
Abstract
The management of women with a pregnancy of unknown location (PUL) can vary significantly and often lacks a clear evidence base. Intensive follow-up is usually required for women with a final outcome of an ectopic pregnancy. This, however, only accounts for a small proportion of women with a pregnancy of unknown PUL location. There remains a clear clinical need to rationalize the follow-up of PUL so women at high risk of having a final outcome of an ectopic pregnancy are followed up more intensively and those PUL at low risk of having an ectopic pregnancy have their follow-up streamlined. This review covers the main management strategies published in the current literature and aims to give clinicians an overview of the most up-to-date evidence that they can take away into their everyday clinical practice when caring for women with a PUL.
Keywords
Introduction
A pregnancy of unknown location (PUL) may be defined as the clinical scenario when a woman presents with a positive urine pregnancy test but the location of the pregnancy (either intrauterine or extrauterine) cannot be located using transvaginal ultrasonography (TVS) at the initial scan. It is important to note that is a classification and not a diagnosis. Further tests and follow-up are then required before the location and/or the viability of a pregnancy can be defined.
The final outcome in a woman initially classified as a PUL is as follows:
Intrauterine pregnancy (IUP – this can either be viable (VIUP) or non-viable (NVIUP));
Failed PUL (FPUL);
Ectopic pregnancy (EP);
Persistent PUL (PPUL).
A VIUP is defined as the presence of an intrauterine gestation sac containing an embryo with a visible heartbeat. A NVIUP is defined as a pregnancy that is confirmed as intrauterine but then subsequently miscarries (meeting national criteria for a miscarriage, which includes a crown-rump length (CRL) of ⩾7 mm with no evidence of a foetal heartbeat or a mean gestation sac diameter of ⩾25 mm in a gestation sac that contains no other structures1,2). A FPUL is defined as a woman who has a negative pregnancy test 2 weeks after her initial follow-up. 3 An EP is defined as an extrauterine mass positively visualized on TVS or confirmed via histology after a salpingectomy. 4 The definition of a PPUL remains contentious but is commonly defined as when >3 serial serum human chorionic gonadotropin (hCG) levels change less than 15%, while the location of the pregnancy remains unclear using TVS.
Women with a PUL may undergo multiple blood tests, ultrasound scans and visits in the fear that an EP is being missed. The reality is that the majority of PUL will either have a final outcome of an IUP (17%–41%) or FPUL (47%–70%) rather than EP (8%–16%). 5 There is, therefore, a clinical need to rationalize the management of PUL so few EP are missed while avoiding unnecessary and costly follow-up for the remaining PUL with a final outcome of FPUL or IUP. Accordingly, there has been a move towards managing PUL based on the likelihood that they will be associated with complications (in general related to EP), that is, as either ‘low risk of complications’ (i.e. a final outcome of IUP or FPUL) or ‘high risk of complications’ (i.e. a final outcome of EP or PPUL), rather than focussing on determining the location of the pregnancy. 6 This approach to risk stratification is clinically relevant as it allows follow-up to be focussed on those deemed at high risk of complications with the follow-up of women at low risk reduced. Having a robust evidence-based system that allows management to be streamlined offers several advantages both for the woman concerned and the healthcare system within which she is seen.
Many women classified as having a PUL will present with lower abdominal pain or vaginal bleeding. These symptoms, however, are not useful determinants of which PUL are at high risk of complications.7,8
It is inevitable that there is a degree of heterogeneity within populations of pregnancies classified as being a PUL. The number of early pregnancies initially classified as PUL within a unit has been reported as anywhere between 8% and 42%. 6 A lower PUL rate is felt to correlate to higher quality ultrasonography as it relates to the ability of examiners to identify the location of a pregnancy at an initial ultrasound scan. 6 As a general rule, a PUL rate of <15% is accepted as an indication that the quality of scanning in early pregnancy is adequate. 9 It should be noted, however, that other factors (such as the gestational age women present at) unrelated to the scanning quality in a unit can also contribute to the PUL rate.
Defining PUL
There are two time-points when the classification of a PUL is clinically relevant:
At the initial scan and when reviewing both initial and subsequent 48-h serum hCG levels (to plan further management);
When the final outcome is defined (to determine the risk of future negative pregnancy outcomes).
An issue encountered when considering the management of PUL is variation in the way it is initially defined. Various consensus documents have been published to resolve this issue,9–11 but there also remains variability between these. The most widely accepted is the consensus classification system published in fertility and sterility. 10
We propose two simplified classifications derived from the data above (see Figure 1).

Schematic for PUL classification at the initial transvaginal ultrasound scan.
PUL classification at the initial scan:
True PUL (no evidence of a pregnancy seen inside or outside the uterus);
PUL likely EP (possible adnexal mass seen);
PUL likely IUP (possible intrauterine gestation sac but no yolk sac or foetal pole seen);
PUL likely miscarriage (possible products of conception seen in the endometrial cavity).
Defining final outcome in PUL (see Figure 2):
FPUL;
IUP;
EP;
PPUL.

Schematic for PUL classification to define the final outcome.
This list is in order of prevalence, with a final outcome of FPUL being most common and that of a PPUL least common.
Investigation/biomarkers
Several management protocols have been put forward to achieve reliable risk stratification in PUL. These centre on the serum biomarkers progesterone and hCG.
Serum progesterone
A meta-analysis on the accuracy of single progesterone levels for predicting pregnancy outcome in PUL found it is a good predictor of pregnancy viability but not pregnancy location. 12 It has been shown that serum progesterone levels of ⩽10 nmol/L are associated with a failing PUL13,14 and that this can be used as criterion to select women for reduced follow-up. The cut-off value used is a trade off, as selecting a threshold of 10 nmol/L is associated with more EP being misclassified into the low risk group. On the other hand, lowering the threshold exacerbates the main drawback of using progesterone by classifying almost all VIUP as high risk. 15
Serum hCG
Serum hCG is the most common commercially available biomarker used to manage women with a PUL. Single measurements of serum hCG are generally not helpful. Furthermore, a ‘discriminatory zone’ (i.e. a single hCG cut-off of 1000 or 1500 IU/L above which an IUP should be visualized) should not be used to decide when to perform a TVS as the majority of EP will be visualized at hCG levels under 1000 IU/L. 16 It is particularly important that the discriminatory zone is not used to make a presumptive diagnosis of EP. The assumption that a VIUP is incompatible with findings of a PUL and an hCG of 1000 or 1500 IU/L is dangerous and should never form the basis for a decision for intervention with methotrexate as it could lead to the inadvertent termination of a wanted IUP. 16 National guidelines in the United Kingdom 1 support this, stating that single hCG values are not useful but trends in hCG levels help predict the final outcome in a PUL. This finding is also supported by a meta-analysis 17 which showed that an absolute single serum hCG level has no diagnostic value. Various approaches to the interpretation of hCG trends are in current clinical use.
hCG ratio
The hCG ratio is defined as the 48-h hCG level divided by the initial (0-h) hCG. A ratio of <0.87 (consistent with a drop in hCG levels of ⩾13% over 48 h) is considered consistent with a final outcome of FPUL. 18 A ratio of >1.66 is likely to result in a final outcome of IUP 19 and a ratio in between those two values is more indicative of an EP/PPUL (see Figure 3).7,20

hCG ratio cut-off values and the likely final outcomes with a PUL.
Mathematical prediction models
Mathematical models developed as decision support tools help determine the likely location and therefore risk of complications in women classified as a PUL. 7 The M4 model 21 is a logistic regression model based on the initial serum hCG and the hCG ratio as variables. It was found to be able to classify 69.6% PUL as at low risk of complications with a negative predictive value (NPV) of 97.5% (i.e. the model was correct in its low risk classification 97.5% of the time). 5 It had a sensitivity of 88.0%, that is, it correctly classified 88.0% of PUL with a final outcome of EP/PPUL as at high risk of complications. This model was found to be superior in performance to a single progesterone cut-off of <10 nmol/L or the hCG ratio alone. 15
The M4 model has been validated clinically as part of a multi-centre cohort study 22 where 835 women classified as a PUL were managed according to the M4 model. It predicted 70% (585/835) PUL as low risk, of which 568 (97%) were confirmed as an FPUL or IUP (see Figure 4). Of the 17 EP/PPUL misclassified as low risk by the model, none came to any significant harm (i.e. none of the missed EP had ruptured either on TVS (on the basis of visualizing blood in the pelvis) or at the time of surgery, required a blood transfusion, had a prolonged hospital stay or suffered any other additional impairment). The low number of adverse events demonstrates that expectant management of PUL using the M4 prediction model is effective and safe.

Flowchart of final outcome data and correct versus incorrect risk stratification by the M4 model.
Further work following on from this has led to the development of a two-step protocol with a new prediction model (M6). 23 This utilizes both serum hCG and progesterone levels in the expectation that when used in combination, they may improve the risk stratification of PUL. The first step selects low risk PUL at presentation if the serum progesterone is ⩽2 nmol/L. These women have no further serum hCG levels or ultrasound scans, but a follow-up urine pregnancy test in 2 weeks to confirm a negative result. In this study, this cut-off threshold applied to 16% of PUL. The remaining PUL have a 48-h serum hCG level taken and are triaged using the M6 model (see Figure 5). This logistic regression model is based on the hCG ratio and the initial serum hCG and progesterone levels. There is also a second version of the M6 model that does not use the initial serum progesterone as a variable for women who are on progesterone supplementation.
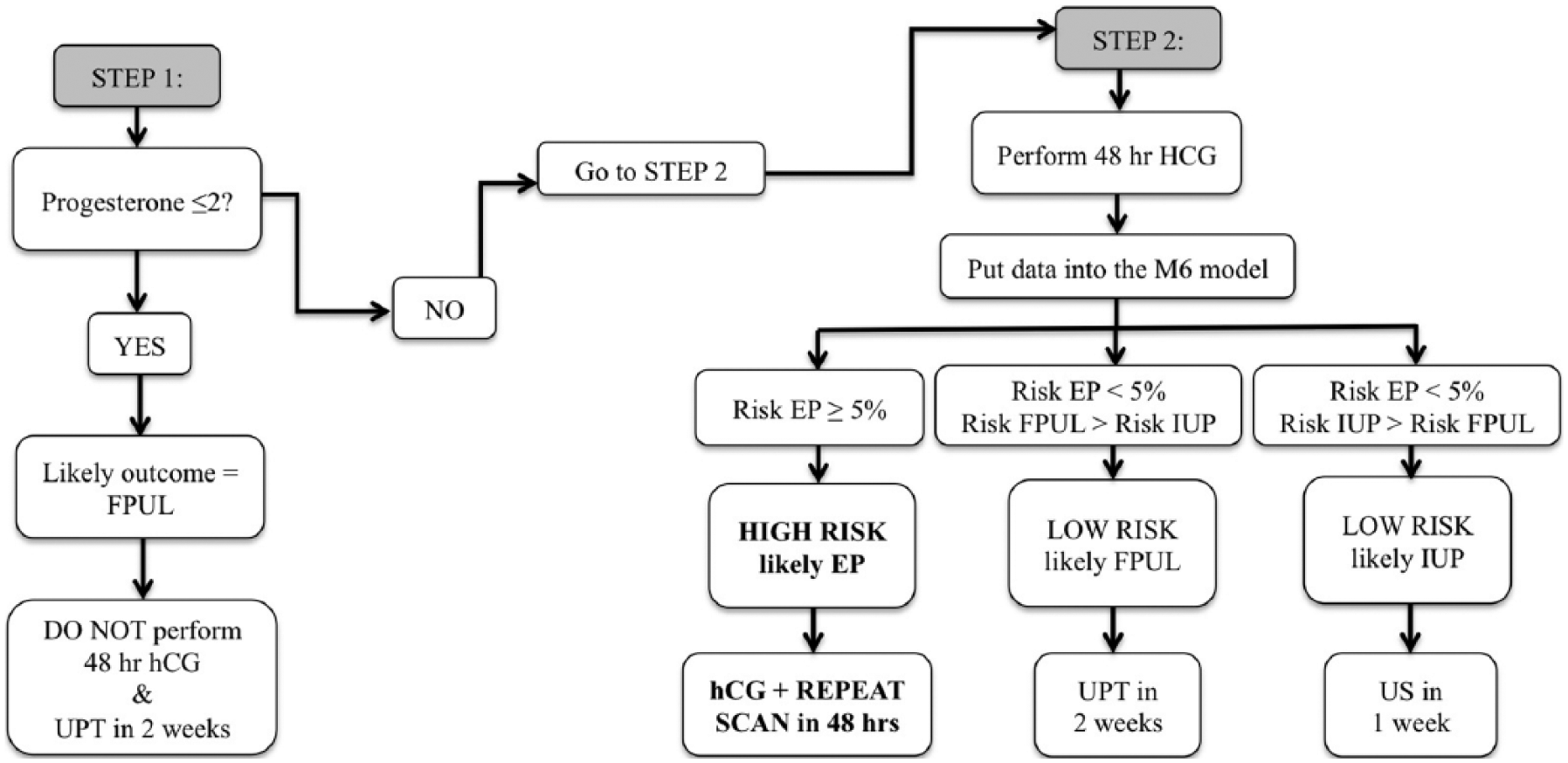
Flow diagram of the two-step approach for managing PUL.
The M4 model required a minimum of two visits for all women. The aim of the two-step protocol was to utilize the initial serum progesterone level to allow discharge of some PUL after just one visit. Furthermore, the M4 model had been developed on a relatively small number of PUL, so to improve accuracy and reliability, the M6 model was developed on a much larger cohort of 2753 cases of PUL. Overall, the two-step protocol classified 62.1% of PUL as low risk, with an NPV of 98.6% and sensitivity for correctly classifying EP as high risk of 92.0% (see Table 1).
Performance of PUL classification approaches.

Source: Taken from Van Calster et al. 23
EP: ectopic pregnancy; PUL: pregnancy of unknown location; prog: progesterone.
Confidence intervals are given between parentheses.
There is a prospective multi-centre cohort study across eight sites in the United Kingdom currently underway to assess the utility of this two-step protocol in everyday clinical practice. In all, 3000 PUL have already been recruited. The M6 model is available for clinical use at no charge via this link: www.earlypregnancycare.com/m6. It can also be downloaded as an app for smartphones (search ‘early pregnancy Leuven’).
Novel biomarkers
Biomarker discovery with PUL is focussed on five key areas (adapted from Cartwright et al. 24 ). This includes biomarkers associated with abnormalities in the:
Fallopian tube (e.g. creatine kinase (CK) and vascular endothelial growth factor (VEGF));
Uterus (e.g. activin B and leukaemia inhibitory factor (LIF));
Embryo/trophoblast (e.g. hCG, pregnancy-associated plasma protein (PAPP-A), α-fetoprotein (AFP), activin A and cell-free foetal DNA);
Corpus luteum (e.g. progesterone, oestradiol, relaxin and inhibin A);
Inflammation/peritoneal irritation (cancer antigen 25 (CA125), interleukin 6 (IL-6), IL-8 and tumour necrosis factor (TNF-α)).
While serum hCG and progesterone remain the only biomarkers in current clinical use for the management of PUL, there is a limit to their accuracy in risk stratification. This has led to the search for numerous novel biomarkers that may be useful either in conjunction with, or as a replacement for, hCG and progesterone.
Studies in this field have concluded that it is unlikely that there will be a single biomarker capable of determining which PUL are at high risk of complications. Future work in this field is now focussing on developing multiplexed serum biomarker tests25,26 that can then potentially be incorporated into logistic regression models.
Management
As long as the patient is haemodynamically stable, PUL should be managed expectantly until the final outcome is determined. Women should be given clear written information advising them that until the location of the pregnancy is known, there is a risk of EP with its associated complications. Those with a final outcome of an IUP or FPUL will rarely need any intervention.
What is the best treatment option if the final outcome is a PPUL?
The classification of PPUL assumes that a final outcome of a VIUP has definitively been ruled out. Similar to EP, PPUL can be managed either expectantly, medically (Methotrexate) or surgically (laparoscopy/uterine curettage). There is no consensus on which of these management options is best. There is currently a randomized controlled trial (RCT) underway to address this question where women with a PPUL are randomized to one of three arms: expectant management, treatment with Methotrexate or uterine curettage. Women undergoing uterine curettage are given Methotrexate if their hCG levels do not sufficiently decline after the procedure. 27
Conclusion
More sophisticated interpretation of serum hCG and progesterone levels have allowed us to improve the care we offer to women with a PUL. EP still accounts for the highest rate of maternal deaths related to early pregnancy. 28 Accordingly, the correct classification of PUL as at low or high risk of complications is clinically important. Single progesterone levels, the hCG ratio and risk prediction models are currently used to risk stratify PUL. Risk prediction models have been shown to be superior to other management strategies. 15 The M6 model is available for clinical use and is based on one of the largest cohorts of PUL reported to date. It is an evidence-based tool to rationalize and improve triage in this cohort of women.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.B. is supported by the NIHR Biomedical Research Center based at Imperial College Healthcare NHS Trust and Imperial College London. S.B. is supported by NIHR CLAHRC NWL (Collaboration for Leadership in Applied Health Research & Care, Northwest London). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. M.A.-M. is supported by Tommys’ National Centre for Miscarriage Research.