
Abstract
Objective:
Palpitations during peri- and post-menopause are common. It is unclear what variables are related to palpitations in peri- and post-menopausal women. The purpose of this scoping review was to summarize potential correlates of palpitations in women transitioning through menopause.
Methods:
The review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). Authors included English-language, full-length, peer-reviewed, cross-sectional research articles on palpitations in menopausal women published through December 18, 2021, from PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and PsycINFO searches. Following de-duplication, screening of titles and abstracts, and review of full-texts, independent reviewers extracted data on variables studied in relationship to palpitations from 84 articles and resolved discrepancies. Authors extracted data on (1) demographic, clinical, biomarker, and symptom/quality of life variables and (2) data analysis method (bivariate, multivariate). Authors classified each variable as a likely, unlikely, or unclear correlate of palpitations.
Results:
Articles were diverse in region of origin, sample sizes, and variables assessed in relationship to palpitations. Evidence for any one variable was sparse. Likely correlates of palpitations included race/ethnicity, lower physical activity, worse vasomotor symptoms (VMSs), worse sleep, and worse quality of life. Unlikely correlates included age, employment, education, marital status, socioeconomic status, comorbidities, body mass index, and sexual difficulties. Unclear correlates due to equivocal evidence were menopausal status, smoking, and depression. Unclear correlates due to insufficient evidence (less than three articles) included all of the assessed biomarkers, anxiety, and stress.
Conclusion:
Likely correlates were identified including race/ethnicity, physical activity, VMS, sleep, and quality of life. However, additional research is needed to better understand potential correlates of palpitations.
Introduction
About 21 million women living in the United States today, and 1.1 billion women worldwide by 2025 will experience menopause symptoms. 1 Menopause symptoms can begin in perimenopause (when menses become irregular) and last into the postmenopause (when menses stop for 12 or more months). Women’s individual experiences vary, 2 but up to 75% of women report vasomotor symptoms (VMSs, hot flashes, night sweats). 1 Studies suggest VMS and other menopause symptoms, such as sleep and mood disturbances, can last 10 years (range = 0–15+ years) during the transition from peri- to post-menopause.1,3
Many menopause symptom checklists include palpitations (e.g. rapid, irregular, and/or exaggerated heartbeats), 4 and research suggests palpitations are relatively common. Up to 42% of perimenopausal women and 54% of postmenopausal women report having palpitations. 5 However, although 44%–87% of women aged 40–59 years believed their palpitations required treatment, 6 a systematic review found no Level 1 evidence for managing menopause palpitations. 7 This and other evidence suggests palpitations in peri- and post-menopausal women are common yet relatively understudied in comparison to VMS,4,5,7 may be normalized and/or trivialized like other menopause symptoms, 8 and have been mostly attributed to psychosomatic (e.g. anxiety, stress) rather than cardiac causes. 9
Understanding more about palpitations in peri- and post-menopausal women is important. In the general population, palpitations account for 16% of primary care visits and are the second leading reason for cardiologist visits. 10 Women are more likely than men to report palpitations during outpatient visits, 11 emergency department visits, 11 and during acute cardiac events.12,13 However, there has been a historical and well-documented bias against women in cardiology with poor understanding and/or trivialization of symptoms, such as palpitations, that results in missed or delayed diagnosis of cardiac events. 14
It is unclear what demographics, clinical variables, biomarkers, and/or symptom/quality of life (QOL) outcomes are related to palpitations. Our team found no review of correlates of palpitations in peri- and post-menopausal women. Understanding correlates that are related to palpitations can help researchers control potential confounding variables and potentially identify avenues for mechanistic research to understand the pathophysiological underpinnings of palpitations. Furthermore, understanding such mechanisms as well as understanding modifiable correlates can help guide the development of interventions to alleviate the symptom. A logical first step to understand correlates of palpitations is to review the literature and map or synthesize evidence.
Therefore, the purpose of this scoping review was to systematically map what is currently known and unknown about correlates of palpitations in peri- and post-menopausal women to guide future research and clinical practice. We focused on correlates in cross-sectional studies rather than risk factors or predictors because of the scarcity of longitudinal studies on the topic (n = 2 articles). 5 Our goal was to fully map the current state of the science related to potential correlates of palpitations in peri- and post-menopausal women. Our questions were as follows: (1) what demographics, clinical variables, biomarkers, and/or symptom/QOL outcomes have been studied in relation to palpitations in peri- and post-menopausal women? (2) What is the evidence for these associations from bivariate and multivariate statistical tests? (3) What variables are likely, unlikely, or unclear correlates of palpitations based on review findings regarding the number of articles assessing each association, type of statistical tests performed, and article results?
Methods
Protocol
The scoping review methodology was the review methodology most closely matching the goal and research questions. Scoping reviews can be thought of “reconnaissance” to determine boundaries of what is known and unknown on a topic and are most useful when other literature reviews are lacking. 15 They are intentionally broad and differ from systematic reviews that focus on subsets of articles that are narrowly defined and pass quality filters. 16 Scoping reviews aim to visually map available evidence using tables or figures.15–17 Thus, scoping reviews are useful for identifying gaps in the field for future research and may or may not be used as a stepping stone in conducting future systematic reviews or meta-analyses.15,17
This scoping review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Review (PRISMA-ScR, see Supplementary A). 17 The authors did not register the review protocol as this step is not required for scoping reviews. 17 Ethics board approval was not applicable because the review did not meet criteria for human subjects’ research. 18
Eligibility criteria
Articles included in the review needed to be English-language, full-length, peer-reviewed, cross-sectional, descriptive research on palpitations (or similar symptoms such as racing heart), in menopausal women (per accepted nomenclature for defining perimenopause and postmenopause),19–21 and reported results of testing at least one variable in relation to palpitations. Studies that included pre-menopausal women as a comparison group were included but those that focused solely on premenopausal women were excluded.
Articles excluded from the review were not full-length (e.g. abstracts), not data-based (e.g. editorials), studies of other populations (i.e. adolescents or other premenopausal women, transgender or gender transitioning populations, men, or animals), studies where populations were labeled as “menopausal women” or “symptomatic women” without further clarification or definition of menopausal status, and studies that provided data on palpitations but did not assess at least one variable in relation to palpitations. Regarding factor analytic studies, we excluded those where the only relationships assessed were inter-item correlations from a single scale (e.g. factor analyses of a symptom checklist in psychometric studies) and included those that assessed at least one other variable.
Information sources
An experienced librarian performed the searches. The librarian drafted the initial search strategies and further refined them after team discussion. The final literature searches included all articles published through December 18, 2021. The librarian used three gold standard biomedically focused databases selected for their breadth: PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), and PsycINFO. Because of the health-related focus of the review, authors did not search outside the biomedical literature (e.g. Scopus which contains general science journals as well as textbooks, abstracts, and other non-full-length writings, or the Education Resources Information Center (ERIC)).
Search strategy
The search strategy relied on the National Library of Medicine Medical Subject Headings terms and keywords: (“Menopause” OR menopaus*) AND (palpitation* OR heart racing OR heart pounding OR irregular heart). The word “palpitations” was too specific to locate pertinent articles, and therefore, we searched for the articles that used standard menopause symptom assessment tools known to assess palpitations. 4 These included the Blatt–Kupperman Index,22–24 the Greene Climacteric Scale, 25 the Heinemann Menopause Rating Scale, 26 the Holte/Mikkelsen Menopause Checklist, 27 Hunter’s Women’s Health Questionnaire, 28 the Menopausal-Specific Quality of Life (MENQOL) scale, 29 the Menopause Symptom Checklist, 30 the Midlife Women’s Symptom Index, 31 Neugarten and Kraines’ Symptom Checklist, 32 and the Study of Women’s Health Across the Nation menopausal symptom scale. 33 The final electronic search strategies are shown in Supplementary B.
Selection of sources of evidence
Authors used a structured program available at Covidence.org to de-duplicate articles and track progress on the screening and full-text review processes. After de-duplication, four reviewers working in pairs screened article titles and abstracts to determine if they met criteria for inclusion or exclusion. The reviewers discussed screening disagreements and achieved consensus through group discussion. Reviewers were overly inclusive at this screening stage and retained articles that referred to menopausal symptoms in general, as we could not determine whether menopausal symptoms included palpitations. Next, four reviewers working in pairs performed full-text review. At this stage, reviewers were more selective and excluded articles that did not include data on palpitations or did not assess at least one potential variable in relation to palpitations. The reviewers discussed disagreements on full-text review and reached consensus after group discussion.
Data charting methods
Two reviewers developed a data-extraction form in Microsoft Excel. Four reviewers working in pairs extracted data from approximately 10 articles, met to discuss the process, and updated the data charting form with additional details. For all articles, one author performed extraction and at least one additional author verified accuracy. Each row represented an article, and each column contained data about the article.
Data items
There were four types of data extracted. First, authors extracted general information about the articles including author, title, country of origin, and sample size. Second, authors extracted information on variables assessed in relationship to palpitations within articles. Authors applied a simple four-category taxonomy to organize correlates during the data extraction process: (1) demographics, (2) clinical variables, (3) biomarkers, and (4) symptoms/QOL. The list of variables under each of these headings can be found in the results’ tables. Third, authors extracted whether evidence was based on bivariate or multivariate test statistics. Bivariate tests for association included chi-square tests, Mann–Whitney U tests, t-tests, analysis of variance, or univariate logistic regression. Multivariate or multivariable tests for association included multiple logistic or multiple regressions that controlled for confounders. If bivariate and multivariate results differed within a study, we report only the higher level adjusted multivariate results. Fourth, during data extraction, authors noted some articles provided data on tests of interactions between variables, and therefore extracted data on those interactions. Significant interactions indicated that a relationship between two variables depended on a third variable. Reviewers met to resolve disagreements and achieved consensus through discussion. Our data extraction table is available upon request.
Critical appraisal and summarization
To determine the amount of evidence available, authors counted the overall number of articles that assessed an association between palpitations and each variable. They then determined the number of articles that did and did not show evidence of association at the bivariate and multivariate levels. At this stage, to facilitate communication among authors and ease summarization, all variables were listed in terms of what worsens palpitations (e.g. older age, lower physical activity).
We then developed criteria to classify each variable as a likely, unlikely, or unknown correlate of palpitations as we were unable to find published criteria. Likely correlates were those supported by significant associations in at least 60% of three or more studies. Unlikely correlates were those assessed but not statistically significant in at least 60% of three or more studies. Conversely, unclear correlates were those where there was either (1) equivocal evidence (less than 60% evidence in three or more studies) or (2) an insufficient number of articles (less than three articles).
Risk of bias
PRISMA-ScR does not require risk of bias assessments in scoping reviews. 17 Other scoping review guidelines discourage inclusion of literature based on risk of bias as the nature of a scoping review is to review and map available evidence, rather than a limited number of studies meeting bias criteria. 16 For these reasons, risk of bias was not assessed.
Results
The PRISMA in Figure 1 shows the flow of records. Of 822 records screened, 632 proceeded to full-text review. Of the 632, a total of 84 articles met criteria for inclusion and were included in this review.33–116 Most articles were excluded for not reporting palpitations-specific data (n = 399). Consistent with inclusion criteria and the dearth of longitudinal studies discussed earlier, all of the included articles (100%) were based on cross-sectional data analysis.
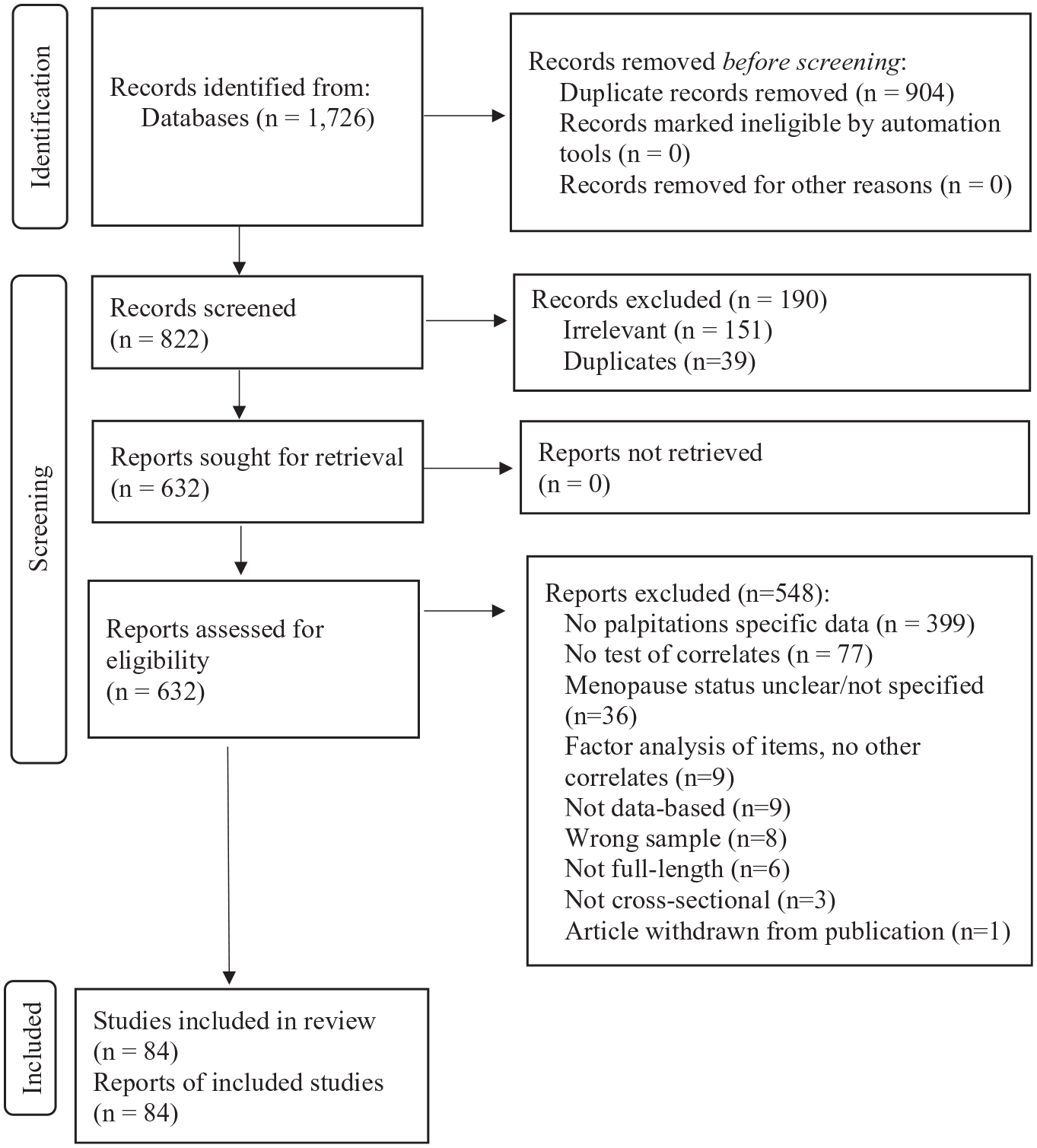
PRISMA flow diagram of records.
Table 1 shows descriptive information about the articles. Only 2% of articles included the word “palpitations” in the title.47,58 Articles originated from multiple regions, most frequently from Asia (East, North, South East, South total n = 31, 37%). Only one article included participants from multiple world regions. Sample sizes varied from less than 200 to over 5000, with between 200 and 500 participants being most common (43%). The upper age range of participants was between 50 and 65 years old in most articles (n = 58, 69%), was greater than 65 in 15 articles (18%), and was not specified in 11 articles (13%) (data not shown). Clinical variables were most frequently studied in relationship to palpitations (77%) followed by demographics (20%), symptom/QOL variables (19%), and least commonly biomarkers (6%). No studies (0%) included all four categories of variables.
Descriptive information about the reviewed articles (n = 84).

QOL: quality of life.
Exceeds 100% because articles could contain more than one category of correlates.
Likely correlates of palpitations
As shown in Table 2, five variables emerged as likely correlates of palpitations. They included one demographic (race/ethnicity), one clinical (less physical activity), and three symptom/QOL variables (worse VMSs, worse sleep, poorer QOL). The number of studies testing each variable ranged from 3 (VMS) to 11 (race/ethnicity). Among studies testing a given correlate, the percentages of studies showing evidence of association were 73% for race/ethnicity, 63% for lower physical activity, 67% for VMS, 75% for worse sleep, and 67% for poorer QOL. Most evidence of association was based on bivariate statistical tests for race/ethnicity, physical activity, and sleep and on multivariate tests for VMS and QOL.
Likely correlates of palpitations in peri- and post-menopausal women based on number of articles, type of statistical tests, and article results with citations.

Bi: bivariate tests for association such as chi-square tests, Mann–Whitney U tests, t-tests, analysis of variance, or univariate logistic regression; multi: multivariate or multivariable tests for association such as logistic or multiple regressions that controlled for confounders; QOL: quality of life; VMS: vasomotor symptom.
Superscripted numbers are the article reference citations.
Race/ethnicity
Greater versus lesser palpitations were found in Hispanic versus White women (p < .05),33,97 Black Columbian versus non-Black Columbian women (p = .003), 82 Black versus Hispanic Ecuadorian women (p < .001), 83 Quechua versus Zenu women (p < .0001), 87 Lebanese versus Spanish, Lebanese, or American women (p < .01), 98 and Turkish versus German women (p < .001). 110 There was a significant difference in palpitations across women of Malay, Indian, and Chinese descent living in Malaysia, but the details were not specified. 34 In contrast, no differences in palpitations were reported between Mosuo versus Han Chinese women in a bivariate analysis 115 or non-Hispanic Whites versus other racial groups in the United States in bivariate 47 or multivariate analysis. 66
Physical activity
Greater palpitations were associated with lower physical activity in five studies.33,39,45,46,67 Greater palpitations were related to somewhat and much less physical activity versus much more physical activity, 33 a sedentary versus active lifestyle, 45 less physical activity overall, 46 and seldom versus daily or one to three times a week exercise. 67 Similarly, lesser palpitations were associated with greater moderate-to-vigorous physical activity. 39 In contrast, in three articles, there were no significant differences in palpitations across low, moderate, and high physical activity groups54,104 or between those who did and did not report regular exercise. 58
VMS and sleep
Greater palpitations were associated with having VMS43,58 and sleep problems (poor sleep including having nightmares at least once a week, 40 greater insomnia, 47 and overall sleep quality and disturbances). 105 In contrast, palpitations were related to VMS bother (but not VMS frequency) in bivariate but not multivariate models. 47 Similarly, although palpitations were associated with more sleep complaints in bivariate analyses, findings did not hold in multivariate analyses. 48
QOL
Greater palpitations were associated with poorer menopausal QOL, 47 poorer physical (but not mental) component QOL, 53 poorer sleep-related QOL, 56 and poorer occupational QOL. 56 In contrast, palpitations were not related to general 51 or sexual 61 QOL.
Unlikely correlates of palpitations
As shown in Table 3, eight variables were not likely related to palpitations. They included five demographic (age, employment/occupation, education, marital status, socioeconomic status (SES)/income), two clinical (comorbidities, body mass index (BMI)), and one symptom/QOL variable (sexual dysfunction/inactivity). The number of studies testing each ranged from 3 (SES) to 11 (comorbidities). The percentages of studies showing no evidence of association were 100% for age, 100% for employment, 80% for education, 80% for marital status, 67% for SES, 100% for comorbidities, 63% for BMI, and 75% for sexual dysfunction. Tests of association were evenly split between bivariate and multivariate tests for education and marital status; were predominantly bivariate for age, comorbidities, and BMI; and were predominantly multivariate for employment, SES, and sexual function.
Unlikely correlates of palpitations in peri- and post-menopausal women based on number of articles, type of statistical tests, and article results with citations.

Bi: bivariate tests for association such as chi-square tests, Mann–Whitney U tests, t-tests, analysis of variance, or univariate logistic regression; multi: multivariate or multivariable tests for association such as multiple logistic or multiple regressions that controlled for confounders; SES: socioeconomic status; BMI: body mass index; QOL: quality of life.
Superscripted numbers are the article reference citations.
Age, employment/occupation, education, marital status, and SES/income
Greater palpitations were consistently not related to age33,47,58,68,85,86,103 or employment/occupation.33,34,65,68,85 Greater palpitations were not related to lower education in four of five studies.47,65,68,85 Greater palpitations were not related to marital status in bivariate34,47 or multivariate33,85 analyses. However, being divorced was associated with higher palpitations severity in one multivariate analysis. 68 In two of three studies, palpitations were not related to lower socioeconomic status 85 or income. 68 In the third article, greater palpitations were associated with greater difficulty paying for basics when controlling for other variables. 33
Comorbidities
For clinical variables, greater palpitations were consistently not related to the presence or absence of the following comorbidities: human immunodeficiency virus,36,59,78 osteopenia/osteoporosis, 37 metabolic syndrome,49,74 atherosclerosis, 58 arrhythmias, 58 risk of sarcopenia, 62 diabetes, 84 thyroid tumor, 86 and Celiac disease. 96
BMI
Greater palpitations were not associated with BMI in four articles33,58,72,95,104 and in the remaining three articles, findings were contradictory. One study showed reduced odds of palpitations with higher BMI 47 whereas other studies showed increased odds of palpitations with higher BMI (e.g. BMI greater than 23 (vs less than 20 or 20–23) 67 or obese BMI (vs underweight or normal or overweight)). 76
Sexual activity and function
Greater palpitations were not related to sexual activity61,76 or sexual function. 109 In another article, greater palpitations were significantly related to sexual dysfunction (total scores and subscales of infrequency, non-communication, dissatisfaction, avoidance, non-sensuality, vaginismus, and anorgasmia) in surgically menopausal women but not naturally menopausal women. 108
Unclear correlates of palpitations
Equivocal evidence
As shown in Table 4, a sufficient number of articles showed equivocal evidence for two clinical variables (menopause status, smoking) and one symptom (depression).
Unclear correlates of palpitations in peri- and post-menopausal women based on equivocal evidence as determined by number of articles, type of statistical tests, and article results with citations.

Bi: bivariate tests for association such as chi-square tests, Mann–Whitney U tests, t-tests, ANOVA, or univariate logistic regression; multi: multivariate or multivariable tests for association such as multiple logistic or multiple regressions that controlled for confounders; post: postmenopausal; peri: perimenopausal; pre: premenopausal; surg: surgically; nat: naturally; QOL: quality of life.
Past smoking increased odds of palpitations (↑), and past and current smoking decreased odds of palpitations (↓).
Superscripted numbers are the article reference citations.
Menopause status
Menopause status was the most commonly studied variable, and evidence was split 50/50 in favor of and against an association with palpitations. The evidence favoring an association generally showed greater palpitations with advanced menopausal stage (e.g. postmenopausal more symptomatic than premenopausal,41,42,44,52,94,113,114 or perimenopausal,44,52,93 post-/peri-menopausal combined more symptomatic than premenopausal,75,79,80,88 perimenopausal more symptomatic than premenopausal33,44,52,76,85,90,91,113,114,116). However, in other studies, evidence for association was reversed (e.g. perimenopausal more symptomatic than postmenopausal) or absent.38,40,47,56–58,64,67,68,70,73,86,92,99,101,102,106,107,111 In addition, three of four studies showed greater palpitations in surgically menopausal women compared to naturally postmenopausal55,63 or premenopausal women, 33 whereas a fourth study showed no association. 108
Smoking
Findings for smoking were equivocal. Past smoking versus never smoking increased the odds of palpitations, 33 both past and current smoking reduced the odds of palpitations, 47 and smoking more than 20 cigarettes per day was not associated with palpitations. 58
Depression
Findings for depression were equivocal. Depression was associated with greater palpitations in two articles47,60 but not two others.41,58
Insufficient number of articles
As shown in Table 5, there were an insufficient number of articles (less than three) for multiple clinical variables, biomarkers, and some symptoms.
Unclear correlates of palpitations in peri- and post-menopausal women based on insufficient evidence as determined by number of articles, type of statistical tests, and article results with citations.
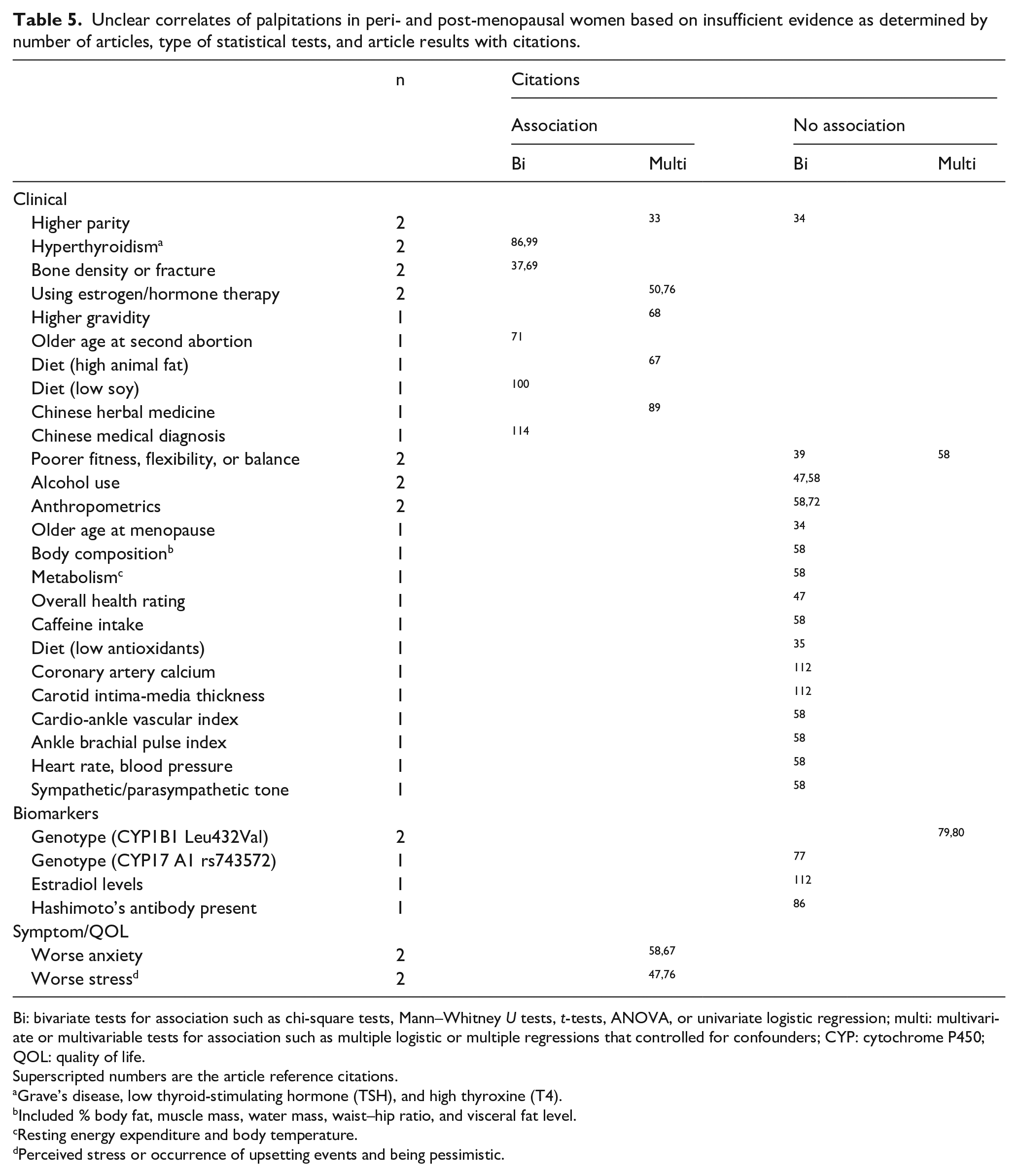
Bi: bivariate tests for association such as chi-square tests, Mann–Whitney U tests, t-tests, ANOVA, or univariate logistic regression; multi: multivariate or multivariable tests for association such as multiple logistic or multiple regressions that controlled for confounders; CYP: cytochrome P450; QOL: quality of life.
Superscripted numbers are the article reference citations.
Grave’s disease, low thyroid-stimulating hormone (TSH), and high thyroxine (T4).
Included % body fat, muscle mass, water mass, waist–hip ratio, and visceral fat level.
Resting energy expenditure and body temperature.
Perceived stress or occurrence of upsetting events and being pessimistic.
Clinical variables
There was evidence for 33 and against parity 34 and some evidence of association for hyperthyroidism,86,99 lumbar 1–2 bone density or fracture,37,69 use of estrogen or hormone therapy,50,76 higher gravidity, 68 older age at second abortion, 71 diet (e.g. high animal fat, 67 low soy 100 ), use of Chinese herbal medicine, 89 and having a Chinese medical diagnosis of Yang-xu. 114 In contrast, there was no evidence of association for poorer fitness, flexibility, or balance,39,58 alcohol use,47,58 anthropometrics,58,72 older age at menopause, 34 body composition, 58 metabolism, 58 overall health rating, 47 caffeine intake, 58 diet (low antioxidants 35 ), coronary artery calcium, 112 carotid intima-media thickness, 112 cardio-ankle vascular index, 58 ankle brachial pulse index, 58 heart rate, blood pressure, 58 and sympathetic/parasympathetic tone. 58
Biomarkers
There was no evidence of association between palpitations and genotypes cytochrome P450 CYP1B1 Leu432Val79,80 or CYP17 A1 rs743572, 77 estradiol concentration, 112 or presence of Hashimoto’s antibody. 86
Symptoms
For symptoms, there was some evidence that greater palpitations were associated with anxiety58,67 and stress.47,76
Discussion
This scoping review summarizes evidence surrounding what is known and unknown about demographic, clinical, biomarker, and symptom/QOL variables in relationship to palpitations in peri- and post-menopausal women to guide future research and clinical practice. The scoping review was appropriate for this task as there were a plethora of variables with varying degrees of evidence for and against associations. By scoping (or mapping) the number of articles, type of statistics used to assess association, and article results, we were able to summarize variables that were likely, unlikely, or unclear correlates of palpitations in this population of women. There were limitations in the reviewed articles, including sparse evidence for any one variable and statistical testing at the bivariate level without control for potential confounders.
The reviewed articles were diverse in country of origin, sample size, and variables assessed. Although palpitations were rarely the main focus (as evidenced by lack of inclusion of the word palpitations in the title), there appears to be global interest in assessing palpitations in peri- and post-menopausal women. However, evidence from one part of the world may not generalize to others. Geographical and racial/ethnic differences may have contributed to variability in findings related to correlates other than race/ethnicity across studies. Although sample sizes varied, most studies (80%) included 200 or more subjects suggesting there was sufficient statistical power to find significant associations between variables and palpitations. Finally, differences across variables assessed suggest there is little consensus on which variables are important when conducting research on palpitations in peri- and post-menopausal women. The fact that no study assessed all four categories of variables suggests there may be a need for a comprehensive analysis of demographic, clinical, biomarker, and symptom/QOL correlates of palpitations in this population.
Findings that palpitations varied by race/ethnicity are not surprising, given that individual differences in other menopausal symptoms exist across racial/ethnic groups. In many of the reviewed articles, palpitations were rarely the only menopausal symptom noted to vary by race/ethnicity. For example, findings from the Study of Women Across the Nation showed multiple symptoms varied by race/ethnicity: more frequent reports of VMS in Black women compared to White women, more forgetfulness in Hispanic women compared to non-Hispanic White women, and more sleep difficulties in White women compared to all other groups. 33
Less physical activity was a likely correlate of palpitations, yet other indicators of physical health tended to show no association with palpitations (e.g. BMI, poorer fitness, flexibility, balance, anthropometrics, or presence of various comorbidities). These differences could be true or due to variations across sample inclusion criteria or ceiling effects on measures in healthy women.
The relationships between palpitations and VMS and sleep problems may be due to greater symptom reporting in some women and/or a shared underlying mechanism. Some authors describe palpitations as part of what is experienced during VMS 117 and VMS are well-known to disrupt sleep. Given the dearth of biomarkers studied in the reviewed articles, additional research is needed to tease apart any potential shared mechanism underlying this trio of symptoms.
The relationship between palpitations and QOL is not surprising. Many menopausal symptoms, including VMS, disrupt a woman’s QOL. The association between palpitations and QOL was similar across different QOL constructs and measures (e.g. menopause QOL, 47 physical component QOL, 53 sleep-related QOL, 56 and occupational QOL), 56 yet there was only one study for each of these measures. Review findings suggest palpitations may be important to women’s QOL; however, additional research to confirm the association is needed.
The lack of information about palpitations in relation to subclinical or overt cardiovascular disease is notable. In the general population, palpitations that affect sleep and work 118 and occur more frequently 119 are more likely to be associated with serious, life-threatening arrhythmias. Only two articles tested associations between palpitations and indicators of cardiac health.58,112 Only one study examined palpitations and arrhythmias and found no association. 58 Much more research will be needed to understand if palpitations experienced during peri- and/or post-menopause are associated with electrocardiographic abnormalities, subclinical cardiovascular disease, or life-threatening cardiac events.
The lack of information about palpitations in relation to biomarkers is also notable. There is little evidence mapped in this review that is relevant to potential physiological mechanisms of palpitations. This scoping review suggests that the field has not yet advanced in the direction of understanding pathophysiological mechanisms of palpitations. Further research on mechanisms of palpitations seems to be warranted.
There were some strengths and limitations to this review. For strengths, the review was based on multiple search engines and pre-specified inclusion criteria to locate pertinent articles. A team of authors carefully screened, reviewed, and extracted data. Two to three individuals were involved at all stages of the review. For limitations, only English-language articles were included. There may be additional evidence in articles written in languages other than English. “Palpitations” is not yet a standard MeSH term, and this could have led to the omission of some articles. The word’s omission as a standard search term is unfortunate and may reflect the historical trivialization and/or understudied nature of palpitations at menopause. VMS are another historically trivialized menopause symptom, 8 and an MeSH keyword “hot flashes” was not added until the late 1990s 120 after decades of research on VMS had been conducted. Finally, the classification as likely, unlikely, or unknown correlate was based on author-developed criteria as we were unable to find a published reference using a similar standard.
Conclusion
In summary, this review mapped and summarized a wide variety of demographic, clinical, biomarker, and symptom/QOL variables in relationship to palpitations in peri- and post-menopausal women. The review highlights the need for additional research to understand cross-sectional and longitudinal relationships between variables identified in this review and menopausal palpitations to guide future research and clinical practice.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221112267 – Supplemental material for Correlates of palpitations during menopause: A scoping review
Supplemental material, sj-docx-1-whe-10.1177_17455057221112267 for Correlates of palpitations during menopause: A scoping review by Janet S Carpenter, Ying Sheng, Caitlin Pike, Charles D Elomba, Jennifer S Alwine, Chen X Chen and James E Tisdale in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221112267 – Supplemental material for Correlates of palpitations during menopause: A scoping review
Supplemental material, sj-docx-2-whe-10.1177_17455057221112267 for Correlates of palpitations during menopause: A scoping review by Janet S Carpenter, Ying Sheng, Caitlin Pike, Charles D Elomba, Jennifer S Alwine, Chen X Chen and James E Tisdale in Women’s Health
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr J.S.C. wishes to disclose personal fees from the University of Wisconsin Milwaukee, Simumetrix, and Mapi Research Trust. Ms C.P., Mr C.D.E., Ms J.S.A., and Drs Y.S., C.X.C., and J.E.T. have no conflicts to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible with support of: (1) an Indiana University Ethel Clarke Fellowship, (2) a Collaboration in Translational Research Grant from the Indiana Clinical and Translational Sciences Institute (Carpenter/Tisdale, multiple principal investigator) funded, in part, by grant no. UL1TR002529 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award (S. Moe, principal investigator), and (3) Dr Sheng’s postdoctoral fellowship under 5T32CA117865 (V. Champion, principal investigator). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.