
Abstract
Objectives:
Mothers of young children have been identified as a particularly vulnerable group during the COVID-19 pandemic. We aimed to explore how occupational, psychosocial and partnership-related factors were associated with their self-reported mental well-being during the first COVID-19 wave.
Methods:
Five hundred fifty participants of the BaBi cohort study (est. 2013, Bielefeld, North-Rhine Westphalia, Germany) were invited to complete an online survey and to take part in email interviews (April–May 2020). With survey data, we assessed self-reported mental well-being through validated instruments (eight-item Patient Health Questionnaire; short version of the Symptom Checklist) and ran linear regression models for occupational, psychosocial and partnership-related factors. We performed content analysis on the interviews’ data to further understand the determinants of the women’s mental well-being.
Results:
One hundred twenty-four women participated in the survey; of which 17 also participated in the interviews. A perceived lack of support in childcare was associated with higher levels of depressive symptoms, while having a higher internal locus of control was associated with lower levels. Psychological distress was higher in those reporting lack of emotional or childcare support. Interviews confirmed the interplay of potential stressors and highlighted the difficulties to reconcile different expectations of motherhood.
Discussion:
Occupational, psychosocial and partner-related factors can act (to varying degree) both as resources and stressors to the self-reported mental well-being of mothers of young children. These impacts took different forms and created opportunities or challenges, depending on specific life circumstances, such as work or family situations, relationships and own psychosocial resources. Although not representative, our study contributes to building the COVID-19 evidence base, delineating the mental health toll of the pandemic on mothers of young children and the factors that contribute to it.
Keywords
Introduction
COVID-19 restrictions, mental well-being and mothering
From the onset, the COVID-19 pandemic has taken a toll on the mental health of populations, with high rates of depression, anxiety, insomnia, posttraumatic disorders and stress-related symptoms being reported in various countries during the initial stages of the pandemic.1–5 The non-pharmaceutical interventions (NPIs) to contain the pandemic (e.g. stay-at-home orders, closures of childcare facilities and schools, home-office requirements) have disproportionately affected families with children because of substantive changes in childcare, organization of work and resulting economic insecurities. Parents were confronted with the stress and pressure caused by a sharp increase in household and childcare work, while at the same time adapting to changing work-related demands.6–10 In parallel, psychosocial resources, such as social interactions and leisure activities (such as physical activity) were put on hold, also (potentially) contributing to higher levels of psychological distress.11–15
Among parents, mothers in particular have been affected by the NPIs as they have been shown to bear most of the additional load16–19 compared to fathers.20–23 Especially, care work is still deeply rooted in and structured by patriarchal and heteronormative gender norms and roles prescribing women to be the primary care provider in a family. 24 Findings from the early months of the pandemic indicate that mothers seem to be at higher risk of adverse mental health than fathers: mothers’ depression and anxiety symptoms have appeared to be higher in the context of COVID-19 in comparison to previously reported population norms in a range of countries and continents (e.g. in Canada, Australia, China, Italy and the Netherlands9,13,25,26). Also, mothers’ perceptions of self-competence and self-reported health have decreased (e.g. in China), 27 particularly for mothers with children up to 8 years old.
Potential resources and stressors for women with young children during the first wave of the COVID-19 pandemic
At the beginning of the pandemic, studies have mostly focused on outcomes, without systematically exploring the factors that may negatively or positively impact those outcomes. In light of the NPIs, the focus shifted increasingly from the public sphere to the family setting and created the aforementioned challenges to align work- and care-related tasks. Based on this development, we have identified three sets of determinants as potential resources and stressors for the mental health of women with young children during the first wave of the COVID-19 pandemic that also emerged in above-cited research: the work domain, psychosocial resources, and partnership and family-related aspects.23,28–33
An extensive amount of evidence has linked various formal employment and paid work-related factors with mental health.34,35 This association is supposed to have intensified during the COVID-19 pandemic with a simultaneous exposure to school and childcare closures and the risk of financial insecurities.32,34,36 Although the ability to be productive at home depends on the employment situation of both partners and the number and age of their children, 37 mothers – especially of elementary school-age and younger children – are more often disrupted by their children than fathers when working in home-office.38,39 In general, mothers were more likely to reduce their working time, withdraw from their work, 29 or primarily work from home, 23 compared to fathers. Having to simultaneously perform in multiple (and potentially conflicting) roles can generate feelings of overload and lead to adverse mental health outcomes,34,40,41 as supported by role strain theory. 42
The association of psychosocial factors, for example, personality traits or social support, and mental health are assumed to be useful to understand coping strategies during the COVID-19 pandemic.43,44 For example, individuals who scored higher in agreeableness showed lower levels of mental health burdens compared to open and extraverted individuals. 44 Also, optimism and social support have been identified as protective factors for mental health outcomes in previous multi-national studies.45–49 Furthermore, the loss of coping strategies and the feeling of loneliness contributed to a rise of depression and anxiety, respectively. 41
Partnership and family-related factors also impact mother’s health – and may play an even greater role when NPIs have put public life mostly on hold. Work–family conflicts can act as potential stressors and have been identified as a crucial social determinant of mental health even before the COVID-19 pandemic.50,51 In light of potentially exacerbated gender inequalities in care work during the NPIs, cross-over effects of the partner can be of interest for mental health analyses. For example, a feeling of equality in the division of unpaid care work within a couple and paternal support in general, as well as good partnership relationship, are essential for the mother’s mental health.40,41
Rationale and objectives
In our mixed-method study, we aimed to explore the respective relevance of employment-related, psychosocial as well as partnership- and family-related factors during the first lockdown of the pandemic and their potential impact on the self-reported mental well-being of mothers of young children. We build our analysis of mental well-being on the broad definition provided by the World Health Organization stating that mental health is ‘a state of well-being in which the individual realizes [one’s] abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to [one’s] community’. 52 Accordingly, we conceptualize (self-reported) mental well-being not only as the mere absence or presence of mental illness but as a state encompassing emotional, psychological and social well-being. 53 Our study is set in Germany, where some studies have emphasized how detrimental to women the redistribution of tasks and roles within households with children is likely to be and how heightened the burden born by mothers has been so far.7,17,18,37,54 Given the unequally higher burden of childcare and housework imposed on mothers compared to their partners during the pandemic, we hypothesized that mothers who were in paid work or working from home experienced lower levels of self-reported mental well-being. We expected mothers with higher levels of psychosocial resources, for example, in terms of social support, tendency to optimism, high internal and external control beliefs and personality traits that enable to adapt easier to new situations, to experience higher levels of self-reported mental well-being. As for the partnership- and family-related factors, we hypothesized that perceived inequality in the distribution of housework, perceived lack of support from the partner, and conflicts with the partner were associated with lower levels of self-reported mental well-being.
Methods
Study design
Our ‘Family study’ is a mixed-method COVID-19-specific follow-up of the BaBi birth cohort study established in 2013 in Bielefeld, North-Rhine Westphalia, Germany. 55 The BaBi cohort study originally explored health disparities from birth to early childhood in almost 1000 newborns and their mothers. In the Family study, we were interested in the experiences, health and well-being of the mothers from the BaBi study during the ‘first wave’ of the COVID-19 pandemic in Bielefeld, North-Rhine Westphalia, Germany. 56 We contacted all 550 participants from the BaBi cohort who previously agreed on being approached again via email on 15 April 2020. We sent a reminder on 28 April 2020 and closed the survey on 25 May 2020. The participants were invited to take part in a quantitative online survey (accessible on computers, tablets and smartphones), qualitative email interviews or both. We obtained consent to link the baseline BaBi cohort data with our Family study data, which enables a rich set of relevant exposures and a longitudinal perspective on the self-reported mental well-being of the participants.
All participants lived in the same geographic area (i.e. Bielefeld) and were thus exposed to the same intensity of and response to the COVID-19 pandemic. The first containment measures had been implemented mid-March. At the time of data collection, schools, pre-schools and nurseries were mostly closed (exception were made for the care of children of ‘essential workers’, e.g. healthcare professionals, and for children attending senior years at different levels). Remote working was strongly recommended but not mandatory. 57 In addition, measures included limiting the number of people in indoor and outdoor facilities, mandatory mask wearing and/or hygiene regulations in different domains of life, for example, in hospitals, public transport, in- and outdoor sports, cultural events and touristic travels (mostly independently of the Covid-19 incidence at that time). Contrary to some other European countries, it was still possible to go outdoors at any time of the day for leisure. 57
The study has been approved by the Ethics Committee of Bielefeld University (Ref 2020-059).
Measurement of exposures and outcomes in the quantitative survey
All scales and measures can be found in the original questionnaire (Supplemental material 1, German language only, validated tools marked with an asterisk). To assess the self-reported mental well-being of the participants, we used two validated, well-established instruments that have been applied to the German context extensively, namely, the eight-item Patient Health Questionnaire (PHQ-8) 58 and a short version of the Symptom Checklist (SCL-K-9). 59 PHQ-8 assesses symptoms of a major depression 60 (e.g. lack of interest, sleeping disorders, fatigue, loss of appetite). The SCL-K-9 is a measure for global psychological distress (e.g. including depressive, dysthymic, vegetative, socio-phobic symptoms). Both scales use Likert-type scales (ranging from 0 = not at all to 3 = almost every day (PHQ-8) or, respectively, 4 = extremely (SCL-K-9) to determine the severity of symptoms over the past 2 weeks. For analyses, we calculated a sum score for the PHQ-8 (max. 24 points) 58 and the global severity index (GSI) for the SCL-K-9 (which is the mean severity over all nine items). 59 To compare the prevalence of depressive symptoms to other samples, we applied the validated cut-off value for PHQ-8 scores ⩾ 10 indicating clinically significant depression (dichotomized into depressive versus not depressive). 58
Our exposure variables were organized in three thematic groups, that is, occupational, psychosocial and partnership-related factors. As for occupational-related factors impacting self-reported mental well-being, we determined whether the women were in paid work (yes/no), had an essential job (yes/no) and experienced changes at work or decreases in the household income due to the COVID-19 pandemic. To explore tensions between occupational and family-related responsibilities, we used the Work and Family Conflict Scale (WAFCS). 61 The WAFCS is composed of two summative subscales (work-to-family and family-to-work subscale, each including five items) ranging from 5 to 35 with higher scores indicating higher levels of conflicts. To capture potential conflicts between occupational and care-related responsibilities, we assessed whether (a) the women engaged in home-schooling activities for at least 1 h per weekday (yes/no) and (b) the family used for at least one of their children ‘emergency care’ (yes/no), an option only available for children whose parent worked in an occupation that was considered ‘essential’ (e.g. teachers, police officers, public utilities).
Regarding psychosocial factors, we asked participants whether they had positive experiences while NPIs were in place (e.g. reconnecting to nature, spending more time together as a family (yes/no)) and the perceived level of social support (based on the Oslo Scale of Social Support, 62 dichotomized to ‘moderate to high social support’ versus ‘low social support’). Since personality traits have been associated with mental health, also before the COVID-19 pandemic, and are considered to be stable over time, 63 we also drew on the baseline questionnaire of the BaBi cohort. Specifically, we integrated the Big Five Personality traits (BFI-10), 64 locus of control (IE-4) 65 as well as optimism–pessimism (SOP2) 66 measures. The BFI-10 has five subscores representing five personality traits (extraversion, agreeableness, conscientiousness, emotional stability and openness). Personality traits are rather stable dispositions in adulthood 63 but seem to be susceptible to gradual change over time. 67 The IE-4 consists of two subscores pertaining to internal and external loci of control. All these subscores represent averages ranging from 1 to 5 with higher values indicating higher agreement to the respective statements. The SOP2 score ranges from 1 to 7 where higher values show higher levels of optimism.
To capture partnership-related factors potentially affecting the self-reported mental well-being of mothers, we analysed the subjective perception of taking over (a lot) more than the equal share of housework (versus taking over the equal share or less), whether the women felt that support from the partner at the household (yes/no), emotional (yes/no) and childcare level (yes/no) was lacking, self-reported frequency of conflicts with the partner compared to pre-COVID-19 times (more frequent/about the same/less frequent) and feeling a closer connection with the partner since the beginning of the pandemic (yes/no).
As covariates, we adjusted for the participants’ age, number of children and highest formal educational attainment (operationalized as a dichotomous variable distinguishing between secondary education/vocational training and tertiary education) to control for traditional markers of health inequalities.
Qualitative data collection
To compare, contrast, enrich and further understand the findings of our quantitative analyses, we also collected qualitative data, through semi-structured email interviews (consolidated criteria for reporting qualitative research (COREQ) 32-item checklist 68 in Supplemental material 2). SBZ conducted the qualitative data collection and introduced herself as a research associate at Bielefeld University to the participants via mail. Considering the strict physical distancing measures in place at the beginning of the pandemic, as well as the closure of childcare facilities and the associated time pressure on the participants, we believed that email interviews would increase flexibility and give more autonomy to the participants as to when they do the interviews.69–71 The interview process included three waves of open questions that were identical for all participants (the interview guide can be found in Supplemental material 3 – German language only) and, from the second wave on, follow-up participant-specific questions to the answers already provided, aiming to initiate a written conversation between interviewer and interviewee. Questions in the first email covered the adjustment to the pandemic situation in terms of re-organizing daily life (work, childcare and household obligations), and perceptions and feelings related to the participants’ role as mothers. The second wave included questions on the family members’ health and well-being as well as the share of responsibility in seeking pandemic-relevant information, and implementing personal protective measures and child-oriented communication about the pandemic situation. The third round finalized this process by asking about views on the future.
We sent two recruitment emails at an interval of 3 weeks and a third email to announce the last possible opportunity to engage with the researchers. Email interviews were conducted between 22 April and 24 May 2020. Throughout this time, email interview responses were read and discussed within the team. We stopped data collection once the team felt confident that saturation was reached (i.e. the data set included a range of diverging yet recurring views and we felt confident that no new type of experience would emerge from further interviews).
Analysis strategy
For the quantitative part of the study, we used descriptive statistics to assess sample characteristics. To explore the associations between the occupational, psychosocial, as well as partnership-related factors and both self-reported mental well-being outcomes, that is, depressive symptoms and psychological distress, we ran linear regression models separately for each set of exposures due to the limited sample size and number of missing values (M1–M6). All regression models were adjusted for the covariates age, number of children and formal educational attainment.
Cases with missing data were excluded from the respective analysis step. Given the small sample size, we used the maximum available number of cases for each regression model we ran (which results in different sample sizes for each regression model).
As sensitivity analyses, we additionally ran linear regression models including only exposure variables that showed significant associations with depressive symptoms or psychological distress in M1–M6 (which resulted in M7–M8). This allowed us to examine whether the associations or estimates of particular factors change when adjusting for factors from all three thematic exposure sets. Since our sample included women being in paid work and non-paid work, we checked whether the associations remained when only performing the linear regression models for the occupational-related factors on the subsample being in work (the number of those in non-paid work was too small for a separate regression model).
In the qualitative part of the study, SBZ and VN performed content analysis to identify key perspectives emerging from the interviews. 72 VN was a research assistant at the time of data analysis and hold a bachelor’s degree in health communication. Both researchers, who identify as women, have received training in qualitative data analysis and content analysis throughout their studies, SBZ has previously conducted qualitative studies independently. SBZ is a mother herself. For coding, we used the software ATLAS.ti 8 and identified five key themes, to which 22 codes were attached. In all, 353 quotes were tagged to codes. In line with the focus of the quantitative data analysis on occupational, psychosocial and partnership factors, we analysed the qualitative data in the three following thematic dimensions: work-to-family and family-to-work conflicts, sense of well-being and quality of experiences (as one important component of psychosocial resources), and partnership. In each dimension, we differentiated between an actional level, and a perceptual and emotional level. At the actional level, we looked at the ‘doing’, that is how participants described their living together, their professional life and their daily routines. At the perceptual and emotional levels, we gathered the participants’ expression of their feelings, thoughts and reflections about the current situation in relation to themselves, their partners, children or work. However, this distinction remained analytical since the quotations revealed the interwovenness of both levels. The coding tree is provided in Supplemental material 4 (German language only).
Quantitative results
Sample description
One hundred twenty-four women participated in the online survey. Of those, 122 women gave consent to link their responses from the Family study with the BaBi baseline survey. To avoid biased estimates for our self-reported mental health outcomes, we excluded two more women with a presumably clinical manifestation of depressive symptoms, that is, women who were categorized as having depressive symptoms based on the PHQ-8 in the Family study and a self-reported diagnosis of depression in the BaBi baseline study.
Our sample was composed of highly educated women, most of whom cohabited with their (male) partner. Most of the women engaged in part-time work (64.2%), while the partner was usually full-time employed. The majority of the families had two children (71.8%) and used formal childcare facilities. Sixteen per cent of the women were immigrants or had a second-generation migration background (Table 1).
Sample characteristics of the Family study, Bielefeld, Germany, 2020 (n = 120).

The prevalence of depressive symptoms (PHQ-8 score ⩾ 10) was 15.7% in our sample. The GSI of psychological distress was 0.7 (SD: 0.5) indicating rather mild symptoms in the overall sample (ranging on a scale from 0 = not at all to 4 = extremely). Women reported on average symptoms of psychological distress for 4.3 (SD: 2.0) of the nine items. When only relating to these items where participants reported symptoms of psychological distress, the overall severity was accordingly higher (1.4, SD: 0.4) (data not shown).
In terms of the occupational, psychosocial and partnership-related factors, descriptive statistics can be found in Table 2. About 40% of our sample considered themselves as essential workers. While 35.3% of the women reported decreases in the household income due to the COVID-19 pandemic and 10.9% could not estimate yet, for 53.8% of the women, the household income did not change. About one-third did not experience any changes at work. In contrast, 39.8% started remote working and 26.2% were facing reduced working hours, dismissals, compulsory leave or decreased activity levels. Regarding work and family conflicts, we saw comparable levels of work-to-family (15.4, SD: 8.1) and family-to-work conflict (15.0, SD: 8.8). Only every tenth family used institutional emergency care for their children and about 30% of the women were involved in at least 1 h of home-schooling per weekday.
Descriptive statistics for occupational, psychosocial and partnership-related exposures, Bielefeld, Germany, 2020 (n = 120).

Variables from the BaBi baseline cohort.
With reference to psychosocial factors, most women reported moderate to high levels of social support (72.3%). On average, the women identified 5.5 (SD: 2.6) out of 13 positive experiences since the pandemic started. Drawing on the baseline survey, we saw that our sample was rather optimistic (SOP2 mean 5.3, SD: 1.0) and showed higher internal than external locus of control. Regarding the personality traits, the women scored relatively high on consciousness, openness, agreeableness and extraversion, while we saw lower levels of neuroticism.
Concerning partnership-related factors, about two-thirds of the women felt that they were taking over (a lot) more than their equal share of housework over the past 2 weeks (64.9%). The areas where they were subjectively lacking support from their partner was highest in the household sphere (39.7%), followed by childcare demands (35.3%) and emotional support (22.4%). Less than one in five women reported that conflicts with their partner increased compared to pre-COVID times, while about every fourth woman reported fewer conflicts. About 25.8% of the women felt that the pandemic and associated NPIs allowed them to become closer to their partners.
Multivariate analysis
In multiple linear regression models, we assessed how the occupational, psychosocial and partnership-related factors are associated with depressive symptoms and psychological distress, when adjusting for age of the women, the number of children and formal educational attainment (Table 3).
Linear regression coefficients for depressive and psychological symptoms by occupational, psychosocial and partnership-related exposures, Bielefeld, Germany, 2020.
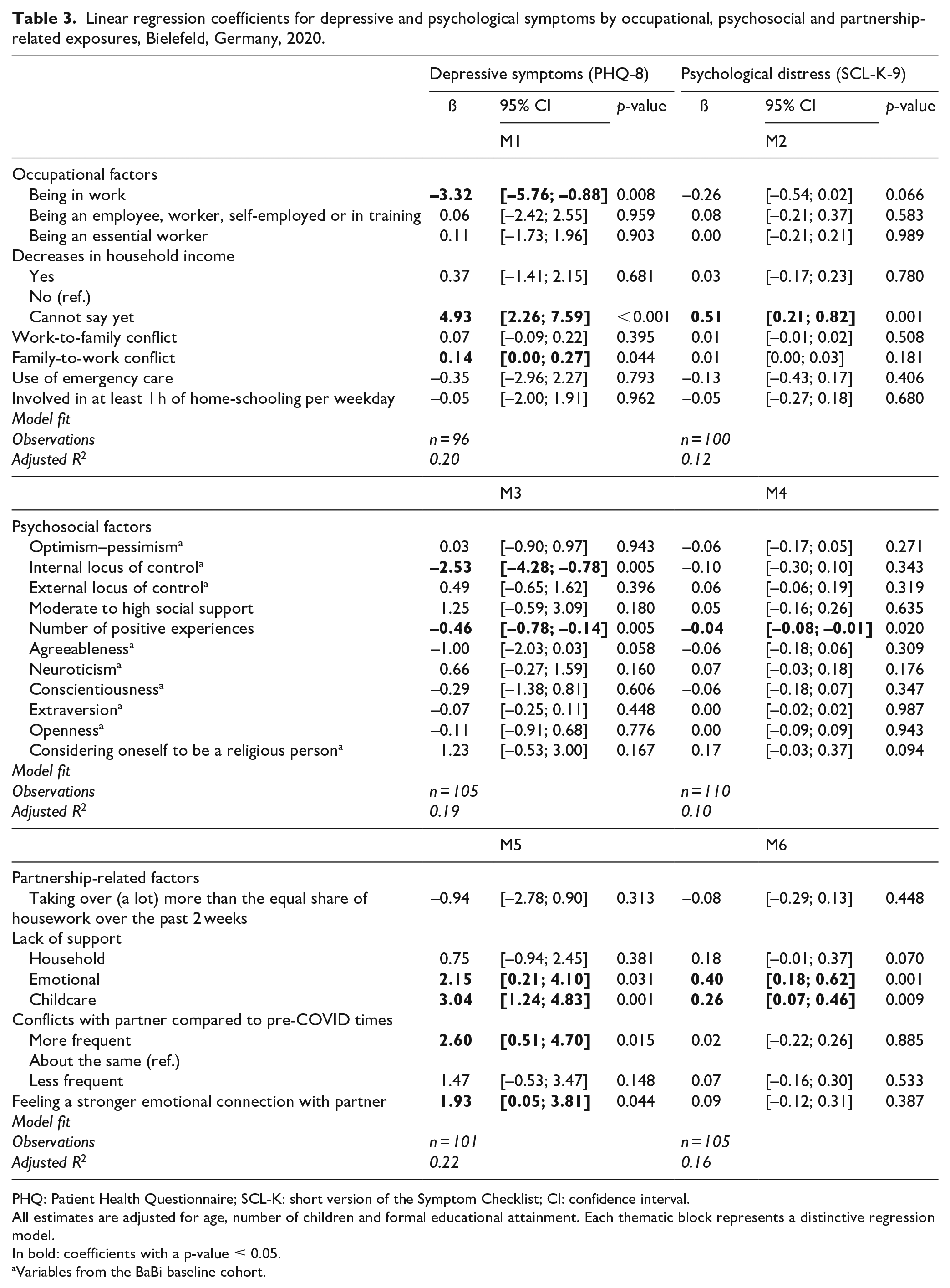
PHQ: Patient Health Questionnaire; SCL-K: short version of the Symptom Checklist; CI: confidence interval.
All estimates are adjusted for age, number of children and formal educational attainment. Each thematic block represents a distinctive regression model.
In bold: coefficients with a p-value ≤ 0.05.
Variables from the BaBi baseline cohort.
For occupational factors, insecurities about decreases in household incomes were associated with higher levels of both depressive symptoms (M1) and psychological distress (M2) compared to no decreases in household income. As for those women who already have experienced actual decreases in household income, we did not see an effect on either of the outcomes. Women being in work showed significantly lower levels of depressive symptoms (–3.32, 95% CI [–5.76; –0.88]) than women who were not in work at the time of the survey. For psychological distress, the estimate indicated the same direction for the association, but it did not reach statistical significance (–0.26, 95% CI [–0.54; 0.02]). Depressive symptoms were slightly higher in those women who experienced higher levels of family-to-work conflict (0.14, 95% CI [0.00; 0.27]). We did not see any significant associations of being an essential worker, occupational groups or work-to-family conflicts with any of the two self-reported mental well-being outcomes.
Regarding psychosocial factors, we saw that only women reporting higher internal locus of control (M3: –2.53, 95% CI [–4.28; –0.78]) and more positive experiences during the pandemic (–0.46, 95% CI [–0.78; –0.14]) showed significantly lower levels of depressive symptoms. For psychological distress, only a higher number of positive experiences showed a significant association (M4: –0.04, 95% CI [–0.08; –0.01]).
In terms of partnership-related factors, women who lacked support from their partner in terms of childcare and at the emotional level experienced significantly higher levels of depressive symptoms (M5: childcare: 3.04, 95% CI [1.24; 4.83], emotional: 2.15, 95% CI [0.21; 4.10]) and psychological distress (M6: childcare: 0.26, 95% CI [0.07; 0.46], emotional 0.40, 95% CI [0.18; 0.62]). Surprisingly, women feeling a stronger emotional connection with their partner since the onset of the pandemic showed significantly higher levels of depressive symptoms (1.93, 95% CI [0.05; 3.81]).
The covariates that we adjusted for, that is, maternal age, number of children and formal educational attainment, did not show significant associations in any of the models of our analyses.
Overall, the findings suggest that the selected exposures were better suited to predict depressive symptoms, since the model fit – estimated with an adjusted R2 – was consistently higher compared to the models with psychological distress as the dependent variable.
Sensitivity analyses
When including all factors that showed significant associations with the given outcome in M1–M6 (due to the small sample size), most of the associations identified in previous models remained (Table 4, M7, M8). For depressive symptoms, being in work and a higher internal locus of control maintained protective effects, while family-to-work conflicts, lack of emotional and childcare-related support, and a stronger emotional connection still presented as potential risk factors. Decreases in household income and conflicts with the partner did not show any significant associations with depressive symptoms. For psychological distress, associations with household income as well as a lack of emotional and childcare-related support remained significant. The number of positive experiences was no longer associated with any of the outcomes.
Linear regression coefficients for depressive symptoms and psychological distress by occupational, psychosocial and partnership-related exposures that showed significant associations in Table 3, Bielefeld, Germany, 2020.

PHQ: Patient Health Questionnaire; SCL-K: short version of the Symptom Checklist; CI: confidence interval.
All estimates are adjusted for age, number of children and formal educational attainment.
In bold: coefficients with a p-value ≤ 0.05.
Variables from the BaBi baseline cohort.
Focusing on occupational-related factors only in women who engaged in paid work at the time of the survey, we additionally integrated changes at work in the regression models (see Supplemental material 5). However, these did not show any significant association with either of the two mental health outcomes.
Qualitative results
Seventeen women participated in the interviews (in addition to the survey). Of these, 12 were caring for their children at home during the data collection period. The remaining five participants’ children attended the ‘emergency care’. Most women were currently employed part-time (50%–75% of full-time work), while five were not working due to varying reasons (homemaker, maternity leave and unemployment). Fourteen of the partners were working in home-office, at least partially.
Work-to-family and family-to-work conflicts
Actional level
The daily working routine has massively changed for most of the mothers from the qualitative data set. One interviewee moved working time slots to the early mornings and established alternating shifts with her partner – with limited success as ‘that works out semi good at best’ (I: 16). Another interviewee (I: 2) outlined that she spent a part of her annual leave to compensate for cancelled childcare before qualifying for emergency day care as it ‘quickly became clear to [her] that childcare and normal work could not be reconciled’ (I: 2). Frequently interrupted work and requirements to be flexible placed expectations on mothers and their children, who were now expected to adapt, independently of their needs: As an executive assistant, I work on call, so I can’t schedule the work myself. Therefore, my son often has to take a back seat as my needs are to get done first. (I: 17)
As illustrated by those few quotes, experiences of conflict came to light during the interviews. The conflicts were directed both towards work duties (taking leave, working outside the usual hours) and the children (considerate behaviour, involuntary withdrawal).
Perceptual and emotional level
The simultaneity of working in home-office, caring for children and managing the household was perceived as an enormous burden by many of the interviewees who currently had a paid job. They articulated a loss of internal and external control, feelings of resignation and capitulation, felt highly stressed and struggled with the guilt of neither meeting their work demand nor their children’s needs: The multiple loads due to home office, home schooling, lack of daycare, the extra demands on the household [. . .], the extra demands on shopping [. . .] puts an extreme strain on me. I have the feeling that I can no longer get everything organized. (I: 13)
Family and work responsibilities were experienced as incompatible, highly stressful and challenging to manage. This concurrency of demands provoked physical stress reactions like ‘shaky hands and a racing heart’ (I: 16), and exhaustion and fatigue (I: 17) as women felt ‘torn between raising children and home office and yet [not being able to] do justice to either side’ (I: 16).
The society’s lack of appreciation for care work, absence of options for professional development and the extra burden that NPIs placed upon her led to resignation and frustration for this mother: In my life planning, it was always clear that I definitely wanted to have children. But I also wanted to remain employed at the same time. Despite various difficulties, I have never regretted the decision to realize both in the past 8 years. At the moment, however, I am asking myself whether I can keep this up for much longer and whether this balancing act is worth it at all. Professionally and socially, you don’t get any recognition for taking on the extra workload. [. . .] But now the burden is simply too great. Why should I continue to take it on? (I: 13)
Likewise feeling marginalized and overlooked as a double-working parent by societal debates and the media, another interviewee experienced anxiety about statements like ‘no kindergarten before the summer vacation starts’ (I: 16).
Overall, most women experienced strong tensions between the family and work domains, that were associated both on an actional, and a perceptual and emotional levels with conflicts and the feeling of being overwhelmed and not doing justice to any of the domains.
Quality of experiences and sense of well-being
Actional level
The interviews revealed that some women experienced the changes due to NPIs as beneficial to their personal well-being and their family life. A leitmotif that emerged in multiple interviews was the ‘forced deceleration’ that lead to a ‘more relaxed’ daily life with ‘less time pressure’ (I: 8) and ‘hardly any obligations besides work and family’ (I: 8). For many interviewees, the increase in shared quality time with their children and partners positively influenced their well-being: I haven’t felt so decelerated in a long time. We do things we’ve always wanted to do (hikes, bike rides, building a tipi, or just goofing off together in the garden). The kids do really great together, so despite working and taking care of the kids, there is always a bit of time for me. (I: 9)
Another woman expressed her relief about the absence of daily stress sources that for her emerged from social constraints and expectations of others. Now, that all the ‘everyday stress is gone’, she ‘can really look towards [herself] and only act for [herself], completely without social constraints’ (I: 5).
The opposite stance emerged from another set of interviews. Here, a mother described how the high and constant level of noise and the lack of breaks and recovery time put a strain on her (I: 1). Also, she found it more challenging to mediate upcoming conflicts: This requires a higher degree of soft skills on my part [. . .] my irritability with regard to certain recurring conflict situations has increased, simply because these situations occur more frequently when we spend the entire day together from morning to evening. (I: 1)
For another interviewee, the situation is ‘emotionally fluctuating’ as she experienced stronger irritability and tension in conflict situations, which led her to have unfair reactions and more scolding towards her children (I: 4). A development shared by another woman, who struggles with ‘days or hours when nothing works out, and the children sense the nervousness and the abnormality of the situation’ (I: 3).
Perceptual and emotional levels
Gratitude and a (new) sense of feeling privileged were brought up in some of the interviews. One interviewee has become aware of how well she and her family are doing thanks to their occupational and housing situation compared to others, as some ‘have a small apartment, no garden’, which ‘has to be stressful’ (I: 15). Another woman described how ‘the observation of deficits and restrictions all around’ made her realize how privileged and secure her situation was (I: 1).
One woman has ‘become more patient and therefore more emotionally stable’ and feels ‘recharged’ by being around her children (I: 5), while another highlights that she is now getting improved sleep ‘even if the night was bad, it doesn’t feel so bad because [she has] better chances to compensate’. A third one expresses happiness as she has so much time for self-care that she ‘would otherwise not have allowed’ herself (I: 9).
The opposite is felt by another (pregnant) woman who acknowledges that her feelings of exhaustion negatively impact her relationships. She depicts her emotional state as volatile and feels overwhelmed by anger or rage: This then triggers a guilty conscience, overwhelming feelings and sadness. In addition, I feel that I am not currently doing justice to the unborn child, which also triggers a lot of sadness and guilt. [. . .]. Physically, emotionally, and nervously, the situation is very stressful and actually puts a strain on all relationships. (I: 4)
Feelings of powerlessness and lack of control over the pandemic situation led to fear and anger for this woman and ‘as a result, [her] psychosomatic symptoms are on the rise again’ (I: 12). A comparable decline of emotional stability and rising overload was articulated by this mother, who felt overwhelmed by all the stimuli that she was not able to process anymore: I notice that I increasingly perceive situations as stressful and cannot process the stimuli properly or perceive them as too much at that time, which is what I often experience before a migraine. (I: 10)
For quality of experiences and sense of well-being, we saw a highly heterogeneous picture. Some women perceived the early phase of the pandemic as decelerating and rewarding in terms of being able to spend more time with their children and partners. These expressed a higher level of mental well-being. In contrast, some women experienced the period as stressful and reported a decrease in mental well-being, for example, exhaustion and feeling emotionally drained.
Partnership
Actional level
Concerning their intimate partnership, the (re-)organization of everyday life impacted most of the interviewees. Although conflicts around an unequal distribution of household tasks and mental load emerged (or intensified), this interviewee found common ground with her partner and did not perceive the fights as a threat to their partnership (I: 16): In the second or third week of the lockdown, there was a major discussion because my mountain of tasks had steadily increased while my husband continued to follow his usual activities but, from my perspective, was better able to ignore the extra workload than I was. Since then, our split has been mostly fair – it’s a very difficult situation for all of us, but I feel we are currently a good team. (I: 16)
Another interviewee is convinced that she and her husband ‘will continue to function as a team’, although they ‘will certainly argue at times’, but then ‘find a common ground’ as they can ‘can rely on each other and try to achieve a good structure’ (I: 10). Another interviewee explicitly stated that her ‘partnership suffers during this time’ as they are ‘only parents now, around the clock’ (I: 5).
Perceptual and emotional levels
While some women perceived that the intensity of their partnership has led to deepened interactions as they now ‘communicate more intensely’ (I: 6), has consolidated and is ‘less conflictual’ and ‘closer’ (I: 9), others showed a darker outlook into their future due to anticipated frictions in family life and partnership as they experience their husband ‘to be unbalanced, thin-skinned and bad-tempered’ (I: 12), which affects family life.
Summarizing the partnership domain, most women reported some kind of negotiation processes (either implicit or explicit) with their partners in order to adapt to the new situation. The experiences of these processes were again mixed: while some women felt a closer, more intimate connection, others were exposed to higher levels of conflicts.
Discussion
This mixed-method study provided new evidence on potential determinants associated with depressive symptoms, psychological distress and well-being among mothers of young children during the first wave of the COVID-19 pandemic in Germany. Our findings indicated that occupational, psychosocial and partner-related factors can act (to varying degree) both as resources and stressors to the self-reported mental well-being of mothers of young children. All interviews showed that the first NPIs have had an impact on the well-being of the participants. This impact took different forms. Depending on life (including work) circumstances, family situations, relationships and own psychosocial resources, the changes have created opportunities or challenges. The women finding joy or appreciation in a reassessment of priorities or re-evaluation of their lives were not marginal. Their testimonies showed that more proximity with children and teamwork with partners were sources of increased well-being. On the other hand, multiple demands and the simultaneity of role expectations and actions (as worker, mother, partner) were causing stress and irritability, which in turn lead to guilt, sadness or physical discomfort for some. Such findings were consistent with the survey findings, which highlighted the protective role of psychosocial resources and a healthy intimate partnership. These two elements, may be more than the occupational factors, seemed to be instrumental in the processing of the changes and their consequences on self-reported mental well-being.
With regard to occupational factors, our findings indicated that the risk of financial insecurities was associated with higher levels of depressive symptoms and psychological distress which is consistent with previous studies.25,73 In the occupational-specific regression model, employed women showed lower levels of depressive symptoms, which at first sight can be a surprising result, as those women were to a greater extent than non-employed women exposed to concurring role expectations as mothers and employees and consequently stress.6,74 Conflicting role expectations were shown to be highly stressful particularly for mothers and leading to exhaustion and fatigue in a German (n = 2278) 6 and Italian sample (n = 1226). 74 While the overlapping and (partly) conflicting demands of work, childcare and household were perceived as stressful as expressed in our qualitative sample, the conflicting role stress might relativize in the light of the general and profound deceleration experienced in daily ‘pandemic’ life. Social support, physical activity, nature connectedness and feelings of gratitude have all been shown to be protective factors for well-being during the COVID-19 pandemic. 75 These findings were further supported by our qualitative findings where women claimed to experience gratitude for having a more intense time with their families and additional time for self-care.
Our findings in relation to psychosocial factors showed that firmer internal locus of control led to lower levels of depressive symptoms but not significantly to lower levels of psychological distress. The latter might be due to the small sample size. Studies conducted in India, 76 Norway and Germany 77 found that internal locus of control was negatively associated with psychological distress in the general population during the COVID-19 pandemic. In addition, having a higher external locus of control was associated with significantly more symptoms of depression in adults of the United States of America and five European countries during the COVID-19 pandemic, 78 but did not reach statistical significance in our population. The qualitative results showed positive perceptions of the COVID-19 pandemic regarding fewer obligations besides work and family, increased quality time with family, gratitude for one’s privileges and fewer social expectations. Nonetheless, some mothers described more conflicts due to the uninterrupted being together, fewer occasions for retreat and an increase of unfair reactions due to stronger irritability or emotional imbalance similar to another study. 79
Results concerning partnership-related factors indicated that women who lacked support from their partner with childcare as well as emotional support showed higher levels of depressive symptoms and psychological distress. As documented in pre-pandemic studies, the degree as well as quality of father’s involvement is likely to impact a mother’s mental health,80,81 which corresponds to the findings in our study. Co-parental conflict and undermining parenting behaviour have been associated with maternal psychological distress and depression. 82 Our qualitative interviews reveal the importance of a perceived fair division of workload, reliance on the partner and the feeling of being a good team. While this was the case for some women, others noticed more irritable reactions, bad temper or sensitivities among their partners and anticipated more arguments in the future. The quality and extent of support of the partnership are essential to overcome childcare and emotional challenges and ultimately ameliorate the self-reported mental well-being. Surprisingly, the quantitative analysis suggested that feeling a stronger emotional connection with the partner increases the level of depressive symptoms, thereby contradicting our qualitative findings and the evidence presented before. Given the small sample size, our estimates were sensitive to changes in the regression models and these findings need further verification in larger cohorts. An Australian qualitative study (n = 2130) investigating the impacts of COVID-19 on family life shows, like in our study, how differently families can be affected. 79 It reveals that while some families report strained relationships up to separations, boredom and depressive moods, others experience deepened bonds, appreciation, gratitude and tolerance.
Regarding the sociodemographic characteristic that we adjusted for, we did not identify any effects on either of the outcomes. Yet, our qualitative findings (to a limited extent) and quantitative studies conducted in Germany83,84 and Europe73,85,86 indicate that socioeconomic position is an important determinant for the direct and indirect economic, social and health-specific consequences of NPIs and the available coping resources. One explanation why we did not observe a social gradient might be that our sample is (a) rather homogeneous in terms of being highly educated with a comparably high household income and (b) potentially too small to be able to detect effects of socioeconomic position.
Strengths and limitations
Mixed-methods research is well suited to address the increasing complexity of public health problems and their solutions, 87 which also applies to the analysis of the multi-dimensional influencing factors of mothers’ self-reported mental well-being during the COVID-19 pandemic. Through the quantitative analyses, we could estimate the association between resources and stressors and self-reported mental well-being, and the magnitude of the impact of the former on the latter. The email interviews captured the participant’s experiences during the pandemic in their own, chosen words and therefore explored the context of the ‘why’ and ‘how’ of our research interest. 88 While this article has a number of strengths, including the mixed-method design, the availability of a rich quantitative questionnaire and the use of validated mental health outcomes, several limitations must be considered. Our sample might be susceptible to selection bias, for example, we might not have been able to include women who felt completely overwhelmed by the situation or felt so pressed for time that participation was not possible. Yet, our sample still comprises women engaging in paid and unpaid work and especially for the qualitative interviews the willingness to participate was high (20 more participants volunteered, but since we had reached saturation, we did not conduct more interviews). Comparing our sample with the study population from the last BaBi cohort follow-up (in 2018), we see that our sample has a higher proportion of women with higher educational attainment, engaged in paid work, who reported higher monthly net household income, and did not have a migration background (Supplemental material 6). Even though some of these demographics are subject to change over time, they still give an indication of a potential selection bias. Another limitation pertains to the sample size. The response rate was acceptable with 22.5%, taking into account the NPIs and increased childcare demands at the time of the survey. The sample size does not allow for more in-depth analysis, for example, a comparison of the self-reported mental well-being impact of different factors for working women and those who are currently not engaged in formal employment. Moreover, there is little variance in terms of psychosocial factors, which might be one of the reasons why the models, except for those with depressive symptoms, have low R 2 values. Furthermore, the operationalization of the work variable without a focus on more specific work stressors (e.g. exact working hours, amount of perceived flexibility, support from employer) limits the explanatory power and the comparability with evidence focusing on work stress. For the email interviews, one strength was the practicability in terms of timing as the interviewees and interviewers conducted the interview asynchronously. The email interviews allowed for a prolonged engagement with the questions, opening the opportunity for a more reflective and thoughtful response process than verbal answers. One major limitation of our email interviews is the sample bias that determined who was first and foremost able to respond. As the interviews were collected online, participants needed to have a computer (or at least a smartphone) and the ability to express their thoughts in German. Another limitation lays in the risk of receiving very short or superficial responses. We noticed this in a few interviews that showed little depth and presented limited potential for qualitative analysis.
Conclusion
Occupational, psychosocial and partner-related factors can act (to varying degree) both as resources and stressors to the self-reported mental well-being of mothers of young children, depending on specific life circumstances, such as work or family situations, relationships and own psychosocial resources. Our findings, together with emerging literature in the field, highlight that any meaningful attempt at supporting their mental well-being should involve public health measures – including ongoing pandemic containment efforts, and workplace policies that contribute to the mitigation of those challenges, for example, by valuing unpaid care work and allowing more flexibility in work–life balance.
Supplemental Material
sj-doc-5-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-doc-5-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Supplemental Material
sj-docx-1-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-docx-1-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-docx-2-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-docx-3-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Supplemental Material
sj-pdf-6-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-pdf-6-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Supplemental Material
sj-xlsx-4-whe-10.1177_17455057221114274 – Supplemental material for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study
Supplemental material, sj-xlsx-4-whe-10.1177_17455057221114274 for Self-reported mental well-being of mothers with young children during the first wave of the COVID-19 pandemic in Germany: A mixed-methods study by Lisa Wandschneider, Stephanie Batram-Zantvoort, Anita Alaze, Vera Niehues, Jacob Spallek, Oliver Razum and Céline Miani in Women’s Health
Footnotes
Acknowledgements
The authors thank all the women who took the time to participate in this study. They would like to acknowledge their colleague Odile Sauzet from Bielefeld University for her valuable feedback on the data analysis strategy.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.