
Abstract
Background:
Virtual reality (VR) allows burn patients to engage in a virtual world and can provide patients with a distraction from pain.
Aims:
To assess the types of VR models available for use in the adult burn population and determine their efficacy regarding pain management and other health outcomes.
Methods:
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines guided this review. We searched the databases of CINAHL and PubMed to identify the peer-reviewed journals that matched the inclusion criteria. We utilised the Joanna Briggs Institute (JBI) quality appraisal tools to evaluate the selected studies.
Results:
The search results ended in nine studies. The types of VR identified included passive and active scenarios with a focus on natural environments. The findings of the quantitative studies indicated that VR decreased patients’ pain during therapeutic interventions. In contrast, the findings of most qualitative studies revealed that VR provided distraction for patients during wound care. Regarding secondary outcomes, VR was shown to improve hand rehabilitation, anxiety and pulmonary functions.
Conclusion:
This integrative review contributes to nursing by synthesising the evidence on VR as a non-pharmacological and complementary intervention to manage pain among adult burn patients. The implications of this review in nursing practice include consideration of staff training and technical support for practising nurses to successfully and safely implement the VR experience into their practice. Healthcare policies should delineate the best practices for VR use among burn patients to guide its implementation, funds to cover the costs of VR equipment, and equitable access to VR experience for all adult burn patients.
Introduction
A burn injury is a form of tissue damage that can result from thermal, chemical, cold, friction, electrical or other sources (Jeschke et al., 2020). An estimated 86% of burns are caused by thermal sources, such as flames, hot solids and scalding liquids (Schaefer and Szymanski, 2023). The depth of a burn ranges from first-degree (i.e. purely superficial) to fourth-degree (i.e. impacting deeper tissues, such as muscles or bones). The size of a burn is typically described as the percentage of total body surface area (TBSA) involved (Jeschke et al., 2020). Minor burns involve <10% of the TBSA (Jeschke et al., 2020).
Burn injuries pose a global public health challenge causing an estimated 180,000 deaths per year, mainly in middle- and low-income countries (World Health Organization (WHO), 2023). Burns are also a common cause of disability, chronic pain and prolonged hospitalisation, resulting in a profound economic burden. In 2020 alone, approximately $3.8 billion was spent on burn injury-related medical costs in the United States (Centers for Disease Control and Prevention, 2023). Based on WHO data, the average total healthcare cost for a burn injury varies globally, ranging from $704 to $717,306 per patient (WHO, 2023). The estimated average cost of treating a burn injury within the UK’s National Health Service is approximately £16,924 per patient (Guest et al., 2024).
Pain associated with burn injuries is complex and includes acute and chronic pain. Acute pain is present during the healing process and is directly related to the burn injury (Castana et al., 2009). Chronic pain persists after burns have healed and is most commonly neuropathic in nature (Griggs et al., 2017). Acute pain consists of background pain at rest, breakthrough pain when background pain is exacerbated, and procedural pain during interventions (Romanowski et al., 2020). Burn injury treatment involves multiple interventions to facilitate the healing process, such as extensive wound dressing changes and physiotherapy, which can intensify the patient’s pain (Griggs et al., 2017). The intensity of pain from a burn can differ significantly among people and is largely determined by the burn’s depth, its location on the body, and an individual’s pain threshold. Generally, the depth of a burn significantly influences the level of pain, with superficial burns causing more pain compared to full-thickness burns, where nerve endings are damaged or destroyed (Morgan et al., 2018).
Inadequate pain control during interventions can lead to patients’ reluctance or refusal to comply with the prescribed treatment regimen, resulting in negative health outcomes. Therefore, appropriate pain management is central to the burn recovery process. Furthermore, insufficient pain control has been linked to longer wound healing, post-traumatic stress disorder, anxiety, lack of sleep, and depression among burn patients (Lan et al., 2023). Pharmacologic therapy is critical in burn pain management, particularly during therapeutic interventions (Romanowski et al., 2020). Opioids are used as first-line treatment medications and have demonstrated significant efficacy in providing pain relief to burn patients. However, prolonged opioid use can lead to many negative outcomes including tolerance and dependence (Von Korff et al., 2011). To address this issue, non-pharmacologic pain control methods have emerged as valuable supplementary interventions for managing pain among burn patients (Gasteratos et al., 2022).
Recent technological advancements have made virtual reality (VR) a viable non-pharmacologic method for managing burn-related pain (Khurram et al., 2022). VR uses a head-mounted display and headphones to immerse users in a computer-generated environment, blocking out the real world (Pottle, 2019). Unlike traditional video games, VR allows realistic interaction with virtual elements, creating a sense of presence. This immersive experience helps burn patients become fully engaged in the virtual world, effectively distracting them from their pain and real-life experiences (Khurram et al., 2022).
VR has been extensively studied as a non-pharmacologic pain management technique in paediatric patients with burn injuries and has been shown to be a valuable tool (Armstrong et al., 2022; Fatma and Ghada, 2019; Hoffman et al., 2020; Khadra et al., 2018; Nordgård and Låg, 2021; Xiang et al., 2021). Furthermore, the American Burn Association guidelines recommend in-depth research on VR as a non-pharmacologic pain management technique among burn patients (Romanowski et al., 2020). Despite limited research, the application of VR in adult burn patients remains an area of interest. Additionally, since most VR research has been conducted in the United States, it is important to synthesise this evidence to extend its reach to other countries, particularly low-income countries, which have the highest prevalence of burn injuries. Research gaps identified from previous study findings indicate that there is no clear consensus on whether active or passive VR is more beneficial for patients. Additionally, the optimal frequency and duration of VR use for pain relief are not well defined (Viderman et al., 2023). The main purposes of this review were to assess the types of VR models available for use in the adult burn population and determine their efficacy regarding pain management and other health outcomes.
Methods
Selection criteria
Study selection
We selected quantitative studies (cross-sectional, randomised control trials (RCTs), quasi-experimental studies), mixed-methods and qualitative studies for this review. The criteria for inclusion were (1) published studies in English from peer-reviewed journals between 1 January 2013 and 1 October 2023, (2) studies with participants aged 18 years and older and (3) studies that discussed VR as a pain management intervention for burn pain. The study period was selected to reflect the most current research on pain management interventions for burn pain and because of recent VR technological advancements. The criteria for exclusion were (1) studies with participants younger than 18 years old; (2) literature reviews, conference abstracts, study designs and expert opinions and (3) studies that are not in English.
Description of participants
The participants in the selected studies were 18 years old or older and had burn injuries of any size, depth and healing stage that matched the criteria for inclusion. Individuals who received inpatient or outpatient burn care were considered for this review.
Description of interventions
Studies that incorporated any type of VR technology as a pain management intervention for burn pain including physical therapy and wound dressing changes were included in this review. The studies utilised VR technology in active and passive scenarios, and some allowed participants to choose the VR simulation.
Description of outcome measures
We evaluated the management of pain related to any aspect of the burn injury healing process, including wound care and physical therapy as the primary outcome measure of this study. We also assessed additional health outcomes as secondary measures.
Search method
This review utilised the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) as a framework to execute our literature search (Moher et al., 2009). A research librarian assisted us in creating the search plan. The PubMed and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases were searched using terms such as augmented reality, virtual reality, VR, mixed reality, burn, burns and burn injury. Medical subject heading terms were used when available and customised to each database. In addition to the included studies, the researchers manually reviewed the reference lists to find any additional relevant papers. The process used in this integrative review is detailed in the PRISMA diagram (Figure 1).
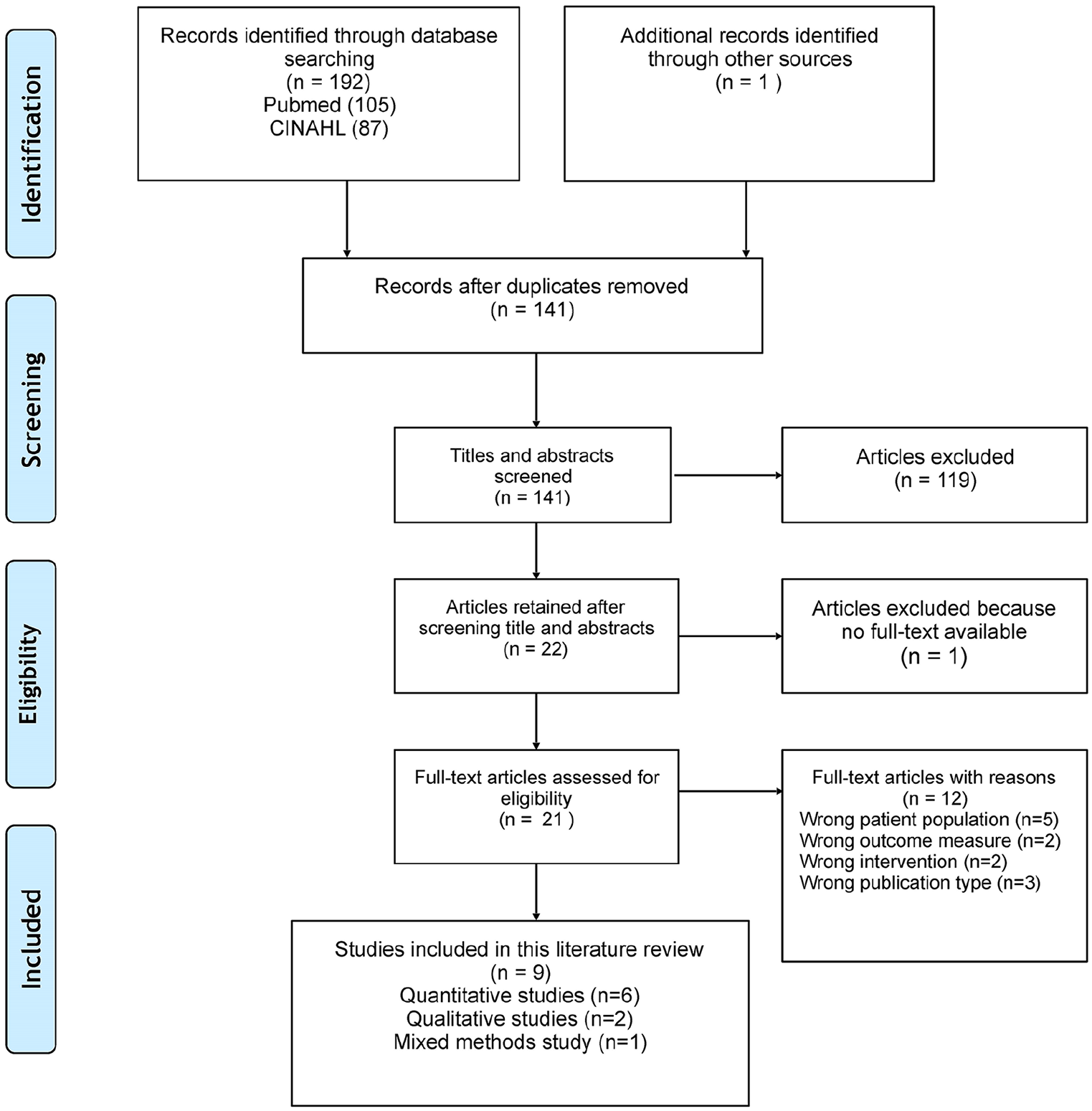
PRISMA diagram.
Quality appraisal
The quality of the studies was evaluated by the first author in terms of their reliability, applicability and conclusions using the Joanna Briggs Institute (JBI) critical appraisal tools, and the second author verified the results (Table 1). The JBI critical appraisal checklists were used for different study types: qualitative studies (Lockwood et al., 2015), RCTs (Tufanaru et al., 2019), mixed-methods and quasi-experimental studies. For mixed-methods, the analytical cross-sectional checklist was used for quantitative parts, and the qualitative checklist for qualitative parts (Moola et al., 2019). The majority of the checklist responses indicated that these studies were of high quality.
Quality appraisal results qualitative studies.
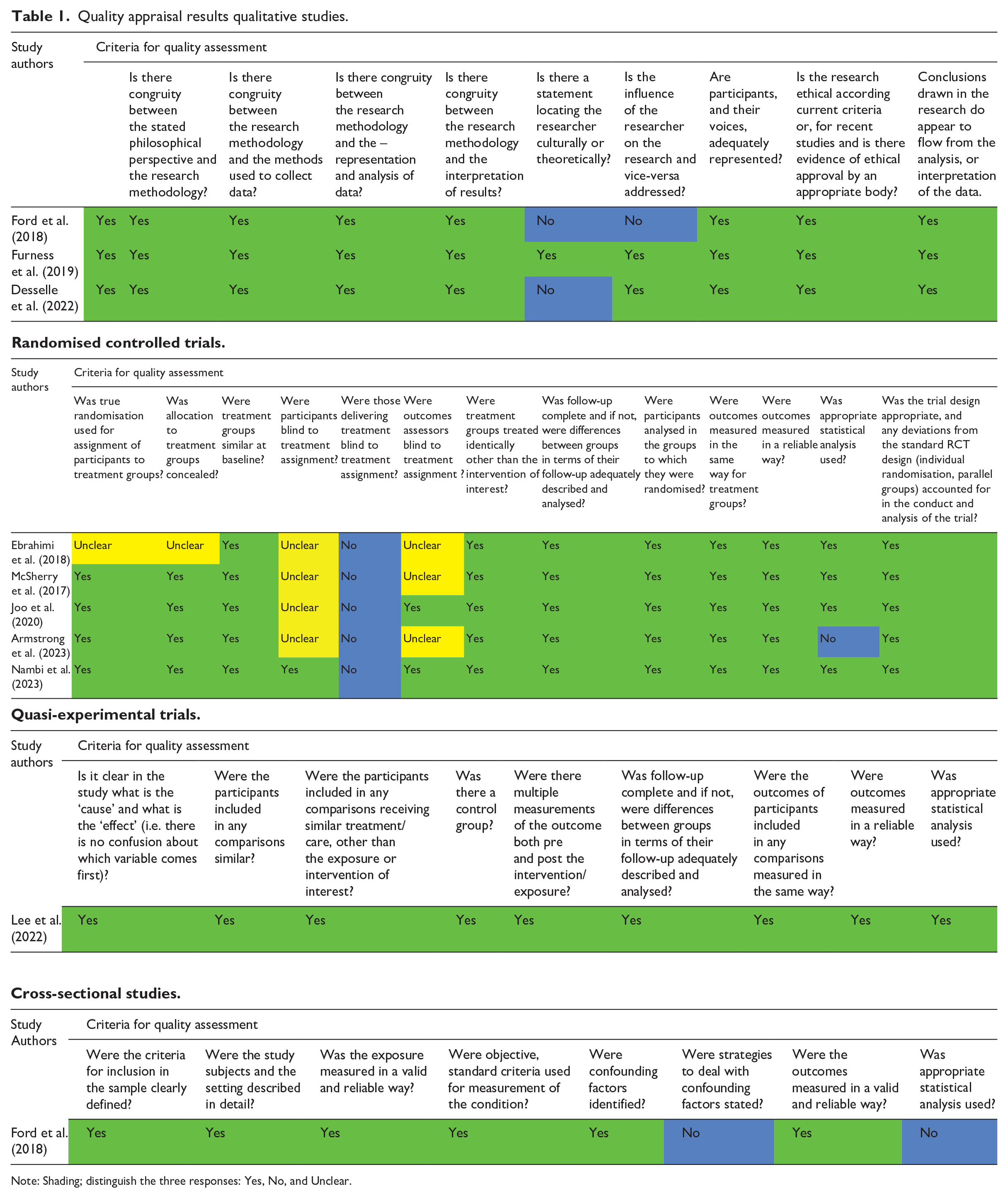
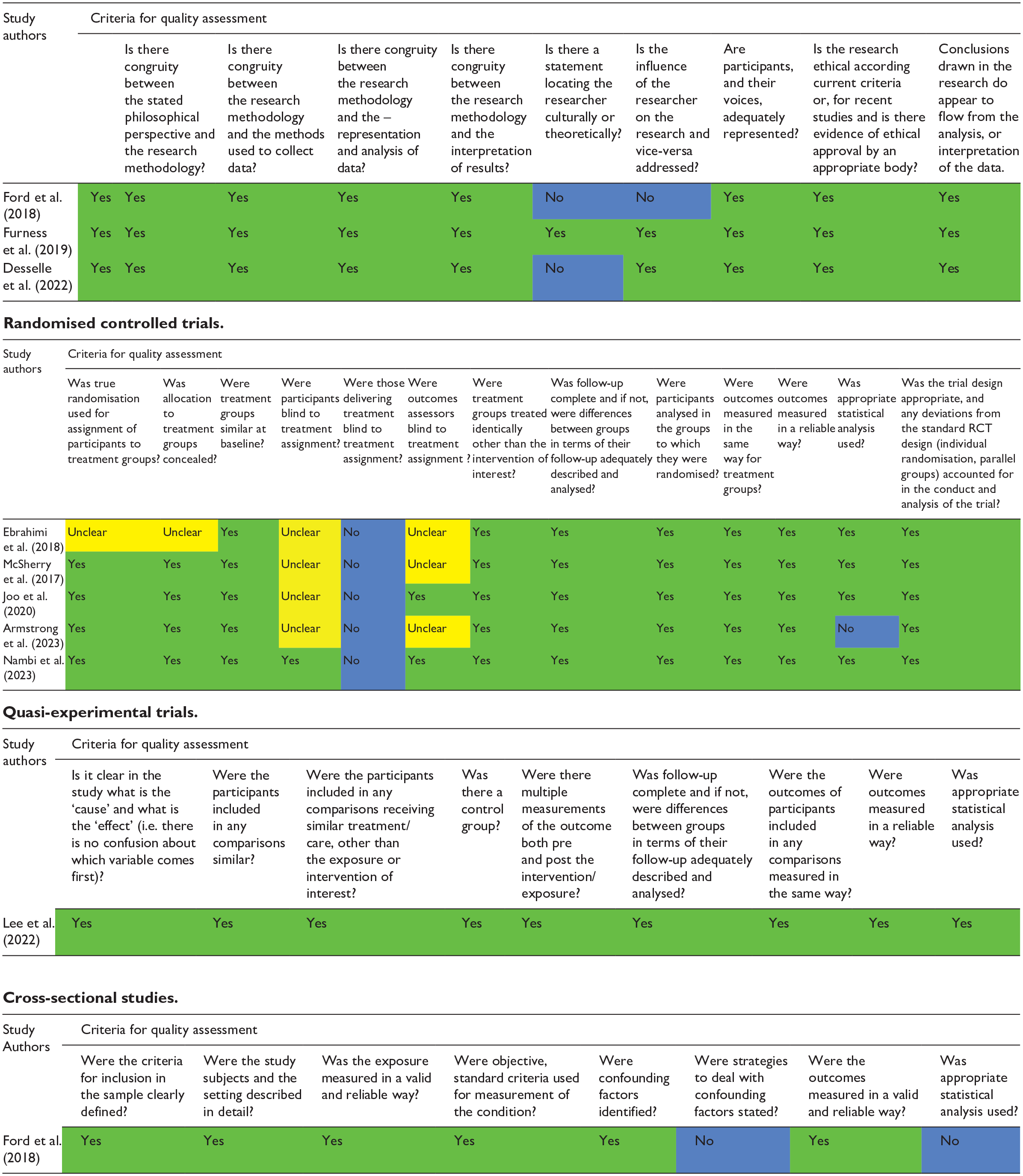
Note: Shading; distinguish the three responses: Yes, No, and Unclear.
Data extraction
We used the following criteria for data abstraction: (1) publication details (author and year), (2) study location and design, (3) details of the sample (age, gender and sample size), (4) intervention details (type of VR used, length of time, reason for pain management), (5) outcome results (pain measurement) and (6) adverse effects of VR use.
Results
Out of the nine papers that met the inclusion criteria, three were conducted in the United States, two in South Korea, one in the United Kingdom, one in Saudi Arabia and one in Australia. See Table 2 for the details about these studies.
Data extraction.
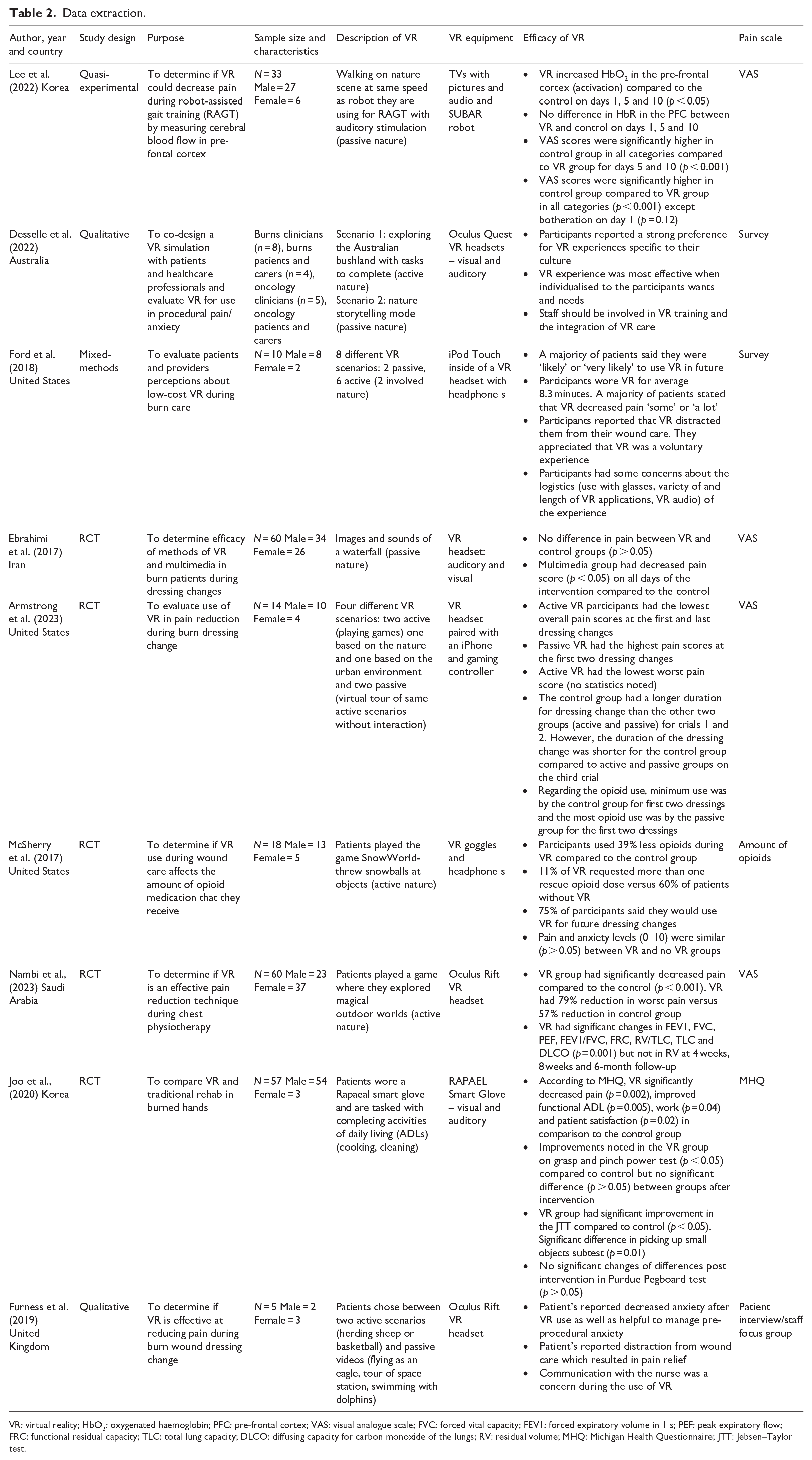
VR: virtual reality; HbO2: oxygenated haemoglobin; PFC: pre-frontal cortex; VAS: visual analogue scale; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; PEF: peak expiratory flow; FRC: functional residual capacity; TLC: total lung capacity; DLCO: diffusing capacity for carbon monoxide of the lungs; RV: residual volume; MHQ: Michigan Health Questionnaire; JTT: Jebsen–Taylor test.
Study characteristics
Regarding the study designs, there were five RCTs, two qualitative studies, one quasi-experimental study and one mixed-methods study. The total sample size was 261 adult burn patients. The majority of patients were male in six studies (Armstrong et al., 2023; Ebrahimi et al., 2018; Ford et al., 2018; McSherry et al., 2017; Joo et al., 2020; Lee et al. 2022) and female in two (Furness et al., 2019; Nambi et al., 2023). One study did not list gender ratios (Desselle et al., 2022). The VR use varied among the selected studies. Six of the studies utilised VR during burn wound care or dressing change (Armstrong et al., 2023; Desselle et al., 2022; Ebrahimi et al., 2018; Ford et al., 2018; Furness et al., 2019; McSherry et al., 2017) rehabilitation in two studies (Joo et al., 2020; Lee et al., 2022), and chest physiotherapy in one study (Nambi et al., 2023). Regarding the type of VR equipment used, one study developed low-cost VR equipment using a refurbished iPod Touch in a VR headset (Ford et al., 2018). Three studies used Oculus VR systems (Desselle et al., 2022; Furness et al., 2019; Nambi et al., 2023). Seven studies employed various VR headsets (Armstrong et al., 2023; Desselle et al., 2022; Ebrahimi et al., 2018; Furness et al., 2019; Ford et al., 2018; Nambi et al., 2023). Joo et al. (2020) used a smart glove, and Lee et al. (2022) used a TV that played VR during robot-assisted gait training.
Types of VR
Active versus passive VR
The studies used passive VR, active VR or a combination. In active VR, participants’ complete tasks, such as herding sheep, cooking or cleaning, or they play games, such as throwing snowballs at objects and directly engaging with the VR simulation. In passive VR, participants observe a VR simulation, such as a virtual tour of an environment, without engaging with it. Four studies allowed the participants to choose active or passive VR scenarios (Armstrong et al., 2023; Furness et al., 2019; Desselle et al. 2022; Ford et al., 2018), three offered only active VR scenarios (Nambi et al., 2023; McSherry et al., 2017; Joo et al., 2020) and two offered only passive VR scenarios (Ebrahimi et al., 2018; Lee et al., 2022).
Natural versus urban environments
All studies involved nature in some capacity. Five studies were fully nature-based (Desselle et al., 2022; Ebrahimi et al., 2018; Lee et al. 2022; McSherry et al., 2017; Nambi et al., 2023). For example, participants explored the Australian bushland and completed a treasure hunt (Desselle et al., 2022) or observed the sights and sounds of a waterfall (Ebrahimi et al., 2018). Three studies included natural scenarios and urban scenarios, such as taking virtual tours of cities, playing basketball in a gym or viewing the inside of a space station (Armstrong et al., 2023; Ford et al., 2018; Furness et al., 2019). In one study, participants completed indoor (e.g. cooking, grocery shopping) or outdoor (e.g. fishing) tasks (Joo et al., 2020).
Efficacy of VR
Pain management
Although all six quantitative studies assessed pain, the measurement methods varied. In four studies, the participants used the visual analogue scale (VAS) to rate their pain during the VR experience (0 = no pain, 10 = worst pain); (Armstrong et al., 2023; Ebrahimi et al., 2018; Nambi et al., 2023; Lee et al., 2022). Active nature VR was used with chest physiotherapy among patients who had chest burns in one of the RCTs which was conducted in Saudi Arabia (Nambi et al., 2023).The participants reported a significant decrease in the intensity of the pain in the VR group (by 79% reduction) compared to those group who did not receive VR (57% reduction; p < 0.001), and these changes lasted for 6 months after the VR use (Nambi et al., 2023). During gait training with the help of a robot, VR that displayed the sights and sounds of a walk through nature was provided to burn patients (Lee et al., 2022). The findings from this study indicated that VR significantly decreased patients’ VAS scores for pain on all days of rehabilitation (p < 0.001) in comparison to the control group who did not receive the VR (Lee et al., 2022). From a pilot RCT conducted in the United States, burn patients were categorised into three groups during their wound dressing change: (1) the active VR group played games, one based on nature and the second one based on the urban environment; (2) the passive VR group had a virtual tour of same active scenarios without interaction and (3) the control group received the routine care (Armstrong et al., 2023). Data analysis revealed that the active VR group reported decreased overall pain in two of the three wound dressings with the lowest worst pain (Armstrong et al., 2023). However, findings from an RCT from Iran which used three different groups (group 1 = VR using images and sounds of a waterfall using a VR headset, group 2 = multimedia group which viewed the same images as the VR group but on a TV, and group 3 = control group) and assessed their pain during burn dressing change (Ebrahimi et al., 2018). The results of this study indicated comparable pain scores between group 1 (VR group) and group 4 (control group) and implementation of the VR did not change the pain scores during burn dressing change. Interestingly, the lowest pain scores were noted among the multimedia group (group 3) in this study (Ebrahimi et al., 2018).
A subset of the Michigan Hand Outcomes Questionnaire measured pain among burn patients in Korea who underwent VR-based rehabilitation revealed a significant reduction of pain scores among the VR group in comparison to the control group (p = 0.002; Joo et al., 2020). Findings from an RCT in the United States reported significantly less use of opioids and decreased requests for opioids during wound care among the patients who played games using the VR in comparison to the control group (p = 0.02 for both; McSherry et al., 2017).
All three qualitative studies relied on patients’ descriptions of their pain relief experiences with VR. The major themes from these studies were related to concerns about logistics and the integration of VR into routine care (Desselle et al., 2022; Ford et al., 2018; Furness et al., 2019). The identified problems included communication with the nurses (Furness et al., 2019), challenges and discomfort while using a VR headset with glasses (Ford et al., 2018), and the costs of VR-related staff and resources (Desselle et al., 2022). In two studies, wound care procedure tolerance increased and pain decreased because VR offered visual and other distractions (Furness et al., 2019; Ford et al., 2018). In other words, actively thinking about the VR simulation took the participants’ minds off the wound care procedure. Findings from a qualitative study in Australia reported themes related to the individualisation of the VR experience to the participants, consideration of their culture, and geographical location (Desselle et al., 2022).
Secondary outcomes
The measured secondary outcomes included increased cerebral blood flow, hand rehabilitation progress, improvement in lung capacity measures, anxiety management, and wound dressing change duration. Findings of a study that implemented robot-assisted gait training with the support of VR, found that VR significantly increased oxygenated haemoglobin (HbO2) in the pre-frontal cortex compared to the control group (p < 0.05); (Lee et al., 2022). The results of the study which measured the hand rehabilitation progress indicated that the VR group had significant improvements in the grasp and pinch power test (p < 0.05), functional ADLs (p < 0.05), work (p < 0.05), and patient satisfaction (p < 0.05; Joo et al., 2020). Active nature VR was used with chest physiotherapy among patients who had chest burns and the findings indicated that the VR group significantly improved in various lung capacity tests (p = 0.001) compared to the control group; such as increased forced expiratory volume, peak expiratory flow, and total lung capacity (Lee et al., 2022). Findings of a qualitative study indicated that integration of the VR decreased patient anxiety, especially pre-procedural anxiety, during burn dressing change (Furness et al., 2019). The patients who participated in VR also benefitted from a shorter dressing change duration compared to the control group in two of the three trials (Armstrong et al., 2023).
Discussion
The goal of this integrative review was to evaluate the different types of VR models available for use in adults with burn injury and to determine their efficacy in pain management among adults with burn injury. Assessment of the types of VR models available revealed the use of both active and passive VR with a focus on nature themes. Most of the reviewed studies supported VR in the adult burn population as an intervention to support pain management. Five of the six quantitative studies and all three qualitative studies reported the benefits of VR for adult burn patients in terms of pain reduction.
A previous review, analysed the effectiveness of VR on burn patients’ pain during wound care and found that immersive VR (i.e. active VR) resulted in a significant reduction of pain during wound dressing compared to the control. However, no significant differences in pain were noted between non-immersive VR (i.e. passive VR) and the control during wound care (Norouzkhani et al., 2022). In contrast, the present review identified that passive VR had a positive outcome with decreased pain during wound care. The differences in these findings could be related to the context in which VR was used. For example, in the present review, one study used passive VR during robot-assisted gait training and found it to be useful in managing pain (Lee et al., 2022). Furthermore, the previous systematic review included studies from both paediatric and adult patients, and the findings did not show that VR is effective for pain management among adult patients (Norouzkhani et al., 2022). In contrast, the present review’s findings indicate that VR might be an effective intervention for pain management in adults with burn injury during various types of treatment. An explanation for this difference could be the limited number of studies that measured the effectiveness of VR in adults with burn injuries in the previous systematic review (Norouzkhani et al., 2022).
An unexpected finding in the present review was that findings from an RCT showed no notable differences in the pain scores of the VR and the control groups during wound dressing change but observed a lower pain score that was statistically significant in its multimedia group (Ebrahimi et al., 2018). A possible explanation for this could be that VR was implemented using a VR headset to play images and sounds, whereas in the multimedia group, digital images and sounds were displayed via a television screen. The patients might have preferred the later technique as they did not need to wear any external appliances.
Despite the benefits of VR for burn patients, it may not be suitable for everyone and can cause discomfort for some individuals. Out of the nine studies reviewed, only five addressed patient comfort or eligibility to use VR during burn care. Two studies excluded participants with head and neck burns (Armstrong et al., 2023; Furness et al., 2019). A third study excluded participants with higher burn body surface area as they were admitted to the Intensive Care Unit (ICU) (Ebrahimi et al., 2018). Additionally, very few participants reported discomfort in wearing a headset, both with and without glasses, and recommended a wireless headphone to enhance patient comfort (Desselle 2022; Ford et al., 2018).
The present review contributes to the VR literature by showing that VR can be useful in adult burn patients, thereby expanding previous studies’ narrow focus on the paediatric population. This study also shows that VR can be used in a variety of healthcare interventions, including wound care, chest physiotherapy and physical rehabilitation. This review demonstrates the importance of VR-related clinical practice. The cost–benefit analysis of incorporating VR into burn care highlighted economic benefits such as faster wound healing and reduced length of stay, which ultimately lowered hospitalisation costs (Brown et al., 2015; Scapin et al., 2018). Since VR has been shown to be useful in practice, researching optimal implementation and safety related to patient care seems important. Given the importance of pain management, healthcare personnel should include VR experiences as a treatment option for burn patients.
This review’s strengths included its examination of five countries, a variety of interventions in which VR could be useful, and various VR styles. It also showed that multiple study designs – RCTs, qualitative, mixed-methods and quasi-experimental approaches – are feasible for this type of research, which can lead to more such research endeavours.
Implications in nursing
The findings of this review have many implications for nursing, particularly nursing practice and nursing administration. The evidence synthesis from this integrative review highlighted VR as a non-pharmacological pain management intervention in adult patients with burn injuries. As an emerging field, many practising nurses in burn centres should be aware of VR as an innovative intervention and receive adequate preparation and training to implement it in their practice (Furness et al., 2019). Nurse administrators should support the nursing staff to select the appropriate VR experience (active vs. passive) depending on the nature of their burn centres. The practising nurses require continuing education, training, and technical support to successfully and safely implement the VR experience into their practice. Emphasis must be made on incorporating patient preferences into the selection of VR and the patient monitoring and teaching associated with the implementation. Staff should be trained in how to maximise the VR experience and decrease VR-related discomfort and anxiety. Additionally, nurses need to engage in future research to identify the optimal duration and frequency of VR use, thereby contributing to the dynamic and evolving field of VR in nursing practice. More studies are required to identify effectiveness of the VR in modulating chronic and acute pain as well as to determine the patient autonomy in VR use, such as the ability to choose the scenario, is effective in reducing pain.
Implications in health and social care policy
As VR becomes more widely used in burn care, it is essential to establish standardised hospital policies on the best practices for VR use among burn patients. These policies should emphasise ongoing education and staff support to ensure that nursing staff are competent in using VR for patient care. They should also focus on ensuring patient consent, preferences and the protection of patient rights with the use of VR technology in adult burn care. Addressing the costs associated with VR equipment is another important aspect that these policies must cover. They should outline the funding mechanisms to incorporate and maintain VR equipment, and how to support research to evaluate the efficacy of VR use in adult burn care units. Lastly, these policies should aim to ensure that VR experiences are available to all adult burn patients, regardless of their socioeconomic status, to promote equity in healthcare.
Limitations
Regarding limitations, this review might have missed relevant papers that were not written in English. Additionally, it was difficult to draw conclusions from some of the RCTs because they were pilot studies. The small number of participants across the studies (n = 261) and the gender ratio (i.e. six studies had a majority of male patients) were also limitations. More studies on VR experience with adult burn patients with adequate sample sizes are recommended to fill these gaps.
Conclusion
This integrative review highlighted the use of active and passive VR in the pain management of adults with burn injury and contributes to nursing by synthesising the evidence on VR as a non-pharmacological and complementary intervention to manage pain among the adult burn patients. Regarding the efficacy of VR, most of the reviewed studies supported the implementation of VR as an effective strategy to help pain management in adult burn population. The other implications of this review in nursing practice include consideration of staff training and technical support for practising nurses to successfully and safely implement the VR experience into their practice. Emphasis must be given to incorporating patient preferences into the selection of VR and the patient monitoring and teaching associated with the implementation. Healthcare policies should delineate the best practices for VR use among burn patients to guide its implementation, funds to cover the costs of VR equipment and equitable access to VR experience for all adult burn patients.
Key points for policy, practice and/or research
• This integrative review contributes to nursing by synthesising the evidence on VR as a non-pharmacological pain management intervention in adult patients with burn injuries.
• Findings from this review indicated the other health implications of VR among adult burn patients related to their rehabilitation, improving their pulmonary functions, and managing their anxiety.
• The other implications of this review in nursing practice include consideration of staff training and technical support for practising nurses to successfully and safely implement the VR experience into their practice.
• Social care policy implications of this review include funds to cover the costs related to VR equipment, and the equitable access of VR experience to all adult burn patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No ethical permissions were necessary for this integrative review. The purpose of this review was to assess the evidence from the existing published literature.