
Abstract
Background:
Shared governance enhances nurses’ participation in decision-making and professional autonomy. The Index of Professional Nursing Governance (IPNG) is a validated tool for measuring such perceptions, but no German version previously existed.
Aims:
This study aimed to translate, culturally adapt, and evaluate the psychometric properties of the German version of the IPNG.
Methods:
A two-phase study was conducted. Phase 1 included forward–backward translation and cognitive debriefing interviews with 10 clinical nurses. In Phase 2, a cross-sectional online survey was administered to 1090 registered nurses at a Swiss university hospital. Structural validity was assessed using confirmatory factor analysis (CFA), and internal consistency was evaluated with Cronbach’s alpha. Known-groups validity was tested based on demographic and organisational variables.
Results:
CFA supported the original six-factor structure with good fit indices (comparative fit index = 0.97, Tucker–Lewis index = 0.97). The root mean square error of approximation (0.09) and the standardised root mean square residual (0.09) exceeded the threshold but remained within the acceptable range for multifactorial models. Most items had factor loadings above 0.70. Internal consistency was strong (α > 0.80). Known-groups validity showed significant differences by age and commitment.
Conclusions:
The German IPNG is a valid and reliable instrument for assessing shared governance.
Keywords
Introduction
Healthcare systems worldwide are experiencing a growing shortage of qualified nursing professionals, which poses significant risks to the quality, safety, and continuity of patient care delivery (World Health Organization, 2020). This workforce crisis is primarily driven by chronic occupational stress and poor working conditions, which contribute to burnout, job dissatisfaction, and premature attrition from the profession (Peter et al., 2020; Tamata and Mohammadnezhad, 2023). Nurses are frequently exposed to emotional strain resulting from patient suffering and death, workplace aggression, time pressure, extended working hours, shift work, and persistent understaffing (Molen et al., 2020; Peter et al., 2024). These challenges are further intensified by limited opportunities for career advancement, ineffective leadership, and lack of professional recognition, all of which reduce engagement and morale (Aloisio et al., 2021; Niinihuhta and Häggman-Laitila, 2022). Irregular and night shifts often disrupt work–life balance and negatively affect nurses’ overall well-being (Musio et al., 2025; Peter et al., 2021). The cumulative burden of these factors has been associated with early departure from the profession (Hudays et al., 2024; Terry et al., 2025).
In response to these challenges, national and international health strategies increasingly emphasise reforms aimed at improving working conditions and advancing nurses’ professional roles (Peter et al., 2024; World Health Organization, 2020). Governance models that support professional autonomy, shared decision-making, and continuous development have been identified as effective strategies to strengthen workforce sustainability and improve the quality of care (Hess, 2017; Joseph and Bogue, 2016).
In this context, shared governance has gained recognition as a model that promotes both autonomy and structural empowerment. It allows nurses to participate meaningfully in clinical and organisational decisions, assume responsibility for outcomes and contribute to leadership within their institutions (Allen-Gilliam et al., 2016; Wilson and Galuska, 2020). The model is grounded in the principles of partnership, equity, responsibility, and ownership and fosters a practice environment defined by open communication, mutual respect, and collaborative engagement between staff and management (Ayaad et al., 2018; Hamdan and Jaafar, 2024; Swihart and Hess, 2023). Research indicates that such environments support professional growth, enhance leadership competence, and improve care delivery (Hamdan and Jaafar, 2024; Hess et al., 2020).
Conceptually, shared governance is a multidimensional framework that defines how healthcare professionals organise, implement, and evaluate care activities within their institutional context (Wilson and Galuska, 2020). Its essential components include accountability, authority, equity, and transparency. These features contribute to a cooperative work culture that promotes collegial relationships, effective teamwork, and alignment of goals across individuals, units and the broader organisation (Ayaad et al., 2018; Porter-O’Grady et al., 2022). In everyday practice, shared governance empowers nurses to influence decisions related to their clinical work and has been associated with better patient outcomes and improved performance indicators (Allen-Gilliam et al., 2016; Jaber et al., 2022; O’Grady and Clavelle, 2021).
To measure the extent of shared governance, the Index of Professional Nursing Governance (IPNG) was developed and psychometrically validated (Hess, 1998). The current version, IPNG 3.0, includes 50 items across six dimensions: personnel, information, resources, participation, practice, and goals. Based on nurses’ responses, institutions are classified as traditional, shared, or self-governed. The instrument has demonstrated solid psychometric properties, including construct validity and internal consistency, across several international studies conducted in the United States (Anderson, 2011; Hess, 1998) and in other countries, such as Finland, where it has been culturally adapted and validated (Kanninen et al., 2022). Its international application underscores the global relevance of the IPNG as a tool for assessing shared governance in nursing. However, a validated German-language version has not been available to date. This gap limits its applicability in German-speaking healthcare systems and hinders opportunities for international comparative research on nursing governance.
The aim of this study was to translate and culturally adapt the IPNG into German and to evaluate its psychometric properties, with a particular focus on structural validity and internal consistency, among hospital-based nurses in Switzerland.
Method
Design
This study was conducted in two phases. The initial phase of the study entailed translating the IPNG from English to German and conducting cognitive debriefing interviews to assess its acceptability and comprehensibility. In the second phase, the psychometric properties of the German IPNG were evaluated. The reporting of results followed the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guidelines, using the relevant data extraction forms for internal consistency, structural validity, known-groups validity, and cross-cultural validity (Mokkink et al., 2012).
Phase 1: Cross-cultural validity
A comprehensive translation procedure is necessary to ensure cross-cultural validity. After that, the instrument’s psychometric properties, particularly its factor structure, must be evaluated statistically (Mokkink et al., 2012). The IPNG scale was translated following the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Principles of Good Practice guidelines for scientific translation processes (Wild et al., 2005). In the initial stage of the process, the items were translated from English into German by a native German-speaking professional translator and a native German-speaking researcher. Subsequently, the two versions were reviewed by an expert panel, resulting in the formulation of a consensus-based final version 1. The expert panel comprised members of the project team and the translators. In the second step, the items were independently back-translated into English by a native English-speaking translator and a native English-speaking researcher. Based on this back-translation, the expert panel developed the final version 2, which the original author of the IPNG subsequently approved (Hess, 1998). In the final step of phase 1, version 2 was evaluated for acceptability, understandability and clarity using cognitive debriefing (Wild et al., 2005). Finally, a professional German translator proofread the final version.
Cognitive debriefing
The final stage of the assessment process for items regarding acceptability, understandability, and clarity is best conducted through interviews, as this method allows for capturing individual subjective experiences (Miller et al., 2014). To evaluate overall comprehensibility, the cognitive interviewing method proposed by Collins was employed in one-on-one interviews (Collins, 2014). For the results to be generalisable, the questions and responses must be clear and consistent across the target group (Miller et al., 2014). However, even responses that initially appear appropriate can result from misinterpretations of the question (Belson, 1986). Individuals may interpret questions and responses differently due to language proficiency, jargon, education, and experience (Miller et al., 2014). Respondents must progress through four distinct cognitive stages to respond to a question: (a) comprehension of the question and available response options, (b) recall of relevant information, (c) formulation of the response, and (d) provision of the answer (Collins, 2014). The verbal probing technique was employed to validate the cognitive processes involved, whereby responses are subjected to further examination through follow-up questions. These additional questions were predetermined and incorporated into an interview guide. In our interview guide, each evaluated question was matched with one to three follow-up questions per stage, following the guidelines set forth by Collins (2014) (see Supplemental Material A).
Recruitment and study sample
Cognitive debriefing requires a minimum of 10 participants (Miller et al., 2014). Consequently, native German-speaking nurses from the research group's network were invited to participate in person.
Data collection
Data were gathered through individual interviews using the interview guide. If the interviewee encountered difficulties in any of the phases, the interviewer took field notes. All interviews were recorded as backup possibilities in case further information was needed, in addition to the field notes.
Data analysis
The cognitive debriefing interviews were subjected to iterative qualitative analysis to reduce content by following the four steps by Miller et al. (2014): (1) summarising, (2) comparing across respondents, (3) comparing across groups, and (4) concluding, using Microsoft Excel.
This approach enables a more profound comprehension of how questions function and how participants process responses (Miller et al., 2014). The difficulties encountered by participants were classified according to the cognitive stages corresponding to them: understanding the question, retrieving information, valuation of the answer, and providing the answer.
Phase 2: Psychometric evaluation
The psychometric evaluation assessed construct validity through confirmatory factor analysis (CFA) and known-groups validation. This approach ensured that the measure functioned as expected by distinguishing between theoretically distinct groups (discriminative validity) and demonstrating equivalence among similar groups. Additionally, internal consistency reliability was examined to ensure the measure’s reliability.
Recruitment and study sample
To assess the structural validity of a given scale using CFA, it is recommended that the sample size should be at least 10 to 20 participants per item or question on the scale (Kline, 2023). Furthermore, the preferred target is a sample size of over 300 participants (Kyriazos, 2018a). According to the established guidelines, the 50-item IPNG would necessitate a sample size of 500 to 1000 individuals for the 50-item scale under investigation. Accordingly, the objective was to obtain a sample size of 1000 participants. A comprehensive recruitment strategy was implemented at a major university hospital in the German-speaking region of Switzerland, which employs 3500 nurses. Based on an estimated response rate of 30%, the calculated sample size was anticipated to be reached by inviting all nurses to participate.
Data collection
The nurse directorate distributed personal emails to all employed nurses within the university hospital containing details about the study’s purpose, inclusion criteria, data protection measures, and a link to the survey. Participation in the study was entirely voluntary.
Instrument
The instrument included questions on individual characteristics (age, sex, education, profession, function, and experience) and the 50 translated IPNG items. There were no mandatory questions. The items of the German IPNG are summarised in Supplemental Material B. The IPNG has six parts: Personnel, Information, Resources, Participation, Practice, and Goals. Each part has between 5 and 12 items, on a 5-point Likert scale: (1) Nursing management/administration only, (2) Primarily nursing management/administration with some staff nurse input, (3) Equally shared by staff nurses and nursing management/administration, (4) Primarily staff nurses with some nursing management/administration input, and (5) Staff nurses only. For the scoring of the IPNG, six dimensions and an overall score can be calculated: Personnel (n = 12), Information (n = 9), Resources (n = 9), Participation (n = 8), Practice (n = 7), and Goals (n = 5). For each dimension, the sum score is calculated as well as for shared governance across all dimensions. With 50 items the minimum score is 50, and the maximum score is 250 for shared governance, 50–10 is defined as traditional governance, 101–200 as shared governance, and 201–250 as self-governance.
For each dimension and for shared governance, cut-off values exist, allowing the allocation of the health organisation into the three stages of governance: traditional, shared, and self-governance. Formal permission to use and translate the IPNG was obtained from the copyright holder (the Forum for Shared Governance). The Forum provides detailed scoring guidelines and classification criteria upon request.
Known-groups validation
Known-groups differences and similarities are components of construct validity. In this study, we tested known differences or concurrences between different groups based on socio-demographic and organisational variables. Four of the six hypotheses stem from the psychometric evaluation of the original questionnaire (Lamoureux et al., 2014). Lamoureux et al. (2014) formulated the following hypothesised known-groups similarities:
H1: The means of the IPNG overall score do not differ significantly between sexes.
H2: The means of the IPNG overall score do not differ significantly between age groups.
H3: The means of the IPNG overall score do not differ significantly between educational levels.
H4: The means of the IPNG overall score do not differ significantly between wards within the health organisation.
Shared governance leads to structural empowerment of nurses in the organisation (Barden et al., 2011). Nurses who are empowered in the organisation have a stronger bond with the organisation and a greater attachment to their work (Hauck et al., 2011; Spence Laschinger et al., 2001). Therefore, we added the following hypothesis to test for known-groups difference:
H5: The IPNG overall score can be discriminated between groups according to their bond with the organisation.
Data Analysis
For the quantitative analysis, we utilised R (R Core Team, 2023) along with the ‘psych’ (Revelle, 2025) and ‘lavaan’ (Rosseel, 2012) packages. Missing data were managed through listwise deletion for incomplete items on the IPNG scale. We calculated descriptive statistics, including mean, median, standard deviation, minimum, maximum, skewness, and kurtosis. We applied the Grubbs’ test to detect a single outlier and removed extreme values based on the outcome.
CFA was conducted to assess structural validity using the Weighted Least Squares Mean and Variance-adjusted (WLSMV) estimator and the ordered option, as the observed variables in the model are ordinal. This estimator is particularly suited for ordinal data (e.g. Likert scale responses). Given the ordinal nature of the data, the CFA employed polychoric correlations, which assume an underlying continuous distribution for each ordinal variable and estimate correlations between these latent continuous variables. Furthermore, bootstrapping (n = 1000) was applied. Structural validity was evaluated at the scale and sub-scale levels by applying a two-stage model with six factors and one general factor solution to the 50 items to test the factor structure of the original instrument. Model fit was assessed using the following criteria: root mean squared error of approximation (RMSEA) below 0.05 indicated good fit, whereas values below 0.08 were acceptable; standardised root mean residual (SRMR) below 0.08 and comparative fit index (CFI) and Tucker–Lewis index (TLI) scores above 0.95 were considered satisfactory (Kline, 2023).
The two numeric variables, age and bond with the organisation, were categorised into four groups using quartiles to conduct known-groups validation. The bond with the organisation was measured using the three-item COPSOQ scale Commitment to the workplace from the German version of the Copenhagen Psychosocial Questionnaire (COPSOQ; Nübling et al., 2017). Items were answered on a 5-point Likert scale. For each participant, a mean score was computed across the three items. For the known-groups analysis, mean scores were categorised into quartiles. The Levene test for homogeneity of variance yielded a significant result for the sector and education variables (H2, H3). Accordingly, an analysis of variance with unequal variances, followed by Games–Howell post hoc analyses, was conducted. For the remaining hypotheses (H1, H4–H5), an analysis of variance with equal variances and the Tukey post hoc test for significant differences was employed in case of significance. Cronbach’s alpha was used to test the scale’s and subscale’s internal consistency. A value of 0.7 or above was deemed to indicate satisfactory consistency (Cortina, 1993).
Results
Phase 1: Cognitive debriefing
A total of 13 native German-speaking nurses participated in individual cognitive debriefing interviews, each lasting between 25 and 50 minutes. Participants had a mean age of 28 years (SD = 9.3), and 70% identified as female. All were currently employed in healthcare. Their professional backgrounds included registered nurses with degrees from a Fachhochschule (University of Applied Sciences; n = 3, 23%), registered nurses with diplomas from a Höhere Fachschule (College of Higher Vocational Education; n = 3, 23%), Fachfrau/-mann Gesundheit (certified healthcare assistants; n = 3, 23%) and students enrolled in a Bachelor of Science in Nursing programme (n = 4, 31%). Three participants (23%) were additionally enrolled in a Master of Science in Nursing programme.
All interviewees in phase 1 demonstrated a general understanding of the items and answered in line with the purpose of the measure. However, several areas of conceptual ambiguity emerged. The term Gremium was interpreted variably, ranging from formal committees to informal clinical groups, creating uncertainty. A clarifying definition was therefore added to the relevant item blocks.
The term Verfahren (procedures) was consistently perceived as abstract and not reflective of daily clinical routines; it was replaced by Prozesse (processes), which was regarded as more appropriate. Similarly, Vorräte (supplies) was changed to Material, a term more commonly used in clinical practice.
Further uncertainty arose from the distinction between Pflegepersonal (nursing staff) and Pflegemanagement (nursing management), particularly in items that used both beurteilen (to assess) and ermöglichen (to enable). These items were revised to clarify roles and responsibilities.
Some participants reported difficulty identifying the appropriate actors responsible for the described activities, occasionally leading to mid-scale responses or answer elimination strategies. Although a few suggested adding options such as ‘not applicable’ or ‘don’t know’, these were not consistently proposed and thus not implemented.
No additional conceptual issues were reported. Given that the wording revisions improved item clarity without altering meaning, a second round of cognitive testing was not conducted.
Phase 2: Psychometric evaluation
In total, 1090 nurses responded to the online survey in September to October 2023, resulting in a response rate of 31%. The mean age was 33.8 years (SD = 10.57). Most respondents were female (n = 1014, 93%) and registered nurses and midwives (n = 558, 51.2%). Of the 1090 respondents, 542 (49.7%) completed the full IPNG scale. This corresponds to 15.5% of all invited nurses and constituted the final analytic sample for the CFA and known-groups validation. A CONSORT-style participant flow diagram is provided in Supplemental Material C.
The sample is summarised in Table 1.
Sociodemographic and professional characteristics of the study sample..
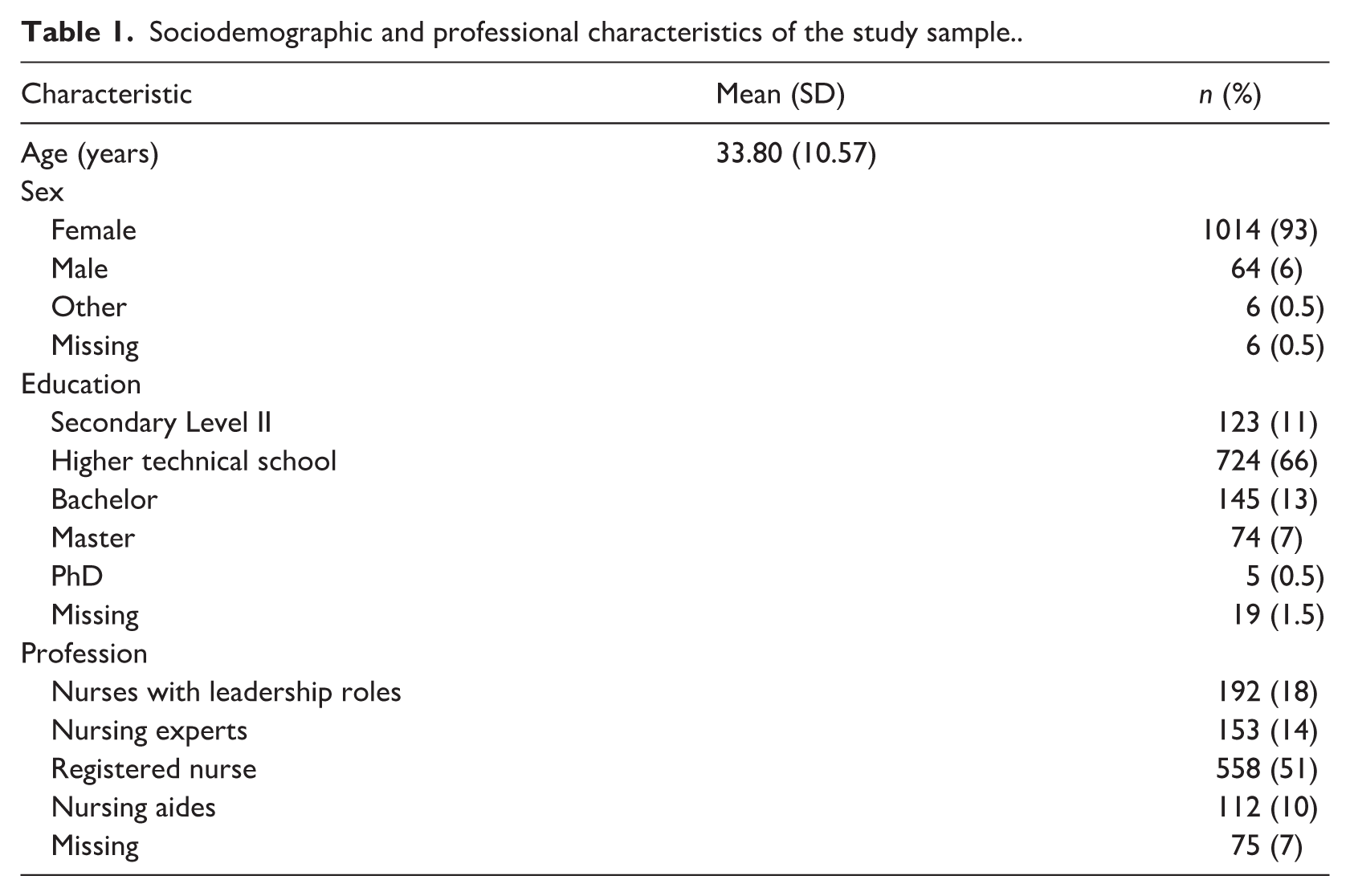
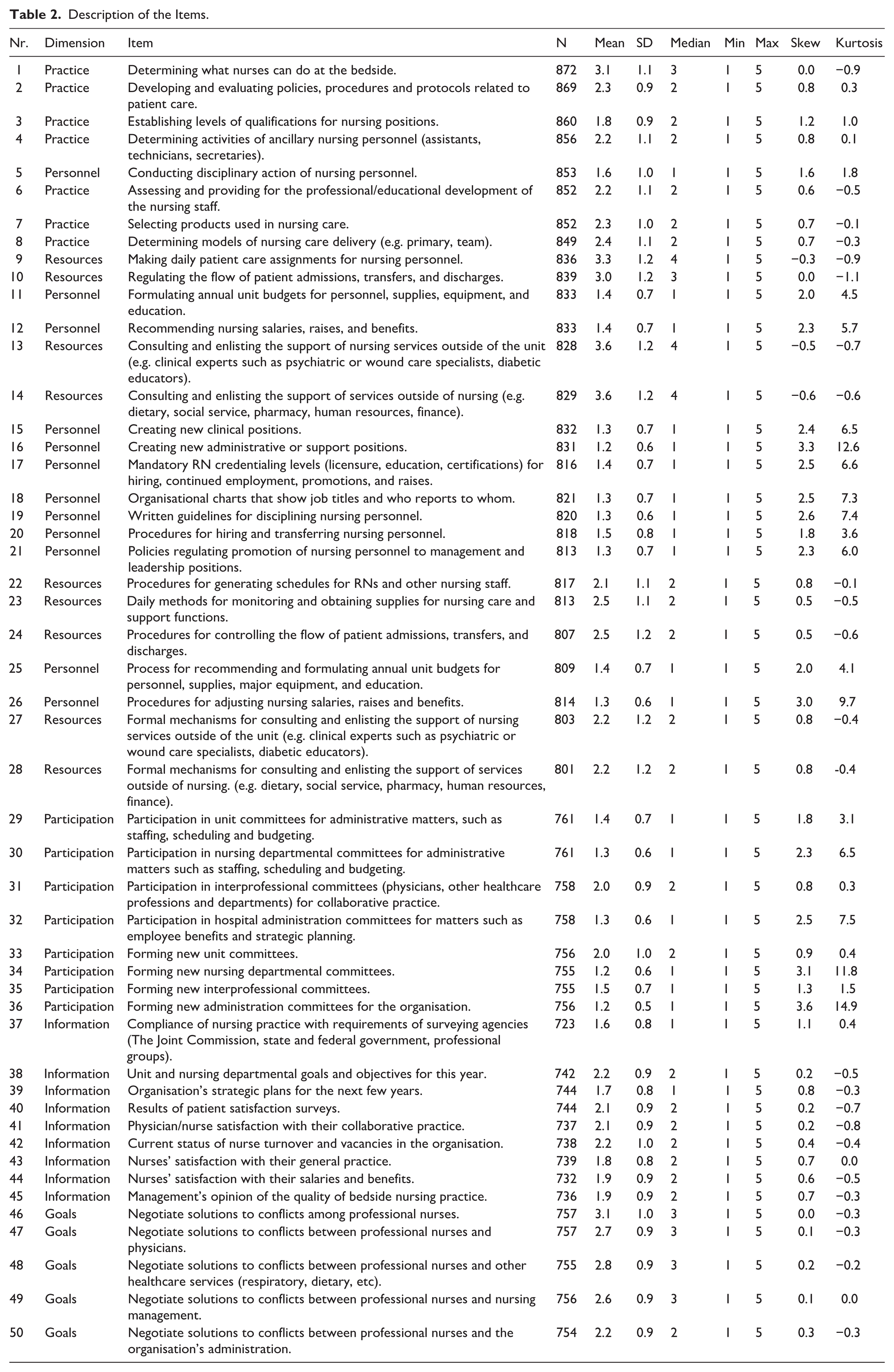
Table 2 summarises the descriptive results of the 50 items. The median of the items ranged between 1 and 4, with high scores indicating tendency towards shared governance/self-governance. Skew and kurtosis for some items were found to be above the cut-offs with <±2 for skewness and <±7 for kurtosis, indicating non-normal distribution. However, since WLSMV is deemed robust to violations of normality.
Description of the Items.
Structural Validity
The results for structural validity are summarised in Table 3. The chi-square test for model fit yielded a significant result (χ² = 6372.519, df = 1169, p < 0.001), indicating a statistically significant deviation from perfect model fit. Although the chi-square test is sensitive to sample size and may not provide a complete picture of fit, additional fit indices suggest the model’s adequacy. The CFI was 0.97, and the TLI was 0.97, exceeding the commonly accepted threshold of 0.95, indicating a good fit between the model and the data. The RMSEA was 0.09, suggesting that while there is some approximation error, it remains slightly above an acceptable threshold of 0.08. The SRMR value of 0.09 further supports an adequate fit of the model, as values below 0.08 are typically considered satisfactory. However, values close to 0.10 can still indicate a reasonable fit, especially in complex models.
Goodness-of-fit indicators of the two-factor solution for the German IPNG.

p < 0.001.
Most items’ standardised factor loadings ranged from moderate to high, reflecting their meaningful contributions to their respective factors. Loadings above 0.7 indicate strong relationships with their factors, consistently observed across most items in F1, F2, F4, and F6 (see Supplemental Material D).
Known-groups validation
No significant difference of IPNG overall score was found between sexes (F2,537 = 1.3309, p = 0.27), leading to non-rejection of H1.
A significant difference of IPNG overall score was found between age groups (F3,292.82 = 6.0253, p = 0.0005). The post hoc analysis suggests that there may be notable differences in the overall self-reported IPNG score across specific age groups. Figure 1 shows a boxplot of the IPNG overall score per age group and indicates the post hoc findings that the youngest and the oldest age groups tend to report higher governance scores. Post hoc pairwise comparisons showed that participants aged 16–24 reported significantly higher IPNG governance scores than those aged 34–41 (p = 0.0014), and participants aged 42–55 reported significantly higher scores than those aged 34–41 (p = 0.0105). In contrast, no other age-group differences were statistically significant. The findings, therefore, reject H2.
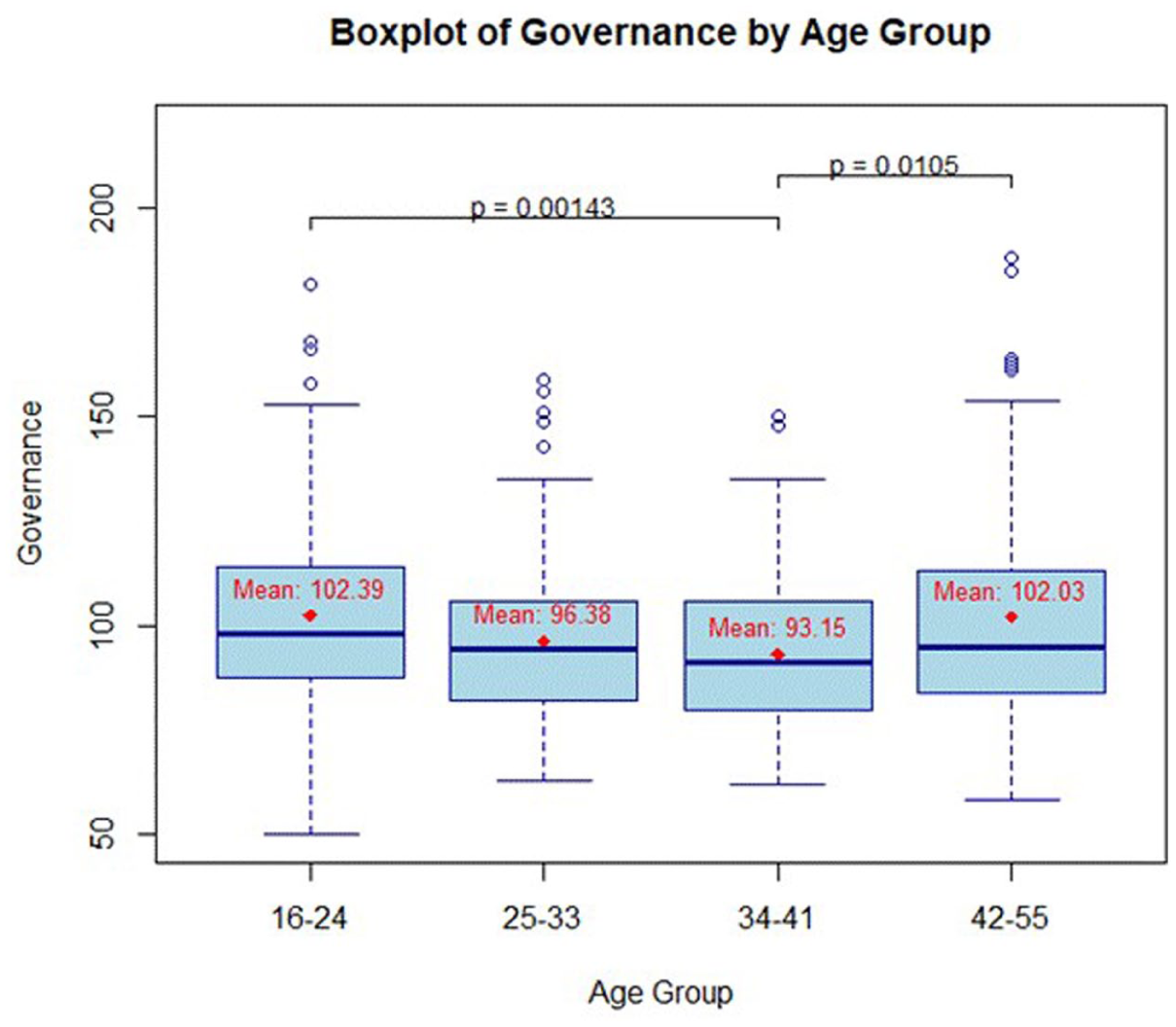
Boxplot of IPNG overall score per age group. The p-values displayed in Figure 1 represent pairwise post hoc comparisons between age groups.
No significant difference of IPNG overall score was found between educational levels (F5,10.057 = 1.2202, p = 0.3673), which leads to non-rejection of H3.
No significant difference of IPNG overall score was found between wards within the health organisation (F11,528 = 1.3639, p = 0.1862), leading to non-rejection of H4.
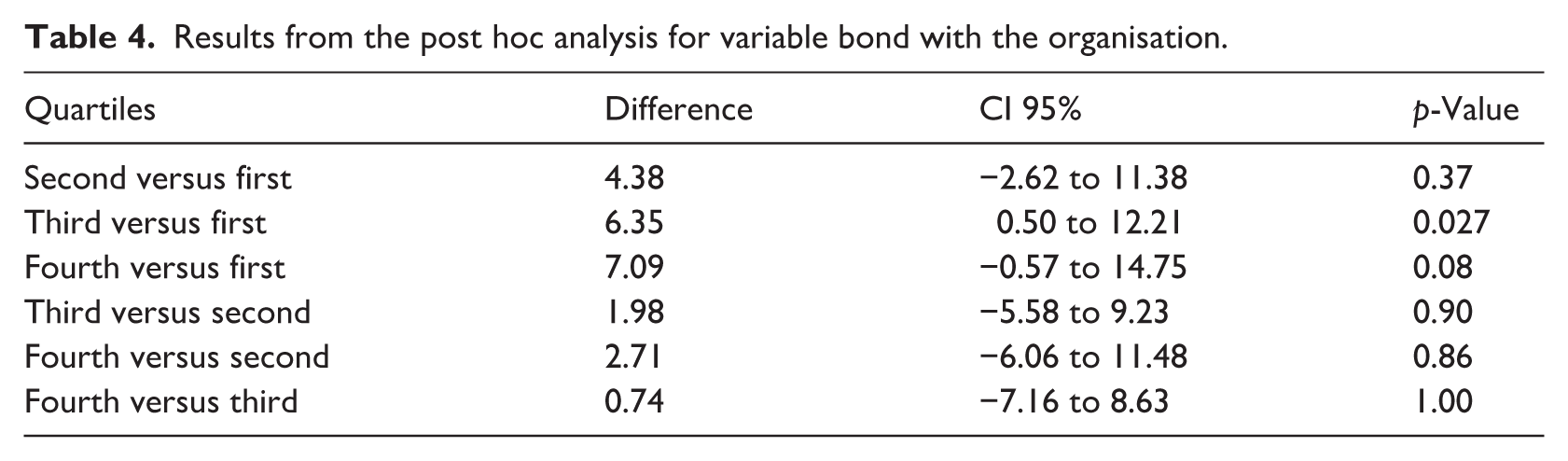
The IPNG overall score can be discriminated between groups according to their bond with the organisation (F3,536 = 3.412, p = 0.01734). The post hoc analysis in Table 4 indicates a significant difference between the first and the third quartiles. This means that on average, participants with higher self-reported bonds with the organisation also self-reported higher IPNG overall scores. The difference between the first and fourth quartiles underlines this tendency but nearly misses significance, which supports H5.
Results from the post hoc analysis for variable bond with the organisation.
Internal consistency reliability
The model showed high internal consistency reliability with α = 0.82 (CI 95%, 0.79–0.83). Cronbach’s alpha did not increase after dropping items (0.75–0.80). The subscales ranged from 0.82 to 0.93 as follows: 0.82 (Practice), 0.83 (Resources), 0.87 (Participation), 0.88 (Information), 0.91 (Goals), and 0.93 (Personnel).
Discussion
This study presents the translation, cultural adaptation, and psychometric evaluation of the German version of the IPNG. The results provide strong evidence for the construct validity and cross-cultural applicability of the instrument. CFA supported the proposed six-factor structure, demonstrating sound structural validity, with all latent constructs significantly loading onto their respective observed variables. Reliability analyses indicated satisfactory internal consistency, suggesting that the German IPNG performs comparably to the original English version.
Model fit indices further supported the validity of the German IPNG. Both the TLI and CFI exceeded the recommended cut-off value of 0.95, indicating an excellent model fit (Kline, 2023). The RMSEA and the SRMR slightly exceeded the commonly accepted threshold of less than 0.08 (Hu and Bentler, 1999; Schermelleh-Engel et al., 2003), but these values remain within an acceptable range for complex and multifactorial models. The complexity of the model, which includes 50 items distributed across six dimensions, along with the ordinal nature of the data, likely contributed to this result, as RMSEA is known to be sensitive to both sample size and model complexity (Kenny et al., 2015; Kyriazos, 2018b). The use of the WLSMV estimator, which is appropriate for ordinal data, ensured robust parameter estimation even under conditions of non-normality (Li, 2016).
The German version of the IPNG demonstrated strong internal consistency, reflecting high internal homogeneity and item reliability across the instrument (Cortina, 1993). These findings align with previous validations of the original English version (Hess, 1998; Lamoureux et al., 2014) and support the cross-cultural and linguistic robustness of the IPNG. Most standardised factor loadings exceeded 0.70, indicating strong relationships between the individual items and their corresponding latent constructs. However, several items within the Practice and Resources dimensions showed weaker factor loadings.
For example, the item ‘Determining what nurses can do at the bedside’ (Item 1) demonstrated the lowest loading (λ = 0.48). This may reflect the inherently complex and context-dependent nature of clinical decision-making, which is shaped by institutional regulations, interprofessional role delineations, and hierarchical governance structures (Bouchez et al., 2024; Essex et al., 2023). In such environments, nurses may perceive decision-making as externally constrained rather than as a collaborative process, limiting their sense of influence and participation in governance (Pursio et al., 2021). The concept of role clarity provides additional explanatory insight. When professional responsibilities and authority are ambiguously defined, nurses may struggle to position themselves within governance structures, resulting in uncertainty about their scope of practice (Machado et al., 2025). This lack of clarity can diminish perceived control and weaken alignment with the foundational principles of shared governance.
From a practical perspective, these findings highlight the importance of clearly defining clinical authority and decision-making roles. Strengthening role clarity, involving bedside nurses in policy development and establishing transparent governance processes may enhance perceptions of autonomy and foster deeper engagement in shared governance. These considerations are particularly relevant for supporting the cultural and organisational integration of professional nursing governance models within German-speaking healthcare contexts.
Similar patterns were observed for items such as ‘Making daily patient care assignments for nursing personnel’ (Item 9, λ = 0.52) and ‘Regulating the flow of patient admissions, transfers, and discharges’ (Item 10, λ = 0.50). These responsibilities are often viewed as administrative or routine, governed by institutional protocols and typically delegated to managerial personnel. Consequently, their relevance to shared governance may not be immediately apparent, which can reduce frontline nurses’ perceived influence within decision-making structures (Murray et al., 2018). This pattern suggests a potential disconnect between operational duties and their perceived contribution to participatory governance. When such tasks are experienced as externally mandated rather than as opportunities for influence, the associated items may not fully capture the intended governance constructs. These findings further inform the cultural adaptation process by identifying items whose meaning or salience may be contextually constrained. These findings emphasise the importance of clearly differentiating between operational, clinical and strategic domains within governance structures. Effective communication of these distinctions may help nurses recognise where their contributions are most impactful. Nurse leaders play a key role in framing routine duties as part of shared governance and engaging staff in policy development, thereby strengthening professional autonomy and ownership.
The weaker performance of some items also suggests a need for further refinement. Conceptual ambiguity, role overlap, or contextual variability may influence item interpretation. Mixed-methods research integrating qualitative interviews or focus groups can offer deeper insights into these discrepancies. Delphi processes with governance experts and frontline nurses may guide future item revision to enhance both cultural fit and empirical validity.
The known-groups validation results were partially consistent with the findings of Lamoureux et al. (2014) and Ghanem Atalla et al. (2023). No significant differences in IPNG scores were observed by sex, educational background, or clinical unit, supporting the structural validity and generalisability of the German version. However, significant differences emerged across age groups. Nurses in early and late career stages reported higher perceptions of shared governance compared to their mid-career counterparts. These findings are consistent with those of Ghanem Atalla et al. (2023), who identified stronger governance engagement and greater career motivation among early-career nurses. This pattern may reflect career-stage-specific differences in motivation, professional role, and organisational integration. Early-career nurses may actively seek involvement in decision-making as part of their professional development and desire for inclusion. In contrast, late-career nurses may benefit from accumulated experience, informal authority, and established roles, enabling greater autonomy and influence within governance structures. Mid-career nurses, however, often face increased clinical demands, supervisory responsibilities, and personal obligations outside of work. These overlapping pressures may reduce both their availability and perceived capacity to engage in shared governance initiatives (Ko et al., 2024).
These findings suggest that career stage is a relevant contextual factor in the design of participatory leadership strategies. Sustaining governance engagement across the professional lifespan requires targeted support, particularly for mid-career nurses. Practical approaches may include structured mentoring programmes, flexible participation models, and regular feedback mechanisms that facilitate meaningful involvement without adding to workload burden. Addressing this group’s specific needs may help strengthen professional identity, preserve institutional knowledge and promote leadership continuity in clinical nursing practice.
A significant association was also found between organisational commitment and IPNG scores. Nurses in the third quartile of commitment reported significantly higher perceptions of shared governance compared to those in the lowest quartile, while a similar trend in the highest quartile approached statistical significance. These results are consistent with empowerment theory, which posits that emotional commitment to the organisation enhances perceived influence, engagement, and participation in decision-making processes (Spreitzer, 1995). Psychological empowerment, as conceptualised by Spreitzer (1995), encompasses the dimensions of meaning, competence, self-determination, and impact. These elements are considered foundational for fostering professional engagement within governance structures. Empirical research supports this relationship, demonstrating that empowerment strengthens organisational commitment and increases nurses’ willingness to contribute to institutional objectives (Loes and Tobin, 2022). Recent findings further suggest that nurses who perceive governance structures as inclusive and supportive are more likely to exhibit strong organisational identification and higher levels of professional engagement (Loes and Tobin, 2022).
These findings point to a reciprocal relationship between structural empowerment and emotional attachment to the organisation. When governance frameworks are experienced as transparent, participatory, and aligned with professional values, they can strengthen morale, promote team cohesion and contribute to workforce stability, particularly in complex and high-pressure care environments.
Strengths and limitations
This study has several strengths. The translation and cross-cultural adaptation followed internationally recognised guidance and was strengthened by cognitive debriefing interviews, supporting linguistic accuracy and contextual relevance. The psychometric evaluation was conducted in a large and professionally diverse sample, enabling robust CFA and known-groups validation.
Several limitations should also be acknowledged. The study was conducted in a single university hospital in the German-speaking region of Switzerland, which may limit generalisability to other institutions, regions, or health systems with different governance structures or levels of implementation. The cross-sectional design precludes causal inference and does not allow assessment of changes in shared governance perceptions over time. Although the overall survey response rate was acceptable, completion of the full IPNG scale was lower, and partial completion and missing IPNG data may reflect response burden. This attrition may have introduced non-response bias if nurses with specific experiences of governance were more or less likely to complete the instrument. In addition, test–retest reliability was not assessed and temporal stability remains to be established. Organisational commitment (‘bond with the organisation’) was assessed by self-report and categorised into quartiles for analysis, which may reduce variability and be sensitive to contextual factors. Responses could not be stratified by hierarchical role (e.g. staff nurses versus nurse leaders), limiting insights into potential role-related differences in governance perceptions. Finally, the study focused exclusively on nurses, which limits conclusions regarding broader interprofessional governance models.
Implications
For nursing education, shared governance concepts and role clarity should be explicitly integrated into undergraduate and continuing education curricula to strengthen nurses’ competence and confidence in participatory decision-making. In clinical practice and leadership, routine assessment of shared governance using the German IPNG can help identify unit-level participation gaps and guide targeted strategies, particularly for mid-career nurses, including flexible participation models, mentoring, and transparent decision-making processes. At the health policy level, embedding shared governance indicators within workforce and quality frameworks may support autonomy-enhancing work environments and contribute to retention and sustainable staffing. For future research, multi-site and longitudinal studies should evaluate test–retest reliability, responsiveness to change following shared governance interventions and generalisability across settings. Mixed-methods studies and expert consensus approaches, such as Delphi panels, are recommended to refine items with weaker loadings and to explore applicability in interprofessional contexts. Given the instrument’s high internal consistency, future research should explore the potential for item reduction to improve feasibility and user engagement without compromising psychometric quality. Longitudinal and multi-site studies are recommended to assess the tool’s stability over time and its applicability across diverse healthcare environments. Expanding its application to interprofessional teams may also increase its relevance for evaluating collaborative decision-making processes in complex care settings.
Conclusion
This study translated, culturally adapted and psychometrically validated the German version of the IPNG, providing a reliable instrument for assessing shared governance perceptions among nurses in German-speaking healthcare settings. The results offer strong evidence for structural validity and internal consistency, with CFA supporting the original six-factor model and most items demonstrating robust loadings, consistent with prior validations of the English version.
Meaningful associations were identified between governance perceptions and contextual variables such as career stage and organisational commitment. Nurses in early and late career phases, as well as those with higher organisational commitment, reported more positive governance perceptions, aligning with theoretical models of professional empowerment. In contrast, some items within the Practice and Resources dimensions showed weaker psychometric performance, suggesting areas for further refinement and contextual clarification.
The validated German IPNG contributes meaningfully to nursing practice and research by providing a rigorously developed and culturally sensitive tool for evaluating participatory governance. Its use can support leadership development, strengthen professional autonomy, and guide strategic initiatives that promote inclusive and empowerment-oriented work environments.
In the context of workforce shortages and increasing care complexity, the IPNG may also serve as a diagnostic tool to identify governance-related challenges and inform the design of autonomy-enhancing interventions. Incorporating governance assessments into routine organisational evaluation processes can foster cultures of transparency, trust, and engagement- key conditions for sustaining team cohesion, staff retention, and high-quality nursing care.
Key points for policy, practice and research
The German version of the IPNG demonstrates strong structural validity and internal consistency, confirming its suitability for evaluating shared governance in German-speaking healthcare contexts.
Lower factor loadings in the Practice and Resources dimensions suggest the need for item refinement and conceptual clarification to improve contextual relevance and content validity.
Perceptions of shared governance varied by career stage and organisational commitment, underscoring the need for leadership strategies that are tailored to different phases of professional development and engagement.
The IPNG can be used as a practical diagnostic tool for nurse leaders and healthcare organisations to identify gaps in participatory governance, strengthen professional autonomy, and guide inclusive organisational development.
Future research should investigate item reduction, longitudinal stability, and interprofessional applications to enhance the instrument’s usability and adaptability across diverse healthcare settings and cultural contexts.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261428075 – Supplemental material for German version of the index of professional nursing governance: translation, cultural adaptation and psychometric validation
Supplemental material, sj-docx-1-jrn-10.1177_17449871261428075 for German version of the index of professional nursing governance: translation, cultural adaptation and psychometric validation by Fabienne Josefine Renggli, André Meichtry, Mirjam Meier, Paula Adomeit, Robert G. Hess and Christoph Golz in Journal of Research in Nursing
Footnotes
Acknowledgements
We are very grateful to all the nurses who participated in this study and generously shared their experiences and time.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Insel Group Ltd.
Data availability statement
The dataset used during the study is available from the corresponding author upon reasonable request.
Ethics Approval
Prior to the start of data collection, the president of the Swiss ethical review board in Bern deemed ethics approval unnecessary in accordance with the Swiss Federal Act on Research Involving Human Beings (HRA; SR 810.30, Art. 2), as no health-related data were collected and the survey component was conducted anonymously. This decision was certified and archived under reference number Req-2023-00673. The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent
Participation was voluntary. Survey participants received written information about the purpose and procedures of the study and provided informed consent by completing the first page of the questionnaire. No personally identifiable data were collected, and questionnaires were completed anonymously. For the cognitive debriefing interviews, participants were verbally informed about the study purpose and procedures (including audio-recording as a backup to field notes), confidentiality and their right to withdraw at any time. Verbal informed consent was obtained prior to each interview. Interview data were anonymised and stored securely.
Supplemental material
Supplemental material for this article is available online.