
Abstract
Breast augmentation is an increasingly popular cosmetic surgery procedure, and breast implants can also be used in reconstructive surgery following mastectomy. Problematic breast implants can present to any discipline of medicine, most frequently to primary care or acute service such as emergency medicine. This guide aims to inform the non-breast specialist in how to assess and treat common problems and when referral to specialist services is necessary.
Introduction
The number of women with breast implants is increasing: over 11,000 cosmetic augmentations were performed in the United Kingdom in 2013. 1 Breast augmentation is the most common plastic surgery procedure in the United Kingdom, and implants are used in some breast reconstructions after mastectomy. In 2009, 21% of women undergoing mastectomy underwent immediate reconstruction (3216 of 15,479 mastectomies), an increase of 11% from the previous year. 2 These women may present to any discipline of medicine with implant-related or incidental problems. This guide is aimed at non-breast specialists facing such patients, in order to advise on their immediate management, referral guidelines and offer reassurance.
Breast implants
Cosmetic breast implants are most commonly inserted via an incision in the infra-mammary fold (IMF), at the lower limit of the breast. Other incisions include circum-areolar, that is, around the areola and through the axilla. The majority of cosmetic breast implants are sub-glandular, which means, inserted under breast tissue and on top of pectoralis major. The remainder implants are sub-muscular, i.e., beneath the muscle. Implants can be silicone gel or saline-filled; both have a firm outer silicone shell to give them shape. Silicone implants give a more natural feel, but if they rupture silicone can leak into the surrounding tissue and lymph nodes causing painful lumpiness, called ‘siliconomas’. If saline-filled implants rupture, the saline is harmlessly reabsorbed. Breast implants are either round or contoured, or ‘teardrop’. Contoured implants have greater projection at the base and are tapered at the top to give a more natural shape.
Common problems with breast implants
The majority of problems are benign and can be dealt with by routine referral to a breast unit. All UK breast referrals are seen within 2 weeks, there is no indication to send patients to emergency services unless they are acutely unwell or the skin on the breast is threatened (Table 1).
Diagnoses.

A lump in the augmented breast
There are many potential causes for a palpable lump after breast implants, both benign and malignant. Any new breast lump should be referred for further assessment by a breast unit.
A change in the shape of the augmented breast
Implant rupture
Implant rupture is a significant complication of breast implants; rupture rates differ depending on the age of the implant. Reported rupture rates vary between 23% in one small study 3 and 1.8% in a large, multicentre trial using modern silicone implants. 4 Rupture is most commonly spontaneous, although trauma or implant failure can be responsible and saline implants rupture earlier than silicone (5.6 years after insertion vs 12 years). 5 Ruptured implants present with breast lumpiness, redness and swelling. Acutely ruptured implants may appear inflamed, hard and painful. They should be managed with nonsteroidal anti-inflammatory drug (NSAID) analgesia and a routine referral to the breast unit. Ultrasound or magnetic resonance imaging (MRI) confirms the diagnosis. Treatment involves surgical removal or implant exchange. Patients should be reassured that this is not an emergency and that there is no danger from silicone leakage. 6 Implants inserted by the National Health Service (NHS) can be replaced by the service, and privately placed implants can be removed by NHS surgeons but not replaced.
Following rupture, silicon can leak into surrounding tissues or migrate to axillary lymph nodes, and there have been reports of pulmonary deposits. 7 Siliconomas are usually removed surgically, although it is safe to leave them once the diagnosis is confirmed.
Capsular contracture
A layer of fibrous tissue called a ‘capsule’ forms around breast implants after surgical insertion. This capsule can become pathologically thickened causing anything from skin tethering to a painful, hard and distorted breast. It is a major cause for patient dissatisfaction. 8 Diagnosis is clinical and treatment is surgical excision of the capsule, with or without an exchange of the underlying implant.
Seroma formation
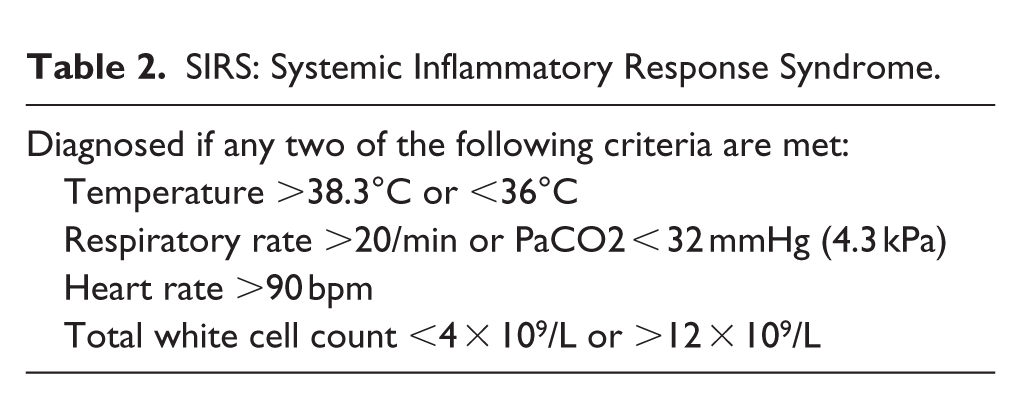
A seroma is a collection of subcutaneous serous fluid, which usually presents as a fluctuant swelling in the early post-operative period (i.e. the first 6 weeks). It can be painful, mostly will be reabsorbed in a given time, but the presence of heat or erythema or an unwell patient usually indicates an infected seroma. Patients who fulfil the systemic inflammatory response syndrome (SIRS) criteria or have seromas large enough to compromise overlying skin, with the risk of, impending necrosis, should be seen acutely by a breast surgeon (Table 2).
SIRS: Systemic Inflammatory Response Syndrome.
Implant rotation
Patients who have had contoured implants may notice a change in the shape of the breast if the implant rotates within the capsule. This will need correcting surgically and should be performed by the surgeon who inserted them.
The hot and red augmented breast
Infection
Infection can affect breast tissue with underlying implants at any time. Risk factors include recent surgery, diabetes, obesity, smoking and lactation. 9 If deep infection affecting the implant occurs, treatment must include implant removal. A patient with breast implants and clinical evidence of infection-associated SIRS or swelling causing impending skin necrosis should be urgently referred to a breast surgeon. Patients with suspected infection and implants that do not meet the criteria outlined above should be treated with empirical oral antibiotics covering skin pathogens and referred to the breast unit routinely.
Capsular tear
Adhesions may form between the implant and capsule, and then, movement of the implant can cause capsular tear. The breast will appear swollen and erythematous due to seroma formation and can be extremely painful. The implant itself is not affected. This can be managed conservatively with NSAIDs and extra analgesia as needed. Avoid aspirating this fluid to prevent introducing infection as in the majority of cases it will be reabsorbed naturally and symptoms will settle. These patients require routine referral to the breast unit to check implant integrity.
Haematoma
Haematoma causes swelling in the immediate or early post-operative period. While it can discolour the breast, if the skin is hot, this implies secondary infection. If the patient does not have signs of SIRS, this can be treated with empirical antibiotics pending a fast-track referral to the breast unit. Occasionally, the patient will need surgical washout of the haematoma if it is large.
The painful augmented breast
Some pain in the immediate post-operative period should be expected and can be managed with simple analgesia. Breast pain alone is rarely a sign of any sinister underlying cause; however, in augmented breasts, it may be due to any of the diagnoses detailed above. Clinical examination should give an indication to the underlying cause, and these patients can be referred to the breast unit on a routine basis.
Advising women with implants or considering implants
Are breast implants safe?
Breast cancer and implants
The largest study of patients with breast implants contained nearly 25,000 women followed up for an average of 20 years and 10 showed a decrease in the number of breast cancers in these women compared to the general population. Possible explanations include the fact that women with breast augmentation tend to have a lower body mass index (BMI), higher socioeconomic class or decreased volume of breast tissue. However, there is no evidence to support any of these theories. These results have been confirmed in two meta-analyses containing over 110,000 women.11,12
Connective tissue disorders and breast implants
A meta-analysis including over 14,000 women found no association between breast implants including silicone-gel-filled implants and any of the individual connective tissues diseases such as rheumatoid arthritis, lupus erythematosus, scleroderma or systemic sclerosis. 13
Breast implants and anaplastic large-cell lymphoma
Anaplastic large-cell lymphoma (ALCL) is a very rare type of non-Hodgkin’s lymphoma. Concern has been raised that there may be a link with breast implants; however, to date, there are only about 170 published cases worldwide in an estimated 5–10 million implants. It presents as a late seroma (i.e. years after implant insertion). Treatment involves surgery to remove the implant and capsule and chemotherapy. The American Food and Drug Administration (FDA) is currently keeping a database of new cases as there is concern that this is an unrecognised condition, which may become more common.14–16
Breast implants and other health considerations
Women who have had breast augmentation had a lower BMI and higher level of daily physical activity compared with the general population in the Women’s Health Initiative Observational Study. 17 The women with breast implants had substantially lower mortality rates and incidence of cardiovascular disease after 12-year follow-up. However, these women reported poorer quality of life and emotional well-being overall with higher levels of depression. Women with cosmetic implants were more likely to smoke and drink more alcohol (Table 3).
The Bottom Line.

Can I breast feed with implants?
Breast implants are inserted behind the breast tissue, so women should still be able to breast feed with implants. There is little evidence, but a small study showed a reduction in success rates of breast feeding in women who had implants compared to those without (63% success with implants vs 88% without). 18 A meta-analysis of three small studies suggests that women with breast implants are less likely to exclusively feed their infants with breast milk and the reasons for this may be multifactorial. 19
Advice for women with Poly Implant Prothèse implants
In 2010, the French company Poly Implant Prothèse (PIP) was found to be deliberately manufacturing breast implants containing substandard silicone. Their rupture rate is two to six times higher than comparable products and they have been banned. Official UK Government advice states there is no need to have PIP implants removed if the patient has no signs or symptoms of rupture. Women are advised to seek removal from the centre where the implants were inserted if they are symptomatic or concerned. The NHS will remove and replace any PIP implants it has inserted. If private providers will not remove or replace PIP implants, the NHS has pledged to remove them but cannot offer replacements.
Breast implants and diagnostic imaging
Breast implants can interfere with diagnostic imaging or cause confusion if the patient thought her implants were irrelevant and has not disclosed them. Some cosmetic appearances are so good that implants may be missed unless specifically examined for.
Echocardiograms
Implants can cause technical difficulties when performing echocardiography both due to the physical positioning and prevention of penetration of ultrasound beams by silicon resulting in reduced accuracy. 15 There is sparse literature concerning this, but as implants become more common and the population with them ages, this may become a greater problem.
Chest X-rays
Implants do not usually interfere with reading chest X-rays, but older implants or those with thickened capsules may be obvious (Figure 1.)

Chest X-ray showing bilateral implants.
More subtle implant appearances can cause diagnostic uncertainty. Figure 2 shows a patient with a left-sided implant and latissimus dorsi reconstruction.
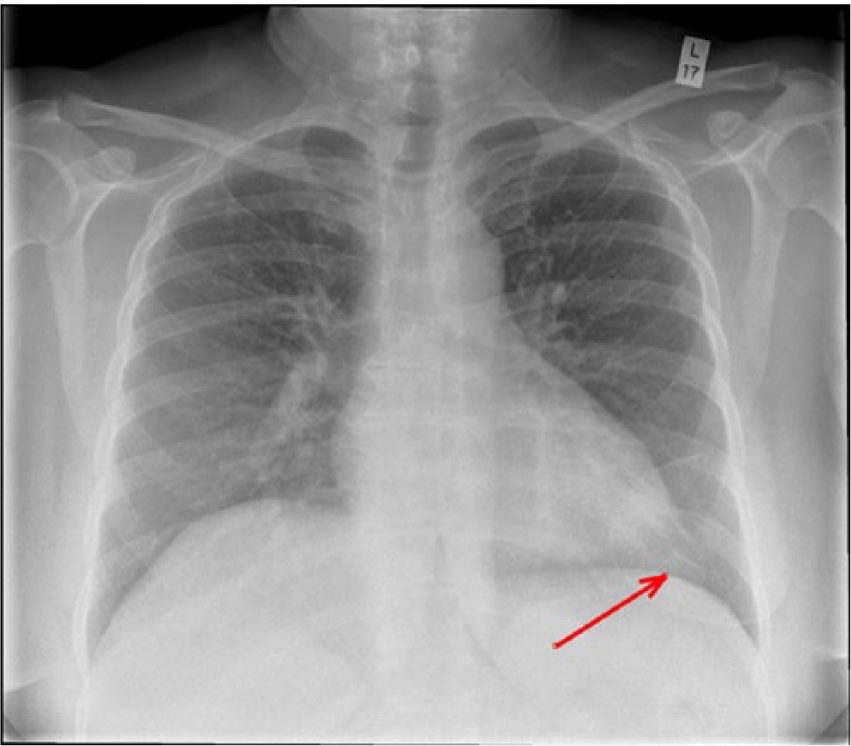
Chest X-ray showing left-sided implant.
Additional imagining
As experience with interpreting the imaging of women with breast implants grows, increasingly implants have not been found to interfere with routine breast imaging (this includes mammography and ultrasound). There is usually no need to perform additional imaging to assess breast tissue in the augmented breast. The main function of breast MRI in implant cases is to assess the integrity of the implants.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.