
Abstract
Background:
Cold application is a non-pharmaceutical method that has been shown to be effective in relieving pain by slowing down or blocking the conduction of peripheral nerves.
Aim:
This study aimed to evaluate the effect of cold needle use during arteriovenous fistula cannulation on cannulation-related invasive pain.
Methods:
A semi-experimental, self-controlled, and double-blind study was used. The cannulation procedure was performed with room temperature needles during the first three haemodialysis sessions and with cold needles during the next three sessions. Patients were those treated in the haemodialysis unit with arteriovenous fistula of a state hospital in Turkey between April and May 2024.
Results:
The study was completed with a total of 33 patients. The mean pain score of the three sessions was found to be statistically significantly lower when a cold needle was used (5.08 ± 0.67) compared to the use of a room temperature needle (6.68 ± 0.68; 1.78 ± 0.94; 95%CI: 1.45–2.12; p < 0.001).
Conclusions:
Cold needle use is recommended during arteriovenous fistula cannulation to reduce invasive pain. Cannulation with cold needle is a non-pharmacological, easy to apply, and cost-effective method. These findings have potential for informing policy and procedure in effective pain management.
Background
Patients experience cannulation-related pain in the range of 10–80% during haemodialysis treatment, which is performed by cannulating through an arteriovenous fistula (AVF) approximately 312 times a year (Alzaatreh and Abdalrahim, 2020). Pain felt during cannulation is due to the activation of pain-sensitive nerve endings in the tissue caused by the skin tear when the needle is inserted (Ozen et al., 2022). Stress, depression, insomnia, and irritability were more commonly reported in patients who experienced pain during AVF cannulation compared to those who did not experience pain (Shabandokht-Zarmi et al., 2017). If this pain becomes chronic, it will negatively affect the patient’s compliance with dialysis treatment and lead to a deterioration in their quality of life (Sadeghpour et al., 2023). Despite advances in its management, pain still remains a serious problem (Abunab et al., 2021; Alabacak and Arslan, 2024; Elzeky et al., 2024). There are varying findings in the literature regarding the factors influencing pain during cannulation. Factors contributing to pain include the direction of the needle cone tip, cannulation technique, arterial needle orientation, presence of fistula stenosis and infection, and the proficiency of the healthcare provider conducting the cannulation (Lok et al., 2020). For example, Akyol Durmaz et al. (2018) found no significant difference in pain scores based on needle cone tip direction, whereas other studies indicated lower pain scores when the needle cone tip was downward compared to upward placement (Ozen et al., 2022). Furthermore, the cannulation technique used can cause pain. Among commonly used techniques for AVF cannulation: area, rope-ladder, and buttonhole; each has distinct advantages and drawbacks in terms of pain and complications. With area cannulation, access is confined to just two small zones – the arterial and the venous areas – and cannulations are always performed systematically within the same site. By contrast, the rope-ladder technique distributes cannulation sites evenly along the entire length of the drainage vein (Sousa et al., 2023). The buttonhole technique, where repeated needle insertion at the same site forms a permanent track into the fistula, has been adopted in several dialysis units. This technique has been advocated because it is associated with less pain compared to the rope-ladder technique (Sousa et al., 2023), although other studies have reported higher pain scores in buttonhole method patients compared to those treated with the rope-ladder technique (Chow et al., 2011; MacRae et al., 2012; van Loon et al., 2010).
Pharmacological and non-pharmacological methods have been used in the studies evaluating the methods employed to reduce invasive pain experienced due to cannulation (Alzaatreh and Abdalrahim, 2020; Kosmadakis et al., 2021). The use of non-pharmacological methods is preferred because they are cheaper and cause fewer side effects and complications (Jafari-Koulaee et al., 2020). Cold application, which is one of the non-pharmacological methods used, is effective in relieving pain by slowing down or blocking the conduction of peripheral nerves. In addition, it stimulates touch receptors by activating the gate control mechanism, increases the release of endogenous opioids and stops the pain by ensuring that the nerve impulses due the cold is transmitted to the Delta fibres. It also reduces tissue blood flow, tissue metabolism, and muscle spasm by causing vasoconstriction. This causes a local anaesthetic effect called cold-induced neuropraxia (Nadler et al., 2004). Although studies conducted on haemodialysis patients have revealed that cold application is effective in decreasing pain, further studies have been suggested due to the small sample groups and deficiencies in the varied methodologies. Cold application in these studies was performed to the area 1 cm above the fistula or between the thumb and index finger of the opposite arm, using an ice pack and an ice-filled glove for 2–10 minutes (Aghajanloo et al., 2016; Al Amer et al., 2017; Ghoreyshi et al., 2018; Golda et al., 2016; Issac and Namboothiri, 2016; Jose and Lobo, 2015).
Many methods such as bags filled with crushed ice, commercially available ice and gel packs and cold spray application are used for cold application (Nadler et al., 2004). In order for ice and gel packs to provide effective anaesthesia, the application period must be long. The sprays are flammable and may cause skin sensitivity, and those containing fluor components result in environmental concerns (Mawhorter et al., 2004). Another method used to prevent needle-related invasive pain is cold needle application. Some studies have shown that the pain felt by patients is decreased by using a cold needle for subcutaneous and intramuscular injections (Denkler, 2001; Jancy, 2019; Thomas et al., 2019), whereas a systematic review has found that neither cold nor room temperature needles were effective in reducing injection-related pain when administering vaccines (Hogan et al., 2010). A study that has shown cold needle application to be effective in reducing cannula-insertion-related pain in dialysis patients is by Alvarez et al (2004). Alvarez et al. (2004) reported in their study with 25 patients that cannulation with a cold needle (−8°C) reduced pain compared to cannulation with a needle at room temperature; however, there are deficiencies regarding the design and methodology of the study. The study did not include details on the method of needle cooling, the technique used to measure needle temperature, the rationale for using needles at −8°, exclusion criteria, and the individuals responsible for performing the cannulation. To address this gap, we examined the effect of cold needle use during fistula cannulation on cannulation-related invasive pain undergoing haemodialysis therapy.
Methods
Study design and participants
This was a quasi-experimental, self-controlled, and double-blind study. The study included patients who were treated in the haemodialysis unit of a state hospital in Turkey between April and May 2024. The nurse who assessed the patient’s pain after cannulation was blinded to whether a room-temperature or cold needle had been used, and the nurse performing the cannulation was likewise unaware of whether the needle provided by the researcher was at room temperature or cold. Hence, the study was conducted using a double-blind design. The sample calculation of the study was determined by using the G*Power 3.1.9.4 software program (Germany). For the sample size calculation, we used the study by Shafii et al. (2019), which evaluated the effect of cold spray application before fistula cannulation on cannulation-related pain, as a reference due to the absence of similar studies in the literature. The difference between mean pain intensity values was planned to be evaluated with the Paired Sample t-test, and the effect value was predicted to be 0.60 with a 95% confidence interval and 95% power, resulting in the calculation that 31 participants would be sufficient for the sample of this study where the patients constituted their own control group. Considering possible losses from the study (hospitalisation, death, changing dialysis centre, etc.), it was planned to include a total of 35 patients.
Inclusion and exclusion criteria
Haemodialysis treatment at the dialysis centre is administered in three sessions on Mondays, Wednesdays and Fridays, and in two sessions on Tuesdays and Thursdays. Patients who presented to the dialysis centre on Mondays and Tuesdays and provided informed consent to participate in the study were included by the researchers. All enrolled participants were patients aged 18 years and older; had been treated with haemodialysis for at least 3 months, three times a week and for 4 hours per session; did not have a psychiatric disorder that would prevent communication, and volunteered to participate in the study. Patients who were known to present difficulties when cannulating the fistula (requiring multiple cannulations), had a history of hematoma or stenosis in the AVF, had an infection at the fistula site, took painkillers within 3 hours of treatment, and did not want to participate in the study were excluded. When repeated cannulations are performed on the same patient, the tissue sensitivity or psychological fear induced by the previous procedure may amplify the perception of pain in subsequent attempts. For this reason, patients who attempted more than one cannulation were excluded from the study.
Intervention protocol
On the first day of data collection, a questionnaire regarding the participants’ descriptive characteristics was completed by the researchers during face-to-face interviews with the 35 patients. The dialysis area should be air-conditioned to achieve temperatures of 70°F–72°F (21.1°C–22.2°C) and humidity levels (Setting up of Hemodialysis Unit, 2020). The dialysis centre where the study was conducted is also climate-controlled to continuously maintain the required temperature and humidity range for dialysis units.
Usual needling procedure (room temperature needle)
Routine practice was continued for three sessions and fistula cannulation was performed with a needle at room temperature. The researcher retrieved the needles and handed them to the nurse for the cannulation procedure. Once the cannulation site was cleaned with an appropriate antiseptic solution, it was allowed to dry for at least 30 seconds. The arterial needle was inserted at an angle of 30°–45° to the skin surface, at least 5 cm away from the fistula anastomosis (BC Renal Hemodialysis Committee, 2020; Ozen et al., 2022). Pain assessment after cannulation was made by a nurse working in the dialysis centre who did not know which patient was cannulated with a cold or room temperature needle and who was not involved in the research. After each cannulation, the patients’ pain level was evaluated using a visual analogue scale (VAS). The venous needle was always inserted after the arterial needle. The same nurse performed all cannulations for a given patient.
A period of 2 days was used as the wash-out period. During the next three dialysis sessions, the patients underwent fistula cannulation with a cold needle. This study was carried out according to the SQUIRE 2.0. SQUIRE guidelines are intended for reports that describe system level work to improve the quality, safety and value of healthcare, and used methods to establish that observed outcomes were due to the intervention (Supplemental File 1).
Cold needle usage
The needle used for fistula intervention was left in its packaging, and it was only removed from its packaging and used by the nurse when it was to be inserted into the patient. The needles were kept for one day in their own bags on the refrigerator shelf, where the temperature was controlled, at the dialysis unit. The needle was removed from the refrigerator before its use and kept on the nurse’s table. The temperature for impairing pain sensation should be below 4°C (Ernst and Fialka, 1994). In studies where cold application was performed with ice packs, it was observed that the temperature of the ice pack varied between 0°C (Gorji et al., 2014), 0–2°C (Sinha et al., 2015), and 4°C (Soydan and Uğraş, 2021). So, the selected temperature for the needle in this study was the same as previous studies (Jancy, 2019; Thomas et al., 2019).
A test of temperatures to standardise the method
In this study, the target temperature for the needle was set at 0–2°C, consistent with previous research (Jancy, 2019; Thomas et al., 2019). However, upon removal from the refrigerator, the temperature of the needle body (excluding the hose and wings), as measured with a digital thermometer, was found to range −4 to −8°C. Therefore, in order to ensure the needle temperature reached the desired range before cannulation and to standardise the procedure, a preliminary temperature test was conducted. In this test, three needles stored in the refrigerator were taken out, and their temperatures were measured immediately using a digital thermometer. The temperature of each needle was then monitored and recorded at 5-minute intervals until it dropped to the 0–2°C range. The results showed that the temperature of the needles decreased to the desired range within 3 minutes at room temperature. Based on this observation, all needles used in the main study were removed from the refrigerator exactly 3 minutes before cannulation to maintain consistent application conditions.
For the control part of the study cannulation was attempted for a total of three sessions with the needle kept at room temperature for the first three sessions. Since the patients came for the next haemodialysis session 2 days later, these days were considered as the wash out period. This 48-hour gap helps ensure that any residual effects – physiological or sensory – that might affect pain perception have returned to baseline, so measurements in the second phase reflect only the new condition. For the next three sessions, cannulation was attempted with a needle that was removed from the refrigerator and had a temperature of 0–2°C. The same nurse attempted the cannulation in each session. The researcher removed the needles from the refrigerator and allowed them to reach room temperature before handing them to the nurse for cannulation. The nurse, wearing gloves, performed the cannulation without touching the metal part of the needle, so she was unaware of whether the needle had been refrigerated or not. The patients were unaware of whether a cold or room temperature needle was used on them.
Variables and instruments
Data were collected with questionnaires on the descriptive characteristics of the participants and a VAS. Pain was assessed through self-report and use of a VAS. The questionnaire on the participants’ descriptive characteristics form was a semi-structured form, which the researchers developed after reviewing the relevant literature (Alzaatreh and Abdalrahim, 2020; Abunab et al., 2021; Jafari-Koulaee et al., 2020; Aghajanloo et al., 2016; Ghoreyshi et al., 2018). The questionnaire included a total of 10 questions regarding the sociodemographic and medical data of the participants. The patients’ existing comorbidity statuses were obtained from their medical records. These medical records are maintained by the responsible dialysis physician, and the diagnoses are determined by the physician. The data regarding the patients’ comorbidity statuses were retrieved directly from the records completed by the physician, avoiding reporting bias from the patients or nurses. The researchers completed the questionnaire within approximately 10 minutes through face-to-face interviews with the patients during the second hour of treatment. Turkish validity and reliability of the VAS scale was originally developed by Price et al. (1994) was conducted by Eti Aslan (2004) by evaluating the presence of pain in patients in the postoperative period. The scale is evaluated from 0 to 10 as 0 = I have no pain and 10 = I have unbearable pain. A total of six pain assessments were made by a nurse independent of the study by using VAS.
Data analysis
The IBM SPSS Statistics for Windows, Version 25.0 (SPSS; IBM Corp., Armonk, NY, USA) software was used to manage the data. The ‘Kurtosis–Skewness value’ was used to investigate the compliance of the measurement values with a normal distribution. Mean ± standard deviation was used to present the descriptive statistics of continuous numerical variables, and number (n) and percentage (%) were used to present the categorical variables. The paired samples test and Repeated Measures ANOVA were used to analyse the variables by standard statistics. A p value <0.05 was considered to be statistically significant when making statistical decisions. This trial is registered at the ClinicalTrials.gov website as NCT06418009.
Ethical considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study was approved by the local ethics committee (Meeting Date: 02.04.2024, Decision No: 2024/50). All necessary institutional permissions and the participants’ written informed consent were obtained.
Results
Two patients were excluded from the study due to repeated needle interventions, and the study was completed with a total of 33 patients. The mean age of the participants was 56.82 ± 13.70 years, the mean duration of haemodialysis treatment was 48.94 ± 23.21 months and the mean fistula age was 37.85 ± 16.59 months. The fistula was seen to be located in the radiocephalic area and to be the first fistula in 78.8% (Table 1). The patients did not experience any skin problems due to the cold needle application.
Descriptive characteristics of the subjects (n = 33).
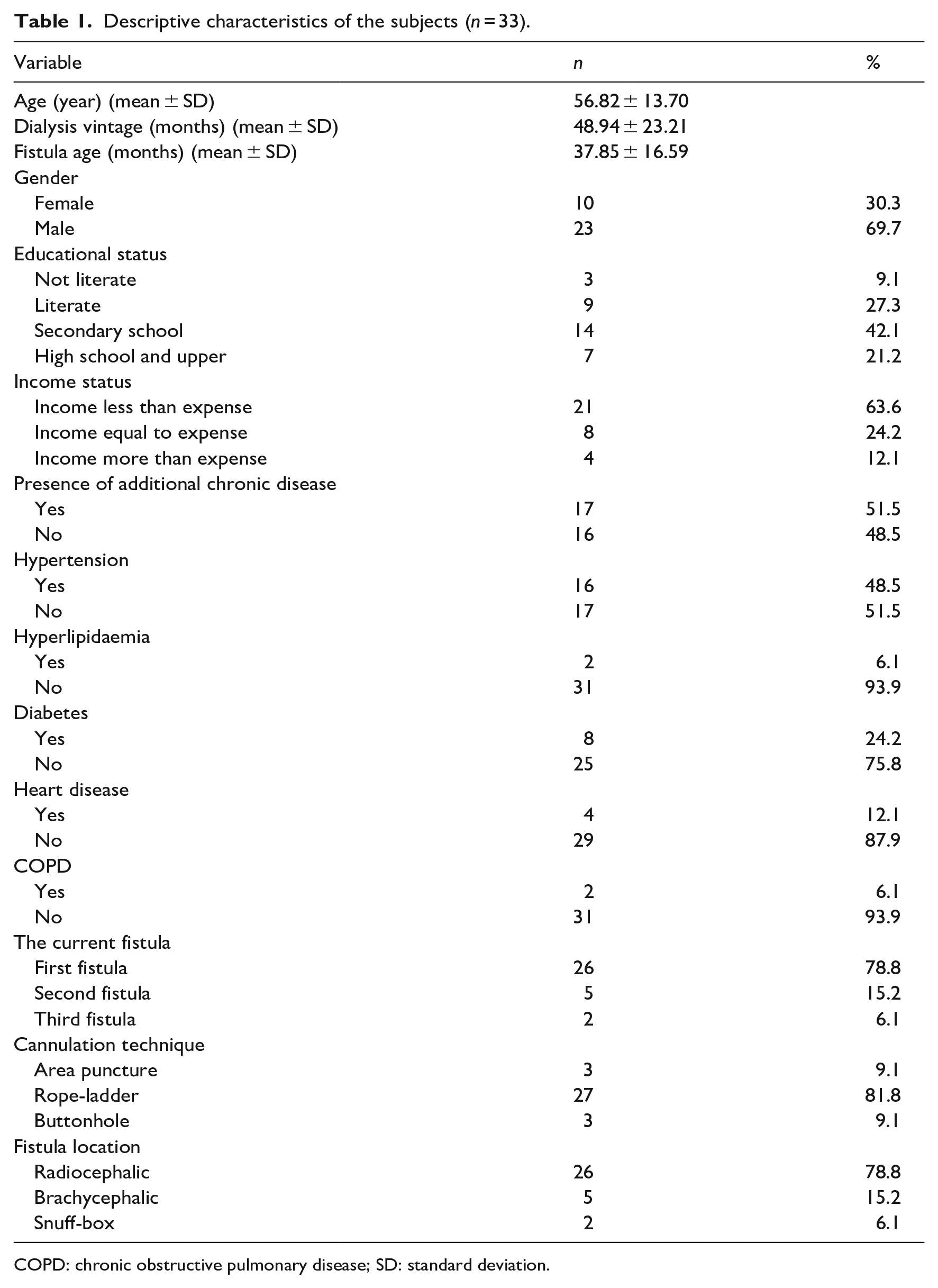
COPD: chronic obstructive pulmonary disease; SD: standard deviation.
In the cold needle application, the VAS scores were 5.48 ± 0.90 in the first session, 4.97 ± 0.84 in the second session and 4.79 ± 0.69 in the third session. Repeated measures ANOVA revealed a statistically significant difference between the sessions (p < 0.001). Additionally, the partial eta squared (ηp²) value was 0.392, indicating a large effect size. In the room temperature needle application, the VAS scores were 7.12 ± 0.74 in the first session, 6.79 ± 0.92 in the second session and 6.70 ± 0.91 in the third session. Repeated measures ANOVA showed no statistically significant difference between the sessions (p = 0.181). The mean pain score of the three sessions was found to be statistically significantly lower when a cold needle was used (5.08 ± 0.67) compared to the use of a room temperature needle (6.68 ± 0.68; 1.78 ± 0.94; 95% CI: 1.45–2.12; p < 0.001; Table 2; Figure 1). None of the patients experienced any complications or reported discomfort during the cold needle procedure.
Change of cold and room temperature needle applications over time according to the VAS (n = 33).
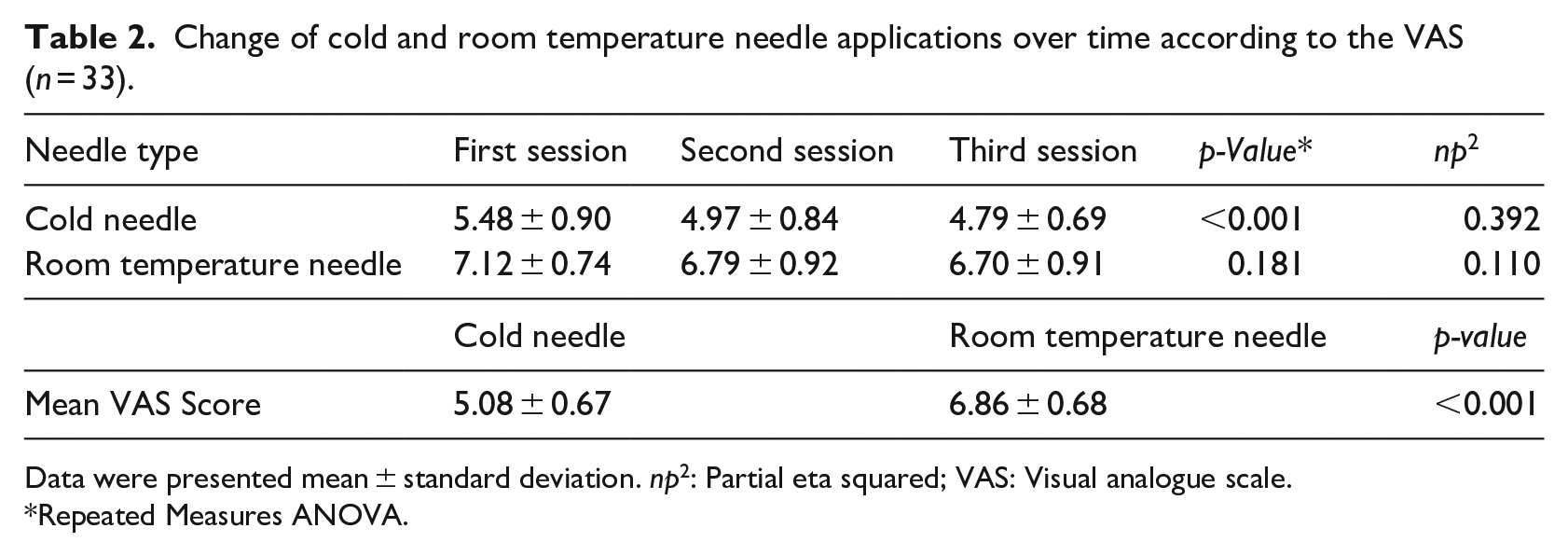
Data were presented mean ± standard deviation. np2: Partial eta squared; VAS: Visual analogue scale.
Repeated Measures ANOVA.
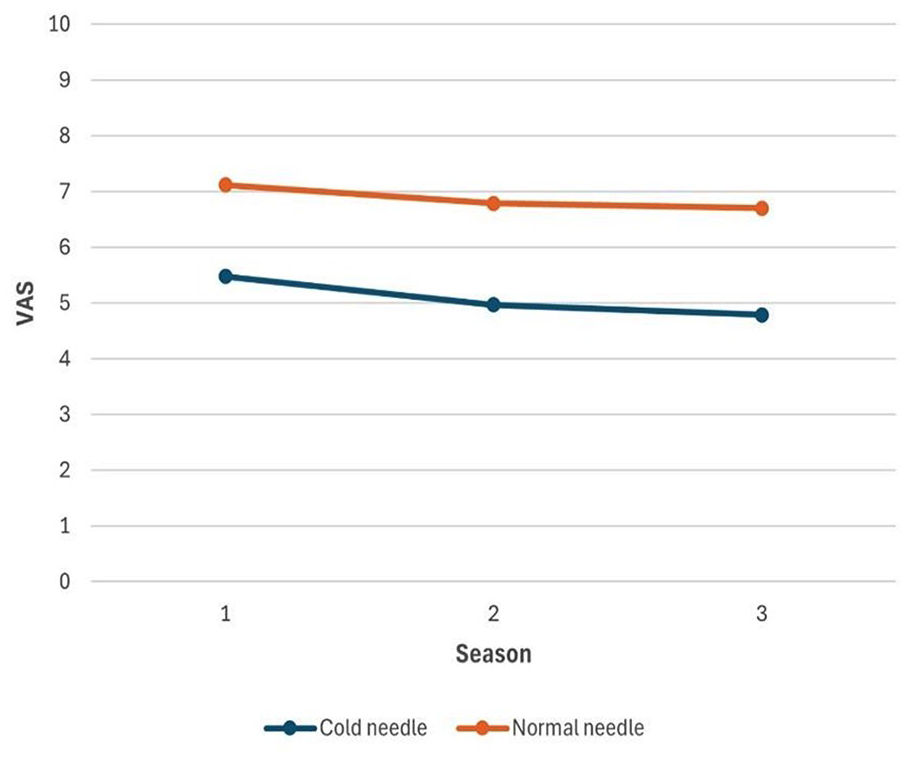
Comparison of the pain scores according to the needle temperature.
Discussion
We found the use of a cold needle during arteriovenous fistula cannulation to reduce invasive pain in a statistically significant manner compared to the use of a needle at room temperature in this study.
Cryotherapy is one of the non-pharmacological methods used to reduce cannulation-related pain in patients with a fistula. This application is performed with various methods such as bags filled with crushed ice, ice and gel packs or cold spray application. For cryotherapy to be effective, the application time varies between 10 and 20 minutes (Aghajanloo et al., 2016; Al Amer et al., 2017; Golda et al., 2016). Cannulation with a needle at 0–2°C was found to reduce invasive pain more than cannulation with a needle at room temperature in this study. Using a cold needle was found to decrease the cannulation-related pain more than the use of a room temperature needle in study of Alvarez et al. (2004). However, it was not specified how the room temperature and cold needles were administered in the study conducted with 25 patients, and it was also not reported whether both the room temperature needle and the cold needle were administered to all patients. In the current study, cannulation was performed with both room temperature and cold needles so that each patient could be their own control. The reason for the decrease in invasive pain after the use of a cold needle could be activation of gate control with cold application. Thus, transmitting cold-induced nerve stimuli to the Delta fibres could be decreasing the invasive pain.
Cryotherapy is one of the interventions used in several studies to alleviate the AVF puncture-related pain. The studies have highlighted the efficacy of cryotherapy methods such as ice packs (Aghajanloo et al., 2016; Al Amer et al., 2017; Golda et al., 2016; Kavipriya, 2016; Sivagami, 2011; Gouda et al., 2023), ice cubes wrapped in gloves (Sundar et al., 2017; Dehghan et al., 2023), skin cooling device (Demırağ and Kulakaç, 2025) and cubes of ice were placed in a plastic bag and covered with a layer of cotton in reducing cannulation pain (Arab et al., 2017). However, these methods often require longer application times (5–20 minutes), which may be impractical in busy haemodialysis settings. In a study using only a skin cooling device, a 5-second application time was required (Demırağ and Kulakaç, 2025). In the study of Golda et al. (2016) cryotherapy started 10 minutes before and in the study of Sundar et al. (2017), it was started 5 minutes before the needle was inserted into fistula and continued until the insertion of needle into fistula. In studies of Aghajanloo et al. (2016) and Sivagami (2011), the duration of cryotherapy before the needle was inserted into fistula was 10 minutes, and in the study of Aghajanloo et al. (2016), cryotherapy was also performed for about 2−3 minutes after the needle was inserted into fistula. In our study, the short application time unlike other non-pharmacological methods used to reduce pain in haemodialysis patients where cannulation-related invasive pain is often experienced. Once the needle is removed from the refrigerator, it is used on the patient after waiting for approximately 3 minutes at room temperature, which also saves time for the healthcare personnel performing the cannulation. In addition, the patients do not feel the cold effect created by ice bags, ice packs or cold spray applications used in cryotherapy procedures.
In this study, a statistically significant reduction in pain scores was observed across the three sessions in which cold needle application was performed. Similarly, previous research has reported that cryotherapy effectively reduces pain levels in patients (Aghajanloo et al., 2016; Al Amer et al., 2017; Dehghan et al., 2023; Sabitha et al., 2008). The analgesic effect of cryotherapy is believed to involve several physiological mechanisms, including reduced nerve conduction velocity, asynchronous transmission in pain fibres, endorphin release, spinal neuron inhibition, and an increased refractory period of nerve cells. These mechanisms collectively contribute to a reduction in sensory nerve impulse transmission, thereby decreasing pain perception (Nadler et al., 2004; Silva et al., 2018). The findings of this study are in line with these known physiological effects. Repeated cold application prior to each cannulation may have elicited similar responses, resulting in decreased pain scores. However, the progressive decline in pain across sessions may also be influenced by psychological factors such as habituation, reduced anxiety, and adjusted expectations regarding pain. Therefore, cold application may provide not only immediate relief but also a psychologically reinforced analgesic effect when used repeatedly. Whether reduced pain through repetitive pain relief mode is a particular benefit of cold needle use needs to be tested through further comparative research.
Strengths and limitations
The strength of this study is that it is the first to be conducted with a self-controlled, double-blind design. Although the absence of randomisation constitutes a methodological limitation, the use of the VAS substantially mitigates this bias by providing a language-independent, patient-centred quantification of pain. By focusing on intra-individual changes relative to baseline scores, the analysis further minimises group heterogeneity inherent in quasi-experimental designs. Moreover, the VAS framework attenuates contextual variability – such as temporal or environmental influences – thereby enhancing the internal validity of the pain assessments. One of the limitations is that the needle temperature used in the study was 0–2°C and needles at other temperatures were not used (Gorji et al., 2014).
Conclusion and recommendations
In conclusion, it was observed that using a fistula needle at 0–2°C was effective in reducing the pain associated with AVF cannulation. It is recommended that a scientific study with high evidence strength be conducted to evaluate the use of cold needle application during fistula cannulation to reduce invasive pain in the haemodialysis unit. In future research, the use of the Short Form McGill Pain Questionnaire and the McGill Pain Questionnaire may be recommended for patients to describe the pain they feel during fistula cannulation. As the study results show, fistula cannulation with cold needles was found to reduce cannulation-related pain experienced by patients. The fact that the pain experienced during cannulation was quite high in patients in the dialysis centre where the study was conducted reveals that procedures aimed at reducing pain should be implemented. Although pharmacological and non-pharmacological methods are used to reduce pain; it is extremely important to increase the frequency of use of non-pharmacological approaches such as cold needle application. Cold needle application is a very simple method and can be implemented by all nurses in the dialysis centre. This simple, nurse-led intervention – applying a cold needle prior to cannulation – not only reduces procedural pain in routine settings but also proves invaluable in emergency situations where analgesia is often bypassed due to urgency; its ease of implementation affords interdisciplinary relevance for physicians and paramedics and may be readily extended to other needle-related procedures, such as immunisations.
Key points for policy, practice and/or research
Cannulation-related pain is high in the patients who has arteriovenous fistula and affect the patient's compliance with dialysis treatment and lead to a deterioration in the quality of life.
This study shows that cold needle application is a quick and effective pain relief process in cannulation.
The benefits of cold needle application in pain reduction have potential transferability to acute settings and other needle-related procedures such as immunisation.
Cold needle application is a simple and effective nurse-led treatment modification that can be incorporated into local policy.
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871251364711 – Supplemental material for Effect of cold needle application on the arteriovenous fistula cannulation-related pain: a self-controlled, double-blind study
Supplemental material, sj-pdf-1-jrn-10.1177_17449871251364711 for Effect of cold needle application on the arteriovenous fistula cannulation-related pain: a self-controlled, double-blind study by Nurten Ozen, Sümeyye Akcoban and Betul Tosun in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors are grateful to staff of the participating dialysis centre and the patients who participated in this study.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethics committee approval was obtained from the Ethics Committee of the Hasan Kalyoncu University Health Sciences Non-invasive Research to conduct the study (Date: April 02, 2024; Decision No: 2024/50).
Trial registration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.