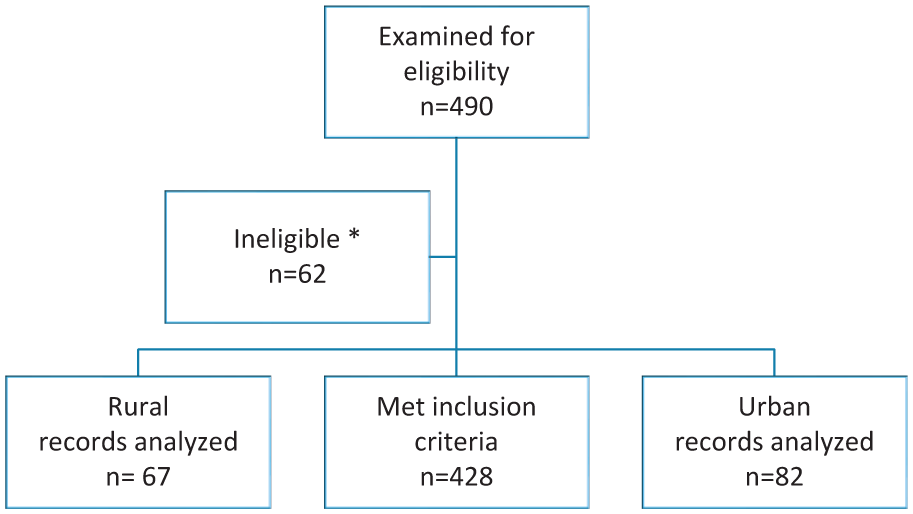
Flowchart for retrospective chart review.
The primary outcome variable collected from the chart review was the documentation of postpartum glucose testing. As routine postpartum follow-up and standard of care according to ACOG and ADA, women diagnosed with GDM during pregnancy should receive a 2-h, 75-g oral glucose tolerance testing (OGTT) at 4–12 weeks postpartum.5,6 Postpartum glucose testing is typically ordered at the postpartum visit. Follow-up visits are routinely scheduled for 6–8 weeks postpartum for women who have received maternity care from the Level IV Regional Perinatal Healthcare Center. For this analysis, postpartum glucose testing up to 12 months postpartum consisted of the documentation of 2-h OGTT, HbA1C, or random glucose testing. HbA1C testing for postpartum glucose testing is not routinely recommended as the blood volume during pregnancy influences the result; however, 2-h OGTT is often not feasible at the postpartum visit. Postpartum glucose testing was analyzed as a count variable and categorized as the number of documented postpartum glucose tests. Because of the high proportion of the sample with no documentation of postpartum glucose testing, it was also analyzed as a dichotomous variable and categorized as either no documentation of postpartum glucose testing or documentation of at least one or more postpartum glucose test.
The documentation of the number of prenatal and postpartum visits for women with GDM was recorded for outpatient office visits within the Level IV Perinatal Healthcare system and institution of delivery only, as records from outside and referring institutions were not extracted for this chart review. Prenatal visits to the maternal-fetal medicine clinic were also included, but emergency room and all other outpatient visits were excluded from the analysis. Because the study was conducted before the extended postpartum coverage policy was enacted in 2022 (from 60 days to 12 months), the postpartum visits typically occurred in the 6–12 week postpartum period. Other variables included the documented number of prenatal visits with documentation of self-blood glucose monitoring. Documentation of self-blood glucose monitoring consisted of scanned or uploaded logs of self-monitoring of blood glucose testing and results performed by the patient. Data were collected on other variables related to maternity care, including the transfer status of prenatal care from satellite OB clinics and referring OB providers, maternal complications during pregnancy, delivery, or postpartum, and use of diabetes-related medication during and after pregnancy. Infant birthweight and date of infant delivery were included in the chart review.
Demographic variables regarding the mother were collected (age, race, insurance status) as well as classification of urban or rural residence. Rural-Urban Commuting Area (RUCA) codes 1–10 were used to further classify urban and rural residence, based on patient address. The addresses were classified with RUCA codes and distributed on a scale from 1 to 10, beginning with 1 as a metropolitan, urban area and up to 10 as rurality increases. Urban residence is associated with RUCA codes 1 and 2, and rural residence is associated with codes 3–10, based on population density, urbanization, and daily commuting. 21
Statistical analysis
Descriptive statistics were calculated for all variables to identify patterns and associations. The mean and standard deviation (SD) were used to represent the continuous variables of maternal age and infant birthweight. Infant gestational age was calculated based on the infant’s delivery date and the estimated due date of the mother. Frequencies and percentages were used to describe count data, including the number of prenatal visits, the number of postpartum visits, the number of prenatal glucose tests performed, the number of prenatal visits with documentation of self-blood glucose monitoring, and the number of postpartum glucose tests obtained. Frequencies and percentages were also used to describe demographic variables, including race, rural/urban classification, insurance, and transfer status.
A Pearson’s chi-square test was used to compare categorical variables of rural/urban status and documentation/no documentation of postpartum glucose testing. Normality analysis was performed using the Kolmogorov–Smirnov test. A two-sample independent t-test was used for group comparison between rural and urban groups for age, infant birthweight, number of prenatal visits, number of postpartum visits, number of prenatal glucose tests, and number of postpartum glucose tests. Postpartum glucose testing as a dichotomous variable was compared to postpartum glucose testing as a count variable with Poisson regression for model fit of data and comparison of rural and urban groups. Poisson regression and t-test for group differences were used to analyze the number of postpartum visits. Statistical significance for all analyses was determined using an alpha level of 0.05. Data was analyzed using SAS software version 9.4 statistical software.
The study adhered to the STROBE/RECORD guidelines set forth by the EQUATOR network. 22 The proposed research was reviewed and approved by the Institutional Review Board (IRB) prior to data extraction and analysis (IRB approval # 1645918). The IRB determined that the chart review had exempt status and written consent was not required for the study. The data was de-identified prior to data analysis and stored in a secure, password-protected, and encrypted electronic folder.
Results
Sample characteristics
Fourteen percent of the 490 charts were designated as rural. The records classified as rural reached maximum eligibility at 67 charts. The study included 149 charts in the review and final analysis, with 82 classified in the urban area group and 67 in the rural area group. Characteristics of mothers and infants are shown in Table 1. The average maternal age was 31.13 years (range 19–43). Of the total sample, 14% were in the 18–24 years old category, which is expected as the rate of GDM increases with the age of the mother. Of the total population in this study, patients who identified as Black women comprised 53%, White women comprised 32%, and Hispanic women comprised 11%. The chi-square analysis showed that no statistical difference was found between the rural and urban groups based on race. Poisson regression analysis with multiple variables was conducted using the generalized linear model procedure in SAS statistical software, and found that demographic variables age, race, and rural status did not have a statistically significant effect on the outcome variables postpartum glucose testing and postpartum visits. This may be due to the lack of a sufficient sample size.
Demographics of mothers and infants.

LGA: large-for-gestational age; SGA: small for gestational age; SD: standard deviation.
Sample size insufficient for t-test group differences.
This sample was representative of a tertiary Perinatal Healthcare Center with a higher acuity level of pregnant women and infants. The rate of birth complications, including C-section rate, premature births, and preeclampsia, especially in this population, was higher than state and national averages. In this cohort, the rate of Cesarean section births was higher among women from urban areas compared to women from rural areas, 40% and 28%, respectively. Preeclampsia occurred at an average rate of 15% in both urban and rural women. Shoulder dystocia, polyhydramnios, placenta previa, placenta accreta, postpartum hemorrhage, and infection occurred in less than 5% of the mothers during or after delivery. The average birthweight was 3199.2 g overall, with a range of 620–4970 g (see Table 1). In the total sample, more than 20% of the births were premature infants, defined as less than 37 weeks of gestational age. The rate of large-for-gestational age (LGA) infants, greater than 4000 g, was approximately 12% in both rural and urban groups. Maternal age, birth complications, and infant birthweight were similar between the urban and rural groups and demonstrated no statistically significant differences.
The chart review comprised patients from 29 counties total, but the majority resided within 2 of the counties within the Regional Perinatal Service area. Applying the RUCA codes to the addresses in the chart review yielded an overall mean of 4.2 and a rural group mean of 7.8. The most frequent RUCA codes were 7 (40%) and 10 (36%) in the rural group of women. The women from urban counties were geographically distributed in RUCA codes 1 (n = 62) and 2 (n = 20). Of women from rural areas, almost 50% of patients attended the satellite OB prenatal clinic of the Regional Perinatal Healthcare Center in a neighboring rural county, but its local hospital does not offer OB delivery services. Table 2 shows the distribution of rural and urban counties in this dataset that have the availability of obstetric delivery care services and demonstrates that many patients required transfer of maternity care to sustain continuity of care.
Geographical distribution of access to obstetrical care.

OB: obstetric care or obstetrical.
Geographical disparities
As shown in Table 3, there were no significant differences in prenatal visits or prenatal glucose testing in the urban group compared to the rural group. The overall number of prenatal visits ranged from 1 to 24 visits. The documented average number of prenatal visits for women with GDM from urban and rural areas was 10.52 (SD 4.30) and 10.72 (SD 5.09), respectively, in the charts reviewed. The mean numbers of prenatal glucose tests for women from urban and rural areas were 2.63 (SD 1.52) and 2.58 (SD 1.27), respectively, also revealing no significant difference between urban and rural groups.
Urban versus rural prenatal and postpartum care.

NS: nonsignificant p value; SD: standard deviation.
p < 0.05.
Conversely, women with GDM from rural areas had significantly fewer documented postpartum visits and postpartum glucose tests than those from urban areas. The mean number of postpartum visits was 1.80 (SD 1.63) for women in urban areas compared with 1.30 (SD 1.07) for women in rural areas. Group differences revealed that these values were statistically significant with both the t-test (p = 0.02) and the Poisson regression coefficient of 0.33 (p = 0.01).
The mean number of postpartum glucose tests among women from urban areas was 0.52 (SD 0.88), and 0.30 (SD 0.46) among women from rural areas were statistically significant (p = 0.05) using t-tests for group differences, and the Poisson regression coefficient for the number of postpartum glucose tests was 0.56 (p = 0.03). This means that the expected increase in log count for 1 unit increase in the number of postpartum glucose testing for the urban group is 0.56 compared to the rural group.
The main outcome variables, number of postpartum visits and number of postpartum glucose testing, were examined as dichotomous variables in the final chi-square analysis. Although urban versus rural group differences were not statistically significant as binary variables, women from rural areas had a lower rate of postpartum visits, compared to women from urban areas, 74.6% versus 81.7%, respectively. Women from rural areas also had lower rates of any postpartum glucose testing compared to women from urban areas, 26.9% versus 36.6%, respectively. Of women who received any postpartum glucose testing, a sub-analysis revealed that 50% had random glucose or HbA1C testing, and the remaining 50% had the recommended OGTT. Overall, most women (67%) in both geographic classifications had no documentation of postpartum glucose testing at all.
Continuity of care and transfer of prenatal care
As expected for a Level IV Regional Perinatal Healthcare Center, a considerable proportion of mothers were transferred from other OB providers for maternity care, either because of having a high-risk pregnancy or a lack of OB delivery services in rural areas. Specifically, 34% (n = 29) of women from urban areas and 73% (n = 49) of women from rural areas transferred from surrounding counties for continuation of maternity care and delivery (see Table 2). The mean number of documented prenatal visits for patients who were not transferred was 11.62 (SD 3.47). Women who transferred care from other OB providers had fewer prenatal visits on average (7.31, SD 4.36). Of the 67 women from rural areas, 26 women transferred care from a neighboring rural satellite OB clinic located 46 miles away from the tertiary perinatal care center and had a higher average of prenatal visits (14.19, SD 4.15). Prenatal glucose testing followed a similar trend. Compared to the overall average number of prenatal glucose tests (2.61, SD 1.42) for women who were not transferred, women from rural areas who transferred care from other OB providers received 2.09 (SD 1.28) prenatal glucose tests on average. Women from urban areas who transferred care and those who received care from the neighboring rural satellite OB clinic received a higher average of prenatal glucose tests, 2.64 (SD 1.64) and 3.04 (SD 1.15), respectively.
Overall, the average number of postpartum visits was 1.58 (SD 1.42). As expected, the mean number of postpartum visits was higher for women who did not transfer care than for those who did transfer care, regardless of the geographic location. Figure 2 illustrates that women from urban areas who transferred care had an average of 1.46 (SD 1.29) postpartum visits, and women from rural areas who transferred care from the neighboring rural satellite OB clinic had an average of 1.31 (SD 1.01) postpartum visits. Those who did not transfer care had the highest average of postpartum visits, 1.92 (SD 1.65). The average number of documented postpartum visits was lowest for women from rural areas who transferred care from elsewhere (1.00, SD 0.95). Postpartum glucose testing showed a similar trend as postpartum visits, with women who did not transfer care receiving greater than the overall average number of postpartum glucose tests. The overall mean number of documented postpartum glucose tests was 0.42 (SD 0.73), and the average was highest for women who did not transfer care, 0.59 (SD 0.89). Figure 2 illustrates that urban women who transferred care received an average of 0.29 (SD 0.60) postpartum glucose tests, and those who transferred from the neighboring rural satellite OB clinic received an average of 0.31 (SD 0.47) glucose tests. The average number of documented postpartum glucose tests was lowest for women from rural areas who transferred care from elsewhere (0.22, SD 0.42).

Postpartum care and transfer of care.
Discussion
Overall, this study illustrates that disparities persist across all levels of maternal health care services, from the availability of obstetrical services at a larger level to the receipt of recommended postpartum care at an individual level. At a systemic level, the availability of obstetrical services disproportionately affects maternal health care for rural women–see Figure 3. Most rural mothers in this sample resided in counties without obstetrical services (Table 2). The geographic disparities in access to obstetrical care also mirror the geographic variability in postpartum glucose testing rates. According to previous research done by Eggleston et al., the South has the lowest postpartum glucose screening rates, along with the lowest concentration of providers in the United States, with an average of 7 rural hospitals per 100,000 women with OB delivery services.10,23 Conversely, the Western states have the highest concentration of access to OB services in rural counties, with an average of 15 hospitals per 100,000 women with obstetrical services, similar to the pattern of the highest postpartum glucose screening rates in the United States. 24

Availability of obstetrical services.
This study supports previous research that demonstrated geographic variability in the receipt of postpartum care and that rural residents are typically less likely to receive postpartum care than urban residents. 26 Compared to the estimated national average rate of 88% adherence to postpartum care among rural residents, only 70% of rural mothers in this chart review had any documented postpartum visits. 26 Variations in the receipt of postpartum care can be partially explained by socioeconomic factors, such as race and educational level. 14
This cohort of rural mothers also had a significantly lower documentation rate of any category of postpartum glucose testing compared to urban mothers, 30% versus 35%, respectively. Although the final data analysis was not sufficient in demonstrating significant group differences for the postpartum glucose testing rates between urban and rural mothers, the transfer of maternity care could be a contributing factor in these disparities. The possible urban versus rural disparities in postpartum glucose are a clinically significant finding and indicate a need for improvements in access to maternity care among rural populations. However, current research and the possible causes of rural-urban disparities in postpartum glucose testing are still lacking. In one of the few studies that looked at urban versus rural residence as a contributing factor to postpartum glucose testing, mothers who were married, had more than an adequate number of prenatal visits, older than 35 years, and participated in diabetes education were more likely to receive glucose testing, but the study did not demonstrate any significant differences between urban and rural mothers. 15 Geographic disparities in postpartum glucose screening exist; however, it is still relatively unknown if rural versus urban disparities occur at a county, state, or national level.
In addition, the continuity of care in this high-risk population is problematic, as they are more likely to utilize more than a single OB provider for maternity care. Fragmented care has been identified as one of the barriers to postpartum glucose testing.27,28 The continuity of care disproportionately affected the rural women in this study, with almost 75% of them transferring care from other providers compared to 35% of urban mothers who transferred care. As expected, a lower number of prenatal and postpartum visits was associated with women who transferred care from other institutions. The cumulative impact of these factors, limited access to obstetrical delivery services and transfer of maternity care, could explain the lower adherence rate to postpartum care and glucose testing among rural mothers. The lower rate of documented postpartum visits could also be related to the lack of Medicaid coverage up to 12 months postpartum, which was not enacted at the time of the study. Other possible systemic factors that could have been associated with variations in postpartum care are the use of appointment reminders, patient care navigators, home-visiting nurse programs, and characteristics of the health care setting. 29
Although postpartum glucose testing is the standard of care for women with GDM, many providers might not prioritize or fail to order this testing at the postpartum visit.26,29,30 Thus, the provision of postpartum care is inconsistent among providers and can affect glucose testing rates for women with GDM. Various components of preventive care should be incorporated in the postpartum visit, such as healthy lifestyle counseling, in accordance with ADA and ACOG guidelines. However, depression and contraception are usually addressed more often than a healthy diet and physical activity in postpartum care.26,30 Previous studies demonstrate that other provider-level factors, such as perceived discrimination and communication, can influence obtaining postpartum care, but these factors could not be assessed in this study. 29 Postpartum care can also vary among different types of providers. Nurse-midwives are more likely to order postpartum glucose testing and provide preventive care compared to obstetricians.30,31 In this study, the rural group of women who attended the rural OB satellite clinic had slightly higher rates of postpartum glucose testing, and visits may have benefited by receiving care primarily from a certified nurse midwife, compared to rural women who transferred their care from other institutions (see Figure 2). This reinforces the importance of continuity of care with regard to adherence to postpartum visits and glucose testing.
This sample of women with GDM and their infants represented a higher level of care, acuity level, and a high-risk, vulnerable population. Women with GDM often necessitate higher-level care for other coexisting conditions, such as preeclampsia, placenta previa, or premature births. Preeclampsia occurred at an average rate of 15% in urban and rural groups in this study, compared to 5%–8% in both state and national averages for preeclampsia. 32 In comparison to the total C-section rate of 40% for women from urban areas and 28% for women from rural areas in this sample, 32% is the national average, and 35% is the state average for total (unplanned and low risk combined) Cesarean deliveries. 23 This sample also represented a higher acuity level and a higher proportion of premature infants, 20%, compared to approximately 10.4% for the premature birth rate in the United States. 23 By comparison, state averages of premature births in this region are 12% and slightly higher than the national average. 23 The number of premature infants was higher among Black urban and rural mothers compared to White urban and rural mothers in this sample population. This study also found that the rate of LGA infants was 12% overall and slightly higher than the 8% national average for LGA infants. 23 (See Figure 4 for the distribution of mothers according to gestational age of infants by race and urban/rural status.) Lastly, although this retrospective study consisted of a limited sample of predominantly publicly insured, Black women, the demographics were similar to the two predominant counties in the service area. The demographics near the Level IV Regional Perinatal Healthcare center consist of 57% Black, 31% White for urban counties and 52% Black, 46% White for rural counties, respectively. 33 In contrast, more than 50% of births occur among Whites, and approximately 15% of the births in the U.S. occur among Black women. 34

Gestational age of infants by race.
This study underscores the need for equitable access to prenatal and postpartum care in both rural and urban populations, especially for high-risk pregnancies. The impact of limited availability of OB services in rural areas has been realized as maternal mortality and infant prematurity rates continue to worsen in certain areas. 35 Rural residents continue to have disproportionately higher rates of severe maternal mortality and morbidity, as well as higher rates of preterm births and infant mortality.18,36,37 Limited access to obstetric services and neonatal intensive care services for infants partially explains the rural-urban disparities in maternal and infant outcomes, but the socioeconomic characteristics in the county of residence also play a significant role. 36 More improvements in the continuity of care during the perinatal period are needed, especially for mothers in rural areas without obstetrical services and mothers who have transferred care during their pregnancy. Health system factors such as the expansion of Medicaid postpartum coverage to 12 months and regionalized, risk-appropriate care have contributed to improvements in access to maternal health care. Models of care, such as group prenatal care and maternal care coordination programs, may also improve maternal and infant outcomes.38,39 Specifically, the Centering Pregnancy Group Prenatal care model has demonstrated improved adherence to postpartum glucose testing. 40
Limitations
These findings were obtained from a high acuity, tertiary Level IV Regional Perinatal Healthcare Center and are not representative of the general population of birthing mothers with diagnosed GDM. Future studies should include a larger sample size for any reasonable conclusions about rural versus urban disparities in postpartum glucose testing. In general, the rate of GDM in pregnancy has been underreported, and birth records are often incomplete. 10 The rate of postpartum glucose testing in this chart review was also based on the accuracy of the electronic medical records. This chart review included the documentation of prenatal and postpartum care obtained from the institution of obstetrical delivery only and may reflect missing data in the complete maternal record. Although most records were taken before the beginning of the COVID pandemic, starting in April 2020, the provision of prenatal and postpartum care could have been affected. Although there was some documentation of the transfer of care from outside OB providers, the specifics of prenatal or postpartum care received at another site were unknown. Another limitation of the study is that nutrition counseling, referrals to diabetes education, or discussion about postpartum lifestyle interventions were not included in the chart review.
Conclusion
Women with GDM are a high-risk population and in need of timely detection of T2DM. This study illustrates a critical gap in maternal healthcare and the need to implement evidence-based methods to improve postpartum glucose screening within rural communities. Utilizing geography and population health data can help improve targeted strategies for postpartum glucose testing and implementation of postpartum lifestyle interventions to reduce the development of T2DM among childbearing women.
Footnotes
Acknowledgements
None.
Ethical considerations
This study IRB# 1645918 “Postpartum Glucose Adherence Rates: Chart Review” was reviewed by the Institutional Review Board at Augusta University.
Consent to participate
This was deemed an exempt study and written consent from the subjects was not required.
Consent for publication
An exemption for consent for publication by patients was determined by the Institutional Review Board.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.