
Abstract
Objectives:
The aim of this study was to describe the psychological impact of the COVID-19 pandemic and the specific impact of a universal SARS-CoV-2 testing programme on obstetric patients and healthcare workers at The Ottawa Hospital.
Methods:
This was a follow-up survey study of obstetric healthcare workers and then-pregnant patients who participated in a SARS-CoV-2 testing programme conducted in The Ottawa Hospital obstetrical triage units from 19 October to 17 November 2020. Surveys explored the effects of the COVID-19 pandemic and the testing programme on participants’ psychological well-being. Responses were collected from April to September 2021. Descriptive summary statistics were calculated for both groups.
Results:
During hospitalization for delivery, obstetric patients (n = 143) worried about giving COVID-19 to their new baby (88.11%), catching COVID-19 (83.22%), and giving COVID-19 to their partner (76.22%). Patients felt relief at being tested for COVID-19 during the universal testing programme (24.65%) and at getting their results (28.87%). Patients also believed that universal SARS-CoV-2 testing was a good way to slow COVID-19 spread (79.72%), reduce anxiety (75.52%), and increase relief (76.22%). In addition, patients felt good about participating in research that could help others (91.61%). Among obstetric healthcare workers (n = 94), job satisfaction decreased and job stress increased during the COVID-19 pandemic. The universal testing programme led to minor increases in healthcare worker job stress and burden, particularly among nurses, but the majority (85.23%) believed it was a valuable research initiative.
Conclusion:
The COVID-19 pandemic has had a negative psychological impact on obstetric patients and healthcare workers. Universal SARS-CoV-2 testing was generally viewed favourably and may serve as an effective strategy for estimating COVID-19 prevalence without adding undue stress onto patients and healthcare workers during the pandemic.
Introduction
The novel coronavirus disease 2019 (COVID-19) pandemic has led to an international mental health crisis, with a widespread increase in anxiety and depression reported in the general population since the beginning of the pandemic.1,2
Pregnant individuals are uniquely vulnerable to psychological distress,3,4 and this has been exacerbated by the COVID-19 pandemic.5–7 In Canada, 37% and 57% of pregnant individuals reported symptoms of depression and anxiety, respectively, 8 compared to pre-pandemic levels of 9%–11% depression 9 and 18%–25% anxiety. 10 Canadians pregnant during the COVID-19 pandemic are also more likely to report other psychiatric symptoms 11 and seek medical attention for psychiatric illness 12 than before the pandemic. Maternal anxiety and depression can lead to many adverse maternal and foetal outcomes, including preterm labour, gestational diabetes, foetal and postnatal growth restriction, and future psychiatric and emotional problems in childhood.5,13–15 Maternal stress can also lead to future psychiatric illness in offspring.16,17
The COVID-19 pandemic has also had a negative psychological effect on healthcare workers (HCWs), leading to higher levels of anxiety, depression, and insomnia 18 than pre-pandemic. A recent study found that 75% of Canadian HCWs scored above the threshold for possible depression on the Patient Health Questionnaire-9 (PHQ-9) and 10% reported recent suicidal ideation. 19 Nurses in Canada have been the most affected by the pandemic, with elevated psychological distress and emotional exhaustion compared to other HCWs. 20 Anxiety, depression, post-traumatic stress disorder (PTSD), and stress have also increased among Canadian nurses since the start of the pandemic.21,22 Increased workload is a strong contributor to emotional exhaustion, 23 burnout, 24 and occupational stress 25 of HCWs during the pandemic, and job dissatisfaction is linked to burnout, anxiety, and depression.23,24
In order to help reduce transmission between HCWs and patients, several hospitals in Canada, the United States,26–29 and internationally30–32 introduced universal SARS-CoV-2 testing programmes for all pregnant individuals admitted for delivery. A study of obstetric patients and HCWs in Philadelphia, PA, found that implementing a universal COVID-19 testing programme decreased anxiety in both populations and increased job satisfaction of labour and delivery HCWs. 33 A similar study in Japan reported increased relief among obstetric patients from being tested but increased worry about the implications of positive results. 34 Midwives and nurses believed that such a programme would be valuable and would reduce anxiety; however, some obstetricians worried that asymptomatic positive patients might be subjected to non-essential medical interventions. 34
Due to the novelty of SARS-CoV-2, there has been a surge of research conducted during the pandemic, and the impact this has on participants and hospital staff has not been well explored. In addition, no studies to date have looked at the impact of universal SARS-CoV-2 testing on the job burden of obstetric HCWs, and none have offered a complete picture of the impact of such a programme on HCWs and patients. The aim of this study was to assess the psychological impact of the COVID-19 pandemic and a universal SARS-CoV-2 testing programme on obstetric patients and HCWs.
Methods
Study design
This was a follow-up survey study involving pregnant individuals and obstetric HCWs at The Ottawa Hospital (TOH). In fall 2020, all consenting pregnant individuals who presented to an obstetrical triage unit at TOH Civic and General Campuses were tested for SARS-CoV-2 and anti-SARS-CoV-2 antibodies as part of the ‘UNIVERSE-OB’ universal testing programme. The goal of the UNIVERSE-OB programme was to determine rates of COVID-19 infection in the TOH obstetrical patient population. Analysis and collection of samples occurred over a 1-month period, from 19 October to 27 November 2020, when Ottawa was in the second wave of the COVID-19 pandemic.
This study assessed the psychological impacts of the COVID-19 pandemic and the UNIVERSE-OB testing programme on UNIVERSE-OB participants and obstetric HCWs at TOH. All individuals who participated in the UNIVERSE-OB study and all staff from the Department of Obstetrics, Gynaecology and Newborn Care at TOH Civic and General campuses were eligible to participate. Study methods are reported using the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) 35 (Supplemental Appendix 1).
Ethics approval and consent to participate
Ethics approval for this study was attained from the Ottawa Health Science Network Research Ethics Board (20200640-01H). Informed consent was obtained based on an implied consent model, with survey submission indicating participant consent.
Study questionnaires and measures
Separate surveys were administered to obstetric patients and HCWs to evaluate the impact of the COVID-19 pandemic and the UNIVERSE-OB testing programme on these groups (Supplemental Appendix 2). Patients were asked about the impact of the COVID-19 pandemic and testing programme on their birthing experience and lives in general. HCWs were surveyed about the impact of the pandemic and testing programme on their day-to-day activities and workload.
The patient questionnaire developed by the study team assessed COVID-19 coping mechanisms, demographic information, and questions about COVID-19 and the UNIVERSE-OB testing programme. Anxiety was assessed using the Generalized Anxiety Disorder-7 (GAD-7) 36 and depression was assessed using the Patient Health Questionnaire-4 (PHQ-4), 37 both validated screening tools. Clinically significant anxiety was defined as a score of ⩾10 on the GAD-7 or ⩾3 on the PHQ-4 anxiety subscale, clinically significant depression was defined as a score of ⩾3 on the PHQ-4 depression subscale, and clinically significant psychological distress was defined as a score of ⩾6 on the PHQ-4. The GAD-7 and PHQ-4 questions were integrated with the patient questionnaire.
The HCW questionnaire developed by the study team assessed job satisfaction, job stress, job burden, COVID-19 coping mechanisms, demographic information, and feelings about the UNIVERSE-OB testing programme. Both online questionnaires consisted largely of multiple-choice questions with some opportunities for open-ended comments.
Recruitment
Patients were contacted by telephone between 13 May and 13 July 2021, where they provided consent to be sent the survey link via email and were also provided with their SARS-CoV-2 virus and antibody test results from the initial UNIVERSE-OB study. The HCW questionnaire was sent to the TOH emails of all HCWs in the Department of Obstetrics, Gynaecology, and Newborn Care.
Survey administration
Surveys were Web-based and hosted on LimeSurvey (Version 2.59.1+170116). 38 Responses were collected through LimeSurvey and stored on secure institutional servers. Survey completion was voluntary. Patient responses were collected between 13 May and 17 September 2021, from the peak of the third wave to the beginning of the fourth wave of the COVID-19 pandemic in Ottawa. HCW responses were collected between 6 May and 22 July 2021, during the third wave of the pandemic. HCWs were incentivised for their participation with a CAD$5 coffee gift card upon completion of the survey.
Analysis
Only submitted surveys were included in the analysis. Survey data were summarized descriptively, using frequencies and percentages to demonstrate the distributions of responses both overall and separated by patient and HCW groups where appropriate. All descriptive analyses were performed using SAS v9.4 (SAS Institute, Cary, NC, USA).
Results
Response rates
Out of 395 patient participants in the UNIVERSE-OB universal SARS-CoV-2 testing programme, 297 were reached by telephone and 273 agreed to be sent the survey link. Of the 273 patients sent the patient questionnaire, 173 commenced the survey, giving a participation rate of 63.37%. Of the 173 patients who commenced the patient questionnaire, 143 completed it, yielding a completion rate of 82.66% (Figure 1).

Population flowchart for patient cohort.
Participation rate could not be calculated for the HCW questionnaire due to not knowing how many HCWs were reached by the mass email. For the same reason, a population flowchart was not created for this group. A total of 103 HCWs started the HCW questionnaire and 94 completed it, yielding a completion rate of 91.26%.
Participant characteristics
The majority of pregnant individuals in our study were between the ages of 30 and 39 (n = 109, 76.22%) and had completed a bachelor’s degree (n = 58, 40.56%) or university education above the bachelor’s level (n = 43, 30.07%) (Table 1). There were 134 (93.71%) who were married or common law and 71 (49.65%) reported a household income above CAD$120,000. The majority of patients were White (n = 97, 67.13%), but there was representation from many Other races and ethnicities. Most pregnant individuals in this study identified as a woman.
Sociodemographic information of obstetric patient and healthcare worker study participants.

Values < 6 were suppressed due to small cell size.
Public colleges in the province of Quebec that are typically required for Quebec university admission.
Initial study refers to the UNIVERSE-OB universal COVID-19 testing study.
Grey boxes indicate questions that were not asked to that group.
HCW ages were evenly distributed across the 18–64 years categories, and the majority had completed a bachelor’s degree (n = 41, 44.57%) or university education above the bachelor’s level (n = 34, 36.96%). There were 65 (69.89%) who were married or common law and the majority lived with others at home, with spouse (n = 63, 67.02%) and child(ren) (n = 50, 53.19%) the most common options. The majority were White (n = 72, 76.60%) and had a household income above CAD$120,000 (n = 47, 51.09%). Nurses represented 61.96% of HCWs (n = 57) and 29.35% (n = 27) were physicians. Detailed demographic information can be found in Table 1.
Impact of the COVID-19 pandemic on participants
Patients reported experiencing COVID-19-related worries during hospitalization for labour and delivery, most commonly about giving COVID-19 to their new baby (n = 126, 88.11%), catching COVID-19 (n = 119, 83.22%), and giving COVID-19 to their partner (n = 109, 76.22%) (Figure 2). Some patients also reported that anxiety about COVID-19 affected their ability to care for their new baby (n = 29, 20.28%) and/or recover from labour and delivery (n = 43, 30.07%). When comparing previous birthing experiences to their birthing experience during the COVID-19 pandemic, multiparous individuals (n = 61) reported more worry and anxiety (n = 50, 81.97%) and loneliness and isolation (n = 43, 70.49%) during their COVID-19 delivery.

Common worries among obstetric patients (n = 143) hospitalized for delivery during the COVID-19 pandemic.
At the time of survey completion, 58 patients (40.56%) screened positive for psychological distress on the PHQ-4 validated screening tool, with 20 (13.99%) experiencing clinically significant moderate-to-severe distress (Table 2). A total of 19 (13.29%) screened positive for depression and 25 (17.48%) for anxiety on the PHQ-4 subscales. The PHQ-4 subscales only give a positive or negative screen with no indication of severity. On the GAD-7, 65 (45.45%) screened positive for anxiety, with 21 (14.69%) experiencing clinically significant moderate-to-severe anxiety.
Prevalence of anxiety, depression, and psychological distress in obstetric patients (n = 143) during the COVID-19 pandemic.
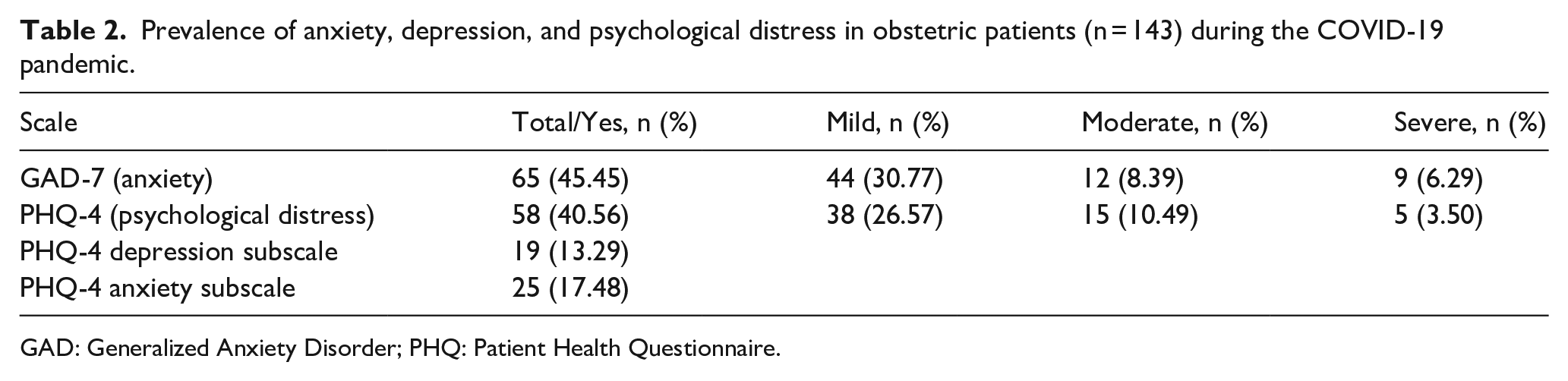
GAD: Generalized Anxiety Disorder; PHQ: Patient Health Questionnaire.
Among HCWs, job satisfaction decreased and job stress increased during the COVID-19 pandemic (Figure 3). Of those who lived with others (n = 88), 80 (90.91%) worried at least a little about transmitting COVID-19 to the members of their household as a result of their job, with 49 (55.68%) worrying moderately to severely.

Job satisfaction (a) and job stress (b) among obstetric healthcare workers at The Ottawa Hospital (n = 94) before and after the start of the COVID-19 pandemic (12 March 2020).
HCWs and patients employed a variety of mechanisms to cope with the COVID-19 pandemic (Table 3). HCWs most commonly coped by increasing the amount they exercised (n = 43, 45.74%) and/or increasing their alcohol consumption (n = 24, 25.53%), and patients most commonly coped by accessing mental health services (n = 46, 32.17%) and/or decreasing their work hours (n = 40, 27.97%).
Common methods of coping with the COVID-19 pandemic among obstetric patients and healthcare workers.

Values <6 were suppressed due to small cell size.
Impact of the UNIVERSE-OB study on participants
Of obstetric HCWs working during the UNIVERSE-OB study (n = 88), the majority reported no impact of the UNIVERSE-OB programme on their job satisfaction (n = 65, 73.86%) or job stress (n = 63, 71.59%) with minimal or no added job burden (n = 64, 72.73%) (Table 4). Increased job stress and burden due to UNIVERSE-OB were reported more frequently among nurses compared to delivery providers (midwives and physicians). The majority of HCWs reported no delays in clinical care related to the UNIVERSE-OB study (n = 76, 86.36%), and most believed it was a valuable research initiative (n = 75, 85.23%).
Impact of the UNIVERSE-OB SARS-CoV-2 testing programme on obstetric healthcare workers stratified by nurses versus delivery providers.
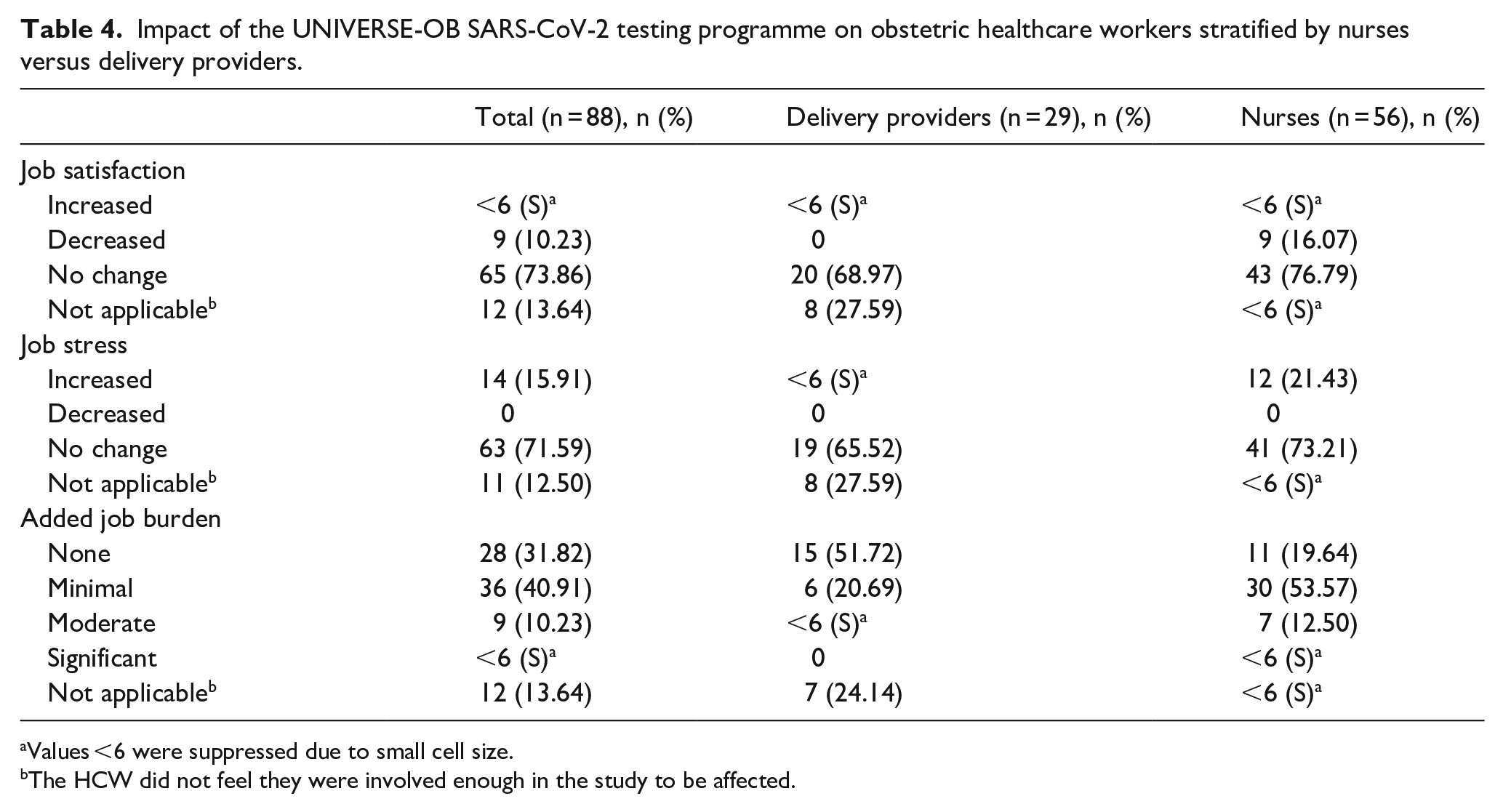
Values <6 were suppressed due to small cell size.
The HCW did not feel they were involved enough in the study to be affected.
Patients’ feedback suggests that they were largely unaffected by participation in the universal testing programme, but a minority reported feelings of relief due to being tested (n = 35, 24.65%) and getting their test results (n = 41, 28.87%). Most patients experienced mild or no worry about the COVID-19 nasopharyngeal test procedure (n = 116, 81.12%). However, most participants reported moderate-to-severe anxiety about the implications of potentially testing positive for COVID-19 (n = 93, 65.03%).
In general, patients believed that universal COVID-19 testing programmes are a good way to slow the spread of COVID-19 (n = 114, 79.72%), reduce anxiety about COVID-19 (n = 108, 75.52%), and increase relief (n = 109, 76.22%). There were 87 patients (60.84%) who believed that everyone who goes to a hospital during COVID-19 should be tested. The majority of patients were either excited (n = 46, 32.17%) or did not mind (n = 88, 61.54%) being approached to participate in COVID-19 research during their pregnancy, and additionally felt good about participating in research that could benefit others (n = 131, 91.61%).
Discussion
The aim of this study was to assess the psychological impact of the COVID-19 pandemic and a universal SARS-CoV-2 testing programme on obstetric patients and HCWs. We found that the COVID-19 pandemic negatively affected the birthing experience of obstetric patients and considerably decreased the job satisfaction and increased the job stress of obstetric HCWs. Participation in the UNIVERSE-OB study did not appear to negatively affect patients, with the majority experiencing benefits from their participation. HCWs reported a minor added job burden due to the study but overall viewed the programme favourably.
Our study sought to fill a gap in the literature around the impact of COVID-19 research on participants and HCWs involved in these studies. This study is the first to investigate the impact of universal SARS-CoV-2 testing on obstetric HCW job burden and to describe the direct impacts of a universal testing programme on nurses versus delivery providers. We also examined patients’ thoughts about universal testing and the effects of testing on multiple patient emotions to obtain a more complete picture of patients’ experiences.
Impact of the COVID-19 pandemic on patients
The COVID-19 pandemic has negatively affected the perinatal experience of individuals giving birth in hospitals, with patients experiencing considerable worry about COVID-19 during hospitalization. Patients in our study experienced the most worry about giving COVID-19 to their new baby, a finding that has been replicated in the literature. 34 Not having their partner present during some or all of their delivery is also very distressing to pregnant individuals.39,40 With some exceptions, most patients in our study were allowed one support person in the delivery room. However, many worried severely about not having additional family present. Many patients have had to choose between having their partner or another support person, such as a doula, with them during their birth. 41 Patients also worried about contracting COVID-19 at the time of delivery and transmitting the virus to other household members, worries that have been widespread among pregnant individuals during the pandemic.34,42,43
Multiparous individuals in our study reported more negative hospital experiences during their COVID-19 delivery compared to previous deliveries, with increased anxiety and loneliness. The COVID-19 pandemic has also contributed to postpartum difficulties in pregnant individuals, including diminished ability to care for their new baby and recover from delivery. These difficulties may be due at least in part to feelings of pandemic-related isolation.33,41
Using validated screening tools, the prevalence of clinically significant anxiety among patients in our study was 14.69% (GAD-7) to 17.48% (PHQ-4 anxiety subscale), clinically significant depression was 13.29%, and clinically significant psychological distress was 13.99%. These values were lower than expected, with previous studies reporting a 37% prevalence of anxiety, 31% prevalence of depression, and 70% prevalence of psychological distress among pregnant individuals during the COVID-19 pandemic. 5 Our values were closer to pre-pandemic levels of 15.2% anxiety 10 and 11.9% depression. 44 This may be due to the majority of published research on perinatal anxiety and depression being conducted during the first wave of the COVID-19 pandemic when uncertainties were higher. This study was conducted after a year of living in the pandemic, and participants have likely adapted. Relatively low community prevalence of SARS-CoV-2 in Ottawa and stringent public health regulations at the time of survey may also have contributed to lower levels of anxiety, depression, and psychological distress in our patient group.
The two most common coping methods used among patients to address the negative impacts of COVID-19 were accessing mental health services (n = 46, 32.17%) and decreasing their work hours due to stress or illness (n = 40, 27.97%). Exercise may have been a less-common coping method as patients would be recovering from delivery and caring for their newborn. Similarly, patients may have decreased work hours due to their pregnancy.
Various strategies have been suggested for reducing anxiety and depression in pregnant individuals during the pandemic. Ensuring adequate access to social support is crucial, including allowing support persons in the delivery room and limiting hospital policies that may cause distress. 45 The World Health Organization recommends that mothers and infants are not separated after birth, even if one or both are infected with SARS-CoV-2. 46 Encouraging physical activity may also be an effective strategy, as exercise has been shown to decrease symptoms of anxiety and depression in pregnant individuals both pre-pandemic 47 and during the pandemic. 8 Ultimately, HCWs should be aware of potential mental health struggles in their patients 45 and offer professional psychological care if warranted. 48
Impact of the COVID-19 pandemic on HCWs
Obstetric HCWs in our study experienced a considerable decline in job satisfaction and increase in job stress since the beginning of the pandemic. It was observed that 43 (46.24%) HCWs were very satisfied with their job pre-pandemic, whereas only 18 (19.35%) were very satisfied during the pandemic. The percentage of HCWs experiencing significant job stress increased from 8.60% (n = 8) pre-pandemic to 63.44% (n = 59) during the pandemic. The decline in job satisfaction and increase in job stress highlights the excessive burden of COVID-19 on HCWs, as they must endure new protocols, increased personal protective equipment (PPE), and overcrowded hospitals. A previous study indicated that 43.6% of resident physicians are experiencing a higher workload due to COVID-19, resulting in 21.7% of those physicians wanting to resign. 49 Stress, worry, anxiety, and fear have increased significantly among many HCWs.22,49,50 Factors contributing to the negative psychological impact of the pandemic on HCWs include resource shortages, organizational unpreparedness, lack of organizational support, and feeling unsafe in the workplace. 21 Nurses and frontline HCWs have been impacted the most severely, with higher depression, anxiety, insomnia, and distress compared to other HCWs. 51
One particularly distressing worry among HCWs in our study was transmitting COVID-19 to household members due to working in the hospital, with 80 (90.91%) worrying at least slightly and 49 (55.68%) experiencing moderate-to-severe worry. This worry has been shared by many HCWs in Canada 21,50 and worldwide. 49
HCWs’ methods of coping with the pandemic included increasing exercise (n = 43, 45.74%) and alcohol consumption (n = 24, 25.53%). They may have been more inclined to increase exercise due to working in a profession that encourages healthy lifestyle behaviours. Conversely, they may have been less likely to seek out mental health services due to the increased stigma surrounding mental health issues in this population and a resulting fear of professional repercussions.52–54 HCWs may also have felt obliged to work the same or even longer hours due to their increased pandemic-related workload, thus with an inability to reduce their work hours they may have instead turned to substances to deal with their increased stress.
Impact of the UNIVERSE-OB study on patients
Most of patients’ emotions, including loneliness and isolation, anger and irritation, sadness, and happiness, did not change due to being tested for SARS-CoV-2 at the hospital or receiving their test result. However, some did experience relief at being tested (n = 35, 24.7%) and receiving their results (n = 41, 28.9%). Similarly, Bender et al. 33 found that 27.6% of pregnant individuals who tested negative for COVID-19 at the hospital were reassured by their negative test result. Much higher figures were reported in a Japanese study, which found that 71.3% of pregnant individuals who were tested for COVID-19, all of whom tested negative, reported that they could now deliver with relief. 34
Pregnant individuals’ most pervasive worry about being tested for COVID-19 at the hospital related to the potential implications of testing positive. In our study, 93 (65.03%) patients worried moderately to severely about this, whereas only 19 (13.29%) did not worry about it at all. Specifically, many commented that they were worried about potential separation from their newborn or partner if they were to test positive. These worries were shared by pregnant individuals in other studies.11,34 Most pregnant individuals in our study experienced mild or no worry about the SARS-CoV-2 testing procedure, thus it appears that the testing process itself did not cause substantial distress.
Our study also examined patients’ thoughts about universal SARS-CoV-2 testing, which to the best of our knowledge has not been previously explored. The majority (n = 108, 75.52%) believed that universal testing could reduce worry and anxiety about COVID-19, but only a minority believed it could reduce other negative emotions such as loneliness and isolation (n = 44, 30.77%), anger and irritation (n = 34, 23.78%), and sadness (n = 31, 21.68%). The majority also believed that universal testing could increase relief (n = 109, 76.22%), but only 47 (32.87%) believed it could increase happiness. These thoughts correlate with patients’ actual emotions after being tested, as described earlier. Thus, it appears that anxiety and relief are the emotions most likely to be affected by universal SARS-CoV-2 testing among patients.
Patients also believed that universal testing is a good way to slow the spread of COVID-19, and the majority (n = 87, 60.84%) believed that everyone who goes to a hospital during COVID-19 should be tested. However, many commented that rapid tests instead of polymerase chain reaction (PCR) would be more effective for this purpose.
Patients experienced multiple benefits from participating in research during the COVID-19 pandemic. Almost all felt good about participating in research that could benefit others, and 40 (27.97%) appreciated being able to ask the research team about COVID-19. Only 10 patients (6.99%) reported no benefits from participating in the UNIVERSE-OB study, and only 6 (4.20%) were unhappy to have been approached to participate.
Impact of the UNIVERSE-OB study on HCWs
Most obstetric HCWs experienced no change in their job satisfaction (73.86%) or job stress (71.59%) due to the UNIVERSE-OB study, with a minority reporting decreased job satisfaction (10.23%) and increased job stress (15.91%). These results differed from Bender et al., 33 who found that universal SARS-CoV-2 testing increased job satisfaction in 61% of obstetric HCWs and reduced job-related anxiety in 66%. This discrepancy is likely due to the use of rapid tests with near-immediate results in Bender et al., which allowed HCWs to know a patient’s COVID-19 status.
There were 36 (40.91%) HCWs who reported a minimal added job burden from the UNIVERSE-OB study, with very few reporting a moderate or significant burden (Table 4). Increases in job burden were more common in nurses than delivery providers, likely due to nurses being more directly involved in sample collection for the study. Nurses are also at a higher risk for many COVID-19-related outcomes than other medical staff, including a higher likelihood of being infected with COVID-19, 55 higher rates of anxiety and depression,56,57 and greater increases in emotional exhaustion. 20
The UNIVERSE-OB study generally did not lead to any delays in clinical care of patients. Despite the minor increases in job burden and stress experienced by some HCWs, almost all (n = 75, 85.23%) believed that the study was a valuable project to conduct during the pandemic, with the remainder unsure of its value (n = 16, 17.20%). Kawamura et al. 34 reported slightly lower values, with 79.1% of midwives and nurses and 54.4% of obstetricians believing that prenatal SARS-CoV-2 testing was useful. Most of those who did not believe testing was useful were concerned that universal testing could lead to unnecessary treatment of asymptomatic patients.
Strengths and implications
The negative effects of the COVID-19 pandemic on pregnant individuals and HCWs have been well-documented, and here we add the experiences of those living in Ottawa, one of the largest cities in Canada. We additionally investigated health behaviour changes in these groups to determine how they were coping with the stresses of the pandemic.
To the best of our knowledge, only two studies have examined the impact of universal SARS-CoV-2 testing programmes on obstetric patients and HCWs.33,34 Bender et al. 33 employed qualitative methods with open-ended questioning for their study, and Kawamura et al. 34 measured the impacts indirectly without implementing their own testing programme. A strength of our study is that we quantitatively examined the impact of a universal SARS-CoV-2 testing programme with some opportunities for open-ended elaboration.
Our study looked specifically at the impact of research involving a universal testing programme, but to a certain extent our results can illustrate the general impact of research on patients and HCWs during the pandemic. From our results, it appears that research can be conducted in hospitals during a pandemic without detrimental effects on participants and HCWs, if they can see value in the study.
Limitations
As the initial UNIVERSE-OB study was designed to estimate SARS-CoV-2 community prevalence and not intended to yield point-of-care test results, patients did not receive their research SARS-CoV-2 virus and antibody results until approximately 7 months after testing. This delay likely limited the psychological impact these results had on participants. Rapid testing with results given to patients immediately could have a greater psychological impact on patients and HCWs, as these results could more directly impact their hospital experiences. For instance, Kawamura et al. 34 reported high levels of relief among obstetric patients who tested negative for COVID-19 pre-delivery. Conversely, Bender et al. 33 found that most obstetric patients were not reassured by negative rapid test results at the time of admission due to worry about becoming infected with COVID-19 while in hospital. The impact of point-of-care test results is thus unclear and warrants further investigation.
When answering questions about the UNIVERSE-OB study, both HCWs and patients could have experienced some recall bias due to a few months elapsing between the initial study and this follow-up survey study. Recall bias can be reduced with shorter recall periods and clearly worded questionnaires, 58 both of which were implemented in our study. Other strategies include the use of memory aids and a backwards recall strategy of starting with questions about the present and continuing backwards in time. 58
We assessed anxiety, depression, and psychological distress in obstetric patients at the time of survey completion, when patients were approximately 6–10 months postpartum. Although many of the stresses of giving birth and caring for a newborn are likely still present, this time delay may make our results less comparable to studies examining COVID-19-related anxiety and depression during pregnancy and the more immediate postpartum period. Depression and anxiety are generally reported to be less-common postpartum than during pregnancy in pre-pandemic studies,4,59 although 64% of pregnant individuals with symptoms of anxiety during pregnancy also experienced postpartum anxiety. 4 A preliminary meta-analysis demonstrated higher antenatal than postnatal depression in pregnant individuals during the pandemic; however, no comparison could be made for anxiety due to insufficient literature. 60 Moreover, most studies in this meta-analysis only examined the immediate postpartum period. 60 Further longitudinal investigation into levels of anxiety and depression throughout pregnancy and the extended postpartum period during the COVID-19 pandemic is thus warranted.
When considering the implementation of universal SARS-CoV-2 testing, it is important to consider the costs involved. As our study was laboratory-based and grant-funded, we cannot comment on the costs of this programme for clinical application. However, the literature has shown that universal SARS-CoV-2 testing programmes are often cost-effective,61–65 especially when conducted in high-risk groups 65 or areas with high community prevalence.61,62
Conclusion
The COVID-19 pandemic has had a negative psychological impact on pregnant individuals and HCWs, and strategies to improve patient perinatal experience and reduce the extra burden of the pandemic on HCWs are needed without delay. Although universal SARS-CoV-2 testing of obstetric patients added a minor job burden to HCWs, it was largely viewed favourably by patients and HCWs. Thus, it appears that research can be conducted during a pandemic without adding undue stress onto participants and staff.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221103101 – Supplemental material for The psychological impact of the COVID-19 pandemic and a SARS-CoV-2 testing programme on obstetric patients and healthcare workers
Supplemental material, sj-docx-1-whe-10.1177_17455057221103101 for The psychological impact of the COVID-19 pandemic and a SARS-CoV-2 testing programme on obstetric patients and healthcare workers by Abigail M Ross, Serine Ramlawi, Romina Fakhraei, Malia SQ Murphy, Robin Ducharme, Alysha LJ Dingwall-Harvey, Ruth Rennicks White, Kerri Ritchie, Katherine Muldoon and Darine El-Chaâr in Women’s Health
Footnotes
Acknowledgements
The authors acknowledge Julia Dobrowolski, Rosemary Larose, and Elisabet White for patient phone calls; Kathryn Denize for supporting the study; Dana Burke for administrative support; Chantal Menard, Lisa Galitzine, and Paula Archambault for nursing leadership support; and all of the patients and providers who took the time to fill out our surveys.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Canadian Institutes of Health Research Foundation Grant (Funding Reference Number: VR4-172760).
Guarantor
Darine El-Chaâr
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.