
Abstract
Background:
Women experiencing substance use during their pregnancies or after the birth of a child report being fearful of losing their children based on care, stigmatized when seeking assistance, and barriers to care such as having to provide the same information to different providers, and having to repeat their lived experiences with substance use in detail. Particularly these service barriers can be confusing, complicated, and difficult to follow, which could lead to non-compliance or not seeking services.
Objectives:
We evaluated components of a service coordination program for women experiencing substance use, their children, and larger families who help with caregiving. We examined stakeholder interest in the program, feasibility providing services over time, and initial program effectiveness.
Design:
Participant enrollment and outcomes as well as service coordination activities provided over a 4-year period was gathered across three demonstration site locations (a birthing hospital, reunification program, and home visiting program).
Methods:
Program information was gathered from needs assessment data, health survey data from enrolled caregivers and infants, training evaluations, and budget recordings of direct aid. In this mixed method design, we examined potential differences between baseline and the last assessment for women and children enrolled in the program. We also utilized univariate analyses of variance to examine the main effects of maternal and infant characteristics on final maternal and infant outcomes.
Results:
Three sites enrolled 182 women and families for program services. Patient navigators provided direct aid, training, goal setting, and service coordination and planning. Families remained in the program, on average, 655 days and were satisfied with the services received. Respondents thought the program elements were easy to implement within the rural setting. The program effectively addressed basic needs, violence (p < 0.001; η2 = 0.34 (0.05–0.53)), infant development (p < 0.02; η2 = 0.51 (0.13–0.61)), and maternal depression (p < 0.05; η2 = 0.9 (0.00–0.22)). Select outcomes did differ by site.
Conclusion:
A service coordination model utilizing a patient navigator role to coordinate client services coupled with an approach that serves the infant and caregiver needs was feasible and desirable by all stakeholders within a rural setting. Service coordination effectively impacted select caregiver and infant outcomes.
Plain language summary
Introduction
Nearly 5% of women in the United States use one or more substances during pregnancy. 1 Alcohol, nicotine, and marijuana are the most used substances during this period, but cocaine and opioid usage has been quickly increasing over the past decade.2,3 Information on substance cessation rates during pregnancy is limited and varied based on the substance. Many women who have used substances, particularly illegal substances, prior to being pregnant abstain from those substances during pregnancy and through the early months postpartum. 4 Unfortunately, relapse rates begin to increase later in postpartum (6–12 months) and have been associated with increased life stressors (e.g., childcare needs, work demands). 5
Women and families living in rural, underserved areas experience unique challenges that relate to limited variability in services, limited access to services that exist near them, and declining quality care due to understaffed workgroups and healthcare professional shortages. 6 These structural and systemic challenges coupled with transportation barriers and socioeconomic limitations enhance the vulnerability of this population. Collectively, these barriers limit opportunities to identify women’s and their infants’ needs, appropriately respond to those needs, and intervene to decrease important health indices such as depression, continued substance use, and parent and attachment opportunities. 7
Increasing access for women to substance use treatment programs (during or after pregnancy) is a step toward decreasing maternal and infant health issues postpartum. 8 Substance use programming for mothers has shifted from a primarily behavior-based approach to a holistic model so that providers identify and potentially address the complex condition of substance use and multiple areas of an individual’s life. 9 Patient- and family-centered approaches are increasingly recommended to incorporate the realistic stressors that impact women and young mothers. 10 Changes to our service models and approach have generally recommended flexibility, a tailored infrastructure, a system that is supported by funding and expertise to help mothers coordinate the services offered to them and work with them to build their self-advocacy skills required to request the care they need during this critical time.
The most recent recommendations from holistic models of care have proposed systems that would allow teams to communicate with one another and reduce duplication of paperwork or burden on women with young children. Feedback from rural health efforts have proposed personnel (e.g., Community Health Workers) who would work with women to navigate the services and link to those that address gaps in their area. 11 Lastly, research from the past two decades and most recently, efforts from the Centers for Medicare and Medicaid Services, have explored the benefits of addressing an individual’s basic needs including physiological needs (housing, utility support, transportation; food insecurity) and safety and security (interpersonal violence) to support for patients’ basic needs to short and long-term health outcomes.12,13 Despite this growing evidence for a more comprehensive treatment approach for women who use, or have used substances with young families, these practices remain unavailable as they require additional financial supports and policy changes for insurance coverage. Programs described in the current literature have offered a patient navigator model to support patients with substance use disorders who are experiencing emergency department services 14 or have explored the potential of using a navigator in emergent situations like COVID through qualitative studies. 15 Much of this work has focused only on the mother rather than on the family unit at large. Existing research has also not vastly considered using the navigator coordination model to connect existing community services.
This study’s purpose was to describe the components of a service coordination program for biological parents and caregivers experiencing substance use during pregnancy and postpartum period (IMPACT WV, Morgantown, WV, USA). The program was specifically designed for rural settings and delivered across three different sites, which included a birthing hospital, a home visiting program, and a family reunification program. Program delivery and impact were examined for the entire sample but also across three different sites where participants were enrolled: a birthing hospital; a home visiting program; and a family reunification program.
Methods
Participants
Patient navigators recruited participants for this study from three different sites within a nine-county region from 2021 to 2023. Women were eligible to enroll in the program if they: (1) had given birth within the last 3 months, (2) had or still were using illegal substances, and (3) lived in one of nine counties in a northern region in West Virginia (WV). Women and infants could be enrolled at any time and followed up to the end of the program or their infants’ third birthday (whichever came first). Therefore, this was a longitudinal cohort study of women–infant dyads during the postpartum period. Women who had not used illegal substances, lived outside of the nine counties, or did not give birth to an infant within the past 3 months were not eligible to enroll.
Procedures
If eligible, women received information about the program and consented if interested. Women and families who consented to participate received incentives at: enrollment, 3-, 6-, 12-, and 18-months. Incentives included commonly needed infant care items (e.g., clothing, diapers, blankets) and/or a gift card. The patient navigator worked closely with enrolled women and families while in the program. Specifically, they identified providers and services that addressed reported needs for the mother, infant, and/or other caregivers within the family (two-generational services). Patient navigators also worked with families to address social service needs (housing, transportation, utility closure, interpersonal violence, food insecurity) if identified over time. Navigators also worked closely with all service providers and the family to identify ways to decrease duplication for the family, increase coordination of services, identify gaps in services and providers to fill those gaps, and address any confusion in the process. All procedures for this study were reviewed and approved by the West Virginia University Institutional Review Board (protocol #: 1904533886 and 2201501210).
Measures of interest
Program components included direct aid for emergency situations, training and technical assistance (TA), goal setting support, and referral/connections to other services. Direct aid was measured as the total amount of funding support provided to women enrolled in the program (overall and by site) and the type of support provided. Training and TA included attendance at available trainings for enrolled families, satisfaction, and use of those training materials (“strongly satisfied” to “strongly dissatisfied”), requests for support from the patient navigator, and information seeking requests (overall and by site). Goal setting was captured with the number of goals identified among enrolled families and the status of those goals over time (e.g., completed, in progress). This information was captured overall and on site. Lastly, referral and connection to services was defined as the number of referrals made and type of services requested (overall and by site).
Participant characteristics included demographic information such as age, gender, marital status, and income. Status of substance use (in the past or present) was queried as was information about the type of substance. Caregiver type (biological mother, father, grandparent) was also reported.
Interest in the program and services received over time was captured based on number of individuals enrolled into the program, number of families who became inactive or changed status of enrollment over time, and length of stay in the program (overall and by site).
Impact of the program services was measured using a series of caregiver and infant outcomes including depression (measured by Edinburgh Depression Scale 16 and Patient Health Questionnaire (PHQ 17 )), family violence exposure (measured by the Risk Assessment Tool (RAT 18 ) and HiTS 19 ), child development (measured by Ages & Stages Scale 20 ), childhood trauma (measured by Adverse Childhood Experiences (ACE) 21 and ACE Questionnaire (ACEQ 22 )), substance use (measured by Screening, Brief Intervention, and Referral to Treatment 23 ), tobacco use (measured by Smoking Cessation and Reduction in Pregnancy Treatment 24 ), and maternal support system (measured by Life Skills Progression 25 ).
Sample size calculation
We calculated a sample size prior to starting the program using GPower, 26 an alpha of p < 0.05; power of 0.80; and a medium effect size. These criteria suggested that 156 women and infants were needed to have enough power for the intended analyses.
Statistical analyses
Participant characteristics were calculated using descriptive statistics and reports of means, ranges, standard deviations, frequencies, and proportions for the sample and each of the three sites (Table 1). We also used descriptive statistics to describe each program component, the extent to which they were provided to the larger sample of families, and involvement in these components at enrollment and over time. We examined potential differences in these participation reports based on participant demographics, substance use status, and caregiver type using a series of Multiple Analyses of Variance (MANOVA) models or chi-square analyses depending on the nature of the variables used in the model. Lastly, we examined the impact of program components on participant outcomes using length of stay in program as the predictor model and the maternal and infant outcomes as dependent variables in MANOVA models. We used a statistically significant level of p < 0.05 and SPSS version 28.0 27 to conduct the analyses and determine the significance of the results. Authors have followed the STROBE guidelines when preparing this manuscript.
Participant characteristics.

NICU: neonatal intensive care unit; GED: general education development.
Results
Sample characteristics
One hundred eighty-two individuals (102 (56.8%) from birthing hospital; 34 (18.9%) from family reunification site; and 46 (24.7%) from home visiting site) consented to receive services in the IMPACT WV program. Most of the participants were the biological mothers of enrolled infants (139; 74.7%); however, the remaining portion of participants included 12 (6.5%) grandparents, 33 (17.8%) foster parents, and 2 (1.1%) biological fathers.
Across sites, participant characteristics differed (significantly in some areas). Within the home visiting site, participants were closely distributed across educational levels except for college beyond the undergraduate level. Participants with more education were noted at the family reunification (42.9% college enrollment) and birth hospital site (22.8% college enrollment).
In terms of participant circumstances, more participants recruited from the home visiting site reported not having a place to live (6.5%), whereas 2.9% of those from the family reunification and 1.0% from the birthing hospital reported that challenge (p < 0.001; ϕ = 0.68). Similarly, close to one-third of the home visiting site participants reported concerns about their utilities being shut off while 2.9% of the family reunification and 6.7% of the birth hospital site participants reported this circumstance (p < 0.001; ϕ = 0.71). Limited transportation was a commonly noted challenge for participants in this study with 34.8% of participants from the home visiting site, 11.4% of participants from the family reunification site, and 21.9% of participants from the birth hospital reporting this need (p < 0.01; ϕ = 0.56). Lastly, mothers enrolled in this program varied in terms of their current substance use. Forty-one percent of mothers recruited from the home visiting site had stopped using substances at enrollment. This was significantly higher than 14.3% of mothers recruited from the family reunification site (p < 0.01; ϕ = 0.53) but not significantly different from the 44.8% of mothers recruited from the birthing hospitals who had stopped using substances at enrollment.
Half or slightly more than half of the children recruited to the program were male (home visiting—52.2%; family reunification—48.6%; birth hospital—49.5%). Sites did differ significantly in terms of infants who spent time in the neonatal intensive care unit (NICU). No children in the home visiting site had been in the NICU compared to 2.9% of children recruited from the family reunification and 20.0% of children recruited from the birth hospital (p < 0.001; ϕ = 0.62).
Participation in program components
Women and families enrolled to received services received services focused on direct aid, goal setting, training and TA, and service coordination, assessment, and referral.
Commonly used direct aid funding
Patient navigators provided direct aid to families who identified emergent needs (e.g., basic needs such as diapers, formula, clothing; repair tires for transportation solutions; dental care; medical care). Direct aid could be used for infant and caregiver needs up to $250/family. Prior to designating direct aid, patient navigators would work with families to identify sustainable funding options (e.g., state waiver support, insurance, local non-profit efforts). Table 2 includes the total amount of direct aid used across the program and by each site. More than 22,000 dollars were delivered to clients for basic needs during the program period. Direct aid distribution was comparable between the reunification and home visiting sites but significantly lower in the birth hospital site (p < 0.001; η2 = 0.64 (0.19–0.72)).
Program component offerings over course of program delivery period.

Goal setting
Patient navigators met with women and their families monthly if not more frequently based on their level of interest, need for services, and other supports. During those visits, one of the activities conducted was to identify current goals designed to be steps completed to meet a noted need in services, care, or training. Table 2 displays the number of goals identified at any time for a woman and her family during the period of the program. Overall, 197 goals were documented for all enrolled participants. These goals were evenly distributed in frequency across the program sites. When we examined the status of those goals, however, we found differences by site and status. Specifically, we noted more goals were documented among mothers and families who were supported by a patient navigator within the reunification program than their peers who were supported by a patient navigator from the birthing hospital (p < .001; ϕ = 0.81) or home visiting site (p < 0.02; ϕ = 0.47). In review of all goals by status, we found that most of the documented goals were in progress (114; 57.9%) and that more goals in progress were documented by the patient navigator in the home visiting than the remaining sites (p < 0.01; ϕ = 0.55). A small portion of the goals documented within the program had not been started (32; 16.3%). Most of these goals were documented by the patient navigator at the birthing hospital and significant differed in frequency from the other two sites (p < 0.001; ϕ = 0.71). It should be noted that a single participant in the program could have more than one goal documented while another participant may not have set a goal. The numbers reflected here are cumulative at the site and program levels.
Documented goals for women and their families included 112 entries throughout the program period. Goal plans discussed adoption (n = 20), employment (n = 10), education (n = 18), treatment/recovery (n = 8), food insecurity (n = 1), childcare (n = 2), transportation (n = 13), housing (n = 14), reunification (n = 12), child development (n = 7), child protective services (n = 2), finances (n = 1), parenting skills or family planning (n = 2), legal (n = 1), and domestic violence (n = 1).
Types of needs identified that required referrals
In the process of coordinating service needs for women and their families, patient navigators linked them to additional services they needed but did not already have a connection to. These services were two-generational in nature meaning they could pertain to the caregiver and/or mother’s needs or the infant’s needs. Two hundred eight referrals were made over the program period. Referrals and other linkages did not differ in frequency across sites. Referrals were made for child development, food insecurities, interpersonal violence, utilities, transportation, education and employment, housing, health, clothing, finance, and other. Referral programs included home visiting, treatment, education and employment, women, infants, and children, birth to three, recovery support, counseling, primary care physicians, the Center for Excellence in Disabilities, car seat safety, dental, state department of health and human resources services, day care, legal aid, and basic needs organizations.
Training and TA
Caregivers, family members, and service providers had access to various training opportunities and TA during the program period. Trainings included an on-line, self-paced training portal with individual topic modules designed separately for audiences, 1-h topic presentations (Lunch and Learns), Community of Practice (CoP) presentations and summaries, and in-person trainings varying in length by audience. Training topics were identified not only by the program team but also by families (22 session topics) and providers (69 session topics). In total, 52 training sessions were available to program stakeholders; 4015 individuals attended these sessions. Participant knowledge, which was measured based on baseline and post-training quiz scores significantly increased following trainings (p < 0.01; d = 0.46 (0.21–0.69)). More than half of the total training participants (2,714; 67.6%) provided their level of satisfaction with one or more training courses. Most respondents were “strongly satisfied” with the training (57.6%); 39.7% were “satisfied,” 2.1% were “dissatisfied,” and 0.7% were “strongly dissatisfied.”
Patient navigators provided TA to 153 individuals and/or families throughout the program. TA reports did not differ by demonstration site within the program or by any individual demographic variables. TA was provided to the IMPACT Team and Patient Navigators, students, providers, stakeholders, community members, and families. Resources and information about substance use were provided along with data collection support and learning Portal assistance. Focus groups, needs assessments, and training discussions compiled TA requests from family, provider, and other stake holders. As a result, 22 topics were identified by families, and the topics were addressed with 18 TA responses; 17 topics were identified by providers plus 16 from the provider survey to total 33, and the topics were addressed with 63 TA responses; and 82 topics were identified by stakeholders, and the topics were addressed with 68 TA responses. TA responses included sharing and developing resources and training (modules, webinars).
Program interest and services over time
The enrollment and retention patterns across sites varied greatly for this program. The patient navigator within the birthing hospital enrolled more women and families than other patient navigators (p < 0.001; η2 = 0.25 (0.03–0.41)), but the patient navigator within the home visiting site had fewer families become inactive over time (p < 0.001; η2 = 0.46 (0.22–0.64)). The patient navigator from the reunification site did not lose anyone to follow up compared to other navigators (p < 0.01; ϕ = 0.58). More women and families enrolled from the birthing hospital left the program over time reporting that their needs had been resolved, and they had no outstanding service coordination needs (p < 0.001; ϕ = 0.78) and more women and families from the birthing hospital withdrew from the program over time for other reasons (p < 0.02; ϕ = 0.52). Overall, women and their families remained in the program for an average of 656 days. Women and families enrolled from the reunification program stayed in the program longer (804 days) than their peers in other sites (p < 0.01; see Table 3 for standard deviation across sites).
Program enrollment and status overtime.
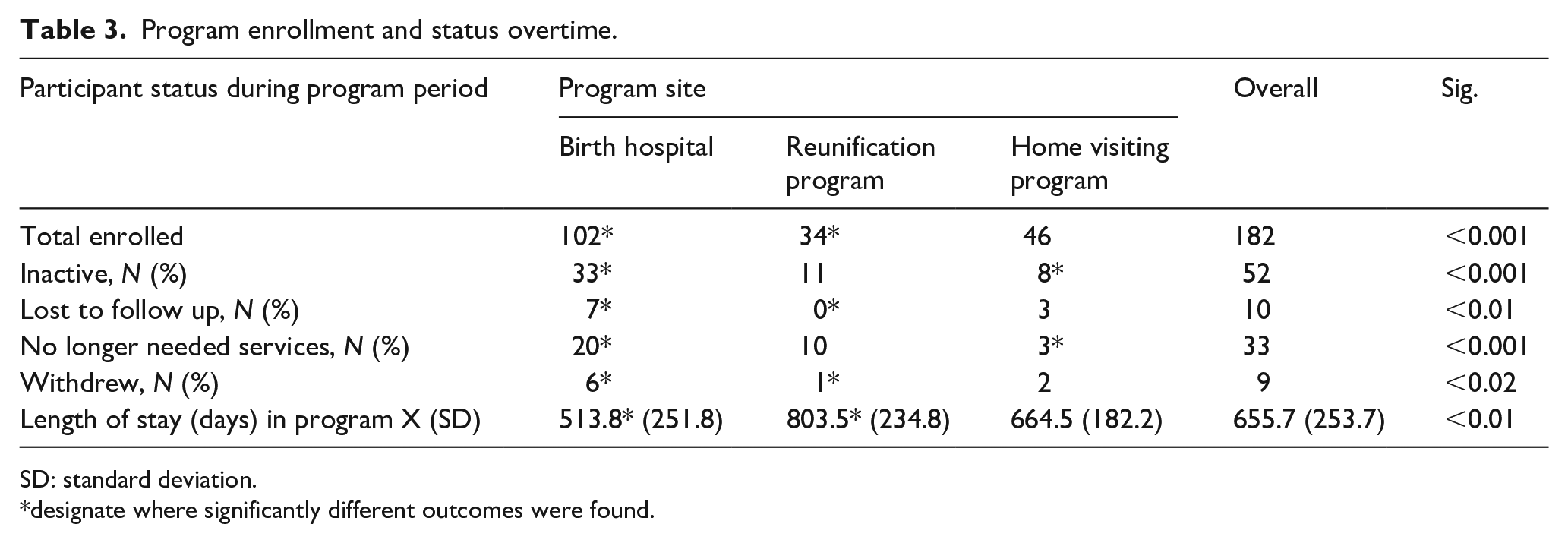
SD: standard deviation.
designate where significantly different outcomes were found.
Women and children completed measures of health outcomes while enrolled in the study. Table 4 delineates comparisons between a participant’s initial and last assessment score on various outcomes. Significant differences were specifically noted between baseline and last infant development (p < 0.02). Maternal and/or primary caregiver report of interpersonal violence also significantly decreased between those two intervals (p < 0.001) on the RAT measure as well as the HiTS measure (p < 0.001). Other comparisons of maternal depression, substance use, and well-being did not significantly differ between these two assessment points.
Maternal and child outcome differences from baseline to final assessment for total sample.

RAT: Relationship Assessment Tool; SD: standard deviation.
We also noticed significant differences when comparing the means and distributions of the most recent assessments across demonstration sites in the program network (Table 5). Maternal depression means (on Edinburgh but not PHQ) were significantly higher within the home visiting program compared to both the birth hospital and reunification program sites (p < 0.05). Similarly, recent caregiver reports of interpersonal violence (measured by RAT but not HiTS) was significantly higher among the birthing hospital site and the reunification site (p < 0.01). No other significant differences were noted by site across the health outcome measures.
Participant health outcomes at program closure by site.

PHQ: Patient Health Questionnaire; SD: standard deviation; SBIRT: Screening, Brief Intervention, and Referral to Treatment; ASQ: Ages & Stages Questionnaires.
We attempted to identify potential caregiver and infant outcomes that were associated with the most recent maternal and infant health outcome reports but found no significant main effects for characteristics such as caregiver education, relationship to the infant, caregiver marital status, infant gender, parent’s substance use history, infant NICU care, and insurance level.
Discussion
The IMPACT WV Program represents a pioneering effort to address the complex needs of women who are, or have used substances and have infants, within a coordinated and community-based framework in the rural setting. Our investigation documented that services for women and their infants can be simultaneously assessed, delivered, and coordinated by a patient navigator in the rural setting. Our findings also demonstrate that in select areas, the coordination and navigation services can improve women’s experiences (e.g., violence; depression) and infant development. In 2020, the National Institute of Health emphasized the importance of streamlined and efficient coordination in improving health outcomes. 28 Researchers have also supported this notion, highlighting the positive impact of coordinated services on infant development and family well-being.29 –31
In this program, women remained enrolled in the program for 21 months, on average. Despite being considered a vulnerable population given the limited services available to them, 3 sites were able to enroll 182 families for services, which was about 70% of those who were eligible at these sites. Those enrolled in the program differed in their family structures and needs. Researchers have highlighted the challenges associated with recruiting and serving this population, noting the need for a consistent support infrastructure for families and accessible materials clearly outlining stigma-free services.32,33 We incorporated these recruitment materials in our own effort for this program but also enhanced how the information was shared and available throughout rural communities. More work is needed to identify which outreach elements of these materials are most impactful to women and families who are seeking services.
We found interesting differences by enrollment site within the program that should be discussed. First, families receiving services slightly differed by site. The finding that 41% of caregivers recruited from the home visiting site had stopped using substances at enrollment aligns with research by Smith et al., 29 which reported similar rates of substance cessation among pregnant women participating in home-based programs. However, other studies such as Roy-García et al. 30 found contrasting results, indicating that substance use cessation rates were significantly higher among mothers recruited from birthing hospitals compared to home visiting programs. Family involvement and length in the study also differed by site. Notably, a more sustained connection between family and patient navigator was observed in the reunification and home visiting sites. This finding resonates with research, which emphasizes the importance of ongoing engagement and relationship-building within community-based programs.
The IMPACT WV program provided unique service coordination through a patient navigator-client model. We found this model to be easily implemented within the rural setting. Families and providers strongly supported the combined patient navigator and two generational model, which was associated with improved infant development and family violence. Our findings contribute to the growing evidence for the patient navigator model, which has been associated with improved morbidity and mortality across different conditions.34 –37 However, Rodríguez et al. have challenged this model, suggesting that its effectiveness may vary based on contextual factors, necessitating ongoing evaluation and adaptation. 38
Direct aid was a commonly used element of this program providing relief to circumstances that made it difficult for the caregiver to consider other services within the program. Goal setting was another important element that contributed to the length of time within the program. The goal-setting component aligns with evidence from Brown et al., 39 who emphasized the effectiveness of patient navigators in helping families set and achieve personalized goals. Other studies have suggested that goal setting alone may not address systemic barriers faced by vulnerable populations, necessitating our broader focus on social determinants of health.40,41
Lastly, trainings, which were available on an on-line portal and desired particularly at a time during the COVID epidemic, but also post-COVID offered opportunities to connect and learn. Providers were highly satisfied with the patient navigator component within IMPACT WV. Sites involved in the study sustained these positions within their agencies to continue to provide these services after experiencing their potential impact on families. The diverse training opportunities provided resonate with findings from Williams et al., 42 who emphasized the value of accessible and varied training formats. These findings have been supported by other groups demonstrating that a combination of online modules, presentations, and in-person sessions significantly enhanced participant knowledge. However, additional research has demonstrated that the ongoing TA provided over time to families is crucial for maintaining knowledge gains over time.43–44
Limitations
When conducting longitudinal studies in rural settings involving women with young infants who use substances, several limitations should be considered. First, the sample size and representativeness of rural populations can pose challenges, impacting statistical power and generalizability. Second, attrition rates due to barriers like transportation or competing priorities may affect data validity. Third, limited access to services and resources in rural areas can influence participant engagement and outcomes. Fourth, stigma and social desirability bias may lead to underreporting of substance use. Fifth, contextual factors unique to rural contexts must be accounted for. Lastly, addressing measurement challenges, such as accurate assessment of substance use, is crucial. By acknowledging these limitations, researchers can enhance the rigor and relevance of their studies.
Conclusion
Our analyses shed light on the program’s potential to transform the lives of vulnerable families, while also highlighting areas for further refinement and expansion. Future studies aimed at enhancing service coordination for women in rural areas who have used or are currently using substances and have young children should focus on several critical areas. First, research should explore innovative models that integrate maternity care, substance use treatment, and social services. Such models need rigorous evaluation to assess their impact on child welfare, maternal health, and overall family well-being. Second, clinical-community care coordination should be a priority. This involves strengthening communication and collaboration between healthcare providers, social workers, and community organizations. By bridging gaps and ensuring seamless transitions, families can receive comprehensive support. Third, a shift in focus toward the parent–child relationship is essential.
Recognizing the critical role of this bond, interventions should prioritize strategies that strengthen parenting skills, enhance attachment, and promote resilience in both mothers and children. Lastly, trauma-informed systems are crucial. Substance use often coexists with trauma, and rural women face unique stressors. Implementing trauma-informed practices across healthcare, social services, and child welfare can improve outcomes for families affected by substance use. Additional attention to subsequent affects for future pregnancies and infants born into a home that has received these services should be given in future studies. By examining the interplay of service components, participant experiences, and health outcomes, we aim to contribute to the ongoing dialog surrounding substance use prevention, maternal–infant health, and holistic support systems.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057241278858 – Supplemental material for Rural service coordination programming for women using substances and their families
Supplemental material, sj-pdf-1-whe-10.1177_17455057241278858 for Rural service coordination programming for women using substances and their families by Lesley Cottrell, Charlotte Workman, Melina Danko, Ellis Walker, Anthony Dmytrijuk, Susan Harrison, Mikisha Lee, Ashleigh McKinsey and Mark C Smith in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.