
Abstract
Objective:
Women’s experiences of sexual violence can be not only psychologically and physically traumatizing but may also have lasting effects on brain functions, including cognitive control relating to the inhibition and processing of emotion. Thus, the purpose of this pilot study is to explore underlying neural correlates of sexual violence’s impact on cognitive control in women.
Methods:
Thirty women (aged 21–30 years) participants underwent a quantitative survey along with an affect-congruent Go-NoGo task. Prefrontal activity was monitored using functional near-infrared spectroscopy, a portable neuroimaging technology. An analysis of variance tested for main effects of the condition (Go versus NoGo), group (sexual violence versus no prior sexual violence), and potential interactions.
Results:
Fifteen of 30 women reported a history of childhood (n = 5) and/or adult (n = 12) sexual violence. Those with sexual violence histories reported significantly higher depression, anxiety, and posttraumatic stress symptoms, as well as increased impulsivity compared to their peers. Behavioral performance did not differ between the groups; however, functional near-infrared spectroscopy data revealed a significant (group × condition) interaction in Optodes 13 and 16. Women with histories of sexual violence had a significantly lower response during the “NoGo” condition and a heightened response during the “Go” condition, in the right dorsolateral prefrontal cortex.
Conclusion:
These results suggest altered prefrontal cortical activity during cognitive processing in women with a history of sexual violence, showing hypoactivity during response inhibition and hyperactivity to the positive stimuli. These findings have strong translational promise for innovative assessment and prevention of untoward effects among women with sexual violence.
Introduction
Sexual violence (SV) is sexual activity when consent is not obtained or freely given. 1 While anyone can experience SV, women disproportionately bear these painful encounters, with an estimated one in three women experiencing some form of unwanted sexual contact in their lifetime. 2 Emerging adult and young adult women are at the highest risk for SV compared to women of other age groups. For example, 54% of sexual assault or rape occurrences are experienced by women between the ages of 18–34 years. 3 Emerging adulthood is also a particularly important time for brain development, marked by dynamic personal and environmental circumstances, and unique patterns of vulnerability to psychological dysfunction. 4 Thus, understanding the impact of SV at the level of the brain in emerging adult women is particularly important to understand the impact of trauma and violence while the brain is still maturing.
Trauma and the Brain
Brain responses to trauma vary depending on the type and nature of the traumatic event. In general, exposure to acute experimental stressors, including violence, has been associated with deficits in working memory,5,6 cognitive flexibility, 7 and with atypical dorsolateral prefrontal cortex (DLPFC) function, 7 whether or not the individual developed any subsequent psychopathology. 8 Similar deficits in higher cognitive function are also common features of acute and chronic posttraumatic stress disorder (PTSD).9–11 Understanding cortical and subcortical impacts of specific types of trauma, however, is important as reviews have shown that there are different impacts at the level of the brain based on the specific type of abuse or maltreatment experienced. 12
Neuroimaging research in SV survivors has relatively recently become an emerging field of study. One review that aimed to understand mechanisms and psychosocial sequelle after SV surveyed 20 neuroimaging studies conducted in this population prior to 2012. 13 This review revealed some findings that demonstrated structural differences between those who had experienced SV and those who had not, including reduced volume in the hippocampus, a region of the brain involved in episodic memory, and impulse control.14–18 However, not all studies found these structural differences.19–21 Other neuroimaging studies used functional imaging to examine neural activation and cerebral blood flow, revealing SV survivors evidenced decreased blood flow in the hippocampus when exposed to emotionally valenced stimuli.16,22,23 In addition, relative to healthy controls, women who experienced sexual abuse as a child and had subsequent PTSD demonstrated decreased blood flow to the orbitofrontal cortex, anterior cingulate, medial prefrontal cortex, hippocampus, and fusiform gyrus when processing emotional word pairs. 23 SV survivors were also found to have greater problems recruiting the prefrontal cortex when attempting to downregulate negative emotional responses. 24 Overall, these findings can be explained as specific modifications to sensory systems and pathways as a means of attenuating the effects of repeated exposures and thus reducing distress. These modifications may shift how an individual responds to traumatic reminders by “altering conscious perception but leaving intact the subcortical pathways that provide a non-conscious route to circuits that can generate a rapid behavioural or emotional response to threats.” 12 However, the mechanisms by which cognitive control may be impacted by SV, particularly when exposed to affective stimuli, remain an area of active investigation.
Since the 2012 review, there have been an increasing number of neuroimaging studies examining the psychological and neural bases of emotion regulation. 25 These findings corroborate what was mentioned above, reporting that the prefrontal cortex, along with the amygdala, displays unique activation patterns among those who have experienced trauma in domains such as symptom provocation, fear processing, and resting states. 26 Studies have also found that maltreatment may particularly impact circuitry related to threat detection and response wherein amygdala activity can be modulated through both a conscious and an entirely subcortical, non-conscious means. 27 Here, maltreatment has been most strongly associated with a reduction in gray matter volume and integrity of regions primarily involved with threat perception and contextual memories. 12 For example, studies have found that there are differences in amygdala activation between maltreated and non-maltreated children to angry, fearful, or sad faces during early phases of the response, when the more rapidly engaged, non-conscious component is likely to predominate.12,28,29 Thus, heightened amygdala responses to perceived threats in maltreated individuals may result from a more-dominant involvement of the unconscious subcortical components as opposed to the more conscious cortical components.
Neuroimaging Research in SV-exposed Populations
To date, most neuroimaging studies in those who have experienced SV and abuse have used functional magnetic resonance imaging (fMRI) technology to measure subcortical regions which has significant limitations in its application for intervention evaluation related to cost, lack of portability, and participant limitations (e.g. claustrophobia, metal within body). The ability to measure the cognitive impact of SV on domains such as cognitive control of vulnerable populations in clinically relevant and accessible manners may eventually enable development of biomarkers for individualized treatments. Thus, there is a critical need to study cognitive control while learning more about the potential differences in cognitive control at the level of the brain in individuals with histories of SV compared to their peers.
Near-infrared light can be employed as a noninvasive probe which can be used to monitor changes in the concentration of oxygenated hemoglobin and deoxygenated hemoglobin during functional brain studies. 30 Analogous to fMRI, functional near-infrared spectroscopy (fNIRS) provides information on local changes in blood oxygenation concentrations. FNIRS is a safe, portable, low-cost, flexible neuroimaging technology for mapping select areas of the human cortex that shows great potential for intervention evaluation, given its ability to reach more diverse populations who may not be eligible for fMRI. 30 In contrast to fMRI, fNIRS is relatively inexpensive, portable, with a rapid application time (5–10 min), and has near-zero run-time costs. FNIRS also has particularly important translational implications for those who have been exposed to trauma, as its application does not require the participant to be enclosed in small spaces, making it a potentially more trauma-informed approach to gather neuroimaging data in this population.
Inhibitory control is an important executive function which guides an individual’s ability to control attention, thoughts, and/or emotions to override prepotent/impulsive responses to external cues. 31 Cognitive control is often studied using the Go-NoGo task, a classic response-inhibition neuroimaging paradigm to understand how deficits in control are mediated, especially in the context of clinical conditions such as trauma. 32 Of particular relevance to this pilot study, recent papers demonstrated that fNIRS can detect the differential pattern of activations expected in Go-NoGo tasks,33–35 with one study finding that lateral prefrontal regions are activated during inhibition (NoGo), while the medial prefrontal cortex is recruited during active responding (Go). 35 This set of findings is very encouraging, as it suggests that fNIRS can be successfully used to assess frontal inhibitory function. Few studies to date have used fNIRS technology to examine these responses during a Go-NoGo task in those who have experienced SV. In addition, prior focus has been on subcortical regions, but there is also an importance in capturing cortical contributions of these response patterns.
The Present Study
This study is a secondary analysis of pilot study using fNIRS to understand neural correlates of sexual risk in young, urban women at risk for HIV. In the present analysis, we used SV survey questions to classify individuals and attempt to understand cognitive control differences between those who had experienced SV and those who had not experienced SV, but were demographically similar. We hypothesized that there would be differences between these groups, with the SV group having lower (impaired) recruitment in the prefrontal cortex during the affective “NoGo” condition, but heightened recruitment during the affective “Go” condition compared to their peers.
Methods
This is a secondary analysis of a cross-sectional pilot study (N = 30) initially developed to understand neural correlates of sexual risk in young, urban women at risk for HIV using survey data and fNIRS tasks. This study compares survey, neuroimaging, and behavioral data of women in this study who had a history of SV (n = 15) compared to women who did not (n = 15). See following references for other neuroimaging studies with similar sample sizes.36–40
Recruitment
Participants were recruited via flyers and provider referrals from a family-planning clinic and from a nearby university September 2016 to July 2017, both of which were located in a large urban area in the northeast United States (N = 30). Individuals were eligible for this study if they (1) identified as a woman, (2) were between the ages of 18–30 years old, (3) read English at a fifth grade level or higher, and (4) were not currently pregnant. Interested participants contacted study staff via phone to schedule their 1.5-h survey and fNIRS data collection session. The study had Institutional Review Board approval from the University of Pennsylvania (Protocol # 816390). All participants provided written informed consent.
Procedure
After completing the informed consent process, a survey was completed using both paper and pencil for demographic and health information, and a Computer-Assisted Self-Interview (CASI) for more sensitive questions related to sexual activity, substance use, mental health, and experiences of violence/abuse. Following collection of demographic and survey information, participants performed cognitive tasks on a computer, while changes in prefrontal activity were monitored using fNIRS (procedure described below). After completing the fNIRS portion of the study, participants received a US$40 Visa gift card for their participation along with a list of women’s health resources in the community pertaining to sexual and reproductive health, mental health, substance use and domestic violence/sexual assault services.
fNIRS data collection
Following the survey, participants were seated in a dimly lit room in front of a computer monitor and keyboard. They were then set up with the fNIRS equipment. FNIRS data were collected using the fNIR Imager 1000 (fNIR Devices, Potomac, MD). Participants’ foreheads were cleaned using an alcohol swab prior to positioning the fNIRS probe over the forehead and securing the straps. Two wavelengths of light (730 and 850 nm) were measured continuously at 500-ms intervals in 16 channels. 41 The positioning of light source and detectors on the sensor pad yielded a total of 16 active optodes. COBI Studio software 42 was used for data acquisition and visualization.
After setup was complete, participants were asked to sit comfortably and interact with the computer by only pressing a designated button with their right index finger. Instructions were presented for each task on the monitor and were read aloud. Testing proceeded once participants acknowledged that they understood all instructions. Each task had a practice session prior to each experimental session to ensure participants understood task instructions.
Tasks
Participants underwent an affect-congruent (Spiders-No, Puppies-Go!) Go-NoGo task. 43 The stimuli for this task were images naturally linked to approach (GO!: baby animals) and avoidance (STOP!: scorpions and spiders), with the goal of representing “real-world” situations (“ecological validity”) engaging the participants, and reducing demands on working memory (see Figure 1). The task has been detailed in previous behavioral 43 and imaging 44 studies. Standard Go-NoGo task(s) usually probe motor pre-potency/inhibition, with arbitrary, non-emotional stimuli. 32
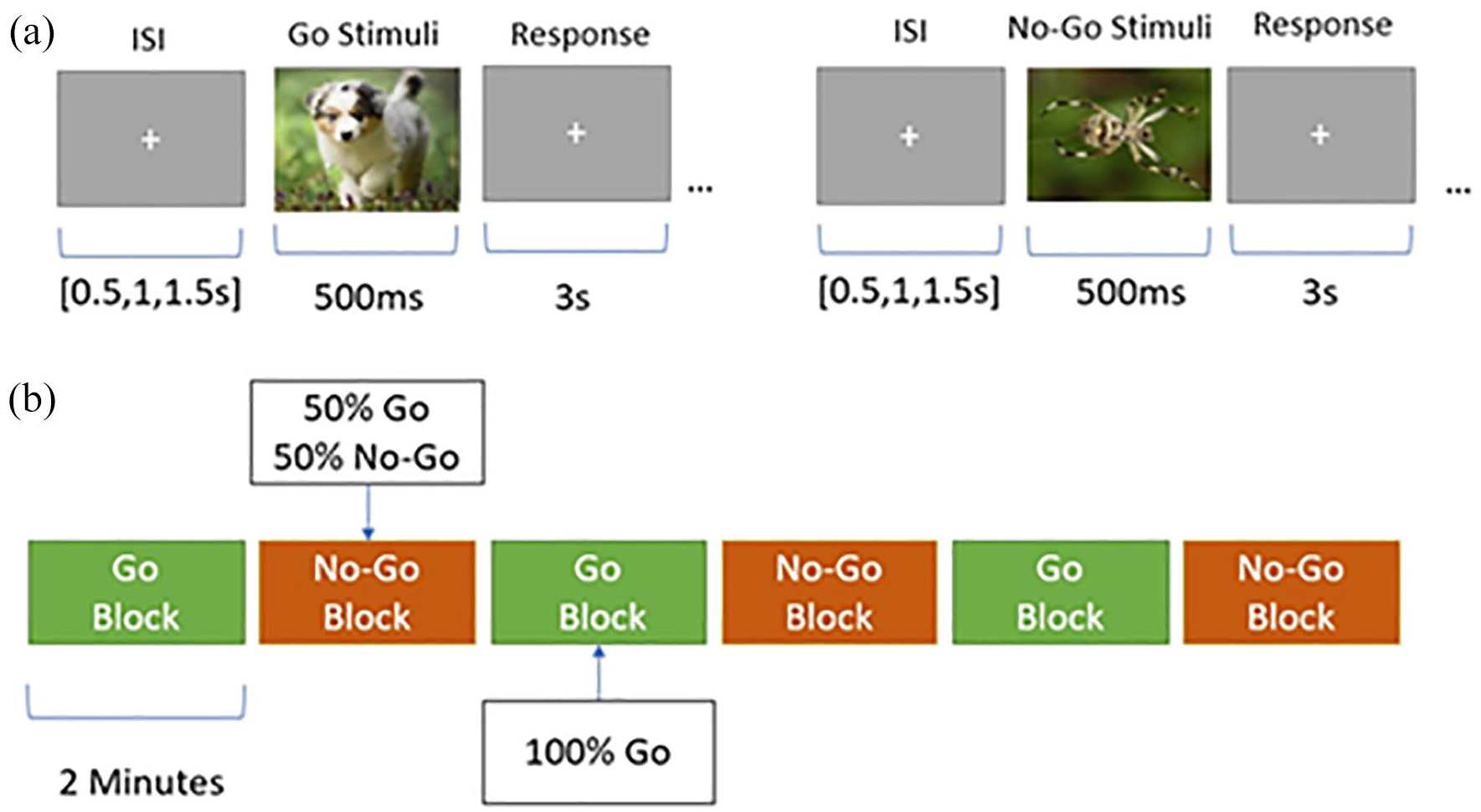
Affective Go-NoGo! Task paradigm. (a) Individual stimuli presentation with interstimulus interval (ISI) lengths, Go/NoGo stimuli presentation, and response block. (b) Go/NoGo task block order and stimuli proportion.
Individuals were instructed to press a button whenever they encountered Go stimuli and withhold their button press response when they encountered NoGo stimuli. The task was arranged in Go and NoGo blocks. Go blocks contained 20 (100%) Go stimuli, whereas NoGo blocks consisted of a quasi-random combination of 10 (50%) Go and 10 (50%) NoGo stimuli per block. The higher proportion of Go versus NoGo trials was used to increase the prepotency of the button press response. For each participant, the task began with a Go block with subsequent blocks alternating between Go and NoGo. Each visual stimulus was presented for 500 ms, and participants were given a window of 3000 ms to respond. The interstimulus interval was jittered at increments of 500 ms to discourage anticipatory responding. This task was intentionally designed with relatively long interstimulus intervals to ensure high levels of accuracy such that the brain substrates of successful response inhibition could be examined independent of performance differences. These six blocks were categorized into two conditions with three blocks per condition.
Survey measures
Demographic and health information
Participants were asked standard demographic questions about age, race, ethnicity, education, number of children, substance use history, and mother’s level of education (as an indicator of socioeconomic status).
SV history
A binary yes/no variable was created using responses to sexual abuse-specific questions from the Adverse Childhood Experiences Questionnaire (ACE) 45 as well as to questions about forced sex in adulthood. The ACE consists of 10 items inquiring about different adverse childhood experiences including abuse, neglect, mental illness or substance abuse by family members, and family dysfunction. This has been shown to be reliable and has been validated in prior research.46,47 Questions taken from this survey include (1) during the first 18 years of life, did an adult or older relative, family friend, or stranger who was at least 5 years older than yourself ever touch or fondle you in a sexual way or have you touch their body in a sexual way?; (2) during the first 18 years of life, did an adult or older relative, family friend, or stranger who was at least 5 years older than yourself ever attempt to have or actually have any type of sexual intercourse, oral, anal or vaginal sex with you? To capture a variety of adult unwanted sexual experiences, participants were also asked about unwanted vaginal or anal sex since the age of 18 years: (3) since you were age 18 years till today, have you ever had vaginal sex when you did not want to?; (4) since you were age 18 years till today, have you ever had anal sex when you did not want to? Participants who responded “yes” to any of the four aforementioned questions were placed in our SV history group (n = 15). Participants who responded “no” to all of these questions were placed in our non-SV history group (no-SV, n = 15).
Depression symptoms
Depression symptoms were measured using the Center for Epidemiological Studies-Depression (CES-D) questionnaire, a validated and widely used instrument related to mood.44–49 This is a 20-item instrument that asks participants to evaluate feelings and symptoms associated with depression (e.g. restless sleep, poor appetite, feeling lonely) on a 4-point Likert-type scale. CES-D scores range from 0 to 60, with high scores indicating greater depressive symptoms. 48 Cronbach’s alpha for this study was 0.91.
Posttraumatic stress symptoms
Posttraumatic stress symptoms were assessed using the PTSD Checklist for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; PCL-5). 50 The PCL-5 is a 20-item instrument that asks participants to evaluate symptoms associated with PTSD on a 5-point Likert-type scale (0 = not at all, 4 = extremely). A score of 33 is the current clinical cut-off for probable PTSD. 51 The PCL-5 has excellent psychometric properties (e.g. test–retest reliability, internal consistency, convergent and discriminant validity) and high scores indicating greater posttraumatic stress symptoms. 51 Cronbach’s alpha for this study was 0.87.
Anxiety symptoms
Anxiety symptoms were measured by the Generalized Anxiety Disorder-7 scale (GAD-7). 52 The GAD-7 is an eight-item instrument, scored on a 4-point scale (ranging from not at all to nearly every day), that is based on DSM-IV diagnostic criteria for Generalized Anxiety Disorder. The response options of the GAD-7 range from 0 to 21, with scores ⩾5 representing mild, scores ⩾10 representing moderate, and scores ⩾15 representing severe anxiety symptom levels. 52 The GAD-7 also has good sensitivity and specificity for the three other anxiety disorders (e.g. panic disorder, social anxiety disorder). 53 Cronbach’s alpha for this study was 0.85.
Impulsivity
Impulsivity was measured using the Barratt Impulsivity Scale (BIS). 54 The BIS is a 30-item instrument that measures impulsive tendencies on a 4-point Likert-type scale (e.g. “I act on impulse,” “I consider myself always careful”). Possible score totals ranged from 30 to 120, with higher scores indicating greater total levels of impulsiveness. A systematic review of psychometric properties of this scale concluded that the BIS has reliability and criterion-related validity across samples. 55 Cronbach’s alpha for this study was 0.82.
Analysis
Signal processing and statistical analysis
For each participant, raw fNIR data (16 optodes × 2 wavelengths) were low-pass filtered with a finite impulse response, linear phase filter with order 20, and cut-off frequency of 0.1 Hz to attenuate the high-frequency noise, respiration, and cardiac cycle effects. 42 Each participant’s data were checked for any potential saturation (when light intensity at the detector was higher than the analog-to-digital converter limit) and motion artifact contamination by means of a coefficient of variation-based assessment. 56 fNIRS data for each training block were extracted using time synchronization markers received through serial port during the experiment, and hemodynamic changes for each of the 16 optodes during each trial block were calculated separately using the Modified Beer–Lambert Law (MBLL). The hemodynamic response at each optode was averaged across time for each trial block to provide a mean hemodynamic response at each optode for each block. Relative changes in oxyhemoglobin (HbO) and deoxyhemoglobin (HbR) for each activation condition were calculated relative to distinct local baselines measured during the first 10 samples at the beginning of the Go and NoGo blocks. Changes in oxyhemoglobin and deoxyhemoglobin for the two activation conditions were calculated relative to respective local baseline segments.
Data analytic approach
To quantify differences in mental health symptom burden and impulsivity by group, Stata statistical software (v15.1) was used. 57 The significance criterion was set to α = 0.05. We then used two sample t tests to understand group differences in symptoms of depression, anxiety, posttraumatic stress, and impulsivity. Descriptive statistics were used to demonstrate sample characteristics.
We used linear mixed effects models to estimate effects of task conditions on cerebral hemodynamics and behavioral performance. Linear mixed effects models offer advantages over analysis of variance (ANOVA) when modeling hemodynamic changes. They do not require an equal number of observations per participant. Linear mixed effects models allow for the estimation of parameters unique to individual participants. Hemodynamic biomarkers were specified as dependent variables. The models were estimated in NCSS 2021 statistical analysis software. 58 For whole-probe analyses, we examined the Level 1 effect of motor response inhibition, controlling Type I error rate using the false discovery rate59,60 to correct for multiple comparisons. For the region-of-interest (ROI) analyses, we examined (1) the Level 1 effect of motor response inhibition, (2) the Level 2 effect of behavioral accuracy (i.e. “true negative” responses on the affective Go-NoGo task), and (3) the motor response inhibition × behavioral accuracy cross-level interaction on participants’ relative levels of oxyhemoglobin in inferior lateral and medial aspects of the PFC during the task. These results were then compared by group to understand differences in prefrontal activation (SV versus no-SV).
Results
Study sample
Thirty women participated in our study with a mean sample age of 25 years old (SD = 2.4). Sixteen women (53%) identified as White, eight women (27%) identified as African American or Black, four women (13%) identified as Asian, and two women (7%) identified as more than one race. Five women (17%) identified as Hispanic or Latina. Fifteen participants (50%) experienced some form of SV (only childhood (n = 3), only adult (n = 10), or both (n = 2)). One adult participant experienced both unwanted anal and vaginal sex in adulthood, but the rest of our sample did not report any unwanted anal sex. Additional demographic characteristics can be found in Table 1.
Study demographic and history results.

SV: sexual violence.
Differences between SV and non-SV groups
Differences in mental health symptom burden between groups
Those with SV histories reported significantly higher depression symptoms (mean CES-D score = 20.6, SD = 10.74) compared to those who did not have SV histories (mean CES-D score = 7.5, SD = 3.64; p < 0.0001). In addition, those with SV histories reported significantly higher anxiety symptoms (mean GAD-7 score = 33.5, SD = 6.93) compared to those who did not have SV histories (mean GAD-7 score = 26.46, SD = 5.27; p < 0.01). Relatedly, those with SV histories reported significantly higher PTSD symptoms (mean PCL-5 score = 32, SD = 8.38) compared to those who did not have SV histories (mean PCL-5 score = 23.46, SD = 6.34; p < 0.01). Finally, those with SV histories reported significantly higher impulsivity symptoms (mean BIS score = 65.13, SD = 10.11) compared to those who did not have SV histories (mean BIS score = 57.6, SD = 9.11; p = 0.04).
Behavioral results
High levels of accuracy (true positive responses, i.e. correctly responding to Go stimuli) were achieved on the affective Go/NoGo task for both the Go (0.98 ± 0.06) and NoGo conditions (0.96 ± 0.09). True negative responses (i.e. correctly withholding responses to NoGo stimuli) averaged an accuracy of 0.85 ± 0.12. Response time to Go trials in both conditions was faster for the Go condition (421.7 ± 62.3 ms) than the NoGo condition (492.6 ± 63.6 ms). Paired t tests revealed a mean of difference of −64.2 ms between conditions (t = −9.98, df = 29, p < 0.0001). However, there were no significant differences in measures of accuracy or response time between individuals with SV histories and those without.
Neuroimaging results
Main effect of task condition
Linear mixed effects models were used to assess the effect of task condition (Go/NoGo) and group membership (SV, non-SV) on evoked prefrontal activity as measured by fNIRS. Multilevel analysis showed a significant effect for the task condition on prefrontal oxygenated hemoglobin changes (see Table 2). The fixed effect of condition was broadly significant for medial prefrontal optodes (Opt 5–12, F > 5.35, df = 1, p < 0.027) (see Figure 2) and showed a weaker effect for lateral optodes (Opt 2, 3, 14, and 15, F > 4.53, df = 1, p < 0.040). In general, estimated fixed effects for the NoGo task condition were positive, suggesting that the Go condition featured an increased cortical response when compared to the NoGo condition.

Parametric plot for fixed effect of Condition during affective Go-NoGo task.
Main effect of task condition (affective Go-NoGo) on prefrontal oxygenated hemoglobin changes.

p < 0.001; **p < 0.01; *p < 0.05.
Differences in Go-NoGo contrasts between groups
Linear modeling assessment of the effect of SV history did not show a significant fixed effect in any optode (all p > 0.1). See Table 3 for multilevel analyses comparing average cortical activation over both NoGo and Go conditions between experimental groups. Significant interactions were observed between task condition and experimental group (see Table 4 and Figure 3) in Optodes 13 (F(1,159.9) = 10.637, p = 0.001) and 16 (F(1,151.9) = 7.149, p = 0.008). However, only Optode 13 survived after adjusting using false discovery rate (FDR) correction (see Figure 4). Post hoc tests showed a significant difference (Bonferroni corrected) between SV versus non-SV during the Go condition in Optode 13 (SV > non-SV, F(1) = 5.67, p = 0.02). In addition, there was a significant difference (Bonferroni corrected) in the SV group, comparing Go versus NoGo conditions (F(1) = 12.47, p < 0.001).

Parametric plot for fixed effect of Condition*Group during affective Go-NoGo task.

Evoked cortical changes in Optode 13 during affective Go/NoGo task by SV history.
Multilevel analyses comparing oxyhemoglobin levels across NoGo and baseline conditions.

SV: sexual violence.
p < 0.001; **p < 0.01; *p < 0.05.
Multilevel analyses comparing oxyhemoglobin levels across Go and baseline conditions.

p < 0.001; **p < 0.01; *p < 0.05.
Discussion
This study found that in a sample of urban, emerging adult women (n = 30), half of our participants reported a history of forced sex in adulthood and/or childhood sexual abuse (n = 15). In this sample population, women who had a history of SV reported significantly higher depression, anxiety, posttraumatic stress, and impulsivity symptoms compared to those who did not. This study employed an affective Go-NoGo task to investigate inhibitory control in individuals with SV when using emotional stimuli. Neuroimaging results showed that women with histories of SV had significantly different cortical responses compared to their peers, with lower activity in the right DLPFC during the “NoGo” condition, but higher activity during the “Go” condition. Our results support prior findings of a high prevalence of SV history among women during emerging and young adulthood, along with further evidence of the high mental health symptom burdens and potential alterations to cognitive processing associated with SV.
It is estimated that approximately one in five (21.3% or an estimated 25.5 million) women in the United States experience completed or attempted rape at some point in their lifetime. 61 These statistics do not include other forms of unwanted sexual contact that can occur in both child and adulthood. In addition, this same study found that 81.3% of women victims experience SV prior to the age of 25 years, indicating the particular high-risk age group of the women we studied. Research also suggests an association between SV and a range of mental health problems—including PTSD, depression, anxiety, and so on and that a high proportion of people in contact with mental health services have experienced SV.62,63 Our findings build on these data, revealing the significantly higher mental health symptom burden women who experience SV can carry compared to their peers, even those who have experienced other types of trauma and abuse in their life.
Our study found that women who experienced SV had significantly higher impulsivity scores compared to the non-SV group. Previous research on impulsivity has indicated an association with suicidal behaviors within adults with co-occuring mental health concerns with links between abuse, impulsivity, and suicide attempts.64–66 This may contribute to why more than half of those who had experienced rape or attempted rape reported having attempted suicide as a result of their experiences. 67 In addition, in survivor populations, impulsivity and other associated behaviors (e.g. substance use and sexual risk-taking) have frequently been found. 62 While many have attributed this to survivors “acting out” or attempting to gain control over their environment, our fNIRS findings reveal that there may be underlying neural correlates that help to explain the differences in conscious choices made by survivors. Future research should seek to understand how the brain responds to other impulsivity-related tasks in survivor SV, including more “real world” scenarios to get a better sense of the relationship between impulsivity, brain reactivity, and risk-taking behaviors at the level of the brain.
Traumatic experiences such as SV incidents are frequently associated with alterations to cognitive processes in domains such as attention, memory, and decision-making7–12 and may be especially impacted when affective processing is a key component in task performance.23–28 Using fNIRS technology, we found that women who experienced SV had different cortical responses compared to their peers, with lower recruitment in the right DLPFC during the “NoGo” condition, but heightened recruitment during the “Go” condition. The DLPFC is primarily associated with executive function, working memory, selective attention, cognitive control, and control over emotion. Thus, the differences in cortical recruitment during inhibition of motor responses may reflect changes in the functional networks associated with cognitive control in women with a history of SV. Interestingly, this same group experienced heightened recruitment in similar regions during the “Go” condition, where participants saw puppies or other baby animals, indicating a potentially hyper response to more positive emotional stimuli. These differences could not be attributed to behavioral performance differences, as errors of commission/omission were similar between groups. We do not know from this initial study whether a heightened response to positive/appetitive stimuli might have maladaptive real-world correlates (e.g. over-response to food, sexual, or drug reward). Although the behavioral scores (“errors of commission”) in Go-NoGo tasks can be used to predict real-world behavior, imaging studies with Go-NoGo tasks show that the brain response during these tasks may be a more sensitive predictor, offering prediction even when the scores themselves through the probe do not differ. 68 This explains why these findings are provocative, and they cannot be attributed to task performance differences.
A key question concerns the fundamental nature of these SV-associated brain differences. To start, our two groups differed significantly in scores related to depression, anxiety, PTSD, and impulsivity, and the physiological effects of this heightened mental health symptom burden may explain some of the cognitive differences noted. In addition, while most postulate that extreme stress or abuse is bad for the brain and especially bad for the developing brain, 69 an alternative perspective is that the brain and the way it processes information may be selectively modified by the stress experienced due to maltreatment in a meaningful manner.70,71 For example, Teicher et al. propose that “childhood abuse alters the development of particular brain regions, in an experience-dependent plastic manner, to facilitate survival and reproduction in what seems, so far, to be a threatening and malevolent world” (p. 653). 12 From this perspective, what we interpret as psychopathology may demonstrate evolutionarily selected alterations in cognition, affect, and behavior.
This study revealed potential differences in cognitive control at the level of the brain when survivors of SV engaged in an affective-congruent cognitive control task. This indicates the presence of processing differences that may not have been discovered when looking at behavioral data alone, highlighting the importance of further understanding the impact of abuse at the level of the brain. In addition to providing more sensitive screening/prediction, neuroimaging through mechanisms such as fNIRS can reveal potential brain targets for interventions (e.g. behavioral, medication, stimulation) intended to bolster inhibitory control. Thus, while this study was the first study of our knowledge to attempt to understand differences in cognitive control, using an affective Go-NoGo task, at the level of the brain for SV survivors, additional research is needed to further explore these findings in this population, to better understand what this might mean for behavior that occurs outside of the laboratory setting.
While this article is primarily focused on brain responses, it is important to recognize the many limitations of looking at these responses in isolation. To start, this study focuses on individual differences and characteristics alone, and does not take into account the protective or destructive role one’s social support, access to resources, and environment can play in the brain’s recovery after SV. Relatedly, due to our study design, we cannot know for certain if differences in cortical recruitment occurred as a result of one’s SV experience—just that significant differences in cognitive control are correlated with SV survivorship. An additional limitation surrounds the stimulus presentation in alternating blocks. While latter ones were well balanced (50% Go and NoGo trials), across the whole presentation sequence of stimuli, the NoGo trials represent a more seldom event. Thus, there is a possibility that what we are interpreting as an inhibition effect could also be a rare stimulus detection signal. We also are aware that while the way SV was operationalized is considered standard, this may not be exhaustive of the types of SV individuals can experience.
This was a secondary analysis of a pilot study with a relatively modest sample size (N = 30) and we were limited by the instruments and tasks given to individuals in the original study. Future research should attempt to see if these findings remain stable with a larger sample size, SV-focused tasks, and a more comprehensive SV history assessment. This will allow a more nuanced interpretation of differences in cumulative versus single event SV as well as potential differences in childhood versus adult SV through better homogenization of experimental groups. Future research should attempt to replicate and expand upon this study to understand how trauma characteristics can further impact cognitive control and decision-making.
Conclusion
The takeaway here is not that survivors are “broken,” but rather that they may have some brain reactivity differences that may explain some of the complex social, behavioral, and emotional consequences they experience. This demonstrates that there is potentially some level of decision-making that is driven by differences of neural activity, which helps to decrease some of the shame and self-blame some survivors feel at their trauma reactions and symptoms. By specifically understanding the neuro-cognitive impact of SV, we can provide better psychoeducation to our patients, understand intervention targets, and measure the impact of interventions at the level of the brain. The portability and affordability of fNIRS makes developing and testing the impact of interventions at the level of the brain possible, to allow for an additional avenue to improve the functioning and lives of these individuals. This study’s findings demonstrate translational promise for innovative assessment and prevention of untoward effects among women with SV.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221081326 – Supplemental material for Neural correlates of cognitive control in women with a history of sexual violence suggest altered prefrontal cortical activity during cognitive processing
Supplemental material, sj-docx-1-whe-10.1177_17455057221081326 for Neural correlates of cognitive control in women with a history of sexual violence suggest altered prefrontal cortical activity during cognitive processing by Laura Sinko, Paul Regier, Adrian Curtin, Hasan Ayaz, Anna Rose Childress and Anne M Teitelman in Women’s Health
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: fNIR Devices, LLC. manufactures the optical brain-imaging instrument and licensed IP and know-how from Drexel University. Hasan Ayaz was involved in the technology development and thus offered a minor share in the new startup firm fNIR Devices, LLC. All other authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by NIMH R21 MH097583 (Anne M Teitelman and Anna Rose Childress, MPI); Penn SON Faculty Pilot Grant Program (Anne M Teitelman); University of Pennsylvania, Provost’s Research Facilities Development Fund (Anne M Teitelman/Anna Rose Childress); T32DA028874-10 (Anna Rose Childress); Drexel BIOMED Faculty Dev Award (Hasan Ayaz).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.