
Abstract
Background:
Many problems regarding the self-care behaviours of haemodialysis patients are recognised; however, the fear experienced by the patients cannot be adequately explained.
Aims:
This study was conducted to determine the relationship between self-care behaviours related to arteriovenous fistula and fear of fistula failure in individuals receiving haemodialysis treatment.
Methods:
In this descriptive and relational study, 259 patients who met the inclusion criteria constituted the sample of the study. A multiple regression analysis enter model was used to evaluate the predictive power of the Self-Care Behaviours in Arteriovenous Fistula Scale.
Results:
It was found that the primary source of fear related to the fistula was the fear of fistula failure with a rate of 79.5%, and the patients who had this fear had a lower mean self-care scale score. The variables account for 12% of the self-care situation, and it is seen that the model is significant.
Conclusions:
It was concluded that increasing the fear of failure decreased the self-care score. This study is important for raising awareness among nurses regarding the fear of fistula failure. Nurses must provide appropriate care for vascular access and try to alleviate patients’ anxiety and fears by listening to them.
Introduction
Chronic Renal Failure (CRF) is a worldwide problem with high morbidity and mortality rates, causing significant labour loss (Ammirati, 2020; Jayanti et al., 2016; Ok and Işıl, 2019; Varol and Sivrikaya, 2018). Haemodialysis is the most preferred renal replacement therapy, which is one of the treatment methods of CRF (Beaudry et al., 2018; Billah et al., 2019; Görgen et al., 2018; Hsieh et al., 2017; Ramezani et al., 2019; Seyahi et al., 2018). In order for haemodialysis (HD) treatment to be provided, the patient must have a vascular access that enables the connection to haemodialysis and this connection should provide sufficient blood flow (Akyol et al., 2015). These patient-specific connections consist of an arteriovenous fistula (AVF), an arteriovenous graft (AVG) or a permanent/temporary catheter (Billah et al., 2019; Nordyke et al., 2020). When the distribution of patients having haemodialysis in Turkey is examined, it is seen that AVF is the most common method with a rate of 77.41%, followed by a catheter with a permanent tunnel (19.14%), a catheter with a temporary tunnel (2.26%), and AVG (1.19%) (Süleymanlar et al., 2018).
Although it has been reported that the most important access is arteriovenous in patients receiving haemodialysis treatment (Gjorgjievski et al., 2019; Sousa et al., 2018), this access is not completely problem-free. Patients experience a number of difficulties in the treatment process, and providing and maintaining vascular access is one of the biggest challenges for haemodialysis patients. It has been reported that 20–60% of patients experience problems during the maturation and use of the AVF (Enworom and Tabi, 2015). Before and after haemodialysis treatment, the care and protection of the vascular access is primarily among the duties of the dialysis nurse (Özdemir and Akyol, 2019). However, in order to experience a relatively smooth process, patients have some responsibilities as well. For this reason, it is very important for patients to develop awareness and self-care of the access.
Patients paying great attention to self-care can face their diseases more easily (Ramezani et al., 2019; Wilcox et al., 2016; Wong et al., 2018). In addition to reducing the complications related to a fistula, self-care performed by the patients contributes to shortening the duration of hospital stay, reducing the cost of care, increasing the quality of life and decreasing the stress level. Most importantly, the level of self-care of patients plays a role in decreasing mortality rates (Abraham et al., 2020; Ghadam et al., 2016; Rayyani et al., 2014; Stavropoulou et al., 2017). Studies have shown that as self-care behaviour increases in individuals receiving HD treatment, a positive change is observed in the well-being of patients (Rahimi et al., 2017). It has also been revealed that patients’ self-care behaviours facilitate compliance with treatment, reduce physical and psychological complications and contribute to creating health-promoting behaviours (Başarır and Pakyüz, 2015; Wong et al., 2018). Failure to develop the necessary self-care behaviour for AVF can cause AVF failure, and patients with fistulas may face some operations and even life-threatening risks (Sousa et al., 2017, 2018; Ramezani et al., 2019; Wang et al., 2019). Patients who realise that they have to protect their AVF access have great anxiety and fear about the risk of AVF failure (Alsaqri et al., 2019; Richard, 2011).
In addition to being a treatment method, haemodialysis is a stressful procedure affecting the lives of patients (Lilympaki et al., 2016; Rioux et al., 2015). Although fear is one of the biggest obstacles to an individual’s early start of haemodialysis (Werner Rêgo et al., 2019), long-term vascular treatments also cause fear in patients (Abraham et al., 2020; Fathy et al., 2017; Kordzadeh and Esfahlani, 2019). Studies conducted on patients with arteriovenous fistula reported that patients fear losing their fistula (Clementino et al., 2018), and as the duration of dialysis is prolonged, the level of fear increases (Babiarczyk and Barcik, 2017). The study conducted by Shafi et al. (2018) revealed that the reasons for rejecting haemodialysis are fear of the haemodialysis catheter (33.9%), fear of AVF needle insertion (24.5%), fear of haemodialysis complications (33.9%) and fear of death in haemodialysis (22.6%). Studies have revealed that self-care and fear are two important concepts in haemodialysis treatment. Although there are studies examining the self-care behaviours of haemodialysis patients related to AVF, no studies have yet investigated the relationship between the fear of fistula failure and self-care. In this respect, this study is believed to make a contribution to the literature by filling the gap and by providing data for and directing future studies. The research questions developed for this study were as follows:
What are the self-care behaviour levels of individuals receiving haemodialysis treatment regarding arteriovenous fistula?
What is the level of the fear of fistula failure in patients receiving haemodialysis?
Is there a relationship between the self-care behaviour levels related to arteriovenous fistula and fear of fistula failure in patients receiving haemodialysis treatment?
Methods
Study design
This study was a descriptive-relational research.
Participants and sample size
It was initially planned to carry out the study in the dialysis centres in the capital of Turkey; however, due to the pandemic, the dialysis centres in public hospitals could not be included in the study. The study was conducted with patients in four private haemodialysis centres. A total of 340 patients was reached between 6 and 8 March 2020 without sample selection; however, 81 patients refused to participate in the study for various reasons (not being willing to complete the questionnaire form, seeing participation in the study as a waste of time, risk of being infected with COVID-19, etc.). Thus, 259 patients constituted the sample of the study. Patients who were 18 years of age and older, who received haemodialysis treatment, who had arteriovenous fistula as the haemodialysis vascular access, who did not have any visual or auditory impairment, who could communicate verbally and who volunteered to participate in the study were included in the study.
Instruments
Patient information form
The form was prepared by the researchers and consists of questions about demographic and disease characteristics.
Questions about the fear of fistula failure
The participants were asked three questions evaluating the sources of fear related to AVF failure, the state of experiencing fistula failure and the frequency of experiencing the fear of fistula failure.
The Scale of Assessment of Self-Care Behaviours with Arteriovenous Fistula in Haemodialysis Patients
The scale was developed by Sousa and colleagues in 2014. It was revised in 2015 (Souza et al., 2015), and the number of items was reduced from 31 to 16. It consists of two parts, which are signs and symptoms (n: 6 items) and prevention of complications (n: 10 items). Responses to each item range from 1, which refers to developing no self-care behaviour, to 5, which refers to exhibiting self-care behaviour at all times. The minimum score that can be obtained from the scale is 16 and the maximum score is 80. The validity and reliability study of the scale for Turkish society was conducted by İkiz and Yıldırım Usta (2016), and the Cronbach’s alpha coefficient of the scale was reported to be 0.91. The Cronbach’s alpha value of the scale was 0.74 for our study group.
Data collection
The data were collected by the researcher using one-to-one interview techniques on a voluntary basis in four private dialysis centres between 6 and 28 March 2020. The researcher went to the clinic the day before and determined the patients who were eligible to be included in the sample. Patients talked about the research both verbally and were informed in writing.
Statistical analysis
The coding and analysis of the data were made using the SPSS 22.0 program. The reliability of the scale for the study group was determined with the Cronbach’s alpha coefficient, and t-test, one-way analysis of variance and Pearson correlation analysis were used for comparison in independent groups. The predictive power of the scale was determined using the multiple regression analysis enter model. The results obtained were evaluated at a significance level of p < 0.05.
Ethical statement
The study was approved by the Selçuk University Faculty of Health Sciences From the Non-invasive Research Ethics Committee (decision no: 74668451-100) and was performed in accordance with the Helsinki Declaration. All the potential participants were requested to submit a written informed consent. Data were collected and recorded in a manner that protected the anonymity of the participants. In all stages of the study, the STROBE checklist was followed.
Results
The average age of the participants was 61.09 ± 14.34; 57.9% were male, 88.8% were married, 40.2% were primary school graduates, 37.8% were retired and 36.7% stated that their income only meets their expenses. When the characteristics of the patients regarding haemodialysis treatment were examined, it was found that an average of 120.9 ± 19.6 weeks passed between the diagnosis and initiation of haemodialysis treatment. The average duration of haemodialysis treatment was found to be 86.17 ± 86.13 months. About 88% of the patients received haemodialysis three times a week, and 54.8% of them had temporary catheters as their first vascular access and 59.8% had another chronic disease. When the descriptive findings from the Scale of Assessment of Self-Care Behaviours with Arteriovenous Fistula in Haemodialysis (ASBHD-AVF) Patients were examined, it was seen that the participants obtained an average score of 65.86 ± 0.65 from the scale. It was further determined that the smallest and largest values were 45 and 77, which showed normal distribution according to the skewness and kurtosis values.
It was determined that 44% of the patients had the problem of fistula failure before and 42.5% always had the fear of fistula failure. The primary source of fistula-related fear of patients is the fear of fistula failure with a rate of 79.5% (Table 1).
Some characteristics of patients regarding fistula failure.
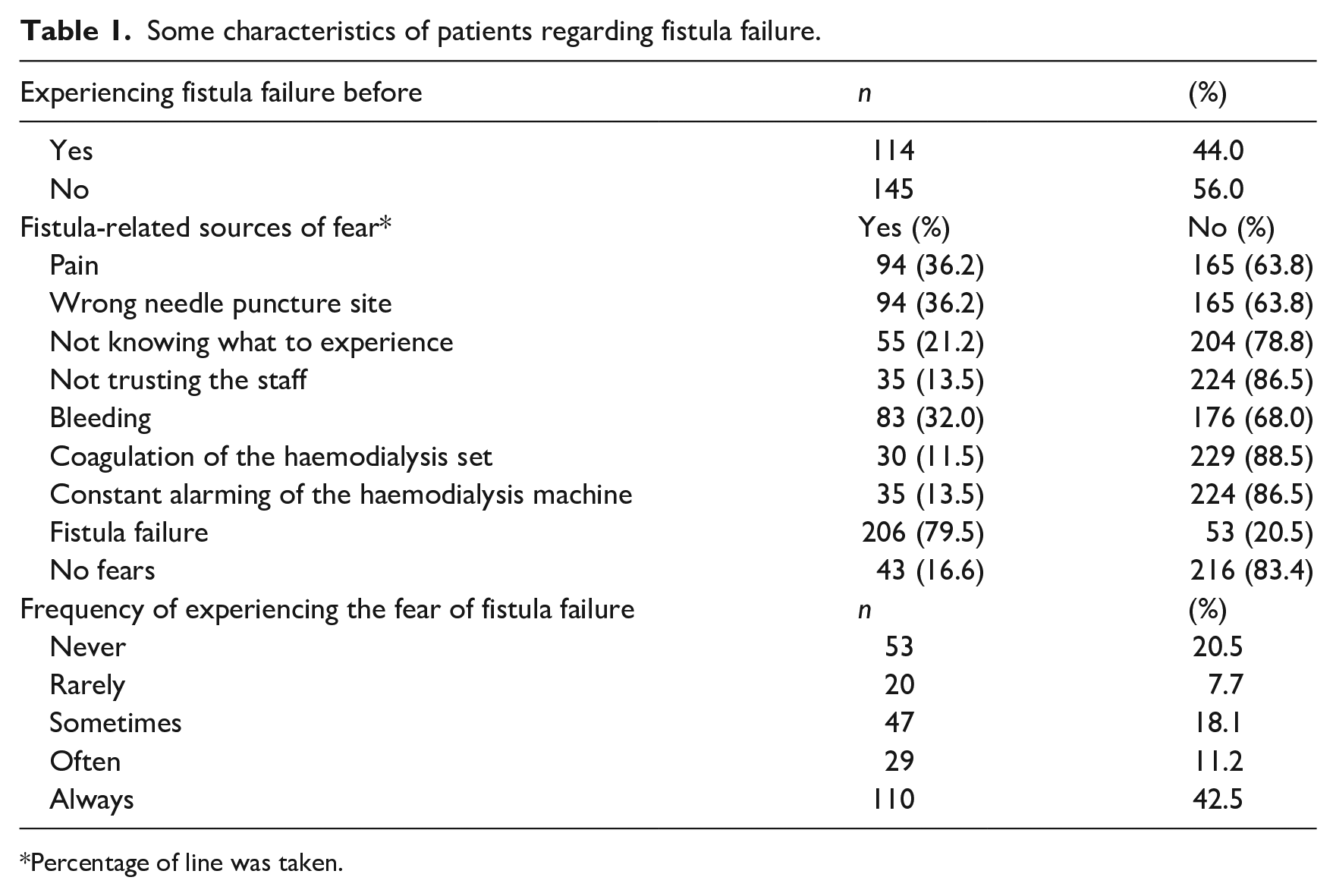
Percentage of line was taken.
The comparison of the ASBHD-AVF Scale according to some socio-demographic characteristics and the presence of chronic diseases is given in Table 2. It was found that women (67.45 ± 6.27) had higher self-care scores than men (64.70 ± 6.84); and those who did not work in an income-generating job (67.36 ± 6.32) had higher self-care scores than those who work (64.86 ± 6.83; p > 0.05). The relationship between the continuous variables and the scale was evaluated using correlation analysis. According to this analysis, there is no relationship between the scale score and age and duration of haemodialysis treatment, whereas the self-care scale score increases as the time between diagnosis and the initiation of haemodialysis treatment increases. It was found that the relationship between these two variables was positive and moderate (r = 0.429; p < 0.05).
Comparison of the scale of assessment of self-care behaviours with arteriovenous fistula in haemodialysis patients with some variables.
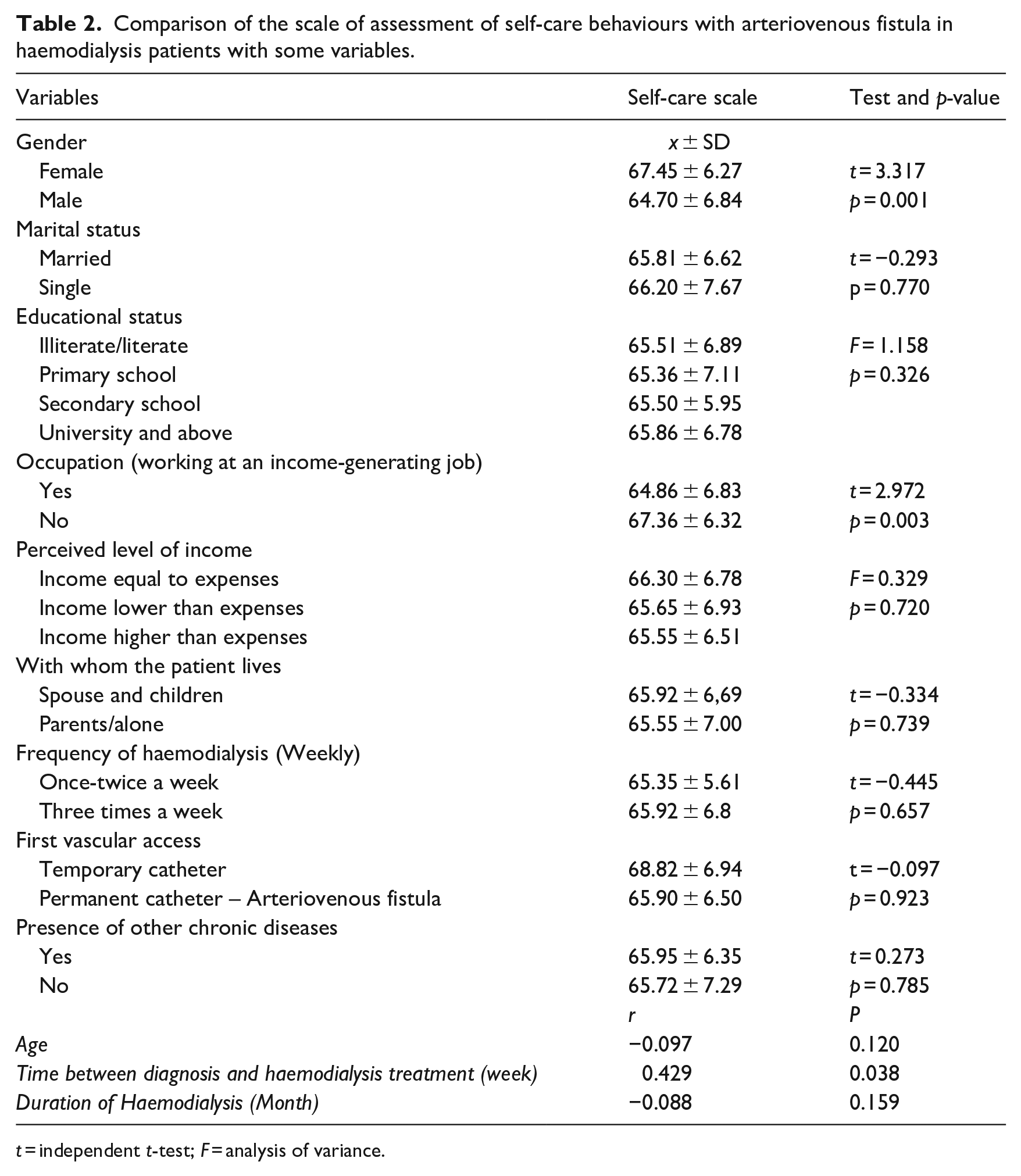
t = independent t-test; F = analysis of variance.
Although the mean scale scores of the patients who had and did not have the fistula failure problem before were similar (p > 0.05), it was found that patients who often/always experience the fear of fistula failure (64.62 ± 6.89) have lower mean self-care scores compared to those who sometimes (67.02 ± 5.16) or never/rarely (67.46 ± 6.92) experience this fear (p < 0.05; Table 3).
Comparison of the scores received from the scale of self-care behaviours within haemodialysis patients according to patients’ fear of experiencing fistula failure problems.
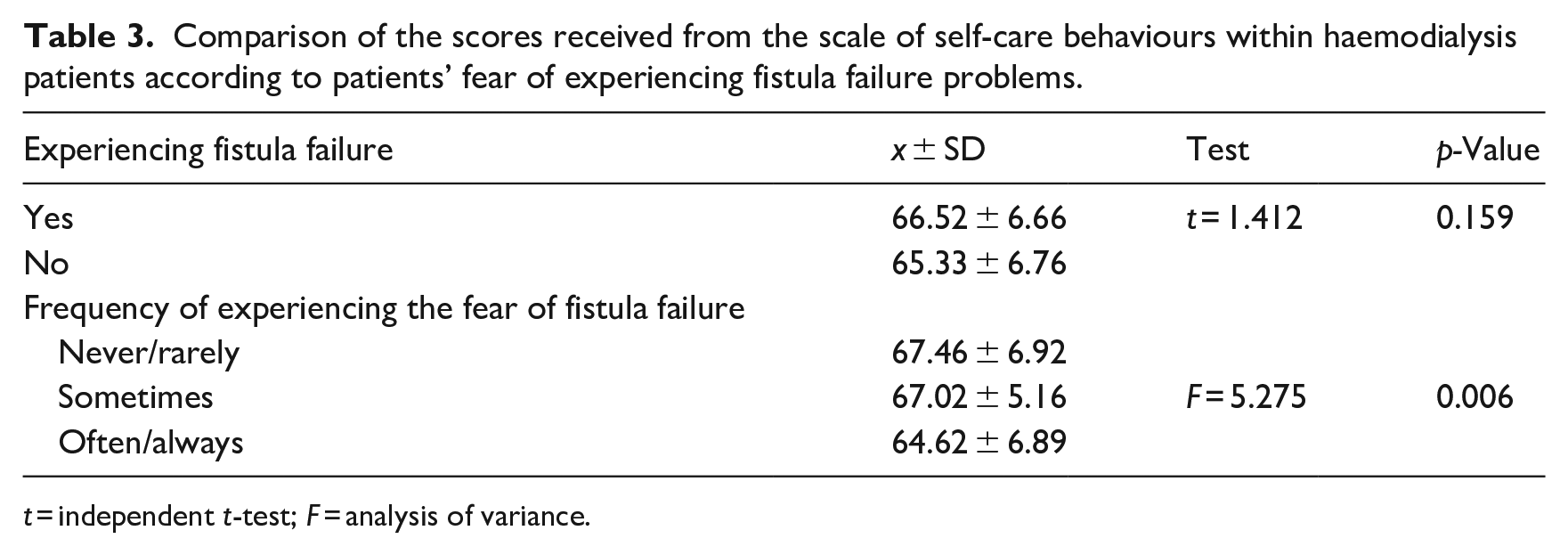
t = independent t-test; F = analysis of variance.
The predictors of the Scale of Assessment of Self-Care Behaviours with Arteriovenous Fistula in Haemodialysis Patients were evaluated using the multiple regression analysis enter method. In independent groups, this analysis was carried out with t-test, one-way analysis of variance and correlation analysis with the variables that were significant. Before the analysis, the database was evaluated in terms of sampling adequacy, autocorrelation and multicollinearity assumptions. The analysis continued as the assumptions were met. Independent variables other than continuous variables are coded as 0 and 1. The variable coded as 1 is shown in parentheses in the table. According to the analysis, the most important predictors of the scale are the duration between the diagnosis of the disease and haemodialysis treatment (β = 0.248) and experiencing the fear of fistula failure often/always (β = −0.153). As the time between diagnosis and haemodialysis treatment increases, the self-care score increases. On the other hand, the self-care score decreases when the fear of fistula failure is experienced often/always present. These variables account for 12% of self-care. It is seen that the model is significant (F = 8.603, p < 0.001; Table 4).
Predictors of the scale of assessment of self-care behaviours with arteriovenous fistula in haemodialysis patients.
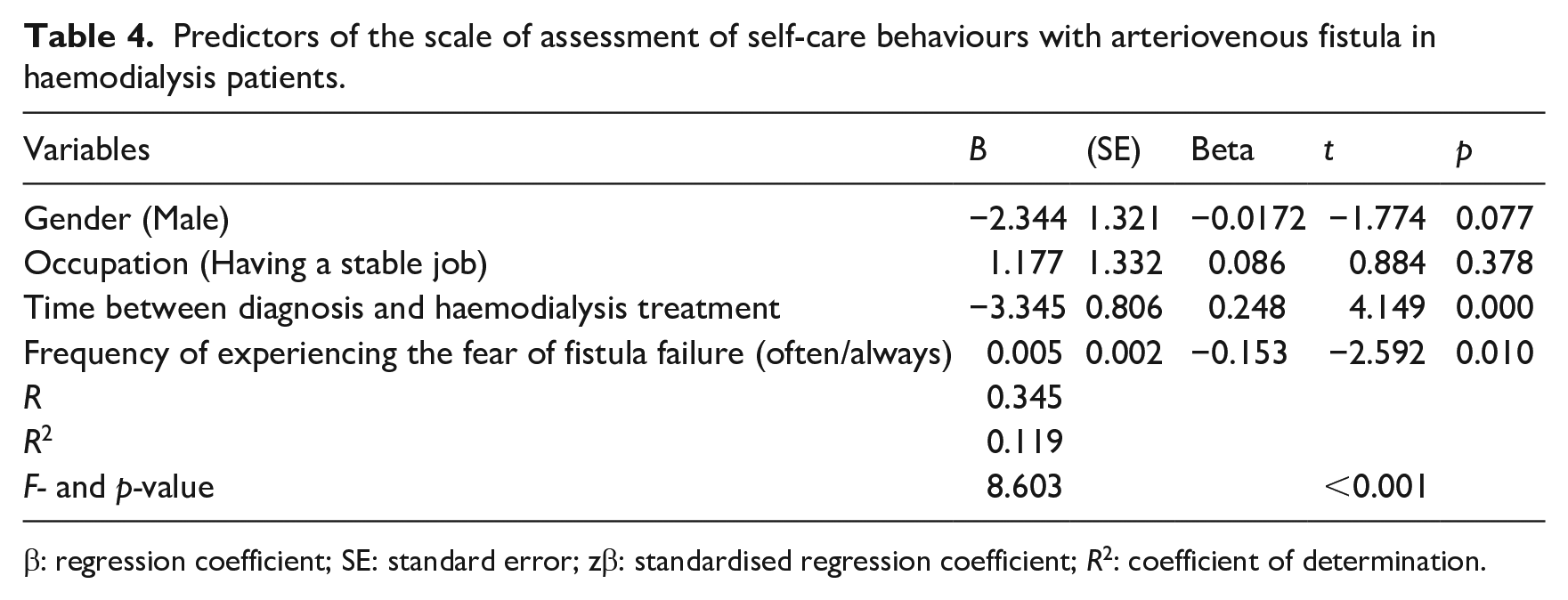
β: regression coefficient; SE: standard error; zβ: standardised regression coefficient; R2: coefficient of determination.
Discussion
Ensuring adequate AVF access is important for patient survival in HD (Gjorgjievski et al., 2019). These access routes are the person’s lifeline, which must be used and maintained carefully. The biggest fear of the patients during the intervention to vascular access is a possible harm to or loss of the AVF (Richard, 2011; Silva et al., 2018). Due to AVF failure, patients are confronted with fistula surgery again (Özdemir and Akyol, 2019). Our study revealed that 44% of the participants had the problem of fistula failure before, and when the sources of fear related to fistulas were examined, different reasons emerged. It has been reported in the literature that more than half of the participants were admitted to the hospital because of one or more fistula failure (De Azevedo Gonçalves et al., 2020; Ozen et al., 2017; Sousa et al., 2018; Stavropoulou et al., 2017). The study conducted by Erdoğan et al. (2016) reported that 14.1% of the participants had a fear of fistula rupture. Mazarova et al. (2017) revealed that patients were afraid of needles and complications, and Clementino et al. (2018) reported that all participants feared losing their fistula. The study conducted by Shafi et al. (2018) revealed that 42.4% of the participants refused haemodialysis. Among the reasons given by the patients to refuse haemodialysis were fear of haemodialysis catheter (33.9%), fear of AVF needles (24.5%), fear of haemodialysis complications (33.9%) and fear of death during haemodialysis (22.6%). Babiarczyk and Barcik (2017) found that as the dialysis period is prolonged, the level of fear increases among patients. Studies have revealed that 88.2% of the participants had access loss due to thrombosis (Sousa et al., 2017), 14.1% had AVF failure (Magar et al., 2020) and 45.6% had the most common complications of thrombosis, bleeding and stenosis respectively due to AVF opening (Atik et al., 2016). Acar (2014) found that 17.5% of the participants were worried about damage to the vascular access. Diab and Mustafa (2019) study indicated that 36.4% of the participants who exhibited adequate levels of self-care behaviours experienced the problem of fistula failure once and 45.5% experienced the same problem twice. Atik et al., (2016) revealed that the patients who had an AVF operation once had lower levels of stress perception compared to those who had two AVF operations.
Early diagnosis and treatment of AVF-related complications is important to prevent AVF loss (Aljuaid et al., 2020). A failed AVF can be seen as a cause of fear. Therefore, the self-care and close observation process should begin immediately after the fistula is opened. It was found that those who often/always have the fear of fistula failure had lower self-care behaviour scores than those who have no fear. As a result, the fear of fistula failure decreases in patients whose self-care behaviour scores increase. There is no study in the literature investigating the relationship between the self-care behaviours of patients with or without AVF failure, which limited our discussion. However, since the self-care behaviour scores of patients whose AVF has failed and whose AVF has not failed are similar, it may be thought that other physical factors or lack of proper care may have caused vascular access problems.
Self-Care Regarding Arteriovenous Fistula in Haemodialysis Patients: It was determined that the average score they received from the behaviour scale was 65.86 ± 0.65. In some studies, consistent with our study, it was found that patients’ self-care behaviours decreased (Diab and Mostafa, 2019; Han and Kim, 2016, Yang et al., 2019). Unlike our study, there are studies in which the average self-care score increases (Abraham et al., 2020; Atashpeikar et al., 2012; Bettoni et al., 2017; García Araque and Sancho Cantus, 2015; Silva et al., 2018). The positive attitudes of haemodialysis patients regarding self-care behaviours will also positively affect the process of living with the disease.
Our data confirm that the predictors of self-care behaviours in people with an Arteriovenous Fistula are gender (male/female), the duration of time between diagnosis and haemodialysis treatment and the intense fear of fistula failure, which are also the main problems in AVF patients. When the studies are examined, although there are studies where men’s self-care behaviours are found to be higher than women (Atashpeikar et al., 2012), there are studies where women’s self-care behaviours are higher than men (García Araque and Sancho Cantus, 2015; Iqbal et al., 2018). According to the findings obtained from the literature, different study results were obtained regarding the significance of self-care behaviour scores according to gender. It was thought that these different results may be due to sociocultural factors.
As the time between diagnosis and haemodialysis treatment is prolonged, the self-care scores of the patients increase. In addition, the intense fear of experiencing fistula failure lowers the self-care scores. In our study, it was found that 44% of the participants had fistula failure problems. In the literature review, it was reported that approximately 53.1% of the participants were admitted to the hospital due to one or more fistula failure (De Azevedo Gonçalves et al., 2020; Ozen et al., 2017, Sousa et al., 2018; Stavropoulou et al., 2017). Nurses should pay close attention to protecting the CKD patient’s vascular access and maintaining access. This access route should be protected and used only for haemodialysis. Because haemodialysis treatment cannot be performed without haemodialysis access and if haemodialysis cannot be performed, it may result in the mortality of CKD patients. Long-term use of AVF will be possible with the patients’ daily AVF self-care plan (Rashid et al., 2018). In this care, it is important to comply with aseptic rules, keep the arm above a certain level, perform individually designed exercises and maintain personal habits in order to ensure AVF durability before haemodialysis (Clementino et al., 2018; Iqbal et al., 2018; Kong et al., 2019). In addition, feeling the ‘thrill’ in the AVF area, listening to the murmur and observing for signs and symptoms such as redness and itching are among the duties of the nurse (Abraham et al., 2020; Alsaqri et al., 2019).
Our study examining the relationship between self-care behaviours related to arteriovenous fistula and the fear of fistula failure in haemodialysis patients reached results consistent with the literature on self-care (Diab and Mostafa 2019; Han and Kim 2016; Yang et al., 2019). However, since there are not many studies investigating the relationship between self-care behaviours related to AVF and the fear of fistula failure, it is believed that this study may be a guide for future studies on the same topic. In line with these results, it can be stated that it is important to develop methods and strategies for nurses to cope with the fear of fistula failure so that self-care is improved and the fear of fistula failure is reduced.
Limitations of the study
This study has some limitations. Firstly, the study was conducted only in four dialysis centres in one region of Turkey. Therefore, generalisations should be made with caution. Secondly, the limited literature on the subject restricted the discussion of the findings. Finally, we did not assess the participants’ self-management across time. More longitudinal studies are necessary to evaluate self-management behaviours of patients under haemodialysis.
Conclusions
This study revealed that the average self-care behaviour scores of patients experiencing the fear of fistula failure are lower, and the most significant determinants of the scale are gender, the time between diagnosis and haemodialysis treatment and the fear of fistula failure. This study is important for increasing awareness among nurses regarding the fear of fistula failure. Nurses should work to alleviate patients’ concerns and fears by listening to them. Addressing concerns related to vascular access and providing care can help individuals overcome their fear of dialysis. When providing education on fistula care to patients, it is important to include training that explains the relationship between fistula failure and fear. Ensuring appropriate care for vascular access to preserve fistula function and regular evaluation of vascular access are crucial. Practices that improve self-care behaviours can reduce the need for referrals to medical centres and ultimately result in cost savings. Further studies are needed to confirm the impact of fistula failure on self-care behaviours.
It is essential to develop a framework to organise and describe the interventions to be developed, which can enable people to develop self-care behaviours with an AVF.
This paper contributed to the current state of knowledge for determining the self-care behaviours of patients with AVF.
The fear of fistula failure decreases in patients whose self-care behaviour scores increase.
Therefore, it is crucial to diminish the lack of self-care in patients and create individualised self-care plans.
It is necessary to identify patients’ fears related to fistula care; nurses should provide suitable care for vascular access, considering both physical and psychological needs, and evaluate the care given.
Footnotes
Acknowledgements
The authors gratefully thank all patients for their participation in this.
Data accessibility statement
The datasets analysed in this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Selçuk University Faculty of Health Sciences From the Non-invasive Research Ethics Committee (decision no: 74668451-100) and was performed in accordance with the Helsinki Declaration. All the potential participants were requested to submit a written informed consent. Data were collected and recorded in a manner that protected the anonymity of the participants. In all stages of the study, the STROBE checklist were followed.
Consent for publication
Individual written informed consent for the research team to publish the study results was obtained from all patients.