
Abstract
Background:
Stroke remains a major global health issue, especially for younger women, who often face poorer rehabilitation outcomes. While current stroke rehabilitation programmes address general recovery needs, they may not fully meet the unique physical, psychological and long-term challenges encountered by younger women.
Aims:
This study aimed to develop a stroke rehabilitation framework specifically for younger women, incorporating insights from both stroke survivors and healthcare professionals.
Methods:
A qualitative, multi-phase study utilising Arksey and O’Malley’s framework methodology gathered data from younger women stroke survivors (18–64 years old) through snowball sampling and healthcare professionals via purposive sampling. Focus groups and interviews were conducted, and thematic analysis synthesised the insights to inform a tailored stroke rehabilitation framework.
Results:
Five younger women stroke survivors (mean age = 40) and five healthcare professionals participated in the study. The MENTOR HUB framework was developed, incorporating key components: Monitoring, Education, Navigation, Tools, Ongoing Support, Recovery, Holistic Care, User-centred Approach and Be-continuous.
Conclusions:
The MENTOR HUB framework integrates the lived experiences of stroke survivors with professional healthcare insights, offering a holistic, user-centred approach to rehabilitation. It emphasises the importance of continuous support and personalised care. Further research is necessary to evaluate its effectiveness in clinical practice.
Keywords
Introduction
Stroke remains a major global health issue impacting individuals across all age groups (Feigin et al., 2017), with younger women facing unique challenges (Ekker et al., 2019; Leppert et al., 2020, 2022). Notably, younger women have a higher incidence of stroke compared to men, with the 2022 Global Stroke Fact Sheet reporting 6.4 million women versus 5.8 million men affected by stroke (Ekker and Leeuw, 2020; Feigin et al., 2022). This gender disparity is evident across various countries, with studies in the United States (Leppert et al., 2020), the Netherlands (Ekker et al., 2019), and Canada (Vyas et al., 2021) showing higher stroke rates among women under 44; and in New Zealand, where women under 65 face a higher fatality rate (61%) than men (39%) (New Zealand Stroke Foundation, 2020).
Younger women survivors experience poorer long-term outcomes, including higher disability rates and reduced quality of life, with these disparities compounded by a longer, more challenging recovery due to their extended life expectancy (Carcel et al., 2019; Stewart et al., 2023; Synhaeve et al., 2016). In addition to physical disability, younger women are also more likely to face mental health challenges, such as depression, which further hinders their recovery and overall well-being (Eddelien et al., 2022; Liljehult et al., 2021). As a result, they experience higher depression rates and increased care costs compared to men (Caponnetto et al., 2021; Qureshi et al., 2022). Younger women face unique challenges in stroke recovery due to a combination of physiological, social and cultural factors. Kim (2023) noted that hormonal fluctuations linked to puberty, pregnancy, lactation and menopause can significantly impact their health and recovery. Additionally, Ospel et al. (2023) highlighted that socioeconomic and cultural factors, such as lower education levels, economic disadvantage and reduced social status, further influence stroke outcomes. As a result, even years after surviving a stroke, many younger women continue to report the need for ongoing support to address their physical, mental and emotional well-being (Tarihoran et al., 2023).
Younger women stroke survivors face unique challenges that underscore the urgent need for specialised self-management programmes. Existing rehabilitation approaches, including traditional methods, telerehabilitation, home-based technologies, immersive virtual reality and self-rehabilitation programmes, have been explored (Chen et al., 2019; Demeco et al., 2023; Doumas et al., 2021; Nascimento et al., 2022; Sharififar et al., 2023). However, these programmes are generally designed for the broader stroke population and do not address the specific needs of younger women. Research shows that younger women experience nearly double the rate of post-stroke depression compared to men, with reduced functional independence being a key symptom (Caponnetto et al., 2021; Eddelien et al., 2022; Mou et al., 2021). In addition, the transition from caregiver to patient creates a profound role shift, often accompanied by emotional distress. Many of these women still bear the responsibility of caregiving for children, aging parents or other family members, which further heightens their emotional stress (Carcel et al., 2020; McCurley et al., 2019). As evidenced by studies, younger women are less likely to utilise healthcare services, including doctor visits and screenings, compared to older women (Jacobs and Ellis, 2021), which further complicates their recovery. This combination of physical, emotional, and caregiving challenges underscores the need for rehabilitation frameworks specifically tailored to younger women stroke survivors. This aligns with the findings of Leahy et al. (2016), the only study to focus exclusively on the needs of younger women in this context.
Current stroke rehabilitation guidelines primarily address general stroke survivors (Teasell et al., 2020) or specific age groups, such as childhood stroke (29 days to 18 years) (Royal College of Paediatrics and Child Health, 2017), young adults (18–45 years) (Holloway et al., 2022), and older adults (65 years and older) (Booth et al., 2019). For younger women (18–65 years), only stroke prevention guidelines exist, with no specific guidelines for post-stroke rehabilitation. To develop an effective rehabilitation programme for this group, it is essential to gather the most relevant and up-to-date insights. To date, much of the research involves mixed-age cohorts (18–85 years) (Beal, 2015; Jacobs and Ellis, 2021; Lever, 2017; Moorley et al., 2016; Yilmaz et al., 2015) or primarily targets older women (68–83 years) (Eilertsen et al., 2010; Hilton, 2002; Tavener et al., 2015), with only one study specifically examining younger women (18–50 years) (Leahy et al., 2016). Furthermore, there is only one study on stroke rehabilitation for younger women, which incorporates healthcare professionals’ perspectives (Kvigne et al., 2005).
This study aimed to develop a stroke rehabilitation framework specifically for younger women, integrating insights from both stroke survivors and healthcare professionals as incorporating insights from both groups can provide a more holistic understanding and therefore, form a robust foundation for evidence-based interventions. The development of this framework is guided by two key research questions: What are the lived experiences of younger women stroke survivors, and what are their specific rehabilitation needs?
Methodology
A qualitative, multi-phase research was employed, utilising a five-stage framework development methodology as outlined by Arksey and O’Malley (2005). These stages included: identifying research questions, defining relevant phases of research, selecting findings, organising the results, and synthesising them into a cohesive framework (Figure 1). The methodology and methods used are described below under the framework headings.
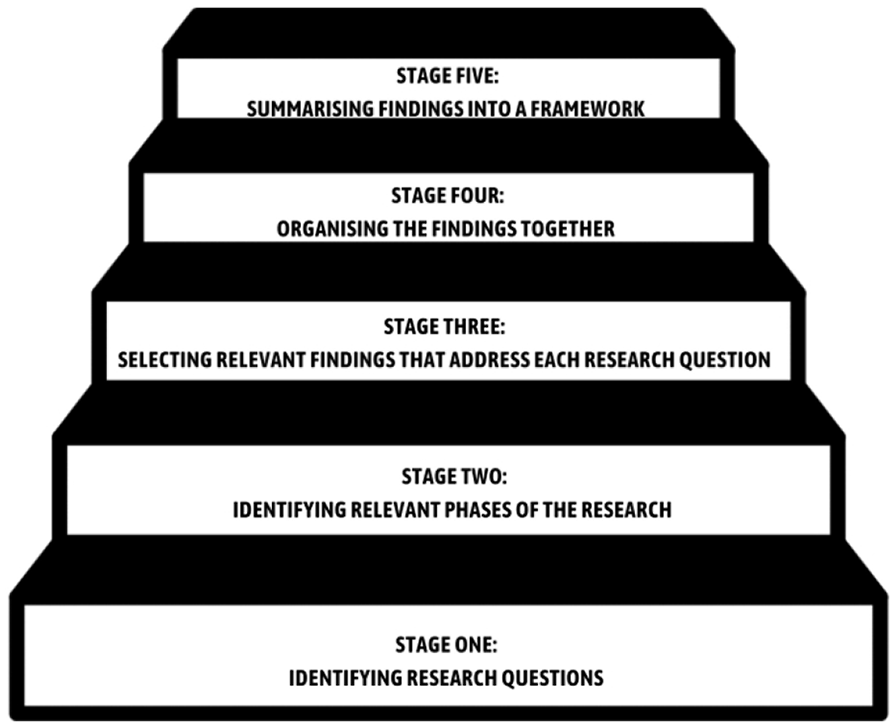
Framework development stages by Arksey and O’Malley (2005).
Stage 1: Identifying research questions
This stage focused on formulating research questions to guide the development of a tailored stroke rehabilitation framework for younger women survivors, addressing their unique challenges and needs. The two key research questions were: What are the lived experiences of younger women stroke survivors, and what are their specific rehabilitation needs?
Stage 2: Identifying relevant phases
This study is conducted in three sequential phases: the first gathers information from younger women stroke survivors, the second explores healthcare professionals’ perspectives, and the third revisits the women to further explore their preferences for stroke rehabilitation based on the insights from healthcare professionals (Figure 2).

Sequential phases of the study.
In Phase 1, eligibility criteria focused on younger women (aged 18–65) who had experienced a stroke at any stage. Participants were recruited through snowball sampling using email invitations from the Stroke Research Clinic’s database, with ethical approval granted (Reference Number 024663 from the University of Auckland Human Participants Ethics Committee). Focus Group Discussions (FGDs) were conducted to explore the participants’ experiences and challenges. Phase 2 focused on healthcare professionals purposively sampled from a large urban hospital. Participants, who were eligible based on their experience working with younger women stroke survivors, were recruited via email invitations, with ethical approval obtained (Reference Number 024663 from the University of Auckland Human Participants Ethics Committee). FGDs were conducted to capture their perspectives on stroke care. In Phase 3, Phase 1 participants were invited to continue their involvement, facilitating a comparison with healthcare professionals’ perspectives and an exploration of the survivors’ rehabilitation programme preferences. This multi-phase approach provided a comprehensive understanding of both survivor and healthcare professional views on stroke rehabilitation.
Adopting a relativist ontology (Denzin and Lincoln, 2011) and a constructionist approach (Crotty, 1998), the researchers aimed to capture the complexity of stroke survivors’ experiences. An interpretive lens was used to explore emotional and perceptual dimensions, fostering a comprehensive understanding of their realities (Chowdhury, 2014). Data from discussions and interviews were transcribed and analysed using Braun and Clarke’s (2022) six-step thematic analysis process (2022), which included familiarisation, coding, theme generation, development, refinement and writing up to identify key themes.
Stage 3: Selecting relevant findings
Thematic results from all phases were organised in relation to the research questions as part of the planning process.
Stage 4: Organising findings
Emerging themes were then integrated and mapped to these questions, guiding and informing the development of the rehabilitation framework.
Stage 5: Summarising findings into a framework
The rehabilitation framework was refined and finalised based on participant feedback to ensure it accurately reflected their rehabilitation needs, challenges, and preferences for post-stroke care.
This study follows ethical principles based on Guba and Lincoln (1994), which emphasise credibility, dependability, confirmability, transferability and authenticity. Strategies used include participant selection and member-checking for credibility, maintaining detailed notes for dependability, including supporting quotes and member-checking for confirmability, providing detailed participant descriptions for transferability and incorporating direct quotes and member-checking for authenticity. These steps together ensure the trustworthiness and rigor of the qualitative research approach. The researchers are experienced professionals with decades of expertise in nursing, education, and research; collectively committed to advancing healthcare through research, clinical practice, and education, with a particular focus on improving patient outcomes in stroke care.
Results
The development of the stroke rehabilitation framework for younger women survivors followed a systematic, multi-stage process.
Phase 1: Younger women stroke survivor’s experiences
The five women in the focus group ranged from 6 to 18 years post-stroke. The ages when they had a stroke ranged from 21 to 63 years (Table 1). Four of the five participants were interviewed in person, and the fifth participant opted to join the FGDs in real time through videoconferencing (Zoom). Phase 1 identified four key themes in younger women stroke survivors’ experiences: stroke impacts, reproductive health, self-management and support.
Younger women stroke survivor’s demographics.
Phase 2: Healthcare professional’s perspectives
Five healthcare professionals (Table 2), including nurses and occupational therapists, were interviewed in person during FGDs, revealing themes of rehabilitation approaches, healthcare challenges, support systems, and patient-centred care.
Healthcare professional’s demographics.
Phase 3: Preferences of younger women stroke survivors for rehabilitation programmes
Building on the insights from Phase 2, four of the five participants who had previously attended the focus group discussion agreed to further explore their preferences for rehabilitation programmes in Phase 3. This phase highlighted three key themes: goal setting, the importance of a multidisciplinary team, and the need for support and empowerment.
Collectively, these findings provide a comprehensive understanding of both patient and healthcare professional perspectives, as summarised in Table 3.
Phases 1, 2 and 3: summary of findings.
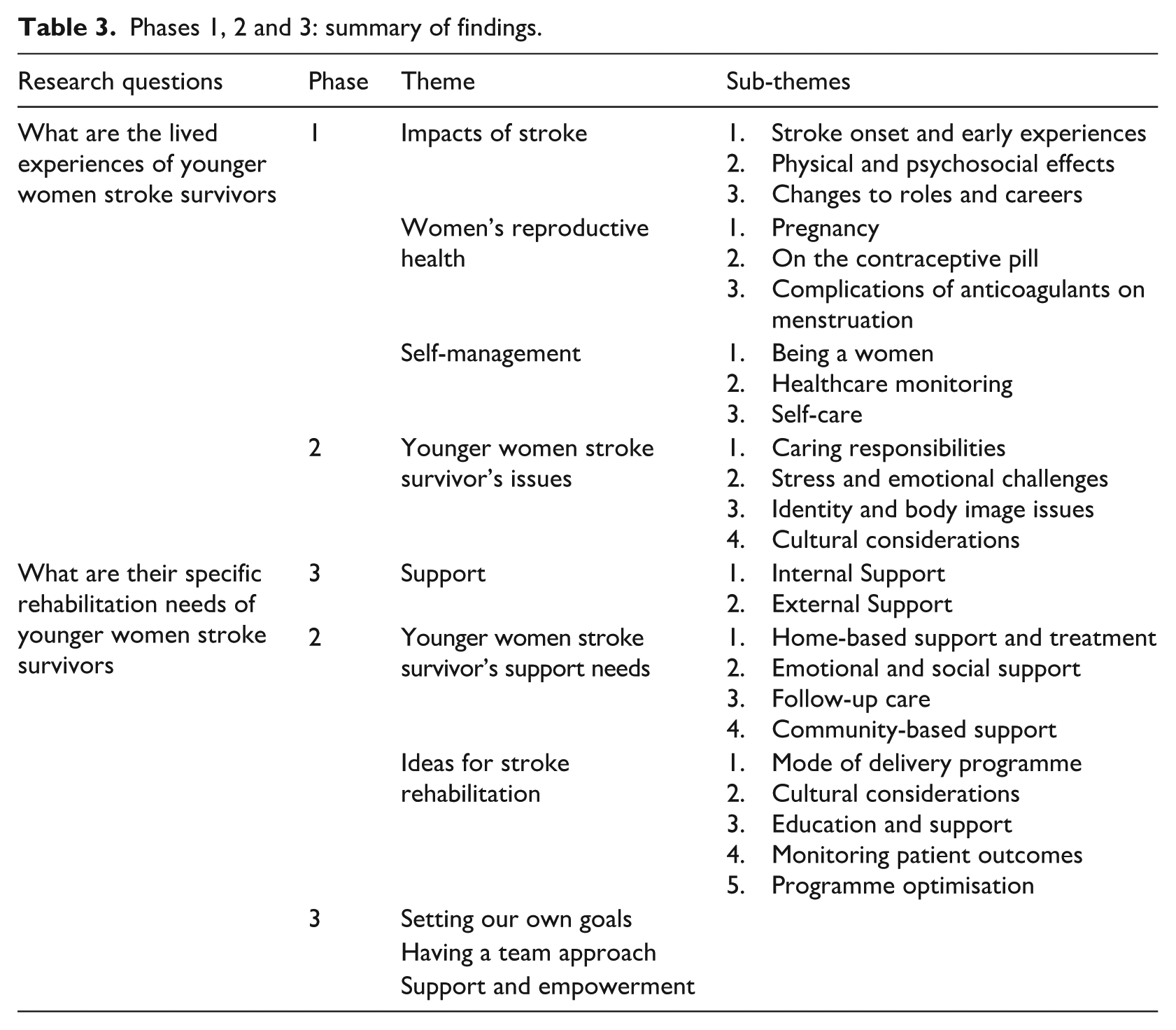
Thematic findings from each phase form the foundation of the stroke rehabilitation framework, encompassing key components such as the impacts of stroke, reproductive health, challenges, self-management, support needs, person-centred goal setting, team collaboration, and empowerment. Monitoring stroke effects is essential for improving health outcomes with targeted education needed for reproductive health concerns. Clear navigation of rehabilitation goals is vital for person-centred goal setting and effective teamwork. Accessible tools for self-management and the high demand for support highlight the need for a specialised recovery programme. These insights are visually represented in Figure 3.
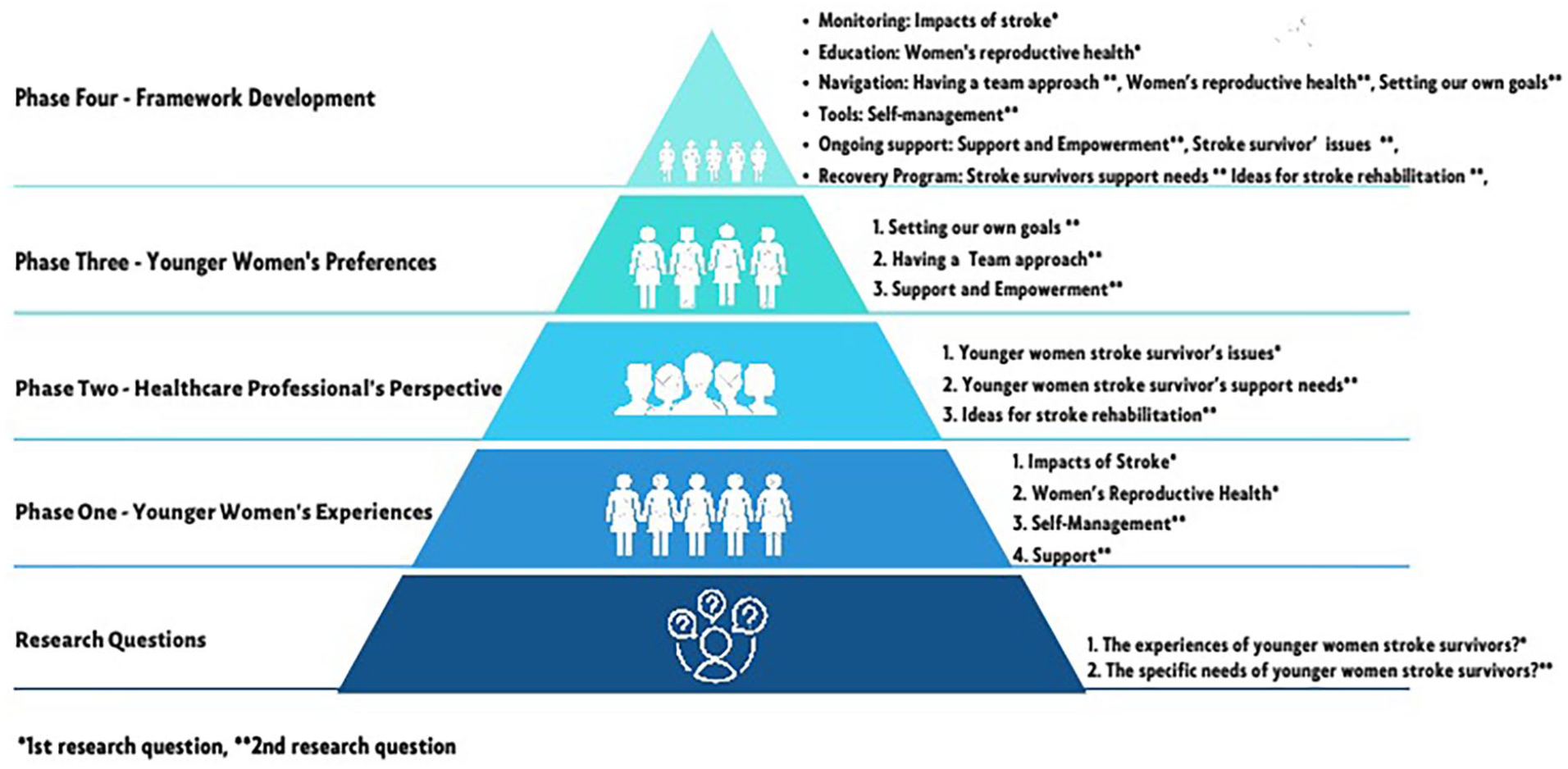
MENTOR stroke rehabilitation framework.
Findings from this study identified the key elements for the Stroke Rehabilitation MENTOR Framework: Monitoring, Education, Support, Navigation, Tools, Online Support and a Recovery Programme. A graphical representation was presented to participants for feedback in Phase 3. All participants confirmed the MENTOR Framework’s relevance and necessity, while also suggesting areas for improvement.
MENTOR HUB framework
The initial MENTOR framework was reintroduced and validated with younger women stroke survivors. Through further exploration and feedback, three key aspects: Holistic, User-centred and Be-continuous (HUB) were consistently highlighted. These insights led to the evolution of the MENTOR framework into the MENTOR HUB Stroke Rehabilitation Framework (Figure 4).
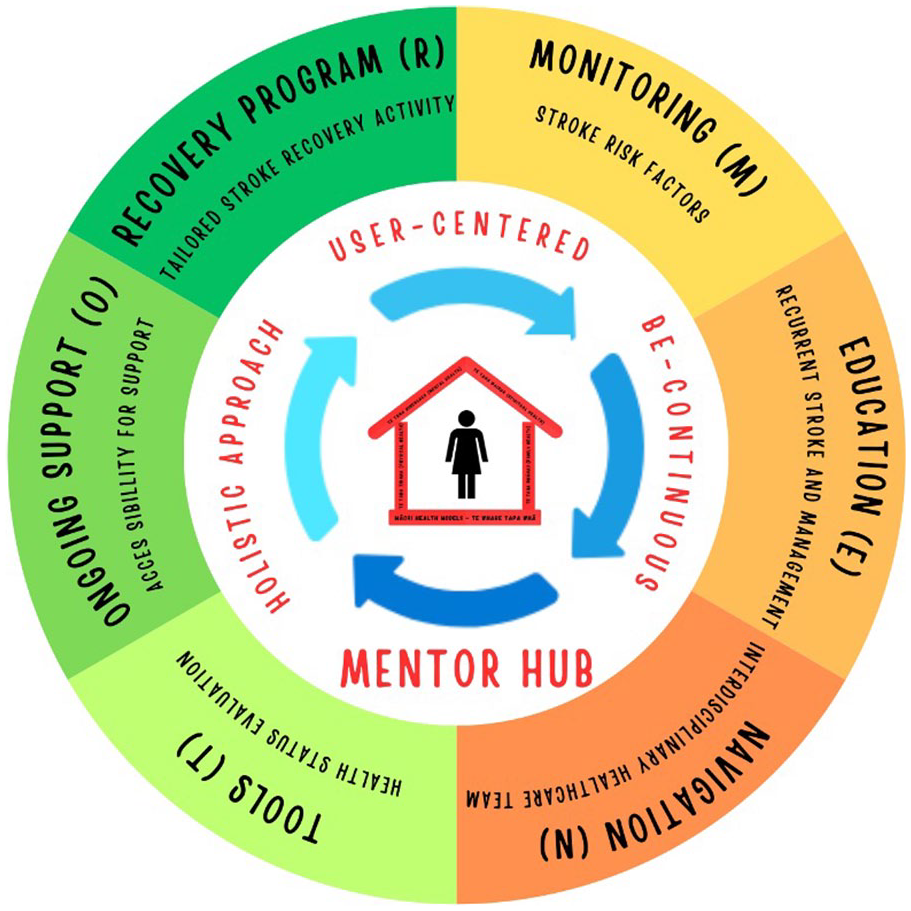
MENTOR HUB stroke rehabilitation framework.
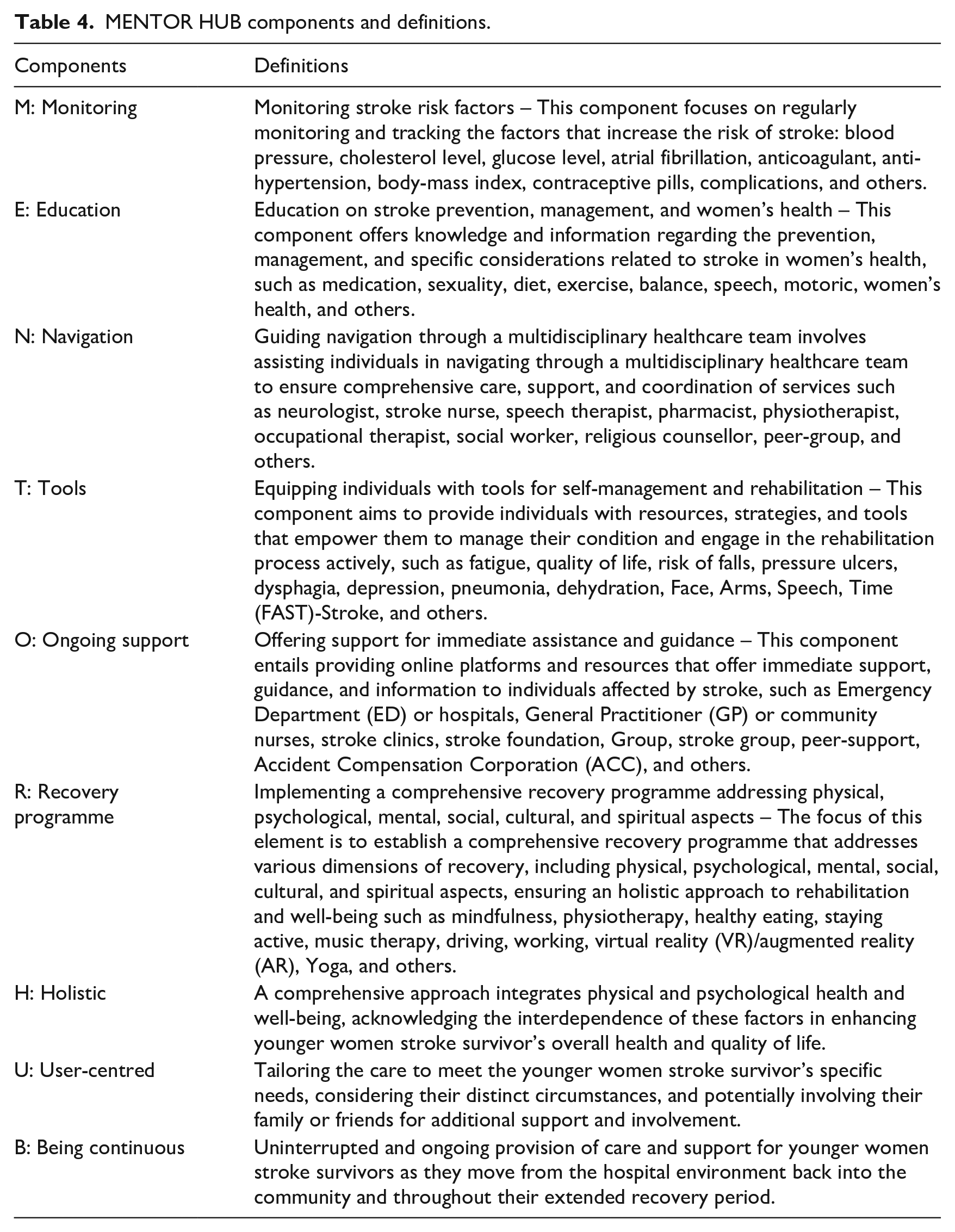
The MENTOR HUB components and definitions are outlined in Table 4 and described below with illustrative quotes highlighting the three core aspects: Holistic, User-centred and Be-continuous (HUB), which were considered essential to consider in any stroke rehabilitation framework to address the unique needs of younger women stroke survivors.
MENTOR HUB components and definitions.
Holistic approach
The first key finding reveals that younger women stroke survivors advocate for a holistic approach in stroke rehabilitation, emphasising the necessity of addressing their multifaceted needs and preferences. One participant stressed the importance of a trusting and intuitive connection, ‘It would be a conversational type, emotional type connection that is based on trust and is intuitively connected to me as a person’ (Lily). Another participant expressed challenges in conveying their experiences to their partner, noting, ‘I did not always tell my partner because he did not know what it was like being in this body now’ (Liz).
Moreover, participants highlighted the role of hobbies in rebuilding confidence. For instance, Linda shared, ‘Cooking is a hobby of mine, and I loved to cook for people. That was how I could manage myself and try to get back to being around people after my stroke. It was a way of rebuilding my confidence’. Additionally, a participant, Lala, emphasised the need to consider the realities faced by young women, including childbearing and maternity issues, during stroke recovery, stating, ‘This was a reality for people that are young women’. These quotes collectively underscore the younger women stroke survivors’ firm assertion that a comprehensive and holistic approach to stroke rehabilitation is imperative for achieving optimal outcomes and enhancing overall well-being.
User-centred approach
The second key finding highlights the crucial need for a user-centred approach in stroke rehabilitation, emphasising user-friendly and accessible care. Participants detailed challenges in using technology, with one person expressing difficulties due to limited mobility, stating, ‘Most people that have had a stroke cannot use a phone. They only have one hand. For the first three months, four months, I could not use a phone at all, Because I could not use either hand’ (Lily). Another participant voiced concerns about creating universally effective apps, noting, ‘For a couple of reasons. Um, I think it is hard to put together an app that will work for everyone’ (Chloe).
Additionally, participants recognised that some stroke survivors may face cognitive difficulties, particularly with complex technologies. One participant remarked, ‘I guess for me, I am thinking, there is many people that have difficulty. It is cognitive, isn’t it? And difficulty, if it gets too complex, especially with technology’ (Lala). These insights underscore the imperative of designing stroke rehabilitation programmes and tools with a user-friendly and inclusive approach, considering varying needs and capabilities, thereby enhancing the overall care experience and recovery journey for stroke survivors.
Aligned with the user-centred approach, any stroke rehabilitation programme must recognise the significance of goal-setting in stroke recovery. Linda emphasised the importance of regaining confidence swiftly, stating, ‘You had to regain your confidence as quickly as possible because you could start to repair and heal. You did need confidence, which was a big thing after a stroke. A very, very big thing!’ Another participant, Chloe, articulated her desire for a personalised goal-setting process that empowers stroke survivors to take ownership of their recovery journey. Chloe stressed the active involvement of stroke survivors in developing their own ideas and goals, noting, ‘It is quite important to get the person that had the stroke to come up with the ideas. To create them themselves, even if they had to hold the pencil or the pen or stand silent until they said something, till they came up with the ideas. Because otherwise, it was not their idea’. Chloe expressed dissatisfaction with generic and predetermined goals often set by rehabilitation teams:
“I did not like getting the generic dished out to me. I liked to get things tailored for me. I liked to get more personal things. My goal was to go home. They were set for, and everybody set all these goal plans and things for me, but I never set any of them”
Being continuous
The final key finding underscores the significance of continuity in any stroke rehabilitation programme, emphasising the need for continuous care throughout the stroke recovery process. Participants stressed the importance of ongoing support and a seamless transition from the hospital to home. Lily expressed this need, stating, ‘And then the person would feel that care, that continuity of care. Often patients say that they do not have continuity of care once they get home’.
Discussion
The findings from all phases of this study highlight the critical need for a robust framework for stroke rehabilitation tailored specifically for younger women stroke survivors which addresses their unique challenges. This aligns with previous research by Gall et al. (2018) which highlighted the heightened challenges faced by women in daily activities, lower health-related quality of life (HRQoL) and increased susceptibility to post-stroke depression. Moreover, depression rates were notably higher in young women compared to men (Caponnetto et al., 2021; Eddelien et al., 2022). Previous study also recognised the unique challenges that younger women stroke survivors face in self-care, daily activities, pain management and emotional well-being, resulting in comparatively lower levels of well-being than male stroke survivors (Phan et al., 2019). As a result, addressing their specific needs and providing adequate support is likely to alleviate their burden and mitigate potential psychological challenges they may face during their recovery journey.
Participants in this study also emphasised the value of a user-centred approach, in which care is tailored to the specific needs and preferences of younger women stroke survivors. To effectively meet these specific needs, the framework must incorporate user-centred principles, allowing for tailored care that reflects the individual preferences and requirements of the younger woman stroke survivor. Including the younger woman stroke survivor in any plan of care would be necessary as previous study demonstrated that patient involvement in rehabilitation decision-making is crucial for optimising healthcare outcomes (Kristensen et al., 2016). Similarly, Martín-Sanz et al. (2022) reinforced the importance of active patient involvement in decision-making and goal-setting. Furthermore, self-directed rehabilitation therapies for stroke survivors have been found to be successful (Noukpo et al., 2022). Therefore, tailored care, user involvement, and integration of self-directed interventions are likely to enhance the overall quality of care for younger women stroke survivors. Empowerment and patient-centred care emerge as key themes in stroke survivors’ rehabilitation experiences (Brown et al., 2014; Lee et al., 2022; Peoples et al., 2011). By adopting a framework that facilitates engagement, healthcare providers can ensure that stroke survivors regain control over their lives, thereby improving their rehabilitation experiences (Wolfenden and Grace, 2015). According to Hartford et al. (2019), approaching stroke care from an empowerment perspective could address shortcomings and disparities in stroke rehabilitation, as reported by stroke survivors, spousal caregivers, stroke support group coordinators, and speech pathologists.
Moreover, the framework should address the necessity for ongoing, long-term support that accommodates the evolving needs of younger women stroke survivors throughout their recovery and reintegration into daily life. Current stroke rehabilitation programmes vary in duration and effectiveness, such as the Comprehensive Post-Acute Stroke Services (COMPASS) programme in Australia, which offers person-centred care for up to 90 days (Duncan et al., 2017). Another Australian-based trial, the ICARUSS programme, focused on stroke risk factor management and continued up to 12 months after stroke (Joubert et al., 2020). In comparison, the UK-based study EXtended stroke Rehabilitation Service (EXTRAS) programme was extended to 18 months after stroke, incorporating continuing assessments and goal-setting (Shaw et al., 2020). Studies have emphasised the importance of ongoing, long-term support in addressing changing difficulties and needs related to disability and community reintegration (Yeung et al., 2015; Zawawi et al., 2020). A 2021 review found unmet psycho-emotional support needs among community-dwelling stroke survivors (Guo et al., 2021), indicating the importance of ongoing care. Caregivers of stroke survivors require support, respite and, emotional support as well (Malewezi et al., 2022; Sidek et al., 2022).
However, many existing programmes may not fully capture the specific requirements of younger women stroke survivors. The issue of unmet needs among stroke survivors appears to be global and has been extensively researched in many countries, including Australia, Japan, Uganda, Denmark, and Canada (Pallesen, 2014; Shipley et al., 2018; Timm et al., 2023). To adequately address the diverse needs of stroke survivors and caregivers, a transition to a survivor- and caregiver-centred framework is recommended (Bartoli et al., 2023). This approach recognises stroke patients as unique individuals and promotes positive care experiences throughout their recovery journey (Chiang et al., 2023). Ensuring a smooth transition from acute care to post-acute care and community reintegration is vital, particularly as physical recovery reaches a plateau (Takashi et al., 2022). A comprehensive framework can facilitate these transitions, providing stroke survivors with the necessary support to navigate their recovery effectively (Dworzynski et al., 2015). Although this study has limitations, such as a small participant rate due to the impacts of COVID-19, the insights gathered provide a foundation for developing a more effective framework tailored to the experiences of younger women stroke survivors. Future research should focus on refining the framework through the incorporation of feedback from stroke survivors and their families, ensuring that it remains adaptable and relevant to the evolving needs of this population. Another area for further research is to test the MENTOR HUB Stroke Rehabilitation Framework in practice.
Conclusion
The MENTOR HUB Framework presents a comprehensive approach to stroke rehabilitation that acknowledges the unique challenges faced by younger women stroke survivors. By integrating both physical and emotional dimensions of care, the framework adopts a user-centred, interdisciplinary model that provides continuous support across all phases of recovery. This holistic approach is anticipated to shape future stroke rehabilitation practices by addressing not only the physical recovery but also the psychological and emotional well-being of survivors, thereby improving their overall quality of life. Future research includes testing the MENTOR HUB Stroke Rehabilitation Framework in practice and refining it based on the feedback from younger women stroke survivors and their families.
Key points for policy, practice and/or research
Develop gender-specific stroke screening tools to enhance recognition, management, and rehabilitation.
Leverage the MENTOR HUB framework for cost-effective, user-centred stroke rehabilitation tailored to patient needs.
Promote interdisciplinary approaches within MENTOR HUB to address challenges of younger women stroke survivors, improving outcomes.
Establish programmes to increase healthcare professionals’ awareness of the specific rehabilitation needs of younger women stroke survivors.
Validate the MENTOR HUB’s effectiveness in recovery outcomes, guiding the development of comprehensive rehabilitation programmes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from UAHPEC with reference number: 21438.