
Abstract
Background:
Malnutrition and dehydration in residential aged care (nursing homes) are problematic worldwide, particularly for residents with dementia. However, conducting research to improve residents’ nutritional health can be challenging.
Aims:
This paper describes challenges, facilitators and recommendations following an intervention to enhance nutrition and hydration care.
Methods:
Meaningful Engagement in Nutritional Understanding (MENU; 2018–2021) was a participatory nutrition support intervention initiated in two Tasmanian care homes. Mixed methods evaluation explored nutrition and hydration status, knowledge and care practices with residents with dementia, staff and family; and the challenges to, and facilitators of, project implementation.
Results:
This study found nutrition and hydration to be problematic. However, despite multiple challenges, a participatory approach may help engage stakeholders and encourage action in this area. Challenges included resident recruitment, care home and staff engagement, and external factors. Facilitators included Nutrition Champions, the participatory research approach, and tailored resources and education.
Conclusions:
The study has implications for conducting more effective nutrition research in residential aged care, particularly with people with dementia, nursing and other care staff, to better understand their experiences and enhance care practices. Nursing staff are key to effective participatory research in residential aged care and to ensuring residents’ optimal nutrition and hydration.
Keywords
Introduction
Research suggests that the majority of Australians living with dementia in residential aged care homes (also known as nursing homes) are malnourished or at risk of malnourishment (Bell et al., 2015; Gaskill et al., 2008; Iuliano et al., 2017). This is not unique to Australia as the risk for malnutrition and dehydration for residents with dementia is problematic worldwide (Chatindiara et al., 2020; Keller et al., 2019; Leij-Halfwerk et al., 2019; Paulis et al., 2018). Cost and accessibility to fresh and nutritionally healthy food and liquids may limit their provision (Hugo et al., 2018; Iuliano et al., 2017; Pagone and Briggs, 2021). Furthermore, the capacity of people living with dementia to recognise or communicate hunger and thirst is frequently compromised (Anantapong et al., 2022; Mitoku and Shimanouchi, 2014; Murphy et al., 2017). Regardless of underlying causes, malnourishment results in adults with dementia being more vulnerable to delirium, falls, impaired wound healing, urinary tract infections, and unplanned hospitalisations; profoundly affecting their ability to participate in their own care, and decreasing quality-of-life (Agarwal et al., 2013; Beattie et al., 2017; Meijers et al., 2014).
One avenue to improving this situation is to raise awareness of care home staff and transform their knowledge of nutrition and hydration care (Anderson and Blair, 2021; Beattie et al., 2014; Borders et al., 2020; Everink et al., 2021; Lea et al., 2017; Lea et al., 2019; Paulis et al., 2022). Even when nutritional assessments are conducted and care plans developed, staff knowledge about best practice is not always translated into daily care (Etherton-Beer et al., 2021; Koh et al., 2022). Additionally, conducting research in residential aged care can be challenging for multiple reasons (Collingridge Moore et al., 2019; Edwards et al., 2003; Hall et al., 2009; Lam et al., 2018; Law and Ashworth, 2022; Peryer et al., 2022; Stephens and Knight, 2022). Issues include recruitment and informed consent of care homes and residents, staff time constraints and employment turnover, researchers being viewed as a threat, and budgetary factors (Beattie et al., 2018; Edwards et al., 2003; Hall et al., 2009; Lam et al., 2018). Nurses’ role in leading, coordinating and supervising care delivered in residential communities underscores the need for their increased participation in research to improve the quality of care (Micklewright, 2024; Watson et al., 2020).
Using a participatory action and learning approach has been identified as a priority for research in residential care settings. This approach builds the trust and understanding needed to achieve sustained improvements in care (Peryer et al., 2022). Participatory approaches have been used to improve the quality of the physical and social mealtime environment and increase relationship-centred care in programmes in a small number of Canadian (Keller et al., 2021) and Australian aged care homes (Cartwright et al., 2022). However, the approach has been underused to improve the quality of nutrition and hydration for people living with dementia in residential aged care, and to address the cultural and organisational changes needed to embed sustainability. These changes include welcoming the voices of people living with dementia and those who provide care. Including these voices is advocated internationally (Banerjee, 2022) and is reflected in Australia’s revised and strengthened aged care quality standards (Australian Government, 2025).
The MENU project
Meaningful Engagement in Nutritional Understanding (MENU) is a multi-component participatory intervention we developed to enhance nutrition and hydration care in the context of residential aged care. MENU builds upon suggestions from nursing, care worker, hospitality and other residential aged care staff from earlier research to improve the nutritional care and support of people with dementia (Lea et al., 2017). This qualitative research found that staff have ideas for how to improve such support which are often in accordance with the evidence base; however, opportunities to act on these ideas to implement change are limited. The MENU project’s participatory approach focused on facilitating residents, family members, staff and management working together to understand, choose and implement best nutrition and hydration care and support tailored to residents’ needs and preferences (see Figure 1 – MENU model).
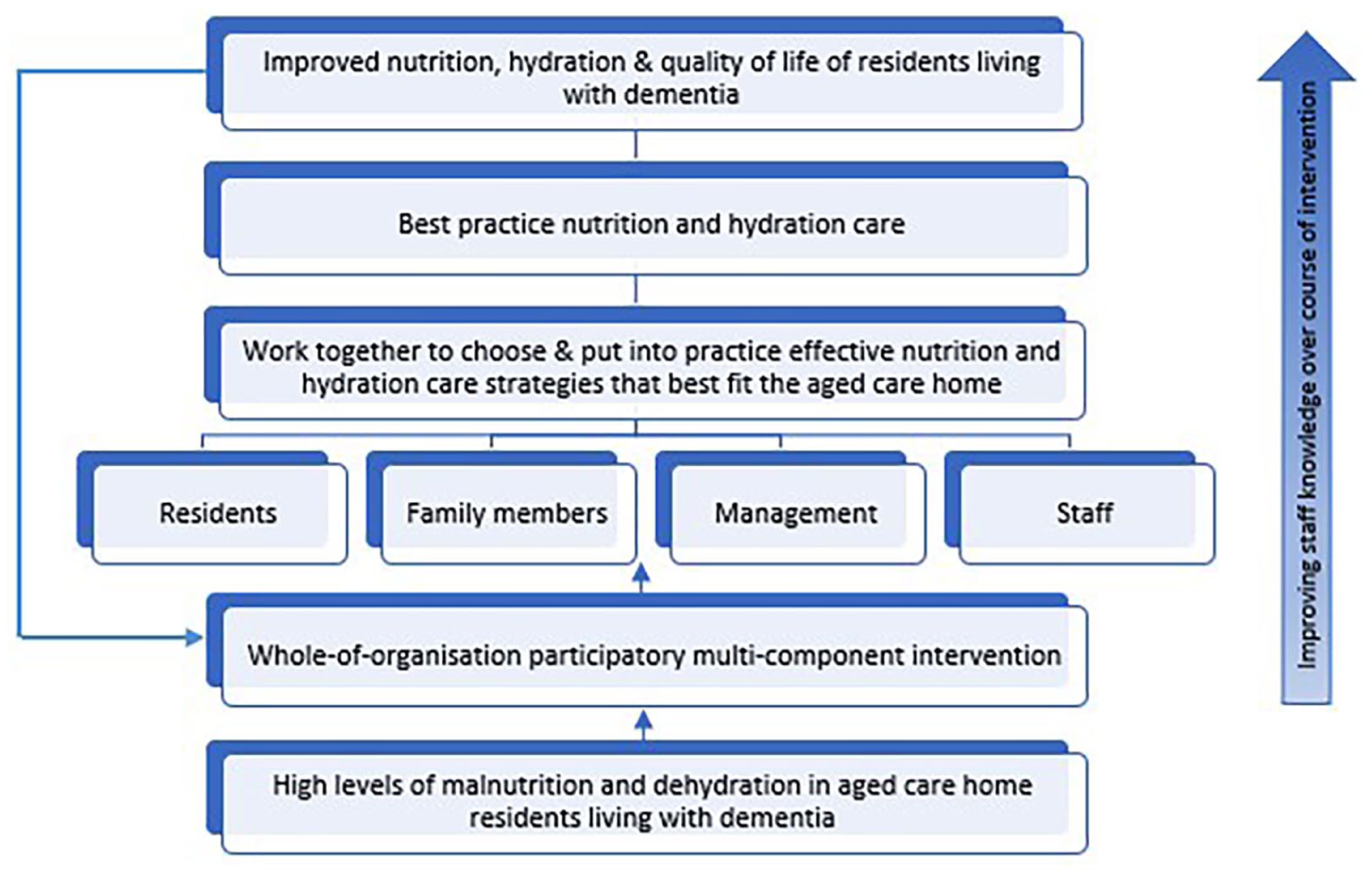
The MENU model.
We implemented MENU from 2018 to 2021, aiming to work with residents and staff in two Australian (Tasmanian) aged care homes. We report our experience with, and key findings from, the MENU project. We present both the challenges and facilitators experienced with implementing MENU in the residential aged care setting. Our experiences and findings guide recommendations for future participatory research using MENU. Overall, this paper contributes to the knowledge base for conducting participatory action research in residential aged care, particularly in relation to nutrition and hydration.
Methods
Design
The MENU mixed method participatory study design centred around five sequential workshops and related actions: (1) baseline data collection of current nutrition and hydration care from staff and family members; (2) baseline data sharing with residents, family members and staff, learning about best evidence care practices for residents, reflecting on this information and identifying key areas for action, and recruiting 4–5 staff per home with an interest in nutrition who volunteered to act as Nutrition Champions to develop home-specific action plans and guide the project; (3) discussing progress and problem-solving any barriers as the intervention took place; (4) collecting post-intervention data and feedback to evaluate the effectiveness and feasibility of MENU and (5) sharing results with residents, family and staff participants at the aged care homes. The 60–90-minute workshops were scheduled to be conducted over a 16-month period.
Participants and sampling
Two metropolitan, not-for-profit aged care homes (Home A; Home B), each with approximately 100–150 residents were recruited (Home B withdrew prior to implementation of their action plan). We then recruited in each home residents living with dementia, their family members, nursing staff, and staff in other roles related to nutrition.
Inclusion criteria for residents were moderate–severe cognitive impairment or dementia, as documented in medical records, and living at the care home for over 4 weeks. A designated nurse in each care home assessed resident eligibility. They also facilitated a letter of invitation being sent to the designated family representative/guardian of each of 126 identified residents, also inviting family participation. We aimed to recruit 35 residents from each home, totalling 70 residents. This was estimated to provide adequate power to assess malnutrition risk pre-and post-intervention, which was one measure of MENU effectiveness. As an example, a two-tailed paired t-test with 35 residents, moderate effect size of 0.5 for change in nutrition status and a significance level of 0.05 yields an acceptable level of power of 82% (Cohen, 1988).
We invited all enrolled and registered nurses at each home to participate, along with direct care workers and hospitality staff. We promoted the project and the invitation to Workshop 1 via flyers, posters, articles in staff newsletters, meetings and word of mouth. The inclusion criterion for staff was their paid employment at one of the participating care homes. We anticipated recruiting a total of 100 combined family/staff members across both aged care homes.
Nutrition champions and action plans
We held a training session at each home for the identified Nutrition Champions, co-facilitated by the chief project investigator (EL) and a dietitian. At these training sessions, the action areas identified during Workshop 2 were developed into evidence-based action plans. Educational resources were suggested to support staff to achieve these actions, tailored to meet residents’ nutrition and hydration needs in conjunction with staff educational needs and preferences, both of which were identified at each home. Customised action plans and educational resources were developed for each home, focused on strategies to raise staff awareness of the importance of hydration and to enhance the mealtime environment.
Measures/data collection
The project team consisted of eight researchers from three universities, including three registered nurse academics, and two representatives from each of the care homes, including one registered nurse. Team members met every 2–4 weeks and kept field notes throughout the project documenting experiences and challenges to problem-solve at project team meetings.
Baseline
We completed a formal nutritional assessment of participating residents at both homes to assess their malnutrition risk (Mini Nutritional Assessment – Short Form [MNA-SF]; Rubenstein et al., 2001) at baseline (November 2018–January 2019). Research assistants trained by the first author administered the MNA-SF along with 3-hour observations of nutrition care practices, and a review of residents’ care files.
We surveyed participating staff and family members via the Nutritional Knowledge Questionnaire (Beattie et al., 2014) to document their nutrition and hydration knowledge and perceptions of nutrition and hydration care (Workshop 1). The questionnaire included 11 multiple choice questions (each worth 1 point) assessing nutritional composition of foods, contributors to malnutrition and dehydration, fluid requirements and appropriate care practices for older adults including those living with dementia. This created a score between 0 and 11.
During project
We audio-recorded workshops at each home and kept field notes to inform the action plans being developed.
Post-intervention
We surveyed Home A staff and family members online and at a workshop with Nutrition Champions towards the end of the project (December 2020–March 2021). The online survey was available to all invited staff and family members regardless of whether they had participated in the intervention. The survey contained core questions from the baseline questionnaire as well as project evaluation questions. The workshop probed participants’ knowledge of nutrition and hydration, perceptions of nutrition and hydration care and their engagement with and perceptions of the project.
Analysis
A malnutrition risk score was calculated for each resident using the MNA-SF. We synthesised baseline data from observations and care file reviews by categorising data into key areas needed for improvement. We summarised qualitative data from the open-ended survey questions, resident observations and workshops by categorising responses. Fieldnotes were summarised into key concerns, barriers and facilitators.
We used descriptive analysis to summarise pre- and post-intervention questionnaire data, including mean nutrition and hydration knowledge score for staff (range 0–11/11), and the proportion of family and staff who had seen or used project resources or made changes to practice post-intervention. Quantitative data analysis was planned if the sample size was sufficient.
Ethics
The project received approval from the University of Tasmania Human Research Ethics Committee (Ref. No. H0017136) on 8 March 2018. We provided all participants with a written Information Sheet. Participants signed a Consent Form, except where consent was implied by questionnaire completion and submission, and where a resident living with dementia was unable to consent. Capacity to consent was informed by researcher discussion with the authorised representative and the resident. When the person living with dementia was unable to consent, their authorised representative provided consent, with verbal assent sought from the resident at time of observation.
Results
Project challenges
Resident recruitment
Of the 126 family members invited to participate, 33 expressed interest, and 20 related residents were consented into the project across both homes. We were able to assess 18 of these 20 residents at baseline. This number was adequate for the ethnographic observations undertaken, and to document each resident’s nutrition status, but not for quantitative assessment of changes in nutrition at the end of the project.
We were unable to reach the target sample size of 70 residents living with dementia due to the complex and time-consuming nature of obtaining informed consent from residents with cognitive impairment. Issues included the time involved in working with staff to identify residents meeting the inclusion criteria, time to determine the capacity of residents to provide their own informed consent and the time needed to contact authorised representatives of residents, initially by mail and then personally for consent. Slow responses from authorised representatives necessitated follow-up mail outs. Staff time expended on recruitment activities was partially reimbursed by the project, but staff time for the project remained limited due to their usual clinical- and care-related responsibilities.
Residential aged care home and staff engagement
In this type of participatory project, engagement of the care home management and staff is crucial to planning and implementation as well as to evaluation. Fewer staff (n = 42, of 457) and family members (n = 7, of 126 representatives) than the anticipated 100 combined family/staff members completed the baseline nutrition knowledge survey (approximately 20 minutes), which was administered at the 90-minute Workshop 1 held in each care home. Staff involvement in Workshops 1 and 2 varied but was lower than we expected. This reflected a range of issues, with a key factor being staffing concerns at both care homes, with high turnover of staff and management engaged with the project (including Nutrition Champions) necessitating regular rebuilding of relationships. Additional and related issues were staff having limited time to participate in research, competing priorities on both an individual and organisational level, and limited understanding of participatory research. For example, challenges were experienced with staff taking time ‘off the floor’ to participate in the research workshops, despite strategies to enhance attendance such as catering being offered at workshops, our consultation with key management staff about the most suitable day and time for workshops, and a reduction in workshop length to 1 hour. In Home B, such challenges could not be overcome, and the home exited the project after Workshop 2.
We needed to administer the final survey online at the end of the intervention period for participants in Home A rather than during a face-to-face workshop (see ‘External factors’ below); this presented additional challenges for staff participation in terms of attracting an acceptable response rate in a busy aged care setting. Of the 306 staff and family members emailed an invitation, a total of 40 completed responses were received from 12 staff and 28 family members (13.1% response rate). Due to factors such as the low sample sizes at both baseline and follow-up, we were unable to make comparisons between the datasets. Further highlighting a challenge of conducting online surveys in this setting and the lack of familiarity of staff with research processes, separate response rates for staff and family were unable to be calculated; Home A stated that their automated email platform was unable to differentiate between the roles of those invited to participate which further constrained data analysis.
External factors
The COVID-19 pandemic interrupted the project for 6 months in 2020, preventing our access to participating homes and necessarily diverting staff attention. This represented a greater disruption to research than the earlier, periodically experienced, shorter and localised interruptions to the research and care home access caused by different infectious outbreaks (Utsumi et al., 2010). A change in advice related to guardianship laws also resulted in a temporary halt to recruitment for all relevant University research projects. The project resumed for 2 months at the end of 2020. We replaced the later workshops and the planned post-intervention resident observations and nutrition assessments with an online survey of staff and family members in the remaining participating care home (Home A). This presented its own challenges in terms of attracting a representative response rate in a busy aged care setting, with staff time reduced further by the implementation of additional infection control measures. Additionally, instead of the planned sharing of final project results with key stakeholders at a workshop, project results were documented via a final report distributed to key stakeholders and participants of both homes.
Project facilitators
Nutrition champions
The Nutrition Champions at each home were pivotal to project implementation. They represented catering, leisure and lifestyle, and administration. Nutrition Champions at the remaining home, Home A, worked together to customise and implement action plans focused on the identified need to know more about hydration, liaising with and engaging other staff members as needed, and mentoring and coaching staff (Figure 2 – Activities). A dedicated champion role meant that they were able to focus on and be more proactive around nutrition and hydration within their existing staff role, as well as being recognised by management and nursing staff as key sources of information on these topics.
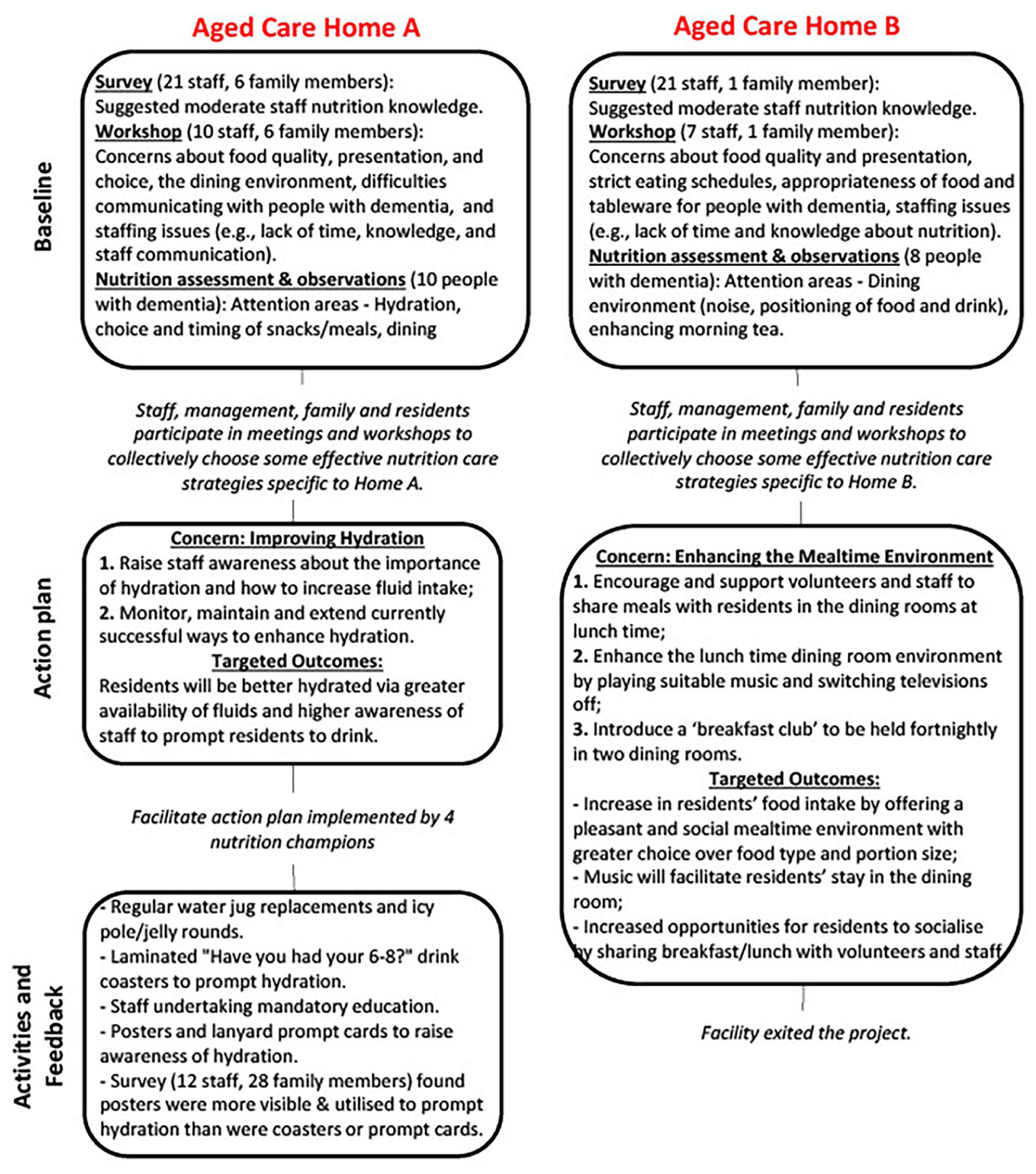
Summary of key MENU activities and evaluation in Aged Care Homes A and B.
Tailored educational resources
The following tailored education resources were developed by the project team and Nutrition Champions:
Coasters with hydration images and key messages to place in resident rooms to prompt hydration and discussion about hydration
Colour posters in various sizes to encourage focusing on fluid requirements, indicators of dehydration and tips to enhance hydration
Credit card-sized plastic lanyard prompt cards for staff on: ● the importance of hydration, indicators of dehydration and tips to improve hydration for people living with dementia, such as offering two clear choices of fluids to drink (e.g., ‘Would you like a hot or cold drink?’), making sure drinks are within reach and using prompts (e.g. ‘Take a sip’) ● the importance of nutrition, indicators of weight loss and tips to improve the mealtime experience for people with dementia, such as using short, direct prompts like ‘Take another bite’, using food aromas to stimulate appetite and encouraging staff, volunteers and family to share meals with residents
4. A PowerPoint presentation about nutrition and hydration, particularly focused on residents living with dementia, which was incorporated into mandatory staff e-learning.
Action plan outcomes
Home A’s action plan was launched at the end of 2019 with an event for staff and residents that included provision of nutritious drinks, high fluid foods and educational resources, presented in a visual display highlighting the importance of hydration. From this point, educational resources were available to all staff and the proposed hydration actions were put into place by the Nutrition Champions, despite COVID-19 interruptions.
At the end of the project, 137 Home A staff members had viewed the PowerPoint presentation on nutrition and hydration that became part of mandatory staff e-learning. Other hydration activities also continued at that time, as initiated by the project. These included enhanced drink rounds, icy pole and jelly rounds, and distribution of educational resources. In these hydration activities, staff were able to implement what they were learning about the importance of clearer, more appropriate communication techniques with people living with dementia, such as using prompts and offering clear choices to encourage hydration.
Despite the lower than anticipated sample size, the collection of baseline data was important to the development of tailored action plans for each care home. The baseline survey found that nutrition knowledge was moderate. The 42 staff participants across the homes – from roles including catering, administration, care workers and nursing – had a mean score of 5.8 (SD = 2.7) out of a maximum achievable score of 11, indicating a need for increased awareness of how to provide effective nutritional care for people living with dementia in aged care. (Note that there were too few staff in any one role to compare across roles.) Survey participants highlighted a range of areas where they felt their care home was doing well (e.g. provision of assistance during meals, availability of allied health practitioners) and some areas where improvements were needed (e.g. 24/7 access to food, staffing levels). Of the 18 residents able to be assessed at baseline, 2 were malnourished, 14 at risk of malnutrition and 2 had normal nutritional status, which also indicated the need for targeted attention to nutrition. Our observations of care practices suggested some key areas for making improvements, including hydration (e.g. prompting to drink), adequacy of snacks between meals and reduced noise levels in dining rooms; these key areas differed in emphasis between care homes. These baseline findings suggested the need for increased awareness of the importance of effective nutritional care for people living with dementia in both homes, supported by tailored nutrition education.
In relation to evaluation of the tailored hydration-related resources in the home remaining in the project (Home A), the majority of staff who participated in the final survey had seen and used the hydration posters (Seen: 100%, Used: 83%), the PowerPoint presentation incorporated into staff e-learning (Seen: 83%, Used: 83%) and plastic lanyard hydration prompt cards (Seen: 75%, Used: 58%). The drink coasters were not as successful (Seen: 33%, Used: 33%). Among family members, the most visible resources were the hydration posters (Seen: 64%, Used: 34%), followed by prompt cards (Seen: 21%, Used: 4%). The coasters and – as expected given the distribution method of incorporation into staff e-learning – the PowerPoint presentation were least visible to family. When staff and family were asked to describe how they had used the resources, most open-ended answers centred around reminding residents to hydrate. Some answers concentrated on remembering to assess (e.g. dry mouth), and learning and reminders in general.
Out of the small number of survey participants (Home A, n = 40), 4 staff (33%) and 3 family members (11%) knew of the activities outside of the educational resources being executed as a part of the MENU project. Participants described drink and icy pole rounds and regular water jug replacements. Half (n = 20) of staff and family member participants indicated they had altered their care practices based on the MENU project resources. The staff noted that they had increased their awareness of residents’ hydration and encouragement of fluid intake, whereas family members stated that they more closely monitored what their loved ones consumed, especially during visits.
Discussion
This participatory action MENU project facilitated the awareness of staff and family members regarding the nutrition and hydration health of people with dementia in residential care, notwithstanding the required adaptation of the project to online education due to the COVID-19 pandemic. Workshops enabled the development of customised action plans for each participating care home and residents, with volunteer Nutrition Champions having a leading role in implementation. These action plans focused on hydration and enhancing the mealtime environment.
Hydration was the key focus of activity for the MENU project as implemented in one aged care home (Home A). Guidelines recommend that adults over 65 years consume 6–8 cups per day of fluids obtained from food and drinks (Masot et al., 2020). Although recent Australian prevalence data are not available, data from other countries suggest that between 1% and 39% of aged care residents have dehydration, with cognitive impairment a significant risk factor (Paulis et al., 2018). A range of intrinsic factors impact on hydration levels among people with cognitive impairment, such as decreased sense of thirst, loss of skills needed to be able to drink from a vessel, swallowing difficulties, forgetting to drink, taste changes, and age-related changes in renal function (Masot et al., 2018; Murphy et al., 2017). The MENU project took a multi-faceted approach to enhance hydration, with a focus on behavioural intervention, in line with current research (Bruno et al., 2021; Cook et al., 2019). Project activities focused on providing increased choice of type of fluids, an increased opportunity to consume fluids, and raising awareness of staff and family members’ understanding of the importance of hydration and how to improve it. Although greater communication about project activities across the care home would have been beneficial, nursing and other staff and family members reported that the activities resulted in nutrition and hydration care enhancements.
Significant challenges hindered more comprehensive implementation of the project. Staff wanted to provide effective nutrition and hydration care for residents, but this was impeded by their not understanding how best to implement evidence-based practice into daily care and not being supported to do so due to an apparent focus on task-based care. Together with the issue of staff turnover typical of the aged care sector in Australia (Isherwood et al., 2018; Mavromaras et al., 2017), these issues speak to the need for management to better understand and support evidence-based care (Lam et al., 2018) and the critical role of nurses being given the opportunity to lead initiatives (Micklewright, 2024; Watson et al., 2020). This aligns with Australia’s dementia policy framework, the National Dementia Action Plan 2024–2034 (Australian Government, 2024), that aims to build residential aged care workforce capability to deliver quality person-centred and evidence-based care through training and supportive organisational culture.
Although crucial to include people living with dementia in research (O’Connor et al., 2022), an Australian study found that most researchers in this area agree that it is difficult or time-consuming to recruit participants with a diagnosis of dementia (Ries et al., 2020). When conducting research in the residential care setting, staff investigators need adequate time to recruit participants and to participate in the research, and to be reimbursed for their time. It would be useful to understand why authorised representatives are or are not interested in being involved in specific research projects, particularly as they may function as informal gatekeepers for participation of residents living with dementia (Ries et al., 2020). Different long-term strategies have been posited to facilitate engagement of people living with dementia in clinical trial research, such as advance research consent, although research is needed around the relationship of these strategies to the vulnerability of this population (Beattie, 2009; Beattie et al., 2019; Holden et al., 2018; Ries and Mansfield, 2021; Soofi, 2022). Timely recruitment of participants is particularly important in the context of research in residential aged care where residents may be experiencing the later stages of dementia (Dobson et al., 2020). Researchers also need to consider the impact of infection control measures on project implementation in these settings (Usher et al., 2021; Utsumi et al., 2010), ensuring alternative methods of data collection are feasible, and building in additional time for such contingencies.
Counteracting the range of challenges experienced in the project, there were some important facilitators, all of which related to the participatory nature of the project design. These were the Nutrition Champions, the use of action plans and the development of tailored resources and education. The staff who were prepared to take a leading role in the research by acting as Nutrition Champions facilitated the implementation of action plans. Nutrition Champions have been posited in other research as potential key players in aged care homes to promote nutrition and person-centred care (Byles et al., 2009; Cave et al., 2021; Gaskill et al., 2009; Perry et al., 2011), although they are not yet common in this setting (Cave et al., 2021). Staff in these positions need support from management, as well as from colleagues, to ensure they can take on this additional activity consistently without becoming overburdened (Byles et al., 2009; Cave et al., 2021; Masso et al., 2011). The use of participatory action plans developed by staff and researchers working together from an understanding of the context and needs of a particular care home is an approach which has been found valuable for other issues in residential care, such as falls prevention and end-of-life care, and may enhance engagement and ownership of proposed changes to care practices (Andrews et al., 2012; Rowley and Taylor, 2011). The tailored resources and education collaboratively developed by the project team, dietitian and Nutrition Champions to enhance understanding of nutrition and hydration, particularly the posters and PowerPoint presentation, were viewed as useful. Previous research on a related aspect of nutrition and hydration, dysphagia, has found that tailored materials are effective to influence care in the residential care setting (Wu et al., 2022). The participatory approach taken in the development of tailored resources and education for the MENU Project may be useful for other aged care homes, so that they can be adapted to be specific to the key issues present in each organisation. This is one approach to help fill a gap in community participation in design of resources and education, as recognised by Australia’s National Dementia Action Plan (Australian Government, 2024).
Limitations
A limitation was that MENU was undertaken only in two care homes from the same region of Australia; hence, the challenges and facilitators identified may not all be readily transferable to other regions. However, the publications cited in this paper outline comparable challenges and facilitators in aged care homes in other regions and countries, including other Australian states, the United Kingdom and the United States (Edwards et al., 2003; Hall et al., 2009; Lam et al., 2018; Law and Ashworth, 2022). This suggests our findings may have broader relevance.
Conclusion
Our study found that nutrition and hydration were problematic for residents in the participating residential aged care homes. This was reflected in moderate staff nutrition and hydration knowledge and the high level of risk of malnutrition among resident participants. Working with staff in a participatory approach, guided by Nutrition Champions and the nursing staff involved in execution of the project (project team, resident recruitment, survey and workshop participation), may help to engage stakeholders and encourage action in this area. The identification of facilitators and challenges in implementing this project may also be useful information for those planning research in other areas of evidence-based practice in this setting. The study has highlighted that there are many barriers to the translation of evidence-based research into improved care practices for nurses and other aged care staff. Staffing issues and financial stressors, a focus of the Australian Royal Commission into Aged Care Quality and Safety (Pagone and Briggs, 2021), continue to be concerns. In line with previous research (Lam et al., 2018), the study also emphasises the need for management support to address organisational barriers affecting the implementation of evidence-based practice in residential aged care. Despite the range of challenges faced by the project, the MENU approach helped nursing staff and other stakeholders work together with residents and families to address nutrition and hydration issues. The MENU approach has in-built adaptability to suit local conditions and needs. It is readily transferable to implement future research in other aged care homes to evaluate its impact on nutrition and hydration care for residents more comprehensively while applying the lessons learned in this study.
Key points for policy, practice and/or research
The provision of adequate nutrition and hydration remains problematic in residential aged care homes, particularly for residents living with dementia, highlighting a need for improved staff awareness and nursing leadership in this area.
Participatory research approaches are important to engage key stakeholders and sustain change. They include researchers working in partnership with residents, family and nursing, allied health and other staff, such as involvement of nursing staff in planning and other stages of research. However, there are challenges to consider when planning and conducting participatory research in residential aged care. These include recruitment of residents living with dementia, organisation and staff engagement and external factors such as the COVID pandemic.
Some challenges to conducting participatory research to enhance evidence-based practice may be ameliorated by implementing practices such as development of champion roles, action plans, and tailored resources and education.
Management support is needed to address organisational barriers affecting the implementation of evidence-based practice to improve nutrition and hydration in residential aged care, such as enabling staff to take time ‘off the floor’ to attend to non-core activities like educational research workshops. Such support would be likely facilitated by policy changes to address staffing issues and financial stressors, and recognition of the role of nurses in guiding participatory action research.
Footnotes
Acknowledgements
We wish to acknowledge the following researchers who were involved in the implementation of the MENU project: Ms Andrea Price, Dr Kathleen Doherty, Professor Liz Isenring, Ms Amber Johnstone and Ms Jane McDougall. We also wish to acknowledge the Nutrition Champions, management, staff, residents and family members at both participating residential aged care homes.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tasmanian Community Fund (Grant number 35Medium00044) and the Wicking Dementia Research and Education Centre.
Ethical approval
The project received approval from the Human Research Ethics Committee (Tasmania) Network (Ref. No. H0017136) on 08 March 2018.