
Abstract
Background:
Uptake of advance care planning (planning future care) in care homes remains low. There is a sparsity of research exploring hospice-led advance care planning education delivered to care home staff.
Aims:
To explore and evaluate advance care planning education delivered by hospice specialists to care home staff in the United Kingdom.
Methods:
A cross-sectional online survey disseminated via national-organisations and social media from August 2023 to April 2024. Participants included staff working in care homes and hospices (registered nurses/healthcare-assistants/managers).
Results:
Eighty-eight valid responses were received. Most respondents working in care homes strongly agreed (56.6%) or agreed (35.8%) that education increased their knowledge and confidence when engaging in advance care planning. About 71.4% of hospice staff and 50.9% of care home staff noticed changes to advance care planning following the COVID-19 pandemic, which included earlier initiation of discussions, and more focus on resuscitation. Identified barriers included, short-staffing and high staff-turnover in care homes. Despite high commitment, a lack of funding and resource capacity hindered hospice staffs’ ability to provide education.
Conclusion:
Education delivered by hospice specialists is important in supporting care home staff to develop knowledge and confidence to engage in advance planning discussions. Future evaluative research is needed to measure the efficacy/sustainability of hospice-led advance care planning education.
Keywords
Introduction
Residents living in care homes have complex health and social care needs, often living with greater complex comorbidities, including frailty and dementia (Gordon et al., 2014). Care homes provide generalist palliative and end-of-life care services amongst other services which are delivered by a generalist team (Care UK, 2025). In this study, the term ‘care home’ refers to both residential and nursing homes, which provide food and accommodation, 24-hour care and assistance. Nursing homes additionally provide care by registered nurses. Staff working in both nursing and care homes are involved in advance care planning.
Illness trajectories of residents living in care homes can be uncertain and unpredictable, and deterioration and death can occur gradually or suddenly (Barclay et al., 2014; Spacey et al., 2018). Given the often uncertain and complex trajectories of dying amongst residents, it is vital that staff working in care homes who are involved in advance care planning (registered nurses and care assistants), together with residents and families engage in regular advance care planning conversations to ensure residents receive end-of-life care in line with their wishes. Advance care planning is described as a process ‘enabling individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with relatives and healthcare providers, and to record and review these preferences if appropriate’ (Rietjens et al., 2017: 546). It has long been established that registered nurses are uniquely placed to have conversations about death and dying, but recognised that more needs to be done to improve their engagement in advance care planning (Rietze and Stajduhar, 2015).
Globally, the Word Health Organization (WHO), despite having no specific directives has long promoted advance care planning and encouraged its implementation in health and social care settings such as care homes (WHO, 2016). Despite the promotion of advance care planning in care homes, international explorations have evidenced a lack of training and skills within the care home workforce as a major barrier to advance care planning (Dixon and Knapp, 2018, 2019; Rietze and Stajduhar, 2015). In the United Kingdom (UK), several recent seminal policy papers have emphasised that all health and social care staff involved in advance care planning should have regular access to up to date training/educational opportunities to ensure they feel prepared and are able to sensitively initiate advance care planning conversations (National Palliative and End of Life Care Partnership, 2021; Universal Principles for Advance Care Planning, 2022). Despite these policy recommendations, concern has been raised that the UK care home workforce do not receive sufficient training in order to be prepared for advance care planning (Care Quality Commission, 2021). The lack of training has been shown to inhibit care home staff’s ability to engage in meaningful care planning discussions with residents and families (Spacey et al., 2021a).
A scope of current literature helps explain these findings, reporting that current educational provision to care home staff is not of a standard that could be expected to alter clinical behaviour and is often short lived in terms of delivery length (Anstey et al., 2016; Spacey et al., 2020). Advance care planning education and its quality are important because care home staff are expected to have regular ongoing advance care planning conversations with residents and families so plans can be updated if care needs and preferences change (Mathie et al., 2012). Furthermore, care home staff need to be able to navigate cases where residents lack mental capacity, and a legally appointed decision-maker engages in the care planning process on their behalf (The Mental Capacity Act, 2005). Literature has also shown that repeated conversations about death and dying as part of advance care planning can take an emotional toll on care home staff if not properly supported and trained (Spacey et al., 2021a, 2021b).
Evidence suggests that hospice specialists are some of the best placed to provide care home staff with vital knowledge and education to support palliative/end-of-life care delivery in care homes due to their specialist training, regular exposure to death and dying and advance care planning (Hospice UK, 2023; NHS England, 2023; Park et al., 2019). Despite this, there is a sparsity of research exploring and evaluating advance care planning education delivered by hospice specialists to generalist care home staff. Consequently, developing a better understanding of hospice-led advance care planning education, and the barriers and opportunities to delivery in care homes may be key to improving future advance care planning practice.
Thus, given the vital role of advance care planning in care homes, policy drivers and the gap in research, there is a need to explore and evaluate advance care planning education delivered by hospice specialists to care home staff. Specifically, exploring the experiences and practices of hospice staff who are involved in developing and delivering advance care planning education, as well as the experiences of care home staff receiving it. The findings from this study will have the potential to inform both regional and national policy in relation to advance care planning education.
Methods
Aim
To explore and evaluate advance care planning education delivered by hospice specialists to care home staff in the United Kingdom.
Design
A cross-sectional online survey was used to explore advance care planning education/training delivered by hospice staff to care home staff. Although the data were not integrated, the survey adopted a nested mixed method design which involved collecting both qualitative and quantitative data concurrently, with the quantitative element being embedded within the larger qualitative (Castro et al., 2010). The survey had two pathways, one for care home staff (focusing on the receival of education) and another for hospice staff (focusing on the delivery of education). The care home staff pathway consisted of n = 12 closed and n = 7 open questions, and the hospice pathway consisted of n = 11 closed and n = 10 open questions. The survey contained both closed and free-text questions and was reported in accordance with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines for reporting e-surveys (Eysenbach, 2004).
Sample
This study included a mix of both purposeful and snowballing sample strategy. Purposeful sampling was utilised as potential participants needed to meet the eligibility criteria of:
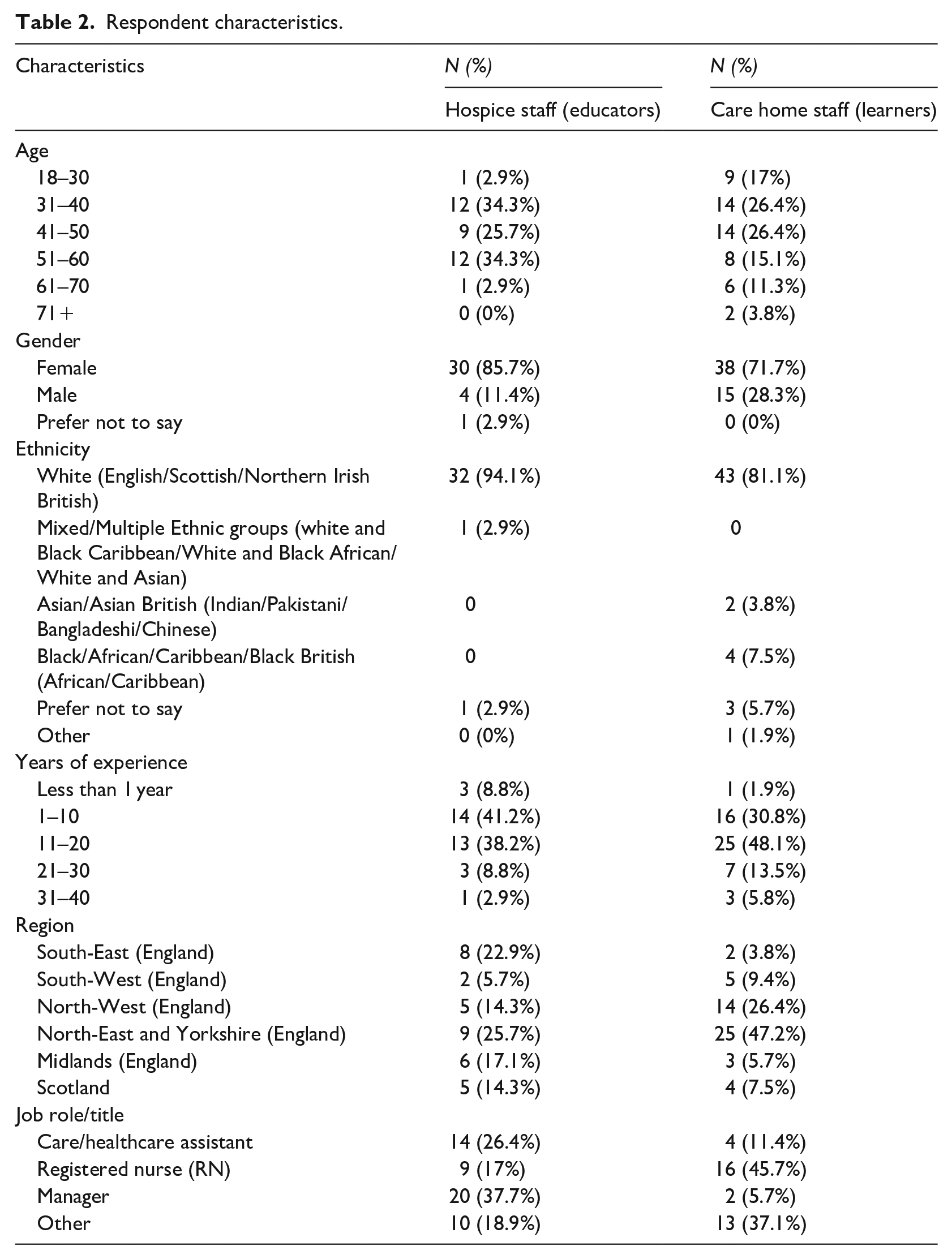
Working in care homes (residential or nursing) or hospices (see Table 1). These included registered nurses, care/healthcare assistants and managers (see Table 2 for breakdown).
Experience in the delivery or receival of advance care planning education.
Setting descriptions.
Respondent characteristics.
In addition, a snowballing technique was also used where potential participants were invited to share the survey with their colleagues and appropriate contacts. Furthermore, the study also incorporated an open method of recruitment; in that, anyone with access to the survey link was able to participate if they received or delivered advance care planning education. Given the nested survey design with numerous free-text qualitative questions and requiring participants to have either received education from hospice staff or delivered advance care planning education to care home staff, a statistically significant sample was not sought. The numbers for the survey were not capped or restricted.
Recruitment
The survey link and information about the study were widely shared via Hospice UK (which is a UK charity with no direct patient care, Hospice UK, 2025) and the National Institute for Health and Care Research (NIHR) Enabling Research in Care Homes (ENRICH, 2024). Personal networks and social media were also used to disseminate the survey. No incentive to complete the survey was offered. All potential participants were required to answer mandatory screening questions to ensure they met the eligibility criteria and complete a consent form.
Data collection
The online survey was developed using Joint Information Systems Committee (JISC, (2023) software, see Supplemental Material 1. The survey used closed and free-text questions, and the survey questions and sections were developed from our previous research (Spacey et al., 2021b; Spacey and Porter, 2023). Pilot testing was carried out by a range of stakeholders (n = 5), including hospice educators, frontline staff and a Palliative Medicine Consultant who provided feedback which led to changes to question wording, structure and the overall survey layout. Participants could only complete the survey once, and it was only available in English language. The survey was open from August 2023 to April 2024.
Data analysis
Qualitative data from the free-text entries was downloaded into Microsoft Excel and analysed using a six-stage guide in reflexive thematic analysis (Braun et al., 2022; Byrne, 2022). Reflexive thematic analysis was chosen to better acknowledge and understand our own role as researchers in shaping the interpretation of the qualitative data. Two researchers read and re-read the free-text comments to familiarise themselves with the data. Codes were independently identified and recorded. Coding was inductive as new codes were identified, and deductive as codes were aligned to the central research aim. The final codes and sub-themes and themes were then agreed on and developed through consecutive discussions between two of the research team (AS and VH), and any discrepancies were settled by the third researcher (KS). This process was used to sense-check ideas and explore multiple interpretations of the data in a reflexive manner to develop richer interpretations rather than reach a consensus.
Quantitative data were downloaded from JISC (2023) into Microsoft Excel and cleaned to remove any duplicates or incomplete entries. Entries were deemed to be sufficiently complete when all four sections of the survey had been attempted, even if all available questions had not been answered. Descriptive statistics were prepared using Microsoft Excel to analyse respondents’ demographic data (e.g. age, gender, ethnicity) and preferences (e.g. preferences on education delivery modes) by A.S. and K.S. The quantitative analysis was integrated within relevant qualitative themes. Demographic data such as age and gender were used to contextualise and provide further depth to our analysis (see Table 2 for breakdown).
Ethics
Approval was granted by the Health and Society Ethics Committee at the University of Salford (REF: 11719 19.07.2023). Informed consent was provided by all the participants in the study.
Results
A total of 88 valid responses were included in our analysis (17.4%). The total study sample comprised 35 hospice staff and 53 care home staff. Table 2 summarises the characteristics and demographics of the respondents.
From the free-text questions, three themes were identified: Perceptions and experiences of advance care planning and education; Design, content and evaluation of education; Contextual factors inhibiting and promoting change.
Theme 1: Perceptions and experiences of advance care planning and education
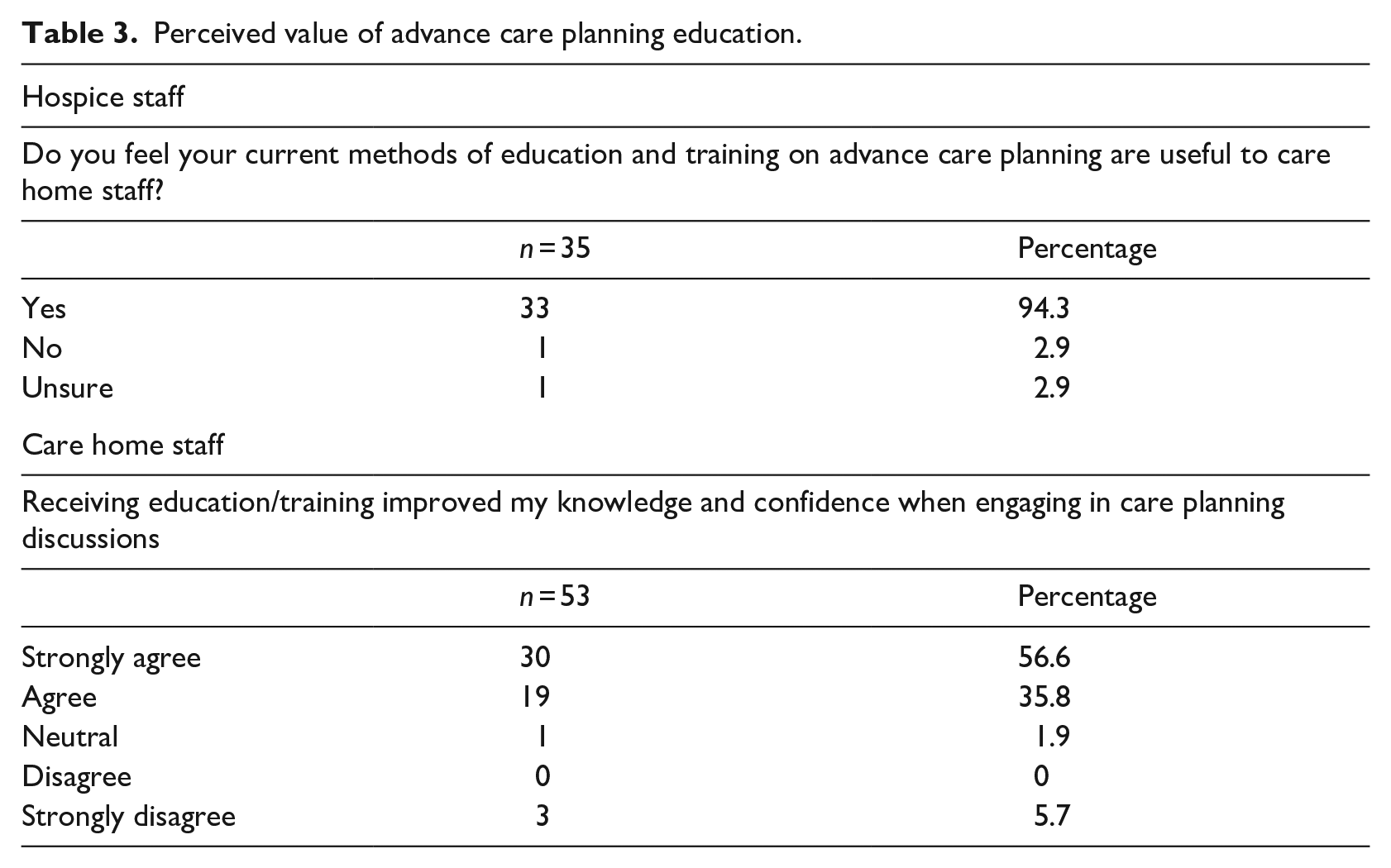
The importance of advance care planning education was well recognised by most respondents with 33 (of 35; 94.3%) hospice staff feeling that their delivery of advance care planning education is useful to care home staff. Similarly, most respondents working in care homes strongly agreed (56.6%) or agreed (35.8%) that education increased their knowledge and confidence when engaging in advance care planning discussions (Table 3).
Perceived value of advance care planning education.
Analysis of the free-text responses shows that care home staff felt education on advance care planning helped build their confidence to engage in sensitive discussions with residents and family members about death and dying. Furthermore, it was identified that education helped care home staff develop a better awareness of the importance of advance care planning.
Gives me confidence to participate with sensitive topics and an awareness of the importance of advance planning. (Female care team lead working in care home) Gives a much better insight into what is required for advanced care planning and has helped with having the discussions with family members. (Female care home manager)
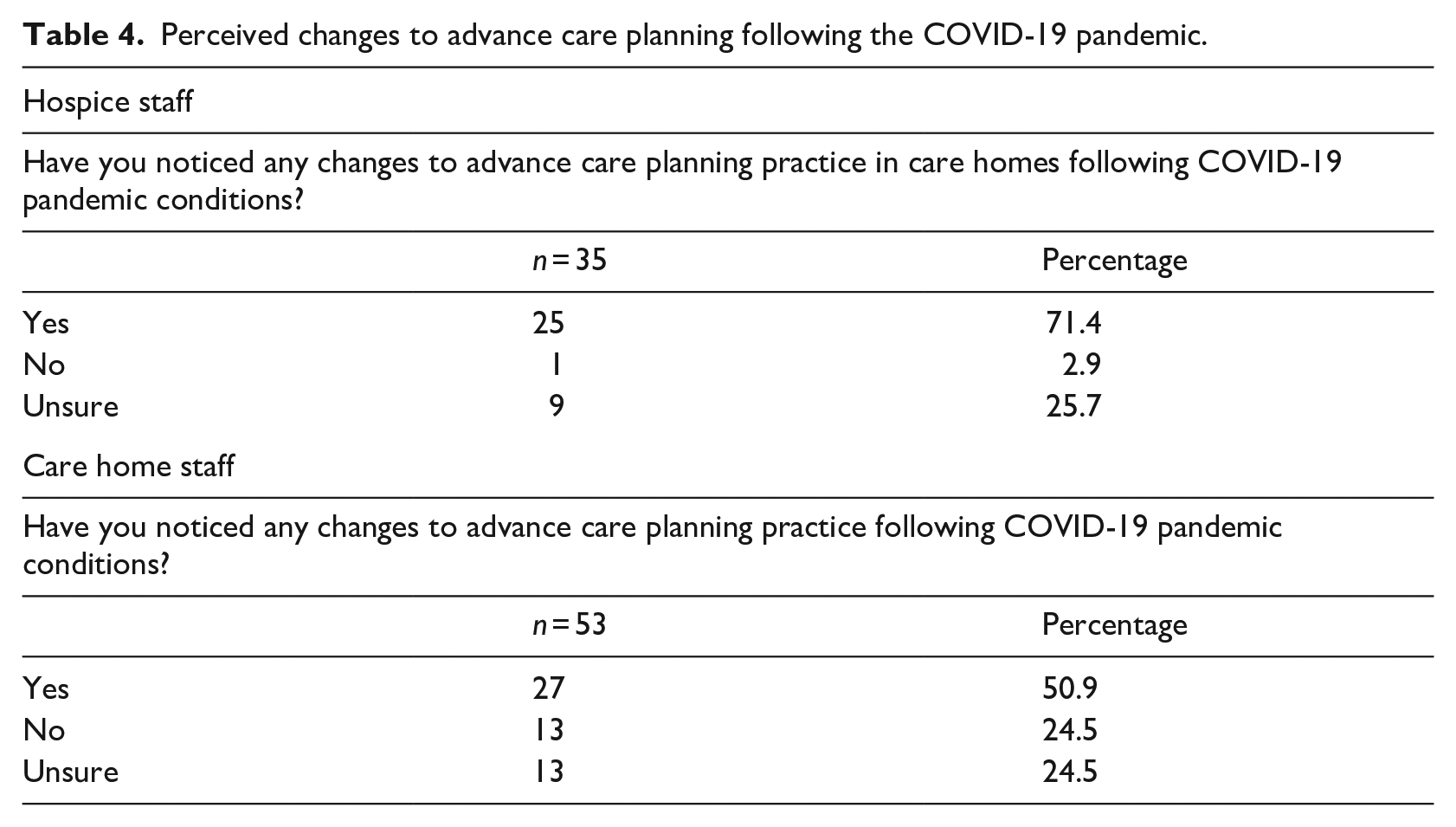
Analysis suggests that perceptions and attitudes towards education were influenced by respondents’ changing perceptions and attitudes of advance care planning following the COVID-19 pandemic. Although our data suggest that hospice staff were more aware of the changes compared to care home staff; 25 (of 35; 71.4%) hospice staff and 27 (of 53; 50.9%) care home staff indicated that they had noticed changes in advance care planning practice following the pandemic (Table 4).
Perceived changes to advance care planning following the COVID-19 pandemic.
Analysis of the free-text responses reveals several perceived changes to advance care planning practice following the COVID-19 pandemic. For example, it was apparent that because many residents died (often unexpectedly) during the pandemic without having an advance care plan containing adequate information on what to do and wishes in cases of sudden deterioration and death. Subsequently, it appears that some care home staff have become more aware of the importance of advance care planning, and what can happen if advance care plans contain inadequate information, or are not in place at all.
We lost a lot of residents during the pandemic and did not have the information in place to action what these residents would have like. [Female registered nurse working in a care home] We are now more aware that it is important to have an advance care plan in place for all residents as you never know what is going to happen. [Female care home manager]
Our analysis suggests that the increased awareness of the importance of advance care planning in the years following the pandemic has led to an increased appreciation and recognition for hospice-led advance care planning education. Consequently, hospice staff believed more care home staff were now willing to engage in their training.
Increased profile and recognition of the importance of [advance care planning] ACP likely due to the COVID-19 Pandemic, meaning that care homes are more proactive in their approach and are therefore seeking out training and education opportunities to facilitate their learning and confidence in supporting their residents with future wishes conversations. [Female specialist nurse practitioner working in a hospice] Care home staff more willing to engage in training, understand its relevance to their setting. [Female clinical educator working in a hospice]
In addition to increasing the profile of advance care planning, it was evident that the pandemic led to changes to advance care planning education. Specifically, hospice staff cited that their education now focused much more on facilitating early proactive advance care planning discussions with residents (rather than reactive). It was also felt that care home staff themselves have become much more proactive in their approach to advance care planning and as a result hospice staff have increased their regular training sessions to facilitate need.
I think care homes are becoming more proactive in their approach to [advance care planning] ACP on the back of the COVID pandemic and the training that I deliver focuses on a proactive approach rather than a reactive approach. [Female registered nurse working in a hospice] I feel staff are more aware of the need to plan ahead and have everything recorded due to the high number of deaths in COVID-19. We have just tried to offer even more regular sessions as a result. [Female hospice manager]
As well as care home staff, it was frequently expressed that residents and families are now also more open to talking about death and dying in a way that was not evident pre-pandemic. Consequently, care home staff highlighted having more advance care planning discussions with residents and families.
There is more emergency care planning arranged which details what that person would like and how we can provide this. More families are facing the topic of death and making preparations such as which funeral directors they would like their loves ones to be taken. [Female registered nurse working in a care home] I think more people are talking about death and dying more openly following COVID because we were forced to. [Male care assistant working in a care home]
Despite encouraging more proactivity, our analysis suggests that there is still a need to shift perceptions that advance care planning pertains to the final days before death shifting to a focus about choices for the future. Hospice staff expressed a perception of a taboo about talking about death and dying amongst some care home staff, following the pandemic and advance care plans were seen as synonymous with death.
Starting to use the term future care planning to get away from it just being about dying as this stops people doing it. There is a lot of fear post pandemic in care homes around death and blame. [Female clinical lead working for a hospice]
Furthermore, it was expressed that a taboo culture around advance planning and death could partly be related to care home staffs’ personal and cultural beliefs. Thus, it was acknowledged that hospice-led advance care planning education could do more to incorporate mechanisms to better support care home staff attitudes and fear of death and the advance care planning process, especially following the pandemic.
Acknowledging and thinking about personal and cultural beliefs of care home staff and how this can impact on their ability to talk about [end of life] EOL issues. Most care home staff were trained overseas and represented a wealth of perspectives to death. [Female registered nurse working in hospice]
Theme 2: Design, content and evaluation of education
Hospice staff used a variety of methods to inform the design, content and structure of advance care planning education packages. Most commonly, hospice staff used national policy and research to inform their designs, as well as their own expertise. Moreover, respondents frequently cited working in close partnership with care home staff to develop their curriculum and establish local needs.
I was involved in the designing and delivery, along with my team. We utilised national guidance as a reference. . . [Female hospice manager] We spent time developing the curriculum through doing [training needs analysis] TNAs across a number of care homes and worked in partnership with them to develop the wider syllabus and the content of the training sessions. [Female educator working in a hospice]
Despite the variety of design influences, analysis identified that the content and curriculum of hospice-led advance care planning education tended to be consistent and focused on how/when to initiate advance care planning, enabling sensitive compassionate conversation, understanding the documentation and difficulties around engaging in sensitive conversations about death and dying.
I have devised [advance care planning] ACP training for care home staff including compassionate conversations techniques and a reflective practice session so practitioners get a chance to reflect on their experiences. [Female registered nurse working in a hospice] Having the difficult conversations about the end of life, when to open up these conversations, advocating for residents in crisis situations, completing online system notes. These are all areas where care home staff can struggle. [Female practice educator working in a hospice]
However, respondents identified that despite content and topics being similar, following the pandemic, a greater emphasis has been placed on the importance of advance care plans being timely, as well as discussions related to ‘do not resuscitate orders’.
The principles are the same, but more emphasis is placed on the importance of [advance care planning] ACP being done correctly and timely. [Female educator working in a hospice] We also probably emphasise more about the discussions needed around do not resuscitate orders. [Female hospice manager]
Furthermore, there has been a greater adoption of hybrid delivery methods following the pandemic. Despite in-person education delivery still being preferred over online for hospice (20 of 35; 57.1%) and to a lesser extent, care home staff (22 of 53; 41.5%; Table 5), free-text responses suggest that delivery preferences are complex and influenced by a range of factors including content and the local needs of the care homes.
Delivery modes.
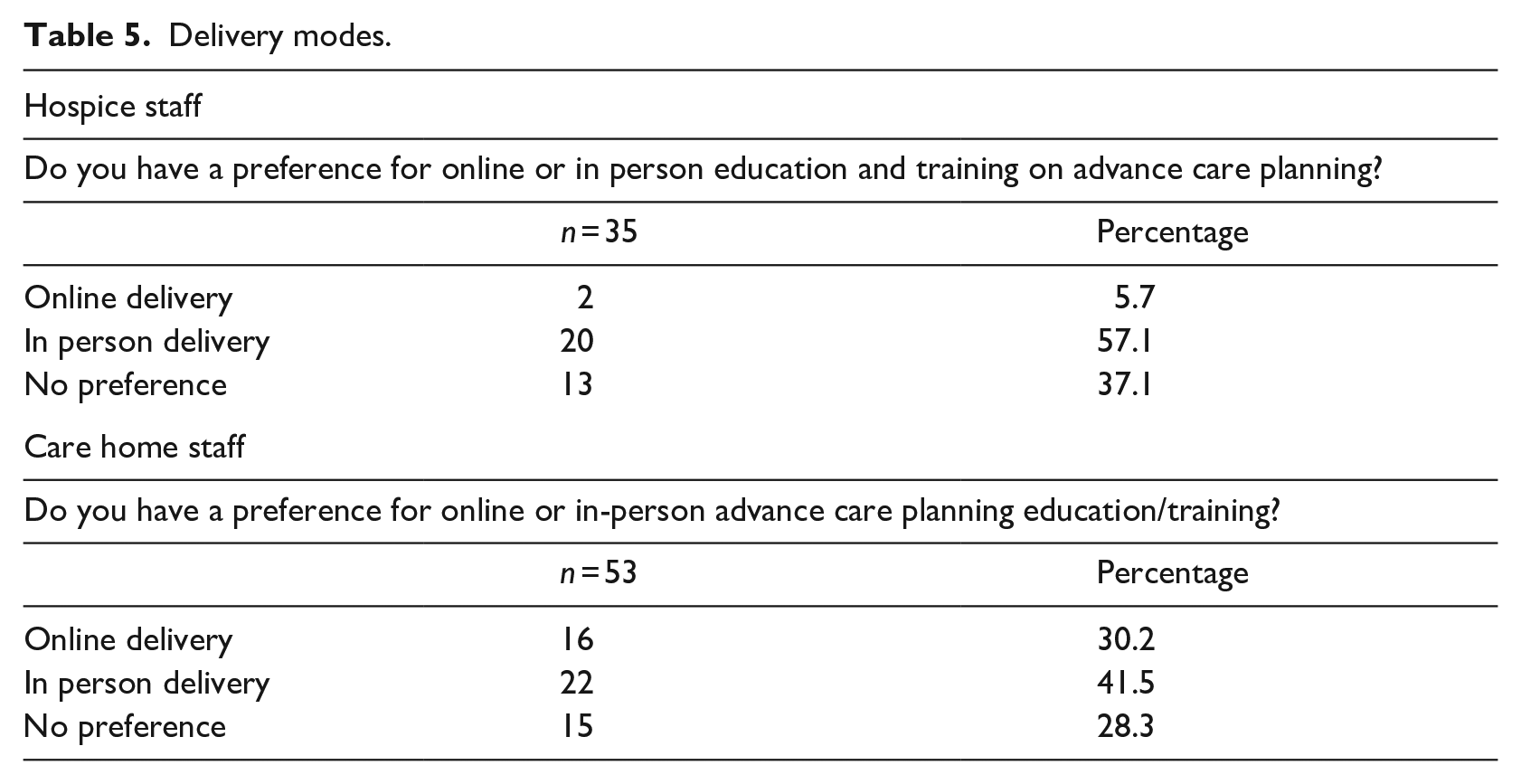
For instance, it was described that in-person delivery is more appropriate for the practical aspects such as how to initiate conversations, whereas online education/training tended to be preferred when learning about policy and key theory that can be rewatched.
Depends, some of the more personal stuff is best in person and the more process and policy stuff is best done online and recorded so we can rewatch. [Male care assistant working in a care home]
Hospice respondents nonetheless recognised the difficulty of measuring the success of different delivery methods, and how different approaches translate into practice. Specifically, they highlighted the most common methods used to evaluate education were asking care home staff or getting them to fill out evaluation forms following education.
The feedback we receive on our evaluation forms suggests that the attendees find this training useful. [Female registered nurse working in a hospice] We always ask and the staff in home are grateful and have said it’s improved their confidence talking to residents. [Female registered nurse working in a hospice]
Despite education being well received, hospice staff felt that self-reported increases in confidence and measuring increases in the numbers of advance care plans were not a sufficient to fully understand and evaluate education/training.
Training is often well received, but it is difficult to measure how this translates into practice. Over time we have seen an increase in the amount of [advance care plans] ACP being recorded for residents but there are many other factors also involved in this. [Female practice educator working in a hospice]
Theme 3: Contextual factors inhibiting and promoting change
Analysis of the free-text responses revealed several perceived barriers to education delivery. The main barrier highlighted by both hospice and care home staff was low staffing levels in care homes which prevented care home staff from attending and having time for education sessions. Furthermore, persistently high levels of staff sickness in care homes appeared to worsen staffing issues.
The usual staffing issues preventing attendance. Staff will book on sessions and then sometimes don’t turn up or they get pulled into work if someone has phoned in sick. [Female hospice manager] Time and opportunity; our home is also short staffed. [Female care assistant working in a care home]
Further analysis suggests that staff shortages have led to increases in the workload and expectations put on care home staff. Inflated workload and expectations were deemed to prevent care home staff attending education either through a lack of time and exhaustion or not having the cover to enable them to attend, particularly at managerial level.
The increasingly heavy workload . . . Staff are exhausted and therefore less keen to attend study sessions in their rest time. [Female clinical educator working in a hospice] Time off the job, People filling in for me whilst I’m studying. [Female care home manager] Some staff are not available to receive the training. [Female registered nurse working in a care home]
In addition to short staffing and increasing workloads, analysis identified that high staff turnover in care homes also negatively impacted on hospice-led education. Hospice staff highlighted that despite training, knowledge was lost when care home staff left the home.
. . .sometimes turnover of staff in care home settings meaning that knowledge is not maintained in specific care home setting. [Female clinical educator working in a hospice]
Similarly, care home staff expressed high numbers of staff leaving preventing training opportunities due to poor sustainability of knowledge within care homes.
Staff leaving is a big thing here and it prevents training. [Male care assistant working in a care home]
Nonetheless, several opportunities were identified to mitigate these barriers. For example, delivering ongoing education on advance care planning was one method proposed to better support the sustainability of knowledge within care homes with high staff turnover. Despite this, it was evident that often education is delivered as a ‘one-off’ session.
High staff turnover in homes means training needs to be ongoing but is often a ‘one off’ training programme. [Female clinical educator working in a hospice]
Another opportunity identified was the use of online/e-learning rather than face-to-face to increase engagement. It highlighted that online delivery often reached wider audiences, especially in care homes that have staffing challenges.
Not all staff can attend face-to-face meetings due to other commitments – online delivery reaches out and can engage more staff. [Female registered nurse working in a care home]
It was however evident that the hospices that did provide ongoing more sustainable educational offerings were able to recognise the importance of this considering high staff turnover in care homes.
We are a dedicated education and support service that provide a sustainable offer to care homes. That’s crucial as the workforce changes a lot. [Female hospice manager]
Aside from staffing barriers, the commitment and attitudes of care home managers towards education and training was highlighted as both potential barrier and opportunity. It was described that managers acted like a gatekeeper, and those who were committed and understood the importance of education/training were more likely allocate staff and support more sustainable educational offerings.
I think a lot depends on the managers commitment to education and training too, we have some managers who allocate staff onto lots of sessions and then others who don’t engage with the education offer at all. [Female hospice manager]
Being able to work with care home staff and managers to establish and agree on learning needs was identified as a key tactic to getting managers’ support and commitment, especially for education/training which requires considerable time from care home staff.
Our programme is over 5 days so requires buy in from care home managers. However, we have successfully run 3 courses with another one planned. Initially working out what training they needed was tricky, as they weren’t sure what they needed. [Female research nurse working in a hospice]
Several barriers were also evident from the hospice side. It was highlighted that a lack of funding for advance care planning training, combined with a lack of staffing and resource capacity inhibited hospice staffs’ ability to support more care homes, despite being highly motivated and committed.
But it is the lack of funding rather than a loss of commitment. Most hospices are still keen to support their local care homes with this teaching but lack the capacity to do so. [Female educator working in a hospice]
Furthermore, funding offered to hospices tended to be fixed term, meaning that support could only be provided to a certain number of care homes for a specific period of time.
The funding for this project was limited to 12 months and 12 care homes. [Female registered nurse working in a hospice]
Discussion
Care home staff, including registered nurses and care assistants, felt that education/training on advance care planning delivered by hospice specialists was essential to building their confidence and knowledge to be able to initiate and sustain sensitive discussions about death and dying with residents and families. Hospice and to a lesser extent, care home staff, felt the perceived value of advance care planning and consequently education associated with it increased in the years following the COVID-19 pandemic due to residents dying (often unexpectedly) in care homes without having an advance care plan in place. Additionally, pandemic experiences also prompted change in educational focus. Specifically, more emphasis being placed on having ‘do not resuscitate’ discussions and supplying care home staff with the confidence and knowledge to adopt a more proactive approach to initiating planning conversations at earlier stages with residents and families. However, an increased fear of death and blame culture post-pandemic seems to have heightened some care home staffs’ reluctance around advance care planning.
Nonetheless, our findings identified several barriers hindering sustained change. The most common being staff shortages and turnover, which often meant that care home staff could not be released to attend training. However, we identified that in cases where hospice staff worked closely with care home managers to agree on learning needs and capabilities, contextual barriers such as staffing could be partly mitigated. For example, offering shorter hybrid education sessions to enable more staff to attend, and delivering ongoing education rather than ‘one off’ sessions to address staff turnover. Yet, a lack of funding and capacity for hospice-led education hindered the facilitation of ongoing education and support offerings for care homes.
Our findings suggest that advance care planning education delivered by hospice specialists plays an important role in care homes. However, despite care home staff reporting perceived improvements in their communication skills and confidence to initiate and sustain effective advance care planning discussions, hospice staff found it difficult to measure how this translated into practice. A scope of the literature on advance care planning education across multiple settings reveals similar self-reported perceived improvements in knowledge and confidence and an improved ability to discuss end-of-life care issues (Anstey et al., 2016; Chan et al., 2019). Subsequently, three systematic reviews have cast doubt on the sustainability and reliability of these self-reported outcomes; highlighting the lack of high quality randomised controlled trials and longitudinal studies exploring the long-term efficacy of advance care planning education (Anstey et al., 2016; Chan et al., 2019; Gleeson et al., 2021). Being able to develop effective education is vitally important given registered nurses (including those working in care homes) are uniquely positioned to have advance care planning discussions; however, engagement has long been limited due to the lack of education opportunities (Rietze and Stajduhar, 2015). Thus, there is a need for future high quality trail research to establish the efficacy and sustainability of hospice-led advance care planning education delivered in care homes.
The need to re-evaluate advance care planning education following the pandemic is important, given our findings highlight that education has evolved with the changing needs of care homes. For instance, we identified an increased educational focus on ‘do not resuscitate’ discussions and promoting a more proactive approach to initiating planning conversations at earlier stages following the pandemic. Several studies conducted during the pandemic noted a stronger tendency for residents and families to focus on topics such as resuscitation during advance care planning in care homes due to them experiencing more death and dying (Brugge et al., 2022; Vellani et al., 2021; Ye and Fry Land Champion, 2021). Furthermore, the threat of the pandemic encouraged earlier and more frequent advance care planning discussions (Spacey and Porter, 2022). Thus, the findings presented in our study suggest that these changes to practice have been sustained and incorporated into advance care planning education delivered by hospice specialists.
Despite the positive influences of the pandemic on advance care planning, we identified several barriers hindering education delivery, all of which appeared to have worsened following the pandemic. The most prominent being staff shortages and high staff turnover. Akin to our findings O’Brien et al. (2016) who evaluated an educational intervention, found that in care homes with higher staff turnover, attendance was negatively impacted, with some homes sending inappropriate staff to attend (i.e. too junior to cascade and share knowledge). Similarly, a systematic review of education interventions found staffing and resource constrains led to the adoption of single ‘short-lived’ education interventions been implemented in care homes on pragmatic grounds, rather than effectiveness criteria (Spacey et al., 2019). Despite this, our findings suggest that ongoing education may be more appropriate in the context of high staff turnover to ensure more opportunities for new staff to be trained. Previous research also suggests that ongoing education enabled content to be updated over time to meet the changing needs of the care homes (Badger et al., 2012; Kinley et al., 2017). Furthermore, our findings suggest that utilising online/e-learning delivery methods in place of or in tandem with traditional face-to-face methods may support better engagement. A recent literature review exploring e-learning in healthcare similarly reported increases in engagement and accessibility for some, however recognised that more research is needed to better understand individual learning characteristics (Ardestani et al., 2023).
Despite the evidence, our findings reveal that a lack of funding and capacity within the hospice sector prevented ongoing care planning education, and meant it was often fixed term/limited support. The lack of funding for hospice-led education is concerning because research has consistently highlighted that uptake of advance care planning in care homes is low, predominantly because of a lack of knowledge and skills within the care home workforce (Wendrich-van Dael et al., 2021). Gilissen et al. (2017) who conducted a systematic review of advance care planning in care homes also found that sufficient knowledge and skills are essential to the successful and sustainable advance care planning practice in care homes (Gilissen et al., 2017).
Yet, despite the clear need for education/training in care homes, advance care planning intervention studies in care homes are few and heterogeneous (Flo et al., 2016); there is a limited evidence-base that can be used to evidence the need for future funding. Thus, evaluative research of hospice-led education interventions is urgently needed to establish the need for increasing funding to support care homes improve their advance care planning practices. However, given the resource constraints and chronic underfunding of the hospice sector in the UK (Hospice UK, 2024), it can be argued that hospice staff are not best placed to provide care homes with education, and other sectors need to do more. In the years following COVID-19, more efforts have been set up to support care homes with advance care planning. For example, Cousins et al. (2022) evaluated online training and information for care staff and family members (developed and delivered by a multi-professional team) regarding advance care planning during COVID-19, and found immediate tangible impacts on staff confidence and family member involvement, leading to more engaged care planning conversations. However, our findings suggest that hybrid delivery rather than purely online was preferred by care home and hospice staff, and preferences for online and in-person were influenced by a range of factors including content and the local needs of the care homes.
In addition, our findings have shown that despite funding limitations, hospice staff were still positive and motivated to provide education and support to care home staff. Furthermore, statutory funding for the hospice sector in the UK has recently increased with large-scale investment by the government (Department of Health and Social Care, 2024). Thus, while increased support from other sectors should be encouraged, there is still a strong motivation and a clear need for hospice-led education in care homes.
Another post-pandemic barrier identified was care home staffs’ fear of being blamed for resident deaths which led to some care home staff being reluctant to engage in advance care planning. This is unsurprising given it has been widely reported care home staff have expressed negative feelings during the pandemic such as not being valued and blamed for residents’ deaths (The Queen’s Nursing Institute, 2020). However, difficulties discussing death and dying have long been reported, for example, Spacey et al. (2021a) found registered nurses and care assistants’ unmet emotional needs led them to avoiding discussions about death and dying with residents. These findings suggest that more needs to be done in terms of education and support to better manage care home staffs’ fears and reluctancies around death and dying during advance care planning.
Limitations
Given the first author’s background in advance care planning research, there was a potential for subjectivity. However, reflexivity was considered throughout the study from design through to analysis via the piloting of the survey questions, reflexive communication during analysis and regular discussion. Moreover, geographical clustering of respondents is also acknowledged with elevated uptake in England. However, given the small numbers of respondents, it was not possible to analyse regions individually. Furthermore, the self-selecting sample may not present experiences and views representative of the entire UK hospice and care home workforces.
Although both closed and free-text questions were used, the closed answer questions produced largely yes/no answers; utilising a wider array of quantitative question designs such as Likert scales may have improved the insight generated. Nonetheless, free-text answers provided rich in-depth qualitative data to achieve the research aim. Lastly, although the survey gained valuable insight from both care home and hospice staff, residents and their family experiences were not collected. We thus recommend future research to address this gap.
Conclusion
Findings suggest that education delivered by hospice specialists is important in supporting care home staff to develop the knowledge and confidence to engage in advance planning discussions. Furthermore, we identified that advance care planning education has evolved following the pandemic with more emphasis on proactively initiating planning conversations at earlier stages with residents and families, as well as more focus on resuscitation. Despite this, we found that there is still a need to shift perceptions that advance care planning is just about the final days and in fact is about choices for the future. Hospice staff still felt there was a taboo amongst some care home staff, especially following the pandemic viewing care planning as just being about death and final days. Thus, we recommend that hospice-led advance care planning education does more to support care home staff attitudes and fear of death and the advance care planning process in the wake of the pandemic.
Short staffing and high staff turnover hindered care home staffs’ ability to attend education. Similarly, despite high commitment and motivation, a lack of funding and resource capacity hindered hospice staffs’ ability to supply ongoing education to care homes. This is important as we found that ongoing education rather than ‘one off’ sessions were more likely to mitigate the loss of knowledge and skills in care homes with high turnover. Moreover, it was suggested that utilisation of online/e-learning delivery methods may help mitigate some of the identified contextual factors.
Lastly, we highlight the need for future high-quality evaluative research to measure the efficacy of hospice-led advance care planning education delivered for care homes. There is also a need to capture residents and families’ experiences to gain a deeper understanding of their evolving care needs to inform future interventions.
Key points for policy, practice and research
Care linked to death and dying is a key part of nursing care in care home (both residential and nursing) settings.
Education delivered by hospice staff was perceived by care home staff to be vital in supporting them to develop the knowledge and confidence to engage in advance planning discussions.
Providing ongoing education rather than ‘one off’ sessions was suggested as more likely to mitigate the loss of knowledge and skills in care homes with high turnover.
Short staffing and high staff turnover hindered care home staffs’ ability to attend education.
Lack of funding for hospice-led advance care planning education was found to result in hospice staff delivering limited or ‘one off’ sessions rather than being able to support care homes over a longer more ongoing basis.
Future research is encouraged to better mobilise the knowledge of hospice specialists in advance care planning to improve nursing care delivered in care homes.
There is a need for future high-quality evaluative research to measure the efficacy of hospice-led advance care planning education delivered for care homes.
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871251365027 – Supplemental material for An exploration of advance care planning education delivered by hospice specialists to care home staff: a cross-sectional UK survey
Supplemental material, sj-pdf-1-jrn-10.1177_17449871251365027 for An exploration of advance care planning education delivered by hospice specialists to care home staff: a cross-sectional UK survey by Adam Spacey, Amanda Stamper, Sarah Owens, Katy Szczepura and Vanessa Heaslip in Journal of Research in Nursing
Footnotes
Acknowledgements
None.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval was granted by the Health and Society Ethics Committee at the University of Salford (REF: 11719 19.07.2023). Informed consent was provided by all the participants in the study.
Supplemental material
Supplemental material for this article is available online.