
Abstract
Aim
This paper reports on a quasi-experimental, longitudinal study on the effects of working in a new type of dementia care facility (i.e. small-scale living facilities) on staff burnout symptoms and job characteristics (job autonomy, social support, physical demands and workload).
Methods
It is hypothesised that nursing staff working in small-scale facilities experience fewer burnout symptoms, more autonomy and social support, and fewer symptoms of physical demands and workload compared with staff in regular wards. Two types of long-term institutional nursing care settings were included: 28 houses in small-scale living facilities and 21 regular psychogeriatric wards in nursing homes. At baseline and at follow-ups after 6 and 12 months nursing staff were assessed by means of self-report questionnaires. In total, 305 nursing staff members were included in the study, 114 working in small-scale living facilities (intervention group) and 191 in regular wards (control group).
Results
No overall effects on burnout symptoms were detected. Significantly fewer physical demands and lower workload were experienced by staff working in small-scale living facilities compared with staff in regular wards. They also experienced more job autonomy. No significant effect was found for overall social support in the total group.
Conclusions
This study suggests positive effects of the work environment on several work characteristics. Organisational climate differs in the two conditions, which might account for our results. This may influence nursing staff well-being and has important implications for nursing home managers and policy makers. Future studies should enhance our understanding of the influence of job characteristics on outcomes.
Introduction
Long-term institutional nursing home care for people with dementia is shifting in terms of philosophy and practice from a medically-oriented care environment towards a resident-centred, individualised care environment (White-Chu et al., 2009). The worldwide trend towards deinstitutionalisation fits within this shift. When the dementia progresses and care demands increase, admission to a long-term care facility often becomes inevitable. In the Netherlands, long-term psychogeriatric care is increasingly organised in small-scale living facilities (Verbeek et al., 2009b), and as many as a quarter of the people with dementia live in small-scale facilities (Te Boekhorst et al., 2007; Wimo and Morthenson Ekelof, 2004).
These facilities emphasise the importance of well-being and differ from regular wards with respect to physical, social and organisational characteristics (Ausserhofer et al., 2016; Verbeek et al., 2009b). Small-scale living facilities aim to offer a homelike environment to a small number of 8–10 residents per group. Small-scale living facilities focus strongly on normal daily life. Residents are encouraged to participate in meaningful activities that are often centred around the daily household (e.g. washing and folding clothes, cooking and cleaning) within a homelike environment. The daily life is determined together by residents, their family caregivers and nursing staff. This is opposed to traditional large nursing homes, in which routines dominate the daily lives of the nursing home residents and which often have an institutionalised hospitalised character (Verbeek et al., 2009b).
Incentives and increased awareness of older persons' needs has supported the worldwide development of these new care settings (Annerstedt, 1993; Eliopoulos, 2010; Kane et al. 2007). The fact that healthcare policy needs to be evidence-based has received worldwide attention and support (Niessen et al., 2000). However, small-scale living facilities were one of the developments implemented with little convincing scientific evidence.
Nursing staff employed in small-scale living facilities have different roles and tasks compared with staff employed in more traditional facilities. Overall, staff working in small-scale living facilities incline more towards integrated care: nursing staff members are part of the household and have integrated tasks, including personal and medical care, organising activities and daily household chores (Kane et al., 2007; Te Boekhorst et al., 2007; Verbeek et al., 2009b). Studies indicate that this may affect job characteristics such as autonomy, social support, workload and demands (Adams et al., 2017; Willemse et al., 2014). For example, in small-scale living facilities daily nursing activities are characterised by working all-round and independently, whereas nursing staff in traditional wards collaborate with each other and have differentiated tasks. Autonomy and social skills specifically were regarded as important by nursing staff working in small-scale living facilities in comparison with traditional nursing homes (Adams et al., 2017).
Despite the increase of small-scale facilities, relatively little is known about the effects of work environments on nursing staff well-being (such as job stress) and job characteristics (Ausserhofer et al., 2016). The few studies that have focused on staff well-being in small-scale living in comparison with regular wards (Alfredson and Annerstedt, 1994; Reggentin and Dettbarn-Reggentin, 2004; Te Boekhorst et al., 2008) showed that working in small-scale living facilities may offer nursing staff attractive work and a favourable work environment (Vermeerbergen et al., 2017). Although most of the studies showed some positive effects on job characteristics, like autonomy and workload, study findings on burnout symptoms were inconsistent. Methodological flaws (i.e. cross-sectional designs) complicate the interpretation of findings.
It is important to be aware of the impact of the staff work environment and how this influences nursing job stress and care for residents (Norbergh et al., 2002). Environmental and organisational aspects have been reported as being important in relation to burnout (Benjamin and Spectator, 1990) and the provision of person-centred care (Willemse et al., 2015). In turn, low levels of burnout and work environment attributes impact on quality of care (Aström et al., 1991; Temkin-Greener et al., 2010). Furthermore, there is growing evidence that residents' quality of life is positively related to non-patient-related factors such as organisational climate (Mattiasson and Andersson, 1995) and nursing staff job characteristics (Chou et al., 2002; Edvardsson et al., 2008; Rosen et al., 2005). Positive associations between the non-institutional environment and staff morale were mentioned by Parker et al. (2004).
The research question of the present study is: What is the effect of working in small-scale living facilities on staff burnout symptoms and various job characteristics (job autonomy, social support, physical demands and workload)? These job characteristics were selected since they are mentioned by many theoretical models of stress as important factors in relation to outcomes such as nurses' job satisfaction and burnout (Karasek, 1985; Kovner et al., 2006).
Methodology
Design
A longitudinal, quasi-experimental study was carried out which compared two types of long-term institutional nursing care settings for people with dementia: small-scale living facilities and regular psychogeriatric wards. The design is described in more detail elsewhere (Verbeek et al., 2009a).
Specifications of the setting
Nursing home care in the Netherlands
Nursing home care in the Netherlands is provided in dementia-specific wards. The wards can differ in size from small-scale wards (up to 10 residents) to more traditional large-scale wards with up to 30 residents (Verbeek et al., 2009b). Nursing homes in the Netherlands are in general part of non-profit care organisations (Bos et al., 2017). About 350 organisations provide nursing home care in the Netherlands for a total of 129,000 residents (Actiz, 2017). Care provided in nursing homes requires a multidisciplinary approach given the severe care dependency of residents (Verbeek et al., 2009b). Therefore, a multidisciplinary team is employed consisting of nursing staff and allied health professionals such as physiotherapists, psychologists, occupational therapists, dietitians, speech therapists and nursing home physicians (Verbeek et al., 2009b). Residents' families and volunteers are involved in the nursing home care provided.
The two nursing home conditions
All nursing homes that offered small-scale living and were located in the southern part of the Netherlands were eligible to participate in the current study. Managing directors received a written invitation to participate.
In the experimental condition, 28 houses in small-scale living facilities were characterised by the following criteria (Verbeek et al., 2009a):
There is a maximum of eight residents per house or unit. Staff, residents and their family form a household together and activities are centred around the daily life and household. Staff perform domestic tasks and prepare meals together with residents and/or their family caregivers. Staff perform integrated tasks, which means that one person may fulfil multiple tasks such as medical and personal care, domestic chores and activities. Residents are cared for by a small, fixed team of nursing staff. Daily life is organised completely or to a large extent by residents, their family caregivers and nursing staff. The archetypal home is a physical setting that resembles a homelike environment.
In the control condition, 21 regular nursing home wards were characterised by the following criteria:
There was a minimum of 20 residents per ward. Staff members have differentiated tasks with a main focus on medical and personal care for residents. Residents and their family members have little control over the organisation of daily life within the ward as it is mainly organised around the routines of the nursing home.
Participants
Nursing education in the Netherlands is divided into five levels: basic nursing aids (level 1), nursing assistant (level 2), certified nursing assistant (level 3), and registered nurses vocational (level 4) and Bachelor (level 5). All nursing staff (i.e. nursing aids, nursing assistants, certified nursing assistants and registered nurses) directly involved in care tasks and working on a permanent basis in either the selected small-scale living facilities or regular psychogeriatric wards were eligible to participate in the study. Temporary staff (such as trainees), permanent night-shift workers and team managers were excluded from the study as they are known to experience different levels of job stress (Ferri et al., 2016). The total number of eligible staff at baseline was 581; 178 in small-scale living and 403 in regular wards.
Measures and outcomes
The current study addresses the findings on secondary outcomes including burnout symptoms as an outcome of job stress and job characteristics (job autonomy, social support, workload and physical demands). The findings concerning the primary outcomes are reported elsewhere (Verbeek et al., 2010a). Data on nursing staff were gathered at baseline (T1), and after 6 months (T2) and 12 months of follow-up (T3) by means of self-report questionnaires.
Burnout symptoms
Burnout symptoms as an outcome of job stress were measured by a five-item self-reported questionnaire (De Jonge, 1995). Previous studies determined its validity, reliability and internal consistency (De Jonge, 1995; De Jonge et al., 1993). Current analyses confirmed good internal consistency (Cronbach's alpha = 0.89). Items ranged from ‘never’ to ‘always’ on a seven-point Likert scale. The total score ranged theoretically from 5 to 35. Higher scores indicated more burnout symptoms. A sample item is: ‘I feel burned-out by my job.’
Job characteristics
Job characteristics (job autonomy, social support, workload and physical demands) were measured by a self-reported questionnaire. Previous studies determined its validity, reliability and internal consistency (De Jonge, 1995; De Jonge et al., 1993). Current study findings confirmed good internal consistency.
Job autonomy was assessed by the Maastricht Autonomy Questionnaire (MAQ) (De Jonge, 1995), which consists of 10 items scored on a five-point Likert scale ranging from very little to very much. Its total score ranges from 10 to 50. Higher scores indicate more job autonomy. The questionnaire includes information on job control and freedom in work tasks and methods. It measures the opportunity for staff to determine a variety of task elements, such as the pace of work and the work goals. A sample item is: ‘My work offers me the opportunity to interrupt my job whenever I want.’ Current study findings confirmed good internal consistency (Cronbach's alpha = 0.90).
Workplace social support was measured by the eight-item scale from the Job Content Questionnaire (De Jonge et al., 2000; Karasek, 1985). The questionnaire inventories work-related social support, both instrumental and emotional, from colleagues and supervisors. One subscale of four items refers to support from colleagues, whereas the other subscale of four items refers to support by supervisors. It uses a four-point Likert scale with items ranging from ‘completely disagree’ to ‘completely agree’. The total score ranges from 8 to 32 and a higher score represents more social support. A sample item is: ‘My colleagues help get the work done.’ Current study findings confirmed good internal consistency of the total scale (Cronbach's alpha = 0.81) and both subscales (Cronbach's alpha, both subscales = 0.85).
Workload (psychological demands) was measured by an eight-item scale that includes qualitative and quantitative demanding aspects such as working under time pressure, strenuous work and job complexity (De Jonge, 1995). Items range from ‘never’ to ‘always’ on a five-point Likert scale. Total scores range from 8 to 40, with higher scores indicating more symptoms of workload. A sample item is: ‘In the unit where I work, work is too complex.’ Current study findings confirmed good internal consistency (Cronbach's alpha = 0.91).
Physical demands were assessed by a seven-item questionnaire ranging from ‘never’ to ‘always’ on a 5-point Likert scale (De Jonge et al., 1999). A total score is calculated and ranges from 7 to 35, with higher scores representing more physical demands. Items refer to heavy physical demands like standing and carrying heavy weights. A sample item is: ‘In my work, I have to bend forward with my upper body.’ Current study findings confirmed good internal consistency (Cronbach's alpha = 0.87).
In addition, the following background variables were assessed: age, gender, education level, months of employment in facility type, years working in elderly care and contract hours per week.
Small-scale environmental characteristics
A self-developed contrast questionnaire (small-scaled characteristics questionnaire) was used to measure typical environmental characteristics in both the experimental and the control group about the small-scaledness of the facility to see whether the two environments demonstrated enough differentiation. This questionnaire consists of 18 items (scoring range 18–90) that relate to a small-scale unit's organisational, social and physical environment. Higher scores indicate greater adherence to the criteria of small-scale living facilities. A sample item is: ‘To what extent are staff and family members part of the household?’
Procedure
An information leaflet about the study (content and process) including an invitation letter was distributed by the researcher (HV) to all nursing staff of the included wards. The study was further explained during a regular team meeting by the researcher. Nursing staff indicating that they would like to take part were screened for eligibility (not working night shifts or temporarily or as a team manager). Eligible staff were then invited to provide written informed consent before receiving the questionnaire. After 2 weeks a reminder was sent by mail to those who did not respond initially. To guarantee confidentiality, nursing staff returned the questionnaires directly to the researchers using a pre-stamped envelope.
Ethical considerations
The Medical Ethics Committee (MEC) of the University Hospital Maastricht/Maastricht University approved the study (reference number MEC 07-4-041). In addition, all local ethical committees of the participating facilities and the managing directors of the regular nursing homes and small-scale living facilities approved of and provided consent for the study.
Statistical analysis
All statistical analyses were conducted using Predictive Analytics SoftWare (PASW) version 17 from SPSS. Differences in characteristics between the two groups at baseline were tested with χ2-tests for categorical variables, individual sample t-tests for normally distributed continuous variables, and Kruskal–Wallis tests for continuous variables with skewed distributions. A mixed-model multi-level analysis was performed, according to the intention-to-treat principle. All nursing staff with a baseline measurement were included in the analyses, regardless of availability of data at follow-up, since multi-level analyses are robust for missing values in the outcome variables.
All selected background characteristics of participants were included as covariates in the model. Missing data for only these covariates were imputed by multiple imputation. First, fixed effects for group by time interaction were tested for significance. If this interaction was not significant, it was removed from the model and only fixed effects for group and time were tested. All tests used a two-sided significance level of 0.05.
Results
Sample
Characteristics of nursing staff participants.
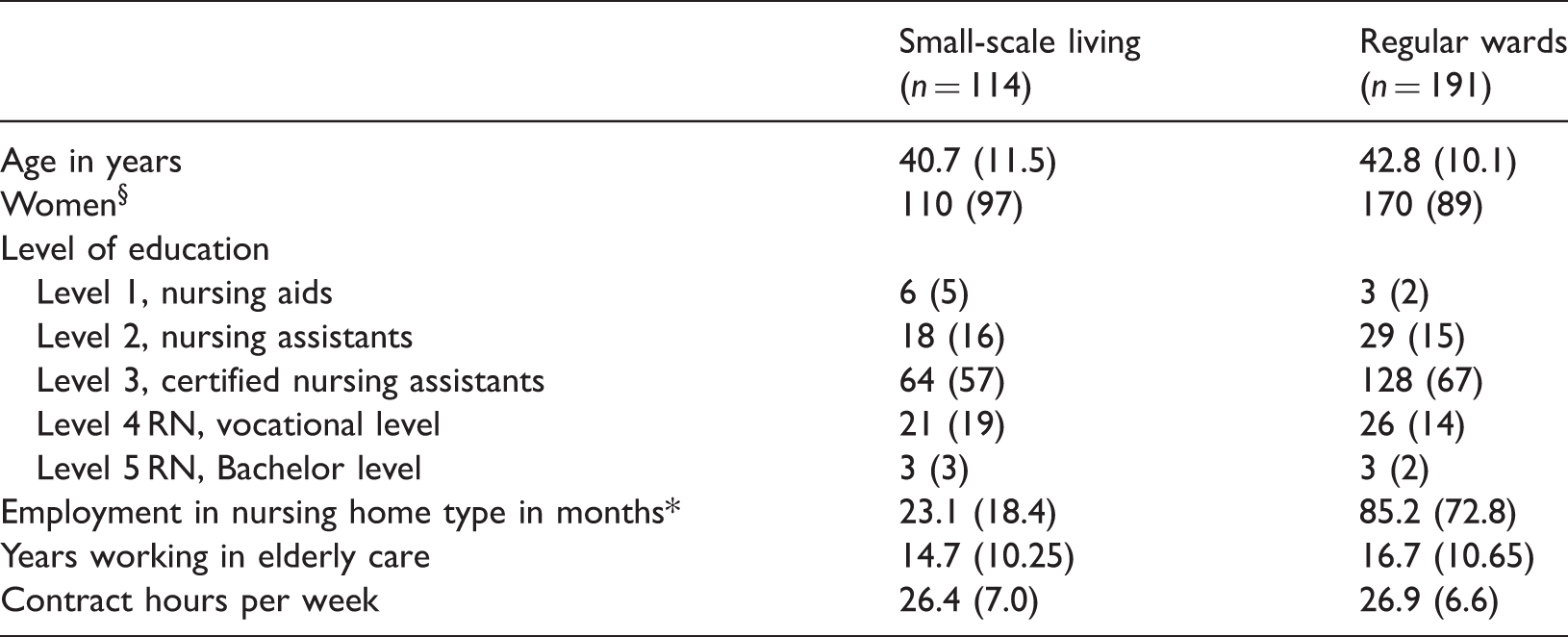
Data are mean (SD) or number (%).
p = 0.021.
p = 0.001.
A substantial contrast between the two environments (small-scale and regular wards) existed. The mean score of the contrast questionnaire in small-scale wards (67.5; range 60–77) was significantly higher than the mean score of regular wards (42.3; range 36–55), with no overlapping scores (mean difference 25 points; p < 0.001). This contrast remained stable over time (mean difference after 12 months 26 points; p < 0.001).
Unadjusted means (SD) of staff outcomes on burnout symptoms and job characteristics like job autonomy, social support, workload and physical demands.
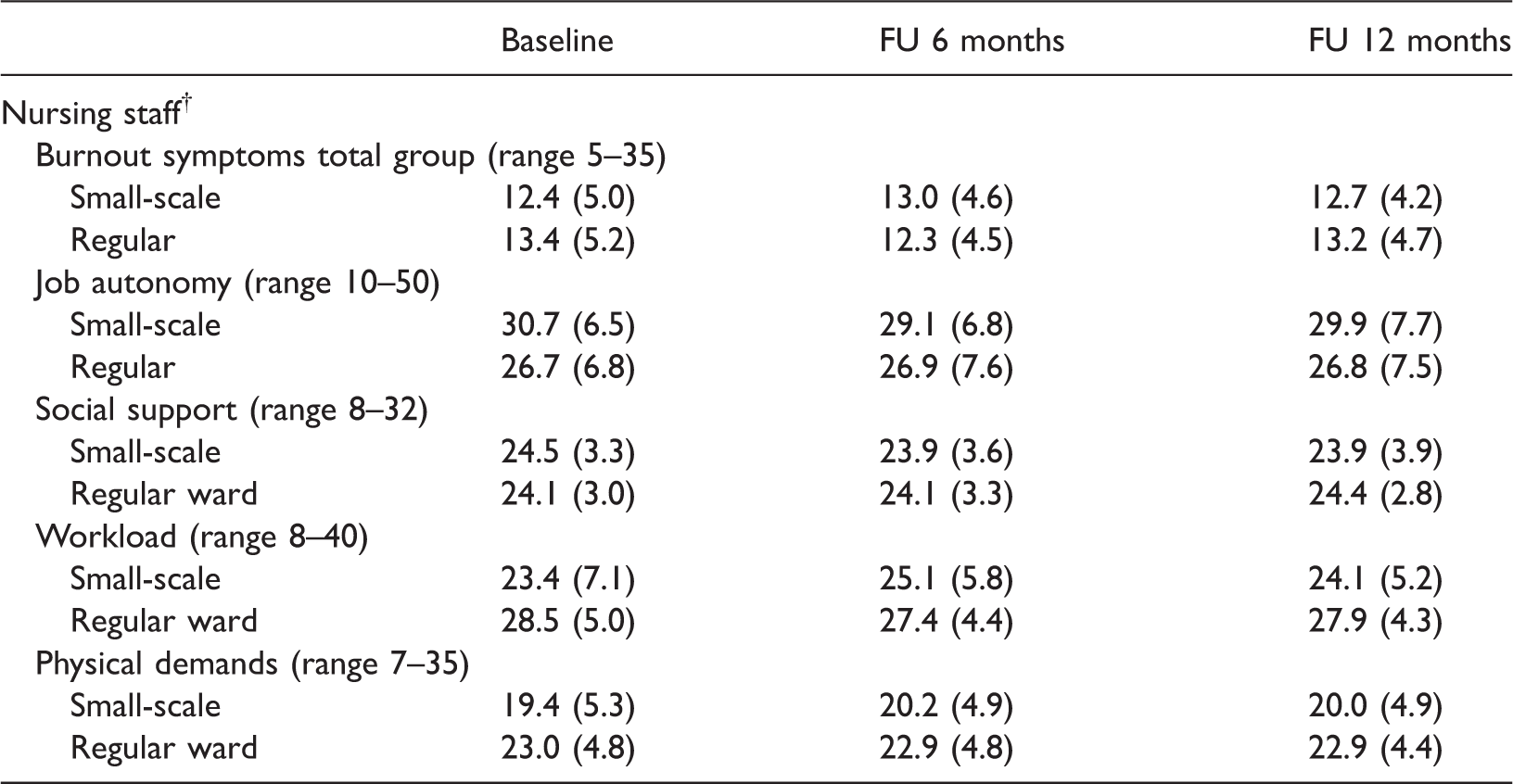
Nursing staff: Baseline nsmall-scale = 114, nregular wards = 191; follow-up (FU) after 6 months nsmall-scale = 72, nregular wards = 109; follow-up after 12 months nsmall-scale = 69, nregular wards = 87.
Higher score indicates more burnout symptoms, autonomy, support, workload and physical demands.
Effects on burnout symptoms
No significant effects on burnout symptoms were found in the analyses of the total participants' group (adjusted mean difference 0.72, 95% confidence interval (CI) −1.19; 2.64, p = 0.458).
Effects on job characteristics
Job autonomy
A statistically significant group effect was found for job autonomy (adjusted mean difference 3.88, 95% CI 1.17–6.59; p = 0.005), demonstrating that nursing staff in small-scale living facilities experienced more job autonomy than staff in regular wards for all measurements. Differences were stable over time.
Social support
No significant effect was found for overall social support in the total participants' group (adjusted mean difference 0.51, 95% CI 0.68–1.71; p = 0.401). Both groups scored relatively highly on social support.
Additional analyses found a significant effect for social support by co-workers for the total group of participants. Nursing staff in small-scale living facilities experienced more social support from their co-workers than staff in regular wards (adjusted mean difference 0.71; 95% CI 0.16–1.26; p = 0.012). No significant effects were found for social support by supervisors (adjusted mean difference 0.24; 95% CI −0.79; 1.26; p = 0.652).
Workload
A significant group by time interaction was found for workload. In small-scale living facilities, less workload was experienced for all three measurements compared with regular wards. Staff in regular wards reported significantly more workload at baseline (adjusted mean difference 5.25; 95% CI 2.39–8.11; p = 0.001), after 6 months (adjusted mean difference 3.12; 95% CI 0.31–5.93; p = 0.030) and after 12 months (adjusted mean difference 4.12; 95% CI 1.27–6.97; p = 0.005) compared with staff in small-scale living facilities.
Physical demands
A significant group effect was found for physical demands. In small-scale living facilities, significantly fewer physical demands were experienced by nursing staff compared with those on regular wards (adjusted mean difference 3.22, 95% CI 1.27–5.17; p = 0.001).
Discussion
This study examined the effects of working in a new type of dementia care facility (i.e. small-scale living facilities) on staff burnout symptoms and various job characteristics. Differences in job characteristics (e.g. job autonomy, workload and physical demands) were found. Nursing staff working in small-scale, homelike care facilities perceived significantly more autonomy, more social support, less workload and less physical demands. No overall effects were found on burnout symptoms for nursing staff in small-scale living facilities in comparison with traditional nursing homes.
The findings in this study are in line with our previous study findings into the effects of small-scale living facilities on staff well-being by Verbeek et al. (2010a). This study did not demonstrate effects with respect to the outcome measures job satisfaction and motivation in the total group of nursing staff. A recent paper by Adams et al. (2017) also found that the ‘dose’ of the home likeness seems to impact in a positive way on the job experience of nursing staff.
Previous studies on burnout symptoms comparing both care conditions are mixed. While Reggentin and Dettbarn-Reggentin (2004) found no differences in burnout symptoms, Te Boekhorst et al. (2008) found differences in levels of reported burnout symptoms in favour of nursing staff working in small-scale living facilities. These studies suggested that differences in job characteristics (i.e. more job control, fewer demands and more social support) may account for these results (Reggentin and Dettbarn-Reggentin, 2004; Te Boekhorst et al., 2008). Burnout symptoms have been found to be significantly higher in jobs that combine higher demands and lower autonomy (Landsbergis, 1988). The findings of the present study though could not confirm this suggestion. While differences in job characteristics were present for the total group of participants, no differences were found for burnout symptoms.
With regard to job characteristics, in this study nursing staff experienced significantly more autonomy and fewer physical demands and workload in small-scale living facilities compared with staff in regular wards. These findings are consistent with those of other studies, suggesting that demands were lower in small-scale living facilities whereas control/autonomy was higher (Reggentin and Dettbarn-Reggentin, 2004; Te Boekhorst et al., 2008; Vermeerbergen et al., 2017). A process evaluation demonstrated that nursing staff experienced high levels of autonomy in deciding on the day structure (Verbeek et al., 2012). This feeling may partly explain their experience of lower demands and workload. Furthermore, a study by Willemse et al. (2014) stated that staff may experience less interruptions by colleagues providing other services and do not need to deal with their colleagues' time schedules and as a consequence perceive less job demands, which could explain differences.
Although overall analyses in total social support showed no differences, staff working in small-scale living facilities experienced more social support by co-workers. This finding may seem somewhat surprising, since small-scale living facilities offer an environment in which only a small fixed team of nursing staff is responsible for a small group of residents, in contrast to the large teams in regular wards. It might be explained by stronger team cohesion of staff working in these new care environments. Future work should address how these care environments need to be arranged in order to create optimal and efficient working environment conditions for nursing staff.
Some limitations of this study need to be acknowledged. Clearly we need to be careful in interpreting our findings. It remains questionable what causes the differences in nursing staff working in small-scale living facilities compared with regular wards. For most variables notable differences between both care conditions were already observed at baseline and remained consistent over time, therefore no causality could be determined. Personality characteristics of nursing staff may account for differences in job characteristics. A recent study by Pot and De Lange (2010) also suggested that staff characteristics (e.g. age, cultural background) play a role in differences in job characteristics like autonomy. In the current study only a limited number of staff characteristics were included. No information was gathered on ward-related characteristics like management mode, staff ratio and skill mix. Furthermore, although the groups' baseline characteristics were comparable in the present study, except for gender and time of employment in the facility, the groups may differ in terms of other characteristics and/or competences that were not assessed. Staff with specific personal characteristics that make them less likely to perceive high levels of job demands might be more likely to work in living arrangements providing small-scale care. This may have biased our findings. Nursing staff are free to choose a facility to work in and probably choose the type in which they feel most comfortable.
In addition, one might wonder whether there were any differences in the kind of patients cared for in the two different settings. A previous study by Verbeek et al. (2010b) showed that residents living in small-scale facilities had a better cognition and functional status compared with residents in regular facilities. However, the findings of the process evaluation (Verbeek et al., 2012) demonstrated that residents' care dependency (more dependent on activities of daily living and cognitive performance) was not mentioned by nursing staff as an important relevant factor. Therefore, we do not think residents' characteristics affected the findings of our current study.
Furthermore, the proportion of non-responders at follow-up was relatively high, and even higher in nursing staff working in regular wards than staff in small-scale facilities. Not returning questionnaires, transfer to another ward or nursing home and maternity/ sickness leave were the main general reasons for non-responding. Insight into the exact reasons for non-responding, however, is lacking. Non-response may be influenced by the social work group cohesion and involvement of small teams working in the small-scale living facilities. Furthermore, it is conceivable that non-responders experienced the highest amount of workload.
Future directions
More attention should be given to the nursing skills and competences required for working in either one of the care settings. Since this study showed that job-related characteristics differed, other competences may be required. If these can be identified, recruitment and selection of staff would be improved and tailored to the skills of nursing staff. Furthermore, educational programmes could be tailored to train nursing staff for work in small-scale living facilities.
Nursing homes offer complex working environments that are influenced by numerous factors. A leading model, originally developed by Karasek (1985), called the job-demand-control model, states that two job characteristics (demands and control) influence well-being and job satisfaction. A combination of high job demands and low job control is particularly suggested to have a negative impact such as low job satisfaction. Johnson and Hall (1988) extend the model with social support, since they assume that support received from supervisors and co-workers could buffer the impact of demands and control. In addition, Spoor et al. (2010) mentioned that job resources and recovery opportunities have to match job demands if outcomes are to be optimised. It remains unclear how these can contribute to interventions focusing on improving staff well-being (Spoor et al., 2010). Further research is needed to examine underlying mechanisms for an understanding of possible relationships among working conditions, job characteristics and outcomes such as job satisfaction and burnout and to reveal mediating effects in both nursing home care conditions. In order to have a clear insight into the underlying mechanism it might also be valuable to include measures on individualised (person-centred) care, resident – staff relationships and team climate in future studies – especially given the fact that it is well known that team climate is a major determinant of quality of care (Backhaus et al., 2017).
Conclusion
The findings of this study on job characteristics suggest that organisational climate could differ between both nursing home conditions and may influence nursing staff well-being. This has important implications for nursing home managers and policy makers. In order to achieve a healthy work environment for nursing staff it is important to be well aware of nursing staff's experienced well-being, especially since staff well-being may directly influence the quality of nursing home care (Gilloran et al., 1995) since job stress has been linked with turnover rates (Larrabee et al., 2010). Future studies should enhance our understanding of the influence of job characteristics on outcomes.
Key points for policy, practice and/or research
This study suggests positive effects of work environment on several job characteristics. Nursing staff working in small-scale, homelike facilities experience significantly more autonomy and fewer physical demands and workload compared with staff in regular wards. Since this study showed that job characteristics differed, other competences may be required. More attention should be given to the nursing competences required to tailor recruitment and selection of staff and educational programmes to train nursing staff. The findings of this study on job characteristics suggest that organisational climate could differ between both nursing home conditions and may influence nursing staff well-being. This has important implications for nursing home managers and policy makers. Future studies should enhance our understanding of the influence of job characteristics on outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study design and protocols were approved by the Medical Ethics Committee of the University Hospital Maastricht and Maastricht University (reference number MEC 07-4-041). In addition local ethics Committees of the participating organisations have given consent to the study protocols and procedures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Maastricht University, the Province of Limburg and five healthcare organisations, all located in the southern part of the Netherlands. Funders had no role in the design, methods, data collections, analysis or preparation of this manuscript.