
Abstract
Background:
Workplace violence (WPV) is an occupational hazard to which nurses are often exposed, which can be a risk factor for severe mental health problems including post-traumatic stress disorder (PTSD). Therefore, understanding the prevalence of WPV and its association with PTSD among nurses may be important for developing effective workplace safety and support.
Objective:
This paper examined the prevalence of WPV and PTSD among nurses in Germany and analyses the association between them.
Methods:
A cross-sectional online survey was conducted among nurses across all clinical settings in Germany (May–June 2024). WPV and PTSD symptoms were measured with standardised scales, and logistic regression tested their association.
Results:
In total, 411 participants (61.0%) were hospital-based nurses. Non-physical violence was more prevalent than physical violence. Suspected PTSD was found among 8.5% of the participants. PTSD symptoms were significantly higher among participants exposed to WPV (OR 3.378; 95% CI: 2.096; 5.445). Availability of employer-provided support following WPV incidents was found to decrease suspected PTSD with an odds ratio of 0.122 (95% CI: 0.031; 0.483).
Conclusions:
In order to lessen the PTSD effects of WPV, present findings emphasise the necessity of reporting mechanisms, employer assistance, and targeted interventions. These steps are also crucial to promoting workforce retention.
Background
Nurses represent a significant profession in the healthcare sector. They provide care to a vulnerable population which relies on healthcare. Nurses provide care in hospitals, nursing homes, and outpatient care settings. The World Health Organization (WHO) estimates that the global number of nurses is approximately 29 million (WHO, 2024). Within the scope of their work, nurses may experience challenges, responsibilities and burdens, which affect not only their professional but also their private sphere and can sometimes lead to negative consequences. This includes workplace violence (WPV) against nurses. The WHO defines violence as: the intentional use of physical force or power, threatened or actual, against oneself, another person or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation (Krug et al., 2002). WPV may occur physically or non-physically. Meta-analyses have shown a global prevalence of 9%–24.4% of physical and 42.5%–48% of non-physical violence (Liu et al., 2019; Zhang et al., 2023). In a study by Schablon et al (2018) in Germany, among nursing and care staff surveyed, 94.1% of those who reported experiencing violence in the past 12 months had encountered verbal abuse, and 69.8% had experienced physical violence. According to the same study, nurses in hospital settings report the highest prevalence of WPV, followed by those in nursing homes and outpatient care; however, structural risk factors such as isolation, understaffing and lack of support may increase vulnerability to violence particularly in long-term and outpatient care settings (Schablon et al., 2018). Nurses’ frequent contact with patients and residents create a high risk of WPV (Kumari et al., 2022). Higher odds to experience WPV in the healthcare sector are associated with less work experience of nurses (Abdulwehab and Kedir, 2025) and previous experiences of WPV. A younger age and less work experience also contribute to an increased risk of WPV (Ekpor et al., 2024; Kumari et al., 2022; Pagnucci et al., 2022). In order to address WPV, it is necessary to report any kind of experienced violence. However, there is significant underreporting (Schablon et al., 2018; Song et al., 2021; Spencer et al., 2023). The main barriers to reporting are: fear of consequences after reporting, nurses’ perception (i.e. violence is part of the job) and lack of knowledge (Spencer et al., 2023). Support after the incident is mainly obtained from colleagues and supervisors (Schablon et al., 2018). Most nurses remain in their clinical setting after the experienced WPV (Gigli and Gonzalez, 2024).
Experiencing violence in the workplace has both direct and indirect effects on the health and sense of security of nurses (Kumari et al., 2022). Health effects are predominantly related to psychological well-being including anxiety and stress or depression (Hassankhani et al., 2018). A comparable study from German-speaking Switzerland found that approximately 23% of hospital employees – including a disproportionate number of nurses – experienced WPV or discrimination in the past year, with exposed staff showing 3–4 times higher odds of mental health complaints such as sleep disorders, stress, and burnout (Stahl-Gugger and Hämmig, 2022). Physical health issues can encompass injuries, sleeping problems or absenteeism (Mohammed et al., 2021). Additionally, WPV is associated with workplace cognitive failure (Arnetz et al., 2024). A major consequence can be post-traumatic stress disorder (PTSD) (Wang et al., 2022). PTSD can occur in persons who experienced, were confronted with, or witnessed a traumatic incident (American Psychological Association [APA], 2023). A survey has shown that in Germany, the prevalence of PTSD within the general population amounts to 2.3% (Jacobi et al., 2014), comparable national data for nurses are not yet available. Major symptoms of PTSD include staying away from workplaces, sleep disturbances, and difficulties concentrating. Symptoms typically occur within the first three months after the incident and can last for over one year (APA, 2023). This can also recur vicariously, for example, a recent study by Zhong et al. (2022) showed that 25.6% of healthcare workers (including other professions than nursing) exhibited symptoms of PTSD following the traumatic public murder of a physician in China, even though most were not directly involved. Similar figures are also seen in a study from Hong Kong (Hong et al., 2023) and China (Lu et al., 2023). A major influencing factor were previous traumatic experiences. Beyond personal mental health, PTSD symptoms exacerbate current staffing crises in the healthcare industry by increasing absenteeism, staff turnover and workforce shortages (Janda and Jandova 2015). The stability of care teams, the standard and safety of patient care and the operational effectiveness of healthcare organisations are all impacted by these outcomes, in addition to the health and longevity of nurses’ careers. Workforce retention is therefore a critical issue. Recent German data show that WPV is strongly associated with emotional exhaustion, a core component of burnout, which in turn threatens retention (Campione and Henschke, 2025; Kim et al 2020; Gedik et al 2023). Retention is not only about preventing premature exits but also about supporting nurses to remain until retirement; Schmedding et al. (2025) emphasised that both attrition and long-term retention must be addressed to sustain the profession. Moreover, retention depends on fostering intrinsic motivators such as professional meaning, autonomy, and supportive work environments (Teutsch et al., 2025). Exposure to WPV undermines these protective factors and, together with its psychological sequelae such as PTSD, should be considered not only a health risk but also a strategic workforce issue. Broadly speaking, the cumulative effect of PTSD-related attrition emphasises how critical it is to prioritise addressing WPV in national policy and health workforce planning, guaranteeing that measures to prevent and lessen WPV are acknowledged as crucial elements of long-term healthcare systems.
Objectives
Based on this overview above, we explored the relationship between WPV and PTSD symptoms among nurses in Germany.
Our primary research question was: Is exposure to WPV associated with an increased likelihood of reporting PTSD symptoms among nurses in Germany?
We hypothesised that nurses with exposure to WPV would show significantly higher odds of reporting PTSD symptoms compared to those without such exposure, after adjusting for relevant socio-demographic and occupational factors.
Method
To achieve these objectives, an online-based cross-sectional study was conducted between 1st May and 30th June 2024. For data collection, the web-based survey tool QUAMP® (Sociolutions GmbH, Potsdam, Germany) was used.
Sample
The survey was addressed to nurses in the following settings: nursing homes, hospitals, and outpatient care facilities. Nurses, currently working in any of these settings in Germany, with the ability to provide information, were included. Explicit exclusion criteria have not been formulated, but due to the nature of online surveys, nurses without access to the worldwide web were, of course, unable to participate. The distribution of the questionnaire was mainly through social media, such as Facebook, Instagram, LinkedIn and X (formerly Twitter). Additionally, the chain-referral method was used. Due to this sampling strategy, the sample is to be considered a non-probability sample (Wiśniowski et al., 2020). All posts contained a very brief introduction and a link to the questionnaire. The questionnaire began with a comprehensive introduction providing information about the purpose of the survey, a trigger warning regarding experienced violence and data protection statements (see ‘Ethics’ section for further details on participant safeguarding). Only upon agreement to participate, could the questionnaire be filled out. The questionnaire allowed the option to skip questions or exit entirely without completion.
Questionnaire
In the first section of the questionnaire, demographic and professional information was collected (see Table 1 for a complete overview). This included variables such as age, gender, professional qualification, care setting, years of work experience, and length of employment with the current employer. Afterwards, two questionnaires were delivered relating to experienced violence and suspected PTSD. Finally, nurses were asked, if employers offered assistance after experiencing WPV and whether de-escalation training was offered in order to mitigate future incidents of WPV. For these two questions, nurses had the options to agree, partly agree, or not agree.
Characteristics of participants.
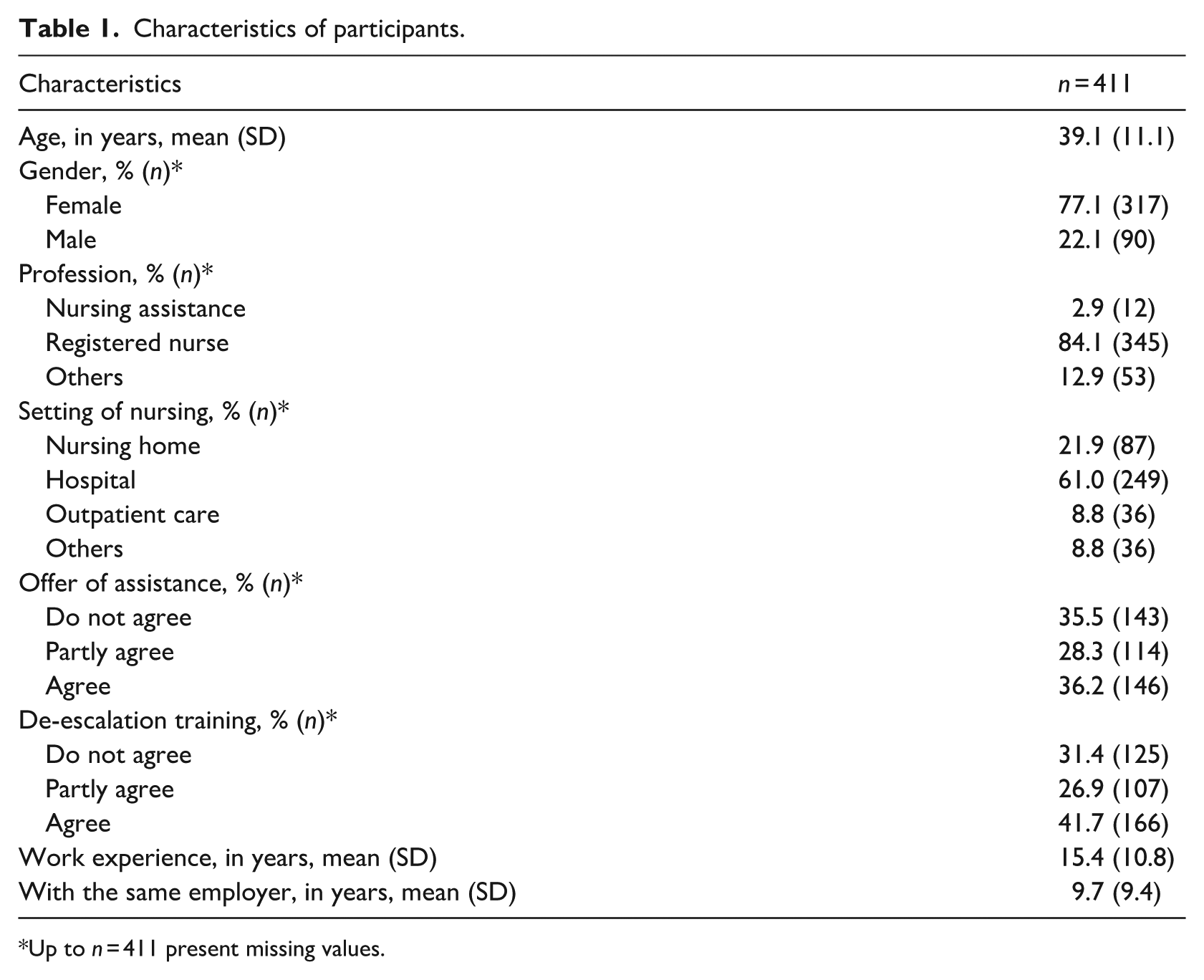
Up to n = 411 present missing values.
Violence: HABS-UG
The standardised questionnaire Healthcare-worker’s Aggressive Behaviour Scale-Users (HABS-UG) (Ruiz-Hernández et al., 2016) contains 14 items and 2 subdomains. The subdomain non-physical violence contains 11 items (e.g. users question my decisions) and the subdomain physical violence the remaining 3 items (e.g. users show their anger at me by breaking doors, windows, walls). All items could be answered on a 6-point Likert incidence scale from never up to daily. Both subdomains were analysed by calculating the mean scores (theoretical range 1–6). Higher scores express more frequent experienced violence. The German version is considered to be valid and reliable (Gräske and Schulz, 2025).
PTSD – IES-R
PTSD was assessed with the standardised instrument Impact of the Event Scale revised version (IES-R) that is comprised of 22 items. The IES-R used a 6-point Likert scale (0 = never, 1 = a little bit, 3 = moderately, 5 = extremely), with 2 and 4 included as intermediate response options without verbal labels (Maercker and Schützwohl, 1998). The subscale intrusion contains 7 items (e.g. other things kept making me think about it), avoidance contains 8 items (e.g. I felt as if it had not happened or was not real) and hyperarousal again 7 items (e.g. I had trouble staying asleep). For all subdomains, items were summed up. The total score was calculated as follows: X = (−0.02 × intrusion) + (0.07 × avoidance) + (0.15 × hyperarousal)–4.36. If X > 0, there is suspected PTSD. This scale has previously been used in a studies among healthcare staff – including nurses – in Shanghai (Li et al., 2025) and the United Arab Emirates (AlJaberi et al., 2024).
Data analysis
After checking for missing data and non-logical data entries, the data were described using means and standard deviation, median, absolute and relative values. A logistic regression was calculated for the dependent variable of suspected PTSD (yes/no). Independent variables were selected based on theoretical relevance and empirical findings from prior studies on WPV and psychological outcomes in healthcare settings (Hong et al., 2023; Lu et al., 2023). These included the following categorial independent variables gender, professional background, setting, offers of assistance by the employer and de-escalation training. The co-variables of age and total violence (HABS-UG total) were also included. Potential multicollinearity was assessed using Pearson correlation coefficients. Due to multicollinearity of work experience as well as time at the same employer with age and non-physical as well as physical violence with total violence were excluded from this logistic regression. Logistic regression analysis was conducted, including calculation of odds ratio (OR), 95% confidence interval (CI), explanatory variance (Nagelkerke’s R2) and overall classification accuracy. All statistical tests were conducted with a significance level of ⩽0.05.
Ethics
This study involved no patients or medical interventions. It was conducted solely with adult nursing professionals who voluntarily participated and provided informed consent. Participation was fully anonymous: no identifying personal data (e.g. names, addresses, IP addresses) were collected, and responses cannot be traced back to individual participants.
According to the Information Sheet on Regulations Governing the Ethics Committee of Alice Salomon University of Applied Sciences Berlin (Satzung der Ethikkommission der Alice Salomon Hochschule Berlin; Borde, 2019), ethical review is recommended for research involving potential risks to participants. As this anonymous, non-interventional survey collected no identifying personal data and posed no foreseeable risks, formal ethics approval was not required.
Nevertheless, the study was conducted in strict compliance with national and institutional ethical standards and adhered to the principles of the Declaration of Helsinki and the International Council of Nurses Code of Ethics. The questionnaire began with a trigger warning regarding experiences of workplace violence, and participants were informed that they could skip any question or withdraw at any time without explanation. To mitigate potential distress, participants were signposted to professional support resources, including national crisis hotlines and counselling services, ‘Telefonseelsorge’, available 24/7, free of charge and online counselling resources (www.telefonseelsorge.de).
Results
After 2 months, 411 questionnaires had been received. Due to the sampling strategy, a response rate could not be calculated. Characteristics of participants are shown in Table 1. Participants are mainly female, registered nurses and work in hospitals. About one-third do not agree that employers provide assistance after experienced violence or offer de-escalation training to handle critical situations better.
Violence and PTSD
Results regarding experiences of violence and PTSD are displayed in Table 2.
Experienced violence and symptoms of PTSD.
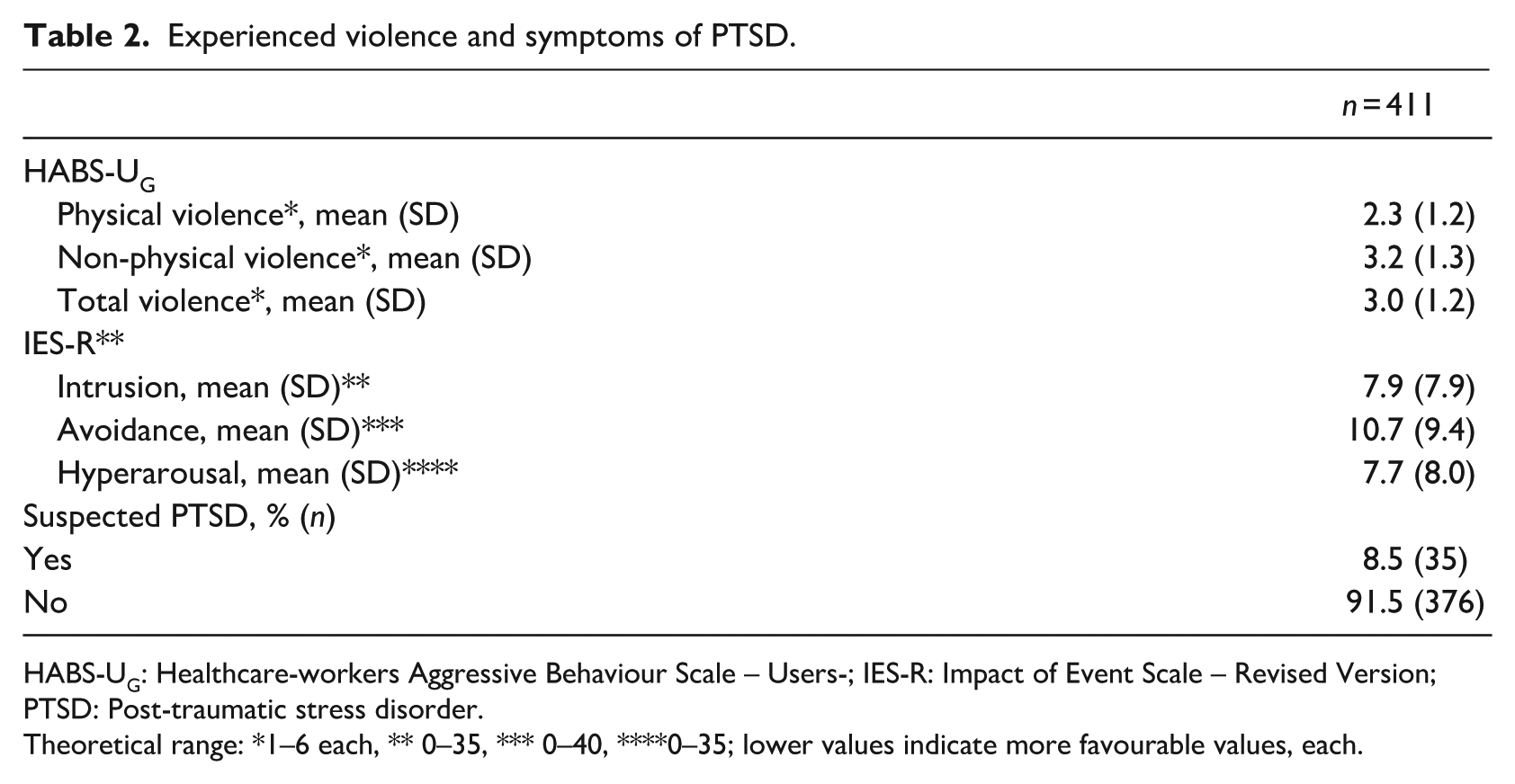
HABS-UG: Healthcare-workers Aggressive Behaviour Scale – Users-; IES-R: Impact of Event Scale – Revised Version; PTSD: Post-traumatic stress disorder.
Theoretical range: *1–6 each, ** 0–35, *** 0–40, ****0–35; lower values indicate more favourable values, each.
Participants reported both physical and non-physical violence. Non-physical violence was more frequent. A total of n = 311 (75.7%) participants reported experiencing physical violence, whereas n = 100 (23.0%) had never experienced it. Similarly, n = 388 (94.4%) reported experiencing non-physical violence, whereas only n = 23 (4.8%) had never experienced it. In total, n = 388 (94.4%) participants experienced at least one form of violence, and only n = 23 (4.8%) reported no experience of either physical or non-physical violence. A suspected diagnosis of PTSD was identified in n = 35 (8.5%) of the participants. As shown in Figure 1, nurses with a suspected diagnosis of PTSD show higher scores in all forms of violence.
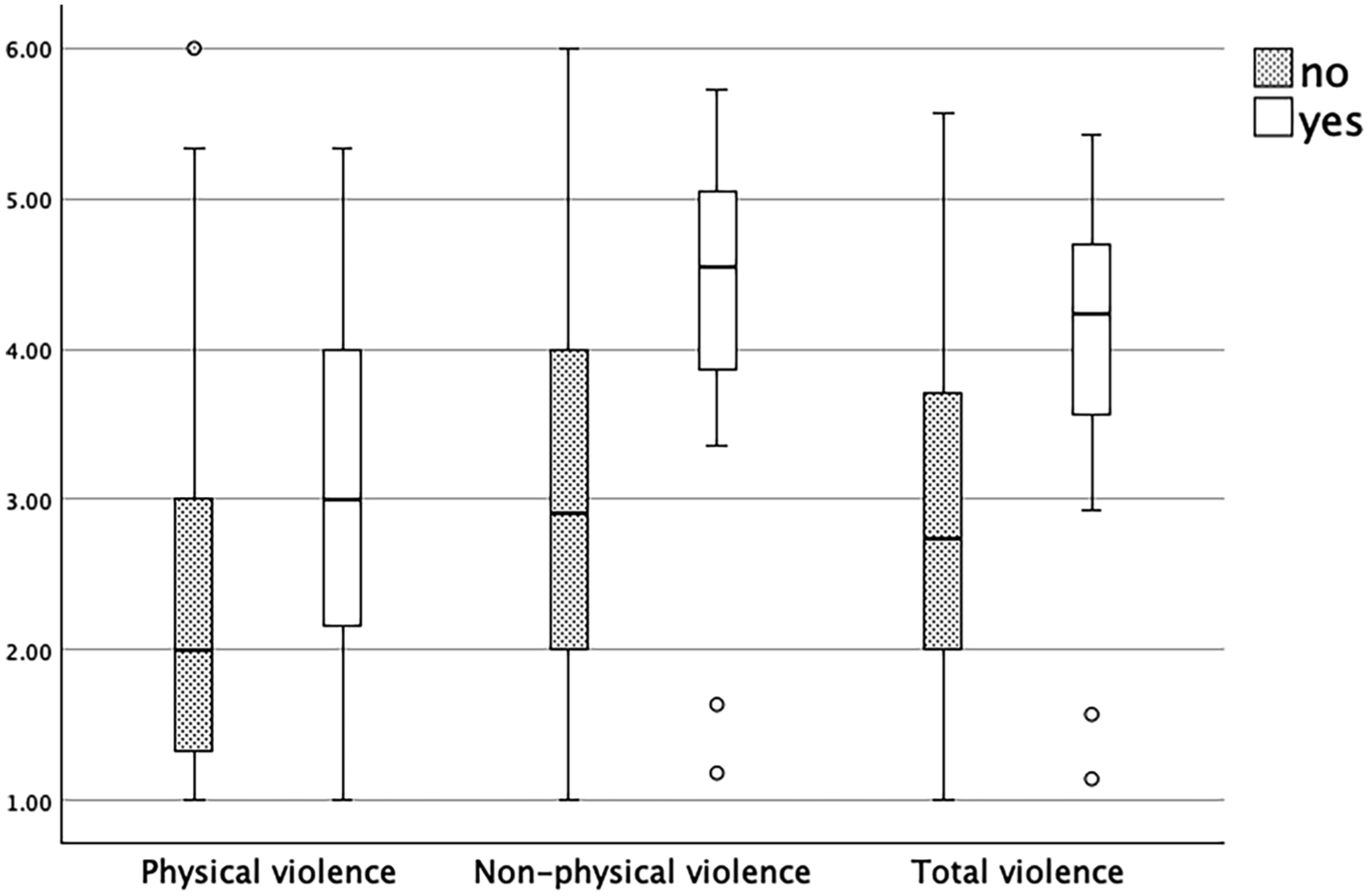
Experienced Violence (HABS-UG) divided into Suspected PTSD (IES-R).
The logistic regression shows a significant result (p < 0.001) with a sufficient explanation of variance (Nagelkerke’s R2 = 0.336). The model correctly classified 92.4% of all cases.
A significant association is identified for nurses who agree that their employers offer assistance after experiencing violence (OR 0.122; p = 0.003) and the HABS-UG total violence (OR 3.378 p < 0.001). All other included independent variables do not show a significant association (see Table 3).
Explanation of suspected PTSD.
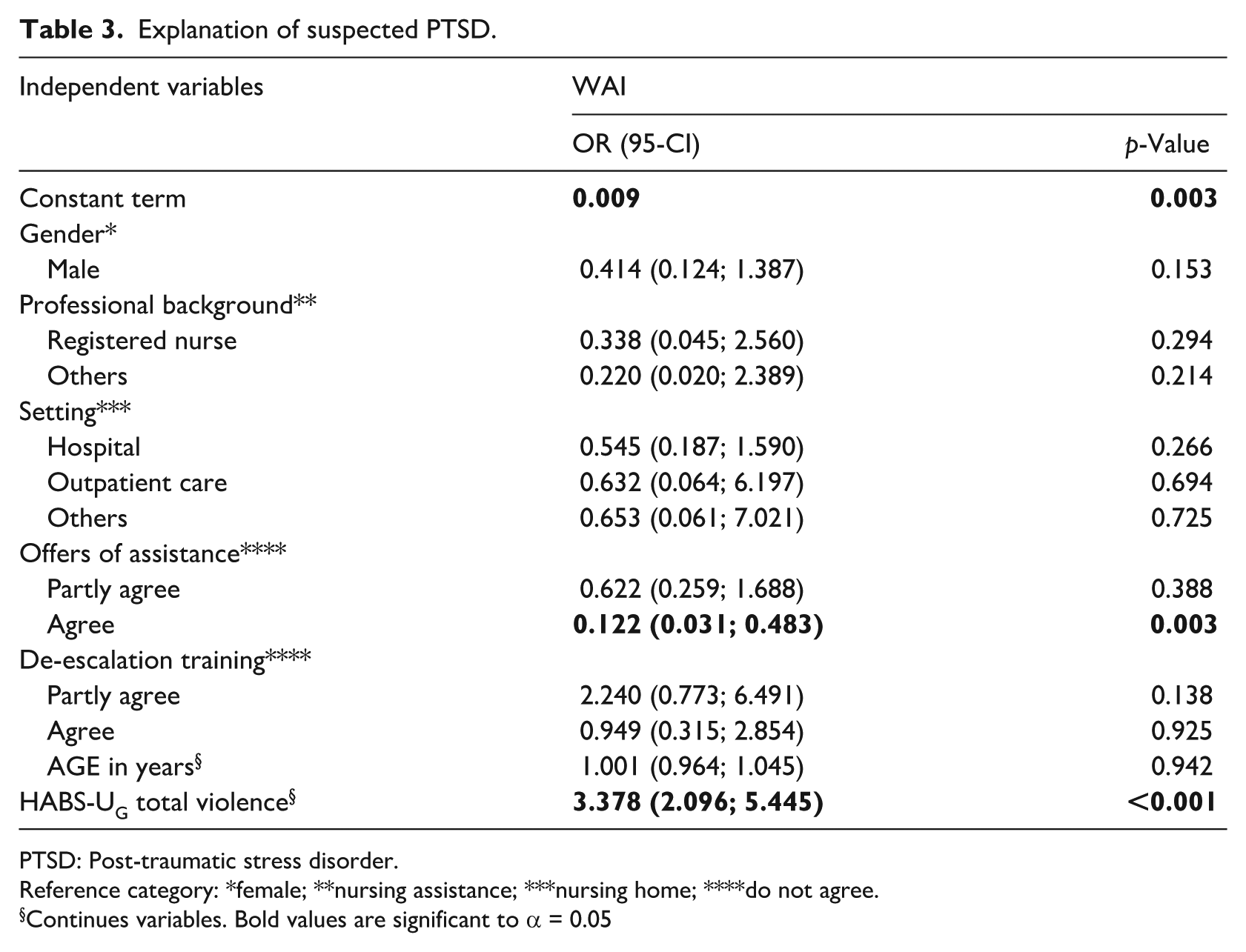
PTSD: Post-traumatic stress disorder.
Reference category: *female; **nursing assistance; ***nursing home; ****do not agree.
Continues variables. Bold values are significant to α = 0.05
Discussion
The objectives were to describe the experienced violence and suspected diagnosis of PTSD and the associations between the two. This is the first time that the included sample shows typical characteristics for a German study population within the nursing profession, with the exception of age (Gräske et al., 2021; Petersen et al., 2023). The participant population is younger than those in other studies.
Forms and frequency of WPV
The included population experienced both physical and non-physical violence. Non-physical violence occurred more frequently and effected a larger proportion of the participating nurses. This aligns with previous studies, who report that verbal aggression and verbal threats are the most frequent forms of WPV (Liu et al., 2019; Zhang et al., 2023). In Germany, Schablon et al. (2018) found that non-physical WPV is the most frequent type of WPV. However, it is known that the incidence of WPV is underreported (McGregor et al., 2025; Schablon et al., 2018; Song et al., 2021; Spencer et al., 2023). This underreporting contributes to the persistent impact of WPV and challenges efforts to understand its full scope. The high prevalence of WPV reported in this study may be partly due to self-selection bias, as nurses with prior WPV experiences might have been more likely to participate. However, the anonymous online format and framing of the study could have encouraged more open reporting giving a more true picture of prevalence.
Association between WPV and suspected PTSD
In this study, the prevalence of a suspected diagnosis of PTSD is 8.5%, which is lower than the identified proportion of about one-fourth (Zhong et al., 2022). However, compared to a larger study of the general German population, the proportions of PTSD are 3 to 4 times higher (Jacobi et al., 2014). The present results show a significant association between WPV and suspected PTSD. This is in line with conceptualisation of PTSD (APA, 2023). Empirical findings state a strong association between WPV and PTSD (Hong et al., 2023; Zhong et al., 2022), which are confirmed by Abdulwehab and Kedir (2025) in their systematic review. In summary, WPV is not only a safety issue, but also it is a health risk factor, that contributes to severe negative health consequences for nurses.
Role of employer support
A key finding is the significant organisational support in mitigation negative consequences of WPV. This is in line with findings of Zhang et al. (2023), who reported that the lack of support is a significant predictor of PTSD symptoms among nurses who have experienced WPV. In addition, Lu et al. (2023) found that debriefing and psychosocial counselling is associated with reduced symptoms of PTSD. These findings underscore the need for health institutions to not only implement preventative strategies but also to ensure visible and accessible post-incident support systems to reduce the lasting impact of WPV. However, the reported lack of support may not indicate an actual absence of supportive pathways, but rather a lack of a clear communication about available support services.
Implications
WPV presents a safety as well as a health threat to nurses, requiring immediate organisational responses. First of all, employers and professional organisations should promote an open reporting culture (McGregor et al., 2025). This includes ensuring protection from negative consequences of reporting WPV. Hospitals should focus on avoiding violence, by running awareness-raising campaigns. Although the study found no significant association between de-escalation training and PTSD, regular training in de-escalation techniques is crucial in preparing nurses to deal with potentially violent situations, minimising the risk of assault. However, WPV can always reoccur. Therefore, a further focus should be the consequences of WPV including PTSD. The results show that WPV is a challenge implicating the safety of nurses. Employers should consider improving their safety concepts. The psychological consequences of violence, including PTSD, should be recognised and addressed as part of occupational health management programmes. This includes access to psychological support and counselling for affected persons. In addition, strategies to prevent and address WPV are not only essential for safeguarding health but also for improving workforce retention. Evidence shows that violence and its psychological consequences contribute to attrition and undermine long-term retention, whereas supportive environments and preventive measures foster stability in the workforce (Campione & Henschke, 2025; Schmedding et al., 2025; Teutsch et al., 2025). Ensuring that nurses remain healthy and motivated to stay in the profession is critical in light of demographic change and increasing care demands. Further research is needed to identify specific prevention strategies and supporting measures that go beyond training and are effective in different care settings. At the national level, policymakers share responsibility to ensure safe working environments, allocate resources for prevention and support and integrate WPV and its psychological consequences into workforce planning and health policy strategies. This also requires cooperation between professional organisations and employers. This is particularly important in light of the current demographic change. An increasing number of people needing care, staff shortages, increased workloads and constantly evolving medical care make it necessary to focus on the health of nurses.
Strengths and limitations
This study has several strengths. To our knowledge, it is the first nationwide study in Germany to look at the link between WPV and PTSD symptoms among nurses. The survey included a large number of participants from various care settings. This ensures the findings represent experiences from hospitals, nursing homes and outpatient care. Another strength is the use of reliable tools, specifically the HABS-UG for WPV and the IES-R for PTSD. This improves the reliability and comparability of the results. Finally, by combining the topics of WPV and PTSD in one study, we offer evidence that is relevant to both clinical practice and policy.
The web-based questionnaire was fully anonymous, which can be considered both a strength and a limitation. Anonymity likely reduced social desirability bias and encouraged honest reporting of sensitive experiences such as workplace violence. At the same time, anonymity prevented us from providing individual follow-up support to participants with suspected PTSD. Due to the sampling strategy, a sampling bias might exist. Only participants with internet access and an account for certain social media platforms were informed about the study. The inclusion of nurses who have limited social media access might change the results. Moreover, a self-selection bias may have occurred, as nurses who had experienced WPV might have been more inclined to participate in the survey, potentially leading to an overestimation of WPV prevalence. Additionally, there may be recall bias, as events could have been forgotten, misremembered, or underreported. Furthermore, the PTSD symptoms were assessed using a screening instrument and not a clinical diagnostic tool. Although the IES-R is widely used and validated, it may not fully capture PTSD symptoms in all populations or cultural contexts. Potential confounders or instrument limitations cannot be entirely ruled out.
Conclusion
Despite some limitations, this is the first study to present associations between WPV and suspected PTSD in nurses in Germany. The results show that both physical and non-physical forms of WPV are commonly experienced by nurses, with non-physical violence being more common. WPV and probable PTSD were found to be significantly correlated, highlighting the negative psychological effects of such experiences. Importantly, our analysis also showed that participants who reported receiving employer support after WPV had a markedly lower likelihood of suspected PTSD, suggesting that organisational responsiveness can play a protective role. These findings highlight the importance of healthcare organisations funding both preventative and post-event support initiatives. Protecting nursing professionals’ well-being and retention requires acknowledging WPV as a mental health issue in addition to a safety concern. Our findings therefore highlight that effective prevention and support following WPV are not only individual or organisational responsibilities to nurses’ health and well-being,but also crucial strategies to sustain workforce retention. Addressing WPV and its psychological sequelae, including PTSD, is indispensable to maintain a resilient nursing workforce and secure long-term care provision at the national level.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: According to ICMJE guidelines, all authors 1) have made substantial contributions to the conception and design, or acquisition of data, or analysis and interpretation of data; 2) have been involved in drafting the manuscript or revising it critically for important intellectual content; 3) have given final approval of the version to be published; and 4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
JG: study design, data collection, data analysis, manuscript preparation; LK: manuscript revision; VvW: study design, data collection, manuscript revision; FS: study design, data collection, manuscript revision; CS: study design, data collection, data analysis, manuscript preparation. All authors have read and approved the final version. All authors declare to have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This anonymous, non-interventional survey was conducted solely with adult nursing professionals who voluntarily participated and provided informed consent. No identifying data were collected, and responses cannot be traced to individuals. In line with the ASH Berlin Ethics Committee regulations (Borde, 2019), formal approval was not required as no risks to participants were anticipated. The study complied with national and institutional ethical standards, the Declaration of Helsinki, and the ICN Code of Ethics. A trigger warning was provided, participation was fully voluntary, and information on support services (e.g., Telefonseelsorge) was offered to mitigate potential distress.
Data availability
The data that support the findings of this article are available upon reasonable request from the authors.