
Abstract
Background:
Patient satisfaction is vital in healthcare, influencing treatment adherence, health outcomes, occurrence of complications, and the likelihood of returning for care.
Aims:
This study aimed to assess the impact of the nursing workforce’s nationality diversity, years of service, and staffing levels on patient satisfaction in a tertiary hospital, in Saudi Arabia.
Methods:
A retrospective analysis was conducted, correlating patient satisfaction scores from Press Ganey® reports with nursing data from hospital manpower reports collected from 1 July 2019 to 30 June 2023. Descriptive statistics were used, with significance set at p ⩽ 0.05.
Results:
Pearson’s correlation coefficient yielded no relationship between: the nurses’ years of service versus mean patient satisfaction scores (r = −0.02, p = 0.695), nursing staff levels versus mean patient satisfaction scores (r = 0.04, p = 0.49; Figure 2) and number of nationalities in the care units versus mean patient satisfaction scores (r = −0.057, p = 0.27).
Conclusions:
These findings suggest that factors beyond nurse numbers, tenure, or nationality diversity might significantly influence patient satisfaction. Improving other aspects of care and addressing diverse patient needs can allow nursing to further enhance patient satisfaction, health outcomes, and the quality of nursing services provided.
Introduction
Patient satisfaction is a crucial aspect of healthcare delivery, and increasingly recognised as a core component of healthcare quality and performance evaluation (Liu et al., 2024). It refers to the patients’ perception of the care received during their healthcare experience, encompassing aspects such as communication, empathy, wait times, environment, and the effectiveness of care delivery (Almohaisen et al., 2023) and is typically measured using standardised, validated tools such as the Press Ganey® Patient Satisfaction Survey. This tool captures patient perspectives across key service areas including nursing, medical care, discharge processes, and overall hospital experience.
Whilst factors such as physician communication, hospital cleanliness, noise levels, and staff coordination have shown to have a significant influence on satisfaction scores, especially in tertiary care centres (Aiken et al., 2018; Almohaisen et al., 2023); nursing care has also been found to be a strong determinant of patient satisfaction (Aiken et al., 2018). In a recent study, Agostinho et al. (2023) stated that compared to other health professionals, nurses spend more time with hospitalised patients and interact with them more frequently, thus having a significant impact on the experience of hospitalisation. Therefore, adequate staffing levels and patient-to-nurse ratios become central in ensuring that patients receive optimal care, allowing nurses to divide their attention among patients, guaranteeing the time to address their needs effectively and efficiently (Aiken et al., 2018; Blume et al., 2021) and preventing adverse events such as mortality and morbidity (Sworn and Booth, 2019). Although recent studies generally support the impact of staffing levels on patient satisfaction, some variations exist. Some literature recognises that lower staffing levels are often a result of financial constraints or of healthcare policies that fail to mandate minimum staffing ratios (Lasater KB, 2024) and are the basis of increased patient dissatisfaction, longer response times and higher rates of adverse events (Blume et al., 2021; Hong and Cho, 2021). Others establish that higher nurse staffing levels are associated with better patient outcomes, including decreased mortality rates and shorter hospital stays (Dall’Ora et al., 2022; Peršolja, 2018), thus improving the patient’s experience and satisfaction (Kim et al., 2024). Delving into specific healthcare settings, Johnston et al. (2020) found that insufficient staffing in intensive care units (ICUs) directly contributes to increased adverse events, family dissatisfaction, and delayed responses to critical changes in patient conditions. In contrast, general medical or surgical wards typically manage more stable patients, and while adequate staffing remains important, the correlation between staffing levels and patient satisfaction is often moderated by other factors such as the quality of nurse–patient communication and staff responsiveness (Zhang et al., 2022). A recent multicentre study in China confirmed that while both settings benefit from higher staffing ratios, the magnitude of impact is significantly greater in ICUs, where the stakes for immediate, life-saving care are higher (Wang et al., 2021). Conversely, increased nursing staff levels and increased nurse–patient interaction time does not always translate to improved satisfaction. McHugh et al. (2016) challenged the literature claiming that the quality of these interactions can be adversely affected by the nurses’ burnout or heavy workloads, which can ultimately diminish a nurse’s ability to engage meaningfully with patients, thereby limiting the potential benefits of frequent contact (Dall’Ora et al., 2022).
Considering the previous statement, and as nurses migrate in search of better career opportunities and working conditions (World Health Organization [WHO], 2020), healthcare organisations became increasingly diverse (Osmancevic et al., 2023). As per the WHO (2020), one in eight nursing professionals are estimated to be presently working in a country different from where they were born or received their nursing training. Osmancevic et al. (2023) recognised that the impact of nursing nationality diversity on patient satisfaction is multifaceted, identifying cultural competence, language proficiency, and understanding of the local healthcare system as critical components that can impact the interactions between nurses and patients. Different expectations and experiences may occur when interacting with nurses from different cultural backgrounds. On one hand, nurses from varied backgrounds bring unique perspectives and insights into different cultural practices and beliefs, enabling them to provide care that is respectful and responsive to each individual patient’s preferences (Americal Association of Colleges of Nursing [AACN], 2023). It fosters stronger therapeutic relationships, leads to better adherence to care plans (Zhang et al., 2023), improves health literacy, and reduces patient anxiety (Shen et al., 2022). On the other, the nationality diversity might introduce communication challenges such as miscommunication between nurses and patients from diverse cultural backgrounds which can result in misunderstandings and suboptimal care, hindering the patients’ experience and satisfaction (Kline et al., 2021). Internationally, no consensus could be found in this regard. Although in countries such as the United States, United Kingdom, and Finland, the employment of a culturally and linguistically diverse nursing workforce introduced challenges in the ability of these nurses to provide care that meets the patients’ expectations, impacting the patients’ experience (AACN, 2023; Aiken et al., 2021; Kamau et al., 2023); in others such as Canada, this diversity helps sustaining service delivery and patient experience, by providing multilingual care to patients from various linguistic backgrounds, particularly for immigrant and minority populations (Covell and Neiterman, 2017).
Following the staffing levels and workforce nationality/cultural diversity, the nurses’ time with the healthcare organisation has also been shown to impact patient satisfaction. Across the healthcare arena, there might be the general assumption that nurses with longer tenures tend to have a better understanding of the organisation’s mission, vision, values, protocols, procedures, and patient population cared for. This familiarity with the patient’s needs and continued and consistent care enhances their ability to provide personalised care, resulting in increased patient satisfaction (Kwame and Petrucka, 2021). In one study, Guo et al. (2023) showed that patients reported higher satisfaction levels when nurses had more years of experience within the organisation, suggesting that familiarity and continuity of care play a significant role in patient satisfaction. The same author identified that nurses with longer tenure are more prone to build and develop good relationships with the patients they care for because of their deep knowledge and vast experience within the organisation. On the other hand, Kieft et al. (2014) claimed that, because of their short tenure, junior nurses in the organisation have too little experience to respond creatively to sometimes complex care situations. Thus, negatively affecting patients’ satisfaction.
The literature presented shows that the interplay between nursing staffing levels, staff nationality, and years in the organisation is a complex topic that has been shown to influence patients’ satisfaction. Adequate staffing levels are conducive to better patient outcomes, whereas culturally competent nurses contribute to improved patient communication and understanding. Moreover, nurses with longer tenures in the organisation tend to be better equipped to anticipate patient needs and provide comprehensive care that meets individual preferences, leading to higher levels of patient satisfaction.
Although preceding studies have examined the influence of individual factors such as the nursing staffing levels, years of service, or workforce diversity on patient satisfaction, few have simultaneously assessed the combined impact of these variables within a single healthcare setting, especially in the context of a multicultural and predominantly expatriate nursing workforce like that of Saudi Arabia. Additionally, most existing literature has focused on Western healthcare systems, with limited research exploring these dynamics in Middle Eastern or Gulf Cooperation Council (GCC) countries, where language barriers, cultural expectations, and workforce composition differ noticeably (Adhikari et al., 2021; Osmancevic et al., 2023). Furthermore, despite the increasing global attention to diversity and cultural competence, a lack of evidence regarding whether mere nationality diversity translates into improved patient satisfaction remains. This study addresses these gaps by analysing the correlations between nurse staffing levels, tenure, and nationality diversity and their influence on patient satisfaction scores over a four-year period in a large tertiary hospital in Saudi Arabia.
In addition, the beginning of 2020 set the whole globe a test. Healthcare systems, healthcare professionals worldwide, and nurses faced an inordinate health challenge: the Coronavirus Virus Disease 19 (COVID-19) pandemic (Arnetz et al., 2020). Despite the significant efforts to maintain the virus outside its borders, the Kingdom of Saudi Arabia was also affected by the pandemic. There were national-level general lockdowns and travel restrictions that hindered the mobility of the international nursing workforce (International Council of Nurses, 2020). This study’s data collection period will include the period pre-, during and post-COVID-19. The reason is to consider the potential effect, if any, of this global health crisis on the nationality mix of the nursing workforce in national healthcare organisations and, in turn, on the patient’s satisfaction with the nursing care received.
Methodology
Study design and setting
A retrospective study was designed to analyse and correlate the quantitative scores contained in the Press Ganey® Patient Satisfaction Reports and the Nursing staff information in the Hospital’s Human Resources Manpower Reports between 1 July 2019 and 30 June 2023, quarterly. This methodology was selected as the data had already been collected, reducing the need for involvement of participants and minimising ethical concerns related to data collection. In addition, it allows the collection and analysis of large amounts of data, throughout a lengthy period, which would be difficult to capture in a prospective study. Although retrospective studies offer logistical and ethical advantages, they have inherent limitations, including reliance on pre-existing data that may lack uniformity or completeness due to inconsistent documentation practices (Hassan et al., 2021). Researchers also have limited control over confounding variables, which can affect the accuracy of conclusions. In this study, temporal confounding is particularly relevant, as the period spans pre-, during- and post-COVID-19 phases, during which not only hospital policies and procedures affecting distancing measures, nurse–patient interactions, but also patient expectations, and workforce dynamics shifted – potentially influencing patient satisfaction independently of staffing levels or workforce composition (Kim et al., 2024; Wang et al., 2022). Recognising these factors is essential for accurate interpretation and generalisability of the findings.
Data sources
From the Press Ganey® Patient Satisfaction Reports, the authors obtained the patient satisfaction mean score with the category ‘Nurses’, which is comprised of seven sub-categories: ‘Friendliness/courtesy of nurses’, ‘Promptness response to call’, ‘Nurses attitude towards requests’, ‘Attention to needs’, ‘Skill of nurses’, ‘Nurse use language understand’ and ‘Extent to which nurses checked ID’.
From the Hospital’s Human Resources Manpower Reports, the number of employed nurses in the unit, the nurses’ average number of years of service in the organisation, and the number of different nationalities, all per included unit, were collected. All the information was de-identified to ensure the confidentiality and anonymity of the employees’ individual information. For this study and as per the Press Ganey® Patient Satisfaction Reports, Nursing Staff, Nursing Workforce or Nurses (used interchangeably) refers exclusively to Staff Nurses involved in direct patient care.
Sample size and sample selection
This study included all the hospital’s inpatient units, which were included in the Press Ganey® Patient Satisfaction Reports and all the staff nurses providing direct patient care in the units. The D4 – Medical/Surgical VIP (Very Important Person) Unit was excluded as VIP patients typically receive a level of personalised attention that can artificially inflate, dilute, or misrepresent care metrics and/or organisational benchmarks (Trzeciak et al., 2021). In addition, two other units were excluded due to the absence of collected survey data.
Statistical considerations
Descriptive statistics were used to summarise and describe the key features of the data. The Shapiro–Wilk test was used to test for normality of continuous data. Normally distributed data were presented as mean ± standard deviation, non-normal data as median (interquartile range [IQR]) and categorical data as numbers and percentages. ANOVA or chi-square tests were used to test between-group differences, and the Student’s t-test (for normally distributed data) or the Wilcoxon rank-sum test (for non-normal data) was used to compare continuous variables. Both univariable and multivariable linear regression models were fitted using STATA to understand the relationship between the explanatory factors and patient satisfaction. In the multivariable model, the authors used the backward elimination technique starting with predictors with the highest p-values until we arrived at a simpler, more interpretable model with fewer predictors. Nursing department is a categorical variable that was entered into the models as factor variable with Emergency Nursing or EMN as the base due to its lowest patient satisfaction mean score. A p-value <0.05 was considered statistically significant. Data analysis was performed using STATA, version 14.0 (StataCorp, College Station TX, USA).
The study occurred in a 1200-bed not-for-profit tertiary healthcare institution in Riyadh, Saudi Arabia, after its approval by the Hospital’s Research Ethics Committee (RAC# 2231452) dated 25 December 2023 and conducted according to the ethical principles of the 2013 Declaration of Helsinki.
Results
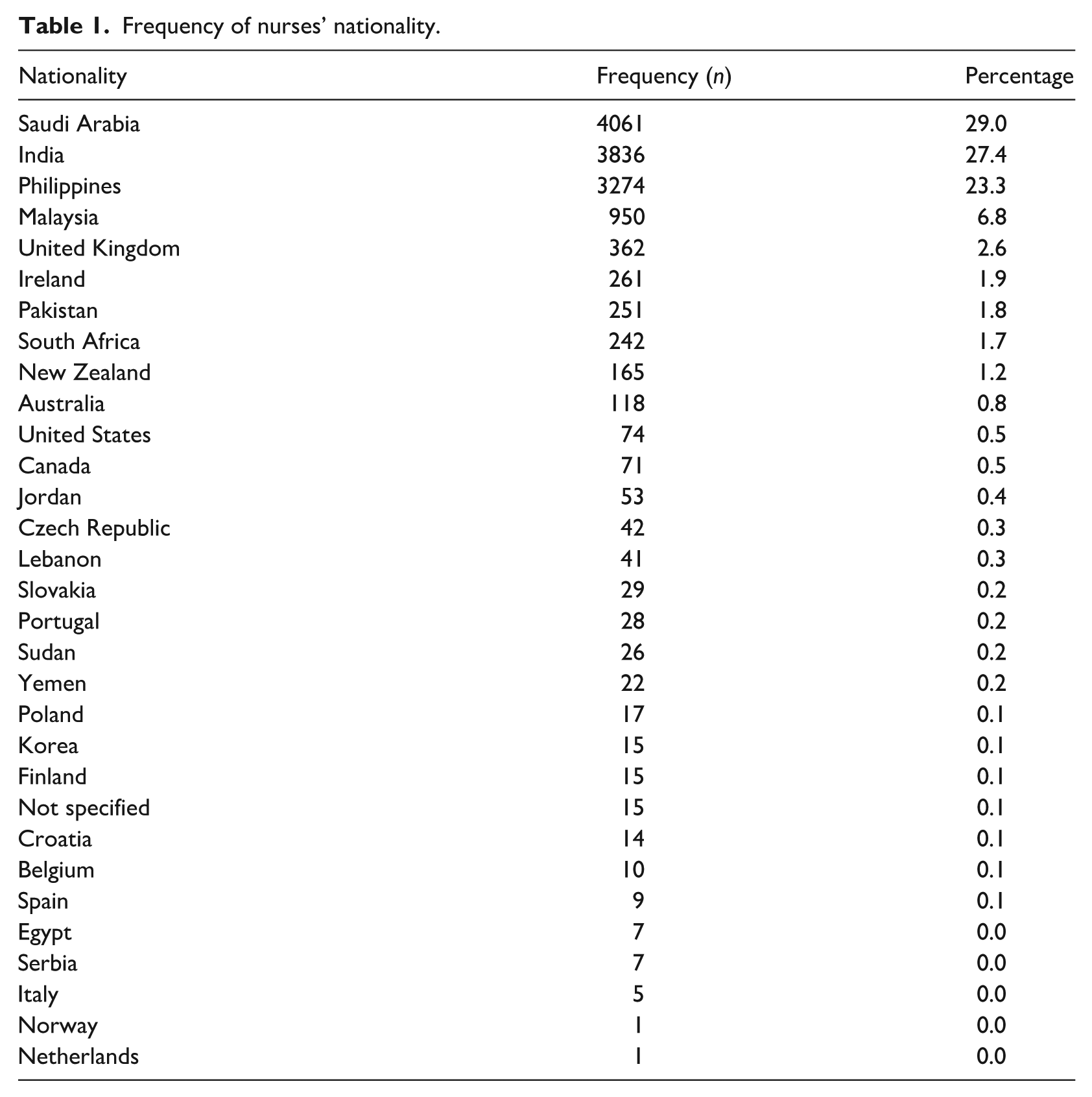
This study included 8 nursing departments that were made up of 31 nursing units. Three of these units were excluded due to lack of complete survey data. Overall, 14,022 nurses, representing 30 nationalities (Table 1), were employed by the study institution during the survey period. Nurses from India and the Philippines formed the largest proportion of the nursing workforce before the COVID-19 pandemic. However, since the pandemic in 2020, the nursing staff levels of Saudi nationals rose steadily every year across all eight nursing departments (Figure 1). Thus, between 2019 and 2023, nurses from Saudi Arabia accounted for 29% of the total number of nurses (n = 4061), followed by India (n = 3836; 27.4%) and the Philippines (n = 3274; 23.3%) (Table 1). Most of the international nurses did not speak Arabic (n = 9561; 68.2%). The number of nurses by department vary widely across the hospital: highest in Medical-Surgical Nursing or MSN (4461), lowest in Critical Care Nursing or CCN (129), with an average length of service of 5.8 years (SD: 1.67), ranging from 5 years (23.8%) to 7 years (20%).
Frequency of nurses’ nationality.
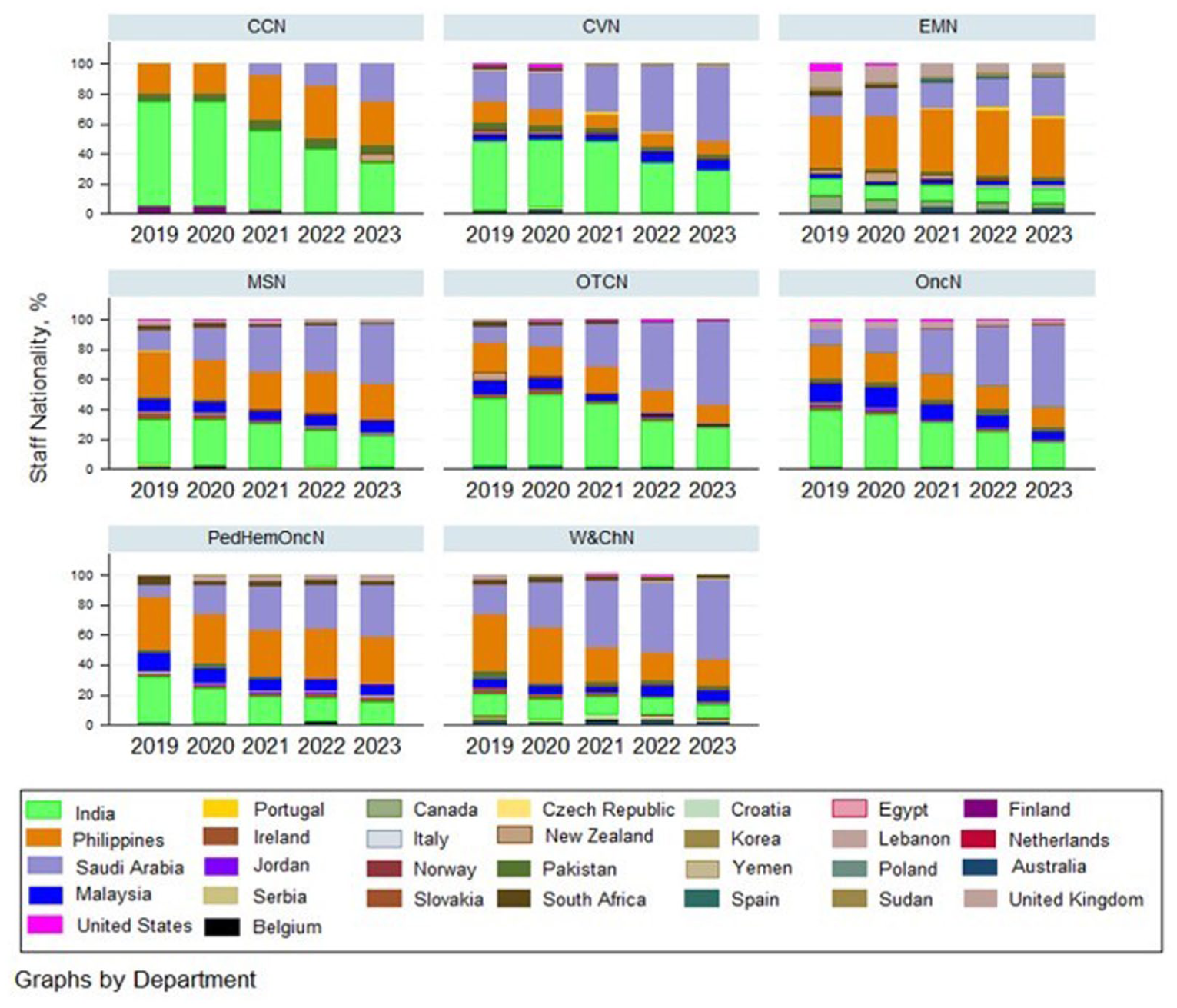
Staff nationality by Nursing Department (2019–2023).
Pearson’s correlation coefficient yielded no relationship between: the nurses’ years of service versus mean patient satisfaction scores (r = −0.02, p = 0.695), nursing staff levels versus mean patient satisfaction scores (r = 0.04, p = 0.49; Figure 2), and number of nationalities in the care units versus mean patient satisfaction scores (r = −0.057, p = 0.27). Furthermore, average patient satisfaction scores show a significant range (min–max) across departments, from 90.96 to 94.79. The highest mean satisfaction is CCN (94.79), being the nursing department with the least nursing staff levels (Table 2, Figure 3). The lowest patient satisfaction score was recorded in the Emergency Nursing department or EMN (90.96; Table 2).
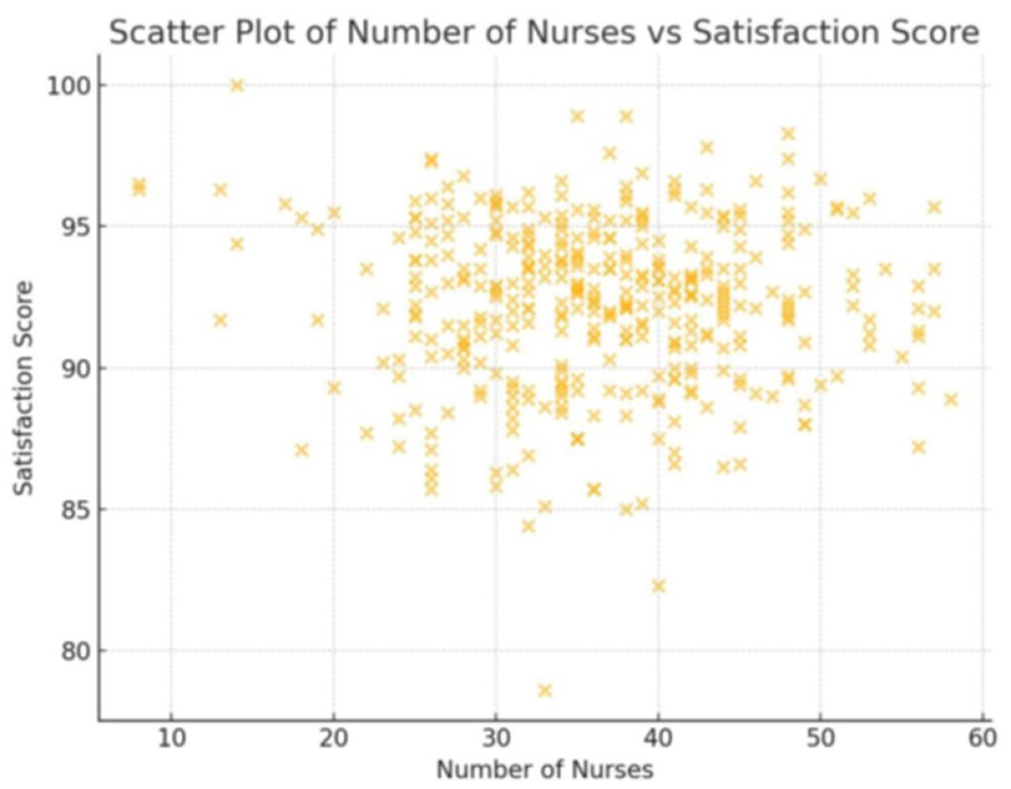
Two-way scatter plot of nursing staff levels versus mean patient satisfaction score.
Overall patient satisfaction mean score for the study period between 2019 and 2023, by clinical department.
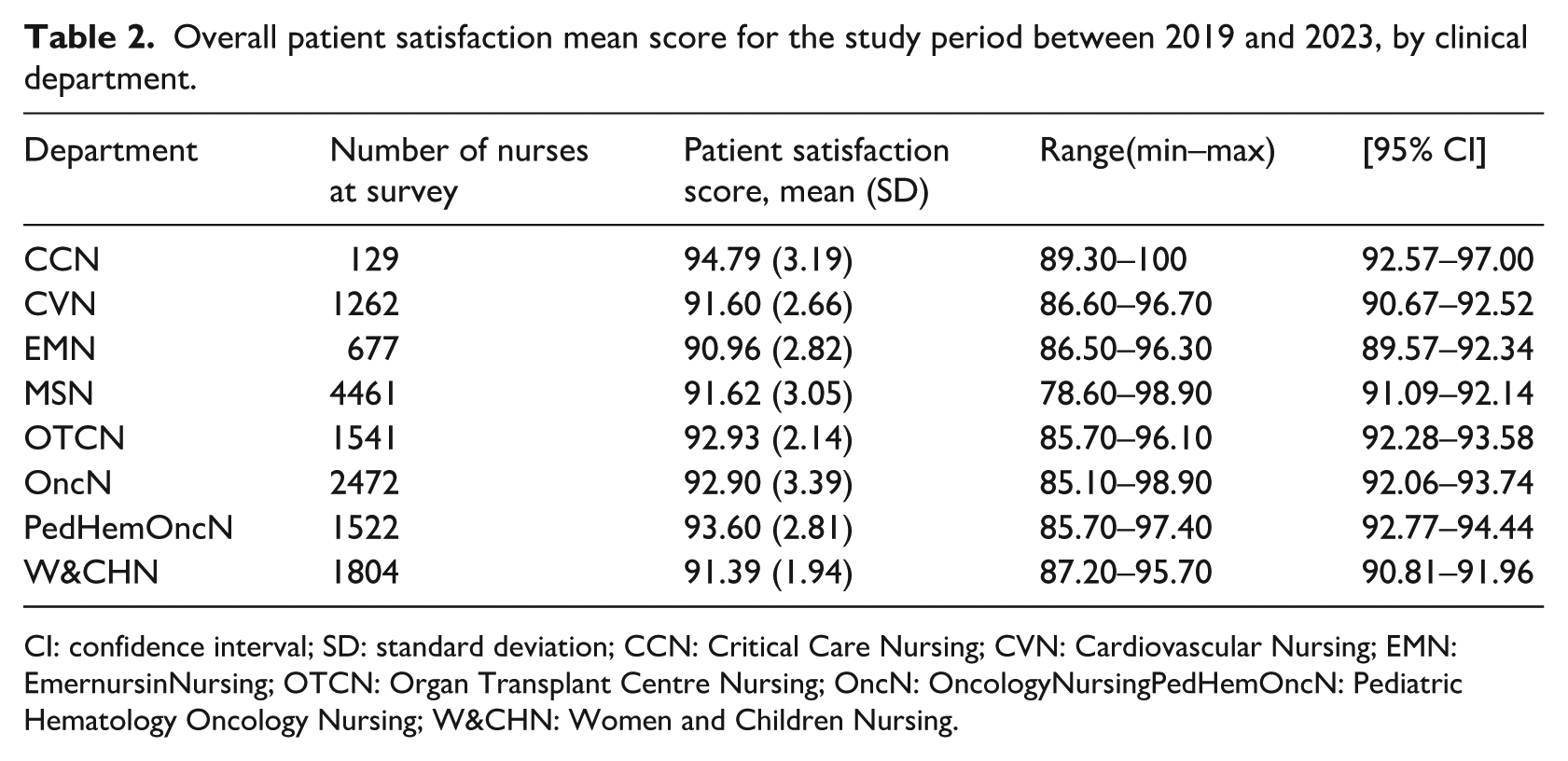
CI: confidence interval; SD: standard deviation; CCN: Critical Care Nursing; CVN: Cardiovascular Nursing; EMN: EmernursinNursing; OTCN: Organ Transplant Centre Nursing; OncN: OncologyNursingPedHemOncN: Pediatric Hematology Oncology Nursing; W&CHN: Women and Children Nursing.
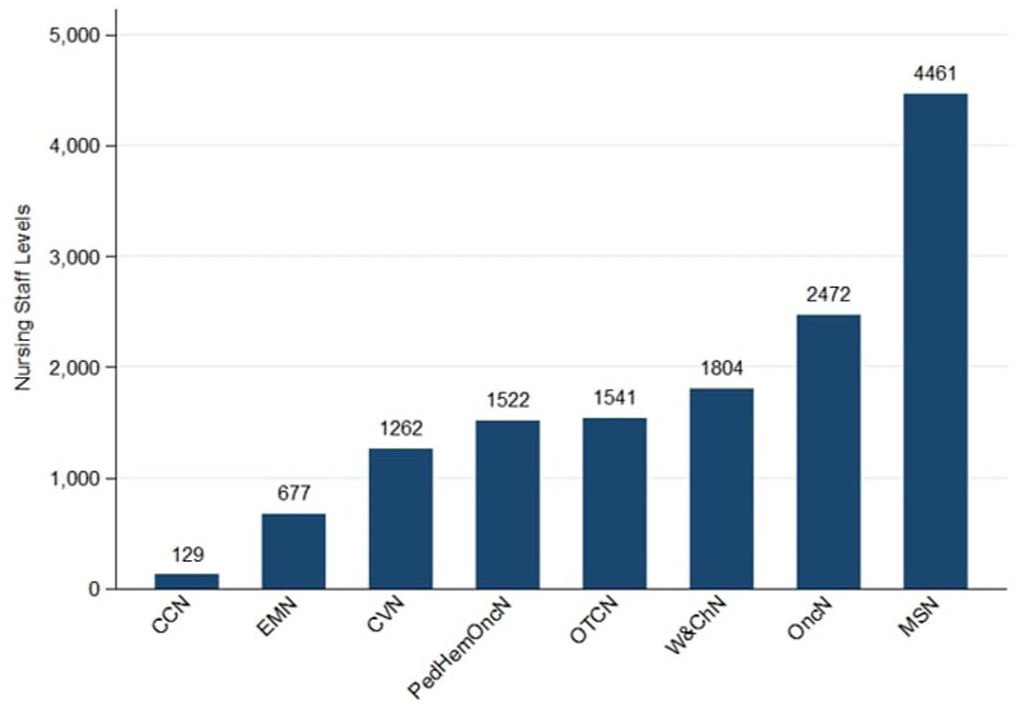
Nursing staff levels by Nursing Department (2019–2023).
Figure 4 displays quarterly variations in median patient satisfaction across the study institution between 2019 and 2023. One-way ANOVA showed significant differences in satisfaction across departments (F = 5.33, p < 0.0001). Bartlett’s test for homogeneity showed unequal variances across nursing departments (χ² = 21.2018, p = 0.003). Post-hoc test with Bonferroni comparison showed a significant difference in satisfaction scores between CCN and other departments, as it scored higher patient satisfaction being the department with the least nursing staff levels. Notable comparisons include CCN versus Cardiovascular Nursing or CVN (p = 0.135) and CCN versus Oncology Nursing or OncN (p = 0.034).
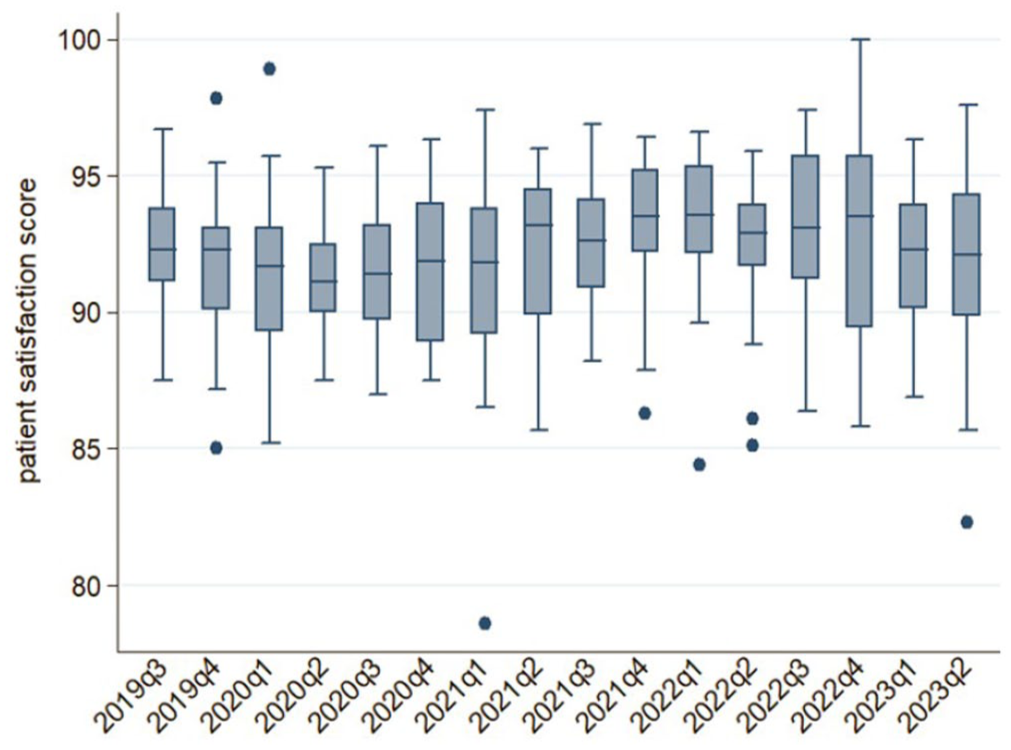
Trends in median patient satisfaction score by quarter (2019–2023).
Table 3 is the output of the univariable and multivariable linear models showing the relationship between the explanatory factors and patient satisfaction. At univariable level, the gradients on year of survey, the mean years of service, the number of nurses in a unit, and the number of nationalities in a department have weaker non-statistically significant effect on patient satisfaction. However, after adjusting for other independent factors in the multivariable model, a substantial, statistically significant positive gradients were observed from factor variables: CCN: 4.60 (p = 0.001), Organ Transplant Centre Nursing or OTCN: 2.54 (p = 0.008), OncN: 2.38 (p = 0.007) and Pediatric Hematology Oncology Nursing or PedHemOncN: 3.19 (p = 0.001). The gradients on year of survey and number of nationalities in a department did not reach statistical significance in the reduced model.
Univariable and multivariable linear regression model showing the impact of explanatory factors on patient satisfaction mean score.
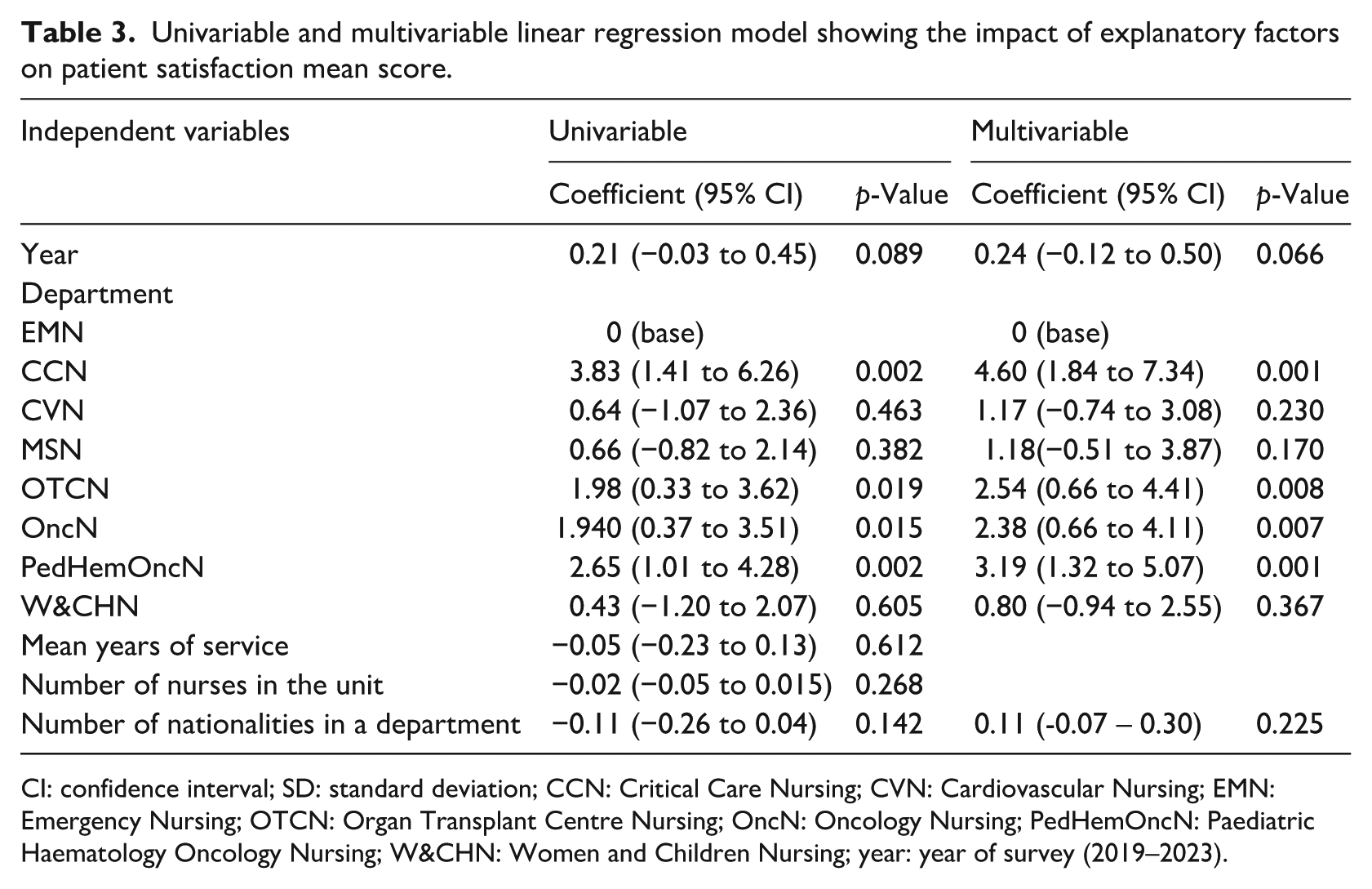
CI: confidence interval; SD: standard deviation; CCN: Critical Care Nursing; CVN: Cardiovascular Nursing; EMN: Emergency Nursing; OTCN: Organ Transplant Centre Nursing; OncN: Oncology Nursing; PedHemOncN: Paediatric Haematology Oncology Nursing; W&CHN: Women and Children Nursing; year: year of survey (2019–2023).
Discussion
This study sought to explore the relationships between nursing workforce characteristics, specifically, staffing levels, average years of service (tenure), and nationality diversity; and patient satisfaction with nursing care, as measured by the Press Ganey® Patient Satisfaction Survey, across multiple inpatient departments of a tertiary care hospital in Saudi Arabia over a 4-year period (2019–2023). By incorporating longitudinal data pre-, during- and post-COVID-19, the study aimed to offer a comprehensive understanding of how structural nursing variables intersect with patient experience in a culturally diverse and demanding complex healthcare environment. Given the increasing globalisation of the nursing workforce and the nuanced determinants of satisfaction in non-Western healthcare systems, this study sought understanding on a critical evidence gap.
Despite prevailing global evidence suggesting that higher nurse staffing levels, longer tenure, and cultural competence (frequently and generally inferred from nationality) positively influence patient satisfaction (Aiken et al., 2018; Guo et al., 2023; Kim et al., 2024), the results of this study revealed no statistically significant direct correlation between these variables and patient satisfaction at the institutional level. The Pearson correlation coefficients for staffing levels (r = 0.04, p = 0.49), tenure (r = −0.02, p = 0.695) and nationality diversity (r = −0.057, p = 0.27) all indicated weak, non-significant relationships. Similarly, the multiple linear regression model confirmed the absence of statistically meaningful associations between these predictors and satisfaction scores, with coefficients for tenure and staffing levels approaching zero, which suggest that other factors such as nurse responsiveness, attentiveness, and/or communication skills may be more influential.
These findings challenge much of the existing literature, which has long highlighted safe staffing ratios and workforce stability as key factors influencing patient-centred outcomes. For example, Peršolja (2018) and Blume et al. (2021) showed that higher staffing levels are linked to better patient outcomes and satisfaction. However, recent critiques argue that these benefits are not automatic and are often moderated by the quality of nurse–patient interactions and organisational culture (Dall’Ora et al., 2022; McHugh et al., 2016). This study’s findings support these more nuanced views by demonstrating that numerical metrics alone may not fully explain patients’ experiences in complex and culturally diverse healthcare settings. An interesting example is the CCN department, which, despite having the fewest nurses, recorded the highest mean patient satisfaction score (94.79), a result that contradicts expectations based on staffing levels alone. This department also showed statistically significant positive effects in the adjusted regression model (β = 4.60, p = 0.001). One possible explanation is the standardisation of lower patient-to-nurse ratios in the organisation’s ICUs, which may lead to greater nurse–patient engagement and increased attentiveness and responsiveness. It is also important to recognise that patients may hold different expectations or exhibit gratitude biases in these settings, where life-saving interventions and emotional support are more visible and deeply valued. Additionally, the COVID-19 pandemic may have subtly shaped patient expectations. The resilience and prominence of nursing during the pandemic may have enhanced public perceptions and patient trust in nursing care, regardless of objective staffing figures or the mix of nationalities.
Although employing nurses from over 30 nationalities, including a notable increase in Saudi nationals after COVID-19, the number of different nationalities per unit did not significantly affect satisfaction scores (r = −0.057, p = 0.27). This aligns with Covell and Neiterman (2021), who indicated that cultural and linguistic diversity alone does not predict satisfaction unless paired with effective communication skills and intercultural training. This finding challenges the literature that states that diverse teams, where members bring different perspectives to the care plan, may lead to better problem-solving and decision-making, ultimately improving patient outcomes and satisfaction (Khuntia et al., 2022). Interestingly, although 68.2% of the nurses in this setting were non-Arabic-speaking, satisfaction remained high in several departments. Potential explanations for this outcome include the availability of interpreter services in some care areas as well as of a promoted supportive and collaborative team dynamics and culture, which frequently allowed Arabic-speaking nurses to help and provide translation for the non-Arabic speaking colleagues, overcoming existing communication barriers.
Similarly, the lack of a statistically significant correlation between nurses’ average years of service and patient satisfaction (r = –0.02, p = 0.695) contradicts expectations that longer-tenured nurses, through deeper institutional knowledge and greater familiarity with patients and protocols, provide superior care (Guo et al., 2023; Kwame and Petrucka, 2021). A possible explanation is that institutional tenure alone may not lead to higher engagement or quality, but rather be moderated by workforce satisfaction or well-being, particularly if longer-serving nurses experience burnout, stagnation, or disengagement. Conversely, Kieft et al. (2014) warned that junior nurses with limited experience might lack the confidence and creativity needed for complex care situations. These mixed signals highlight the need for further exploration into the qualitative aspects of tenure, including the nurses’ job satisfaction, and engagement and health status.
Strengths and limitations
This study demonstrates several significant strengths. It was conducted in a large, accredited tertiary hospital, enhancing the clinical relevance and contextual specificity of the findings. The use of routinely collected administrative and patient satisfaction data ensures ecological validity and reflects real-world healthcare dynamics. A key strength lies in the extensive human resources dataset, which includes a large sample size and enables triangulation across three critical workforce dimensions: nursing staffing levels, years of service, and nationality diversity. This multidimensional approach provides a more comprehensive understanding of the workforce structure and its potential impact on care delivery. Furthermore, the analysis spans multiple years, capturing trends across pre-, during and post-COVID-19 periods, offering valuable insights into temporal shifts in healthcare delivery.
Despite its strengths, the study presents some limitations. The retrospective approach restricts control over confounding variables and depends on the completeness and consistency of existing data, which may vary across different time points, particularly during the COVID-19 period. This pandemic phase introduced unique dynamics, such as a temporary elevation in the perceived value of nursing and reduced geographical mobility among nurses due to travel restrictions and workforce stabilisation efforts. These factors may have influenced staffing patterns and patient perceptions in ways that are not generalisable to non-pandemic conditions.
Although the analysis focused on staffing levels, years of service and nationality diversity, it did not account for important mediators such as patient acuity, nurse–patient ratios, burnout, or communication quality, all of which can significantly affect patient satisfaction.
Satisfaction was measured using a single domain from the Press Ganey® survey without additional validation. Even though this single domain is inclusive of seven subcategories, which reflect patient-facing aspects of nursing care, the study did not confirm whether these items exclusively capture satisfaction with nursing care. It also did not assess whether other elements in the broader patient experience such as physician interaction or environmental factors may have influenced perceptions. Previous research has emphasised the multifactorial nature of satisfaction surveys and cautioned against interpreting them in isolation without controlling for confounders (Kim et al., 2024).
Although the structural variables assessed (the number of employed nurses, the years of service, and nationality diversity) are important indicators of workforce structure, other influential factors such as the nurses’ job satisfaction levels, the nurses’ education levels, the workload intensity, and patient acuity were not measured. These aspects have been shown to significantly affect both nurse performance and patient satisfaction outcomes (Dall’Ora et al., 2022; Guo et al., 2023).
Nationality was used as a proxy for diversity and cultural competence, without evaluating language proficiency, intercultural communication skill, or the use of official or established interpreter services. Language classification was binary (Arabic vs non-Arabic), based on the country of origin, which fails to account for variations in fluency or communication effectiveness.
The findings reflect a single-centre, expatriate-dominant hospital in Saudi Arabia, which may limit the generalisability of the results to other healthcare systems.
Future studies are recommended to incorporate a broader range of structural and process-based indicators. Specifically, investigating nurses’ Professional Quality of Life (ProQoL) (Stamm 2010) could provide deeper insight into how continuous understaffing, compassion fatigue, and burnout affect care delivery and patient experience. This line of inquiry may offer critical understanding of how workforce well-being shapes patient satisfaction and overall care outcomes.
Conclusion
This study offers a nuanced, context-sensitive analysis of the relationship between nursing workforce characteristics and patient satisfaction within a culturally diverse, high-volume tertiary care environment. Although traditional variables such as staffing levels, tenure, and nationality diversity did not significantly predict satisfaction, the consistent excellence observed in certain departments points towards qualitative and contextual determinants of patient-centred care such as interpersonal communication, perceived empathy, continuity of care, and cultural sensitivity. These elements can be difficult to quantify but are essential to shaping the patient’s experience.
In an era where healthcare is increasingly measured, standardised, and optimised, this research urges caution against over-reliance on structural metrics as proxies for care quality. Instead, it advocates for a human-centred approach, where the relational, communicative, and organisational culture dimensions of nursing are prioritised as key levers in delivering exceptional patient experiences in an increasingly globalised workforce landscape. The authors are mindful that the study may indicate that the art of nursing often remains constant within the constraints of practice, enabling high levels of patient satisfaction despite the varied contextual demands placed on nurses. However, it is essential to consider the impact this has on nurses themselves and the wider workforce, particularly in relation to mental well-being, burnout, and staff attrition.
Key points for policy, practice and research
The lack of correlation between nurse staffing levels and patient satisfaction suggests that simply increasing staffing may not directly enhance patient experiences. Nurses often maintain high standards of care despite low staffing, which may come at the cost of their own ProQoL, warranting further research in this area. Importantly, safe nurse-to-patient ratios should not be viewed solely through the lens of patient satisfaction, but as critical to reducing morbidity and mortality and ensuring both patient and staff well-being.
The weak correlation between nurses’ years of service and patient satisfaction suggests that experience alone is not a decisive factor in patient outcomes. Instead, it may highlight the importance of core skills, such as communication, empathy, and patient engagement, which remain essential regardless of length of service. The absence of a relationship between the number of nationalities in care units and patient satisfaction suggests that diversity in staffing does not automatically improve satisfaction, emphasising the need for policies that target cultural competence training rather than simply increasing staff diversity.
The lack of significant difference in patient satisfaction between Arabic-speaking and non-Arabic-speaking nurses suggests that language alone does not drive patient satisfaction, but rather how well nurses can engage and communicate with patients in a culturally sensitive manner. The use of unofficial translation delivered by fellow nurses, native Arabic speakers, might have contributed to this finding.
These findings call for future research to explore other factors influencing patient satisfaction, such as nurse–patient communication, care quality organisational support and policy adequacy and to investigate how the nurses’ job satisfaction/ProQoL, their cultural competence and emotional intelligence may impact patient outcomes more than demographic variables.
Footnotes
Acknowledgements
The author would like to acknowledge Dr Gamal Mohamed, Fatimah Alharthi from the Department of Biostatistics, Epidemiology and Scientific Computing and Ghassan Abudari from the Nursing Cancer Center of Excellence – King Faisal Specialist Hospital and Research Center-Riyadh for their valuable input in the data analysis process for this study.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research received ethics clearance from the Institutional Board Review of the King Faisal Specialist Hospital and Research Center-Riyadh, Saudi Arabia (Reference #2231452). A waiver for informed consent was granted.