
Abstract
Background:
The maternal mortality rate in poor nations remains unacceptably high. The purpose of this study was to identify factors associated with institutional delivery usage.
Methods:
The data came from the Ethiopian mini demographic and health survey, which was conducted in 2019. This study comprised 3978 women of reproductive age who had given birth within the previous 5 years. To uncover significantly linked parameters associated with institutional delivery, we used a multilevel logistic regression model. Statistical significance was declared at p < 0.05, and we assessed the strength of association using adjusted odds ratios with 95% confidence intervals.
Results:
More than half of the women (53.67%) among 3978 women with last birth had their babies delivered in a health facility. In the multilevel logistic regression analysis, women in age group 45–49 (AOR = 2.43, 95% CI: 1.280, 4.591), primary educational level (AOR = 2.21, 95% CI: 1.864, 2.625, secondary and above education level (AOR = 6.37, 95% CI: 4.600, 8.837), being Muslim (AOR = 2.57, 95% CI: 1.245, 2.166), women who visited ANC service four up to seven times (AOR = 2.75, 95% CI: 2.175, 3.473), women visited ANC service eight times and above (AOR = 3.295% CI: 1.685, 6.050), women who reside in middle wealth index (AOR = 1.57, 95% CI: 1.273, 1.950), and rich wealth index (AOR = 3.43, 95% CI: 2.782, 4.225) were more likely to give birth at health institution compared to their counterparts. Furthermore, women being in rural area (AOR = 0.34, 95% CI:- 0.283, 0.474) and protestant women (AOR = 0.1.57, 95% CI: 0.479, 0.852) were less likely to deliver at health institution.
Conclusions:
Ethiopia still has a low level of institutionalized delivery. Institutional delivery in Ethiopia should be improved through context-specific and personalized programs, such as educating women and enhancing access to ANC services.
Introduction
Childbirth is a complicated procedure, and it’s important to remember to supply all that’s required to keep both the mother and the newborn kid safe.1,2 Even though the maternal mortality ratio has decreased from 1990 to 2015, the rate of maternal mortality in poor nations, which account for 99% of worldwide maternal deaths, remains unacceptably high. 3 According to the United Nations International Children’s Emergency Fund (UNICEF), every day 800 mothers and 2700 babies die as a result of complications during pregnancy and childbirth, according to UNICEF data from 2015. 4 In 2015, the MMR in underdeveloped nations was 239 pregnant women per 100,000 live births, compared to 12 in industrialized countries. The number of women giving birth was high at the end of 2015, and over 303,000 women died during pregnancy, with almost all deaths occurring in low-resource areas and the majority being preventable. 5 The majority of maternal deaths occur within 42 days of delivery, with the moment of delivery being the most critical. 6
In Sub-Saharan Africa and South Asia, maternal mortality has been high. With a Maternal Death Ratio (MMR) of 500 per 100,000 live births, Sub-Saharan Africa alone accounts for 56% of maternal death. 7 In Sub-Saharan Africa, Ethiopia is among the developing countries with the highest maternal death rate. 8 According to a 2010 report by the World Health Organization (WHO), the country saw nearly 9000 maternal deaths. 9 According to the four consecutive Ethiopian Demographic and Health Survey (EDHS), MMR was 871 per 100,000 live births in 2000, 673 per 100,000 live births in 2005, 676 per 100,000 live births in 2011, and 412 per 100,000 live births in 2016.7,8,10,11 Ethiopia has devised several initiatives to reduce maternal and child mortality by supporting institutional delivery systems, as maternal mortality remains unacceptably high in poor countries. Only one-fourth of women in the country gave birth in a health facility. 12
Institutional delivery is a critical intervention in reducing maternal and newborn mortality. By assuring extensive medical care and aseptic settings during delivery, institutional delivery reduces the risk of complications and infections. 13 Complications and deaths connected to delivery can be avoided primarily through institutional delivery with the assistance of experienced physicians and strong referrals. 14 – 16 Because maternal problems during delivery can result in infant death, having access to high-quality institutional delivery care improves neonatal health outcomes. 17 As a result, improving access to delivery care is critical for reducing maternal and newborn mortality. Between 2014 and 2019, it is anticipated that about 81% of all deliveries took place in the presence of competent birth attendants, compared to 60% from 2000 to 2006. 4
Despite their efforts, there is a gap in the use of institutionalized delivery services by women from various socioeconomic backgrounds. 10 Women from higher wealth quintiles use health services more frequently than women from lower wealth quintiles, according to studies conducted in Ethiopia and Burkina Faso.18,19 According to a study, women in a metropolitan area with a primary and secondary/higher education were 2.2 and 3.3 times more likely to give birth at a health institution than those with no education. 20 Furthermore, a descriptive analysis of the 2016 EDHS revealed that institutional delivery use varied by region, place of residence, wealth index, and women’s educational level. 10 However, by combining the hierarchical structure of EMDHS data in the population, more research on characteristics associated with institutional delivery in Ethiopia is needed. To reduce maternal mortality in Ethiopia, addressing regional differences in access to maternal health care services should be a top focus. Furthermore, using some advanced statistical methods, the target groups for specific interventions should be selected. Using a multilevel binary logistic regression analysis, this study attempted to see whether there are regional variations or not in the utilization of institutional delivery and to discover the factors linked with the utilization of institutional delivery care in Ethiopia.
Methods and materials
The source data set and study design
The data for this study came from the 2019 EMDHS, a cross-sectional survey that took place between March 21 and June 28, 2019. The EMDHS was created to give estimates of health and demographics in nine geographical regions and two administrative cities.
Sample size determination and sampling methods
The EMDHS 2019 followed a complex sampling design (i.e. combined stratified and cluster in two stages, with unequal probabilities of selection that result in the weighted sample to separate the sample components) and was designed to obtain representative estimates at the national, and regional levels (administratively, the country is divided into 9 geographical regions and 2 administrative cities).
Among 8885 child-bearing mothers interviewed, only 3978 mothers who had given birth within the 5 years preceding the survey were considered to identify factors associated with the utilization of institutional delivery in Ethiopia.
The whole report of the EMDHS 2019, which was the second inclusive survey and was implemented by the Ethiopian Public Health Institute (EPHI), includes detailed information on data management. The results are available online in the DHS database at https://www.dhsprogram.com/data/datasetadmin/loginmain.cfm.
Inclusion and exclusion criteria
Being an Ethiopian national between the ages of 15 and 49, having given birth in the year preceding the interview, and living in Ethiopia during the pregnancy were the only requirements. Mothers with any mental illness and mothers who refused to participate were all excluded from this study. Based on the inclusion and exclusion criteria given above, only 3978 mothers were interviewed with a 100% response rate, and the rest 4907 mothers among 8885 reproductive-aged women were excluded from the study.
Operational definition
Institutional delivery service utilization refers to mothers who had delivered their last baby in hospitals, health centers, private clinics, NGO health facilities, or Health Posts by skilled personnel. 21
Variables
The current study’s outcome variable was the use of institutional delivery. At the time of the survey, women were asked whether they were delivered to a health institution or not. We developed a binary dependent variable that was coded as 1 for institutional delivery and 0 for non-institutional delivery. The outcome variable was institutional delivery denoted by

Where Thus,
The independent variables included in this study were chosen based on past research and extant literature.4,12 These include the age of the women at birth, place of residence, wealth index, religion, women’s educational level, current marital status, number of antenatal care visits, pregnancy complications, and husband/partner’s educational level.
Statistical analysis
The data from the EMDHS 2019 for this study were cleaned, coded, and analyzed using the statistical tools SPSS version 20 and R version 4.1.2. The R packages used for the analysis of the multilevel model were packages “nlme,” “multilevel” and “glmmTMB.” The risk factors for non-institutional delivery were identified using descriptive statistics such as frequency and percentage, as well as a multilevel binary logistic regression model based on inferential statistics. In the multiple multilevel binary logistic regression analysis, the predictor variables that were significant at the 25% (value 0.25) level of significance in the univariable analysis were included.22–24 With a value, of less than 0.05, the estimated odds ratios and 95% confidence intervals in the multivariable analysis show that the variables are statistically significant, and adjusted odds ratios (AOR) with 95% confidence intervals were used to examine the statistical strength. 25 We fitted a multilevel model to account for the hierarchical nature of the data and to minimize possible parameter underestimation from a single-level model. 26 In this study, we use region of residence as a level-2 variable to group respondents. By integrating random effects in the model, this technique improves the single-level logistic regression model. Three models were estimated: the null model, the random intercept with fixed coefficient, and the random coefficient model. As a result, a two-level multilevel model was used to model the log of the chance of using institutional delivery as follows:

Where
Results
Within 11 clusters (9 regions and 2 city administrations), a total of 3978 women were considered in this study to establish the characteristics that influence the utilization of institutional delivery. The result of this study showed that the utilization of institutional delivery was 54% and the rest 46% of the mothers who gave birth were delivered out of the institution or in a home (Figure 1).

An overview of the prevalence of institutional delivery.
Regarding age categories, 259 (60.9%) of the 425 women between the ages of 15 and 19 gave birth at a health facility. The bulk of the respondents was between the ages of 20 and 24, and 692 (58.8%) of the mothers in this age group had given birth in a health facility. The percentage of women who gave birth in a health institution was 36.4% for mothers without formal education, 64.1% for those with a primary school, and 90% for those with a secondary and above education. In all, 137 (3.4%) of the 3978 women in this study had attended a health institution for ANC visit 8 times and above during their previous pregnancy, and from which 123 (89.8%) of women gave birth at a health facility. Women in rural areas make up a higher proportion (74.8%) of the population, and less than half (43.0%) of them give birth at a health institution. Similarly, a high percentage of 1806 (45.4%) of women whose husbands had no formal education, and just 54.2% of them gave birth in a health facility. About half of women (47.0%) live in households with a low wealth index. Detail descriptions of the study participants regarding listed independent variables are presented in (Table 1).
Summary of descriptive statistics results regarding utilization of institutional delivery against predictors variables assigned in this study (n = 3978).

ANC: antenatal care.
In this study, around 54% of mothers delivered their most recent child to a medical facility. The Benshangul Gumz region had the highest proportion of women who gave birth at a health institution (10.9%), followed by Harar (10.7%). Women from Somalia had the lowest number of institutional delivery (3.4%) (Figure 2).

The percentage of mothers in each in 11 regions (clusters) regarding institutional and home delivery.
Multilevel binary logistic analysis of the Data set
A two-level structure was used in the multilevel analysis, with regions as the second-level units and individual mothers as the first-level units. Multilevel models were used to account for and investigate regional heterogeneity in institutional delivery. The information is organized in a two-level hierarchical framework, with 3978 mothers on level 1 and 11 regions on level 2.
The plot shows the estimated residuals for all 11 regions in the sample. For a substantial number of regions, the 95% confidence interval does not overlap the horizontal line at zero, indicating that institutional delivery in these regions is significantly above average (above the zero line) or below average (below the zero line) (Figure 3).

A caterpillar plot, which plots each residual with its 95% confidence band (y-axis) against rank( x-axis) obtained from the null model.
Model selection and heterogeneity test
To analyze the variability of institutional delivery per woman among the 11 regions (9 regions and 2 city administrations), a likelihood ratio test was used. Since the values of LRTs for the null model
Although a null model has no independent variables, it provides estimates of variance between the region ≤
Testing the presence of Intra-class Correlation within the regions from the null model.

The random intercept model has a lower computed deviation, AIC, and BIC value than the random coefficient and null models. In comparison to the intercept-only model and the random coefficient model, the random intercept model fits well to identify the potential variables that affect institutional delivery to differences between and within regions (Table 3).
Summary results of multilevel binary logistic regression model selection criteria.

AIC: Akaike information criterion; BIC: Bayesian information criterion.
Variable selection
A univariate study of each variable is the first step in the deliberate selection process. A candidate for multivariate analysis is any variable that has a significant univariate test at some arbitrary level. The Wald test from logistic regression is used, with a p-value cut-off point of 0.25. The factors of age, place of residence, wealth index, mother’s educational level, religion, and the number of antenatal care visits are statistically significant and the rest of the current marital status, pregnancy complications, and husband’s education level were insignificant at alpha 0.25 (Table 4). Thus those variables insignificant at the univariate level were excluded from the final multivariate multilevel logistic regression model (Table 5).
Summary results of univarite analysis.

significant at 5%, ANC: antenatal care.
Multilevel Logistic Regression results from the 2019 EMDHS showing characteristics related with institutional delivery among women aged 15–49 (n = 3978).
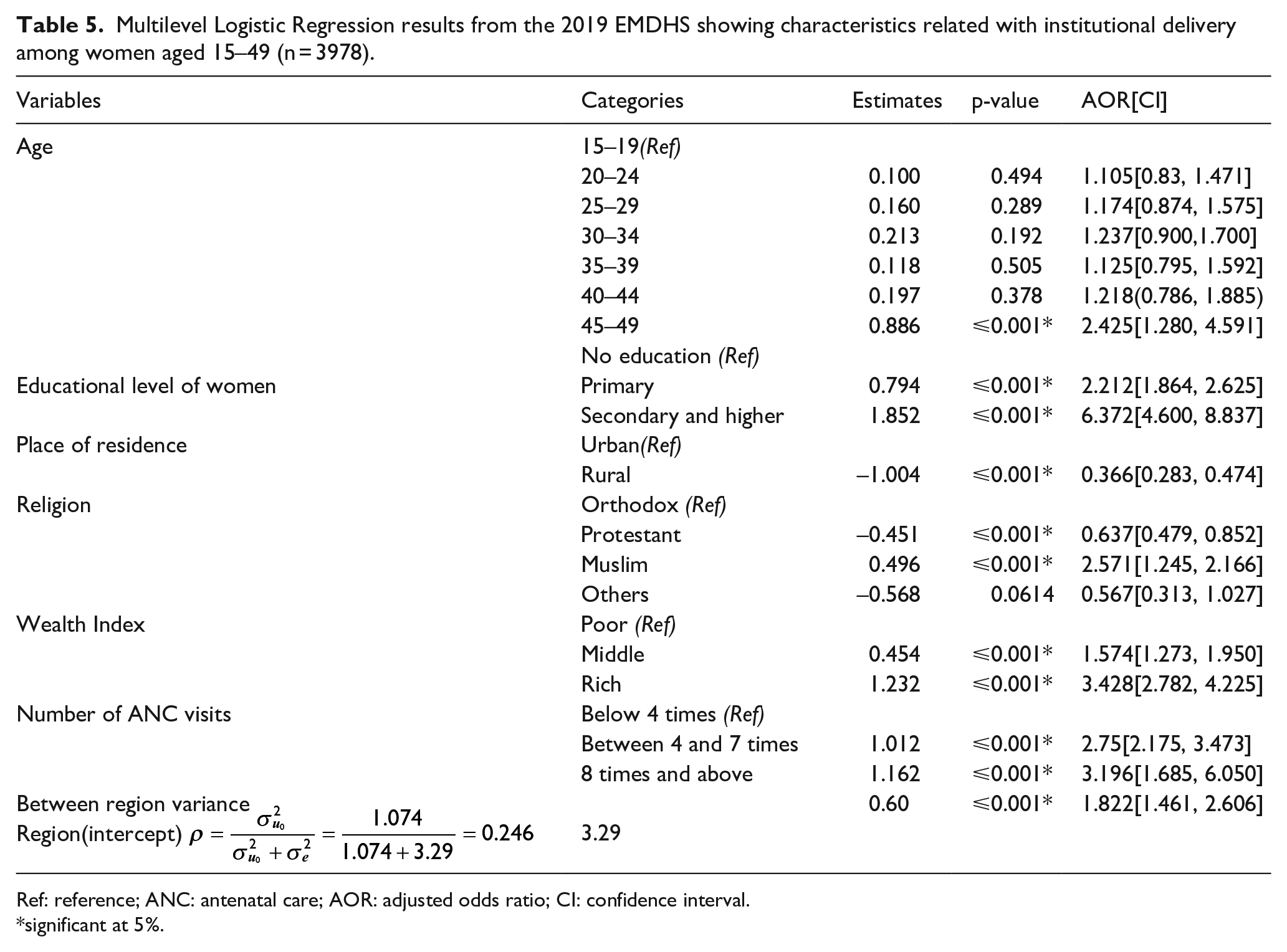
Ref: reference; ANC: antenatal care; AOR: adjusted odds ratio; CI: confidence interval.
significant at 5%.
Factors that contribute to the disparity in the Utilization of institutional delivery in Ethiopia
The model can be generalized so that level-1 covariates have different effects in different locations. In a random intercept model, we allowed the intercept only to vary across regions(clusters) by fixing explanatory variables but the relationship between explanatory and response variables can differ between regions in many ways.
To account for clustering, the multilevel binary logistic regression model with random effects was used first. The model is expected that it would explain the heterogeneity effects due to regional variations (level-2 units). The utilization of institutional delivery per mother differs by region, as evidenced by the fact that the variance of the random intercept at the region level (i.e
From the multilevel binary logistic regression model, the factors age, place of residence, wealth index, mother educational level, religion, and the number of antenatal care visits are statistically significant and differ between regions of the country.
When other variables were controlled for and the intercept parameter was allowed to vary across regions, the likelihood of institutional delivery for protestant is 0.6 times (AOR = 0.637, 95% CI:- 0.479, 0.852) lower and, 2 times (AOR = 2.571, 95% CI: 1.245, 2.166) higher for Muslim religious follower mothers compared with orthodox religion follower mothers. When all other variables are held constant, these odds are reduced by 0.66 times for women in the 25–34 age range. When all other variables are held constant, the odds of delivery at a health institution was higher for women in the age group 45–49 were 2 times (AOR = 2.425, 95% CI:- 1.280, 4.591) higher compared with those mothers in the age group 15–19 years. The frequency of ANC visits was significantly associated with institutional delivery. After adjusting other variables in the model, the odds of giving birth at a health institution was 3 times (AOR = 3.196, 95% CI: 1.685, 6.050) higher among women who had recommended eight or more visits compared with those who had less than four ANC visits. The odds of delivery at a health institution was lower for women residing in rural (AOR = 0.366, 95% CI:- 0.283, 0.474) compared with those mothers residing in urban areas. The odds of delivery at a health institution among women who attend primary school was 2 times (AOR = 2.212, 95% CI: 1.864, 2.625), secondary school and higher was 6 times (AOR = 6.372, 95% CI: 4.600, 8.837) higher compared to women who had no formal education, respectively. Compared to women residing in poor households, the odds of institutional delivery were higher for women residing in with middle (AOR = 1.574, 95% CI: 1.273, 1.950), and rich (AOR = 3.428, 95% CI: 2.782, 4.225) wealth index households (Table 5).
Discussion
Using the EDHS data and an appropriate modeling approach, this study further attempted to identify the determinant factors of institutional delivery service utilization in Ethiopia. By considering the clustered nature of the 2019 EMDHS data set, the multilevel logistic regression model was carried out in identifying factors associated with institutional delivery service utilization. The descriptive result of this study showed that the level of institutional delivery was 54%. The result from multilevel logistic regression analysis showed that age, place of residence, wealth index, mother’s educational level, religion, and the number of antenatal care visits were significantly associated factors with institutional delivery. Across regions, there was a large variance in institutional delivery. According to the intra-class correlation coefficient (ICC), the region of mothers accounts for about 25% of the entire variation in institutional delivery. The multilevel logistic regression analysis confirmed the significance of the regional difference in the utilization of institutional delivery in Ethiopia. The null model suggests that women with the same characteristics in different regions have different rates of institutional delivery suggesting the need for interventions to focus more on the regional level followed by the individual level. 12
Women’s education is crucial in determining where they will give birth.6,7,15,29– 35 Access to information, financial independence, and autonomy are examples of possible processes, all of which contribute to a higher degree of awareness and knowledge of healthcare delivery. These factors may combine to influence mothers’ knowledge of the importance of seeking better medical care, including giving birth in a health facility. 12 The wealth index is a composite measure of a household’s total living standard that can be used to estimate socioeconomic status. The current study revealed that women’s socioeconomic status is a positive association with institutional delivery. This is supported by other studies.7,34 Household wealth can influence women’s choices about where to give birth, access to health care, transportation, and other costs. Women who can afford to pay such fees are more likely to seek medical help. Antenatal care is a proximal predictor of a woman’s choice of delivery location. Women who had the WHO-recommended minimum number of visits were more likely to give birth in a health institution. This is because women who seek medical attention during their pregnancy are more likely to seek medical attention during their delivery. This finding is comparable with other previous studies conducted in Ethiopia and Tanzania.10,12,36– 38 Antenatal care is the most convenient way for mothers to learn more about the risks and complications that may arise during delivery. Women who routinely visit a health institution for ANC services had previously shown some acceptance of the healthcare system and were advised by health experts to give birth there. In the current study, women’s residence was significantly associated with the utilization of institutional delivery services. Women residing in rural areas had a lower likelihood of delivery at a health institution than urban residents. This finding is consistent with other previous studies conducted in sub-Saharan African countries. 39 – 43 Women who live in cities are more exposed to media messages, are better educated and informed, and are closer to health care facilities. For mothers who live in rural areas, the distance to a health institution and transportation issues make it less likely that they will give birth at a health facility. 44 In rural Ethiopia, women’s health seeking behavior is also influenced by deeply established negative attitudes and myths about institutional delivery, insufficient health services, and poor infrastructure. Ethiopian government have tried tremendous work to improve the health of its citizens and to reduce maternal mortality. But there is no considerable improvement compared with the countries five year back report about institutional delivery. 12 Hence, the government have work on again on, women education, health institution coverage, ANC service, and poverty reduction.
Strength and limitation
This was a population-based research project with high sample size. Using advanced methods, multiple confounding variables were examined. The study’s cross-sectional design prevents judgments about the temporal nature of the relationship between the independent variables and the desired outcome. Recall bias and unmeasured confounders such as parity, which were not captured in the 2019 EMDHS.
Conclusion
Ethiopia continues to have a poor degree of institutional delivery services and there are a significant number of women still give birth at home. Institutional delivery was substantially linked with age, place of residence, wealth index, mother’s educational level, religion, and the number of antenatal care visits. These characteristics must be considered in programs aimed at improving institutional delivery in Ethiopia.
Footnotes
Acknowledgements
We would like to acknowledge CSA for allowing access to the 2016 EDHS dataset.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The data from EDHS was accessed with permission from CSA. Because the study subjects did not participate directly and the data was secondary, informed permission was not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets and materials used in this study are available upon request to the corresponding author.