
Abstract
Background
Lymphoedema is a chronic condition that is estimated to affect up to four people per 1000 of the UK population with this increasing with age. Men account for up to 20% of lymphoedema service caseloads with research focussing upon women affected.
Aims
To retrieve primary qualitative research on the experiences of men with chronic lymphoedema.
Methods
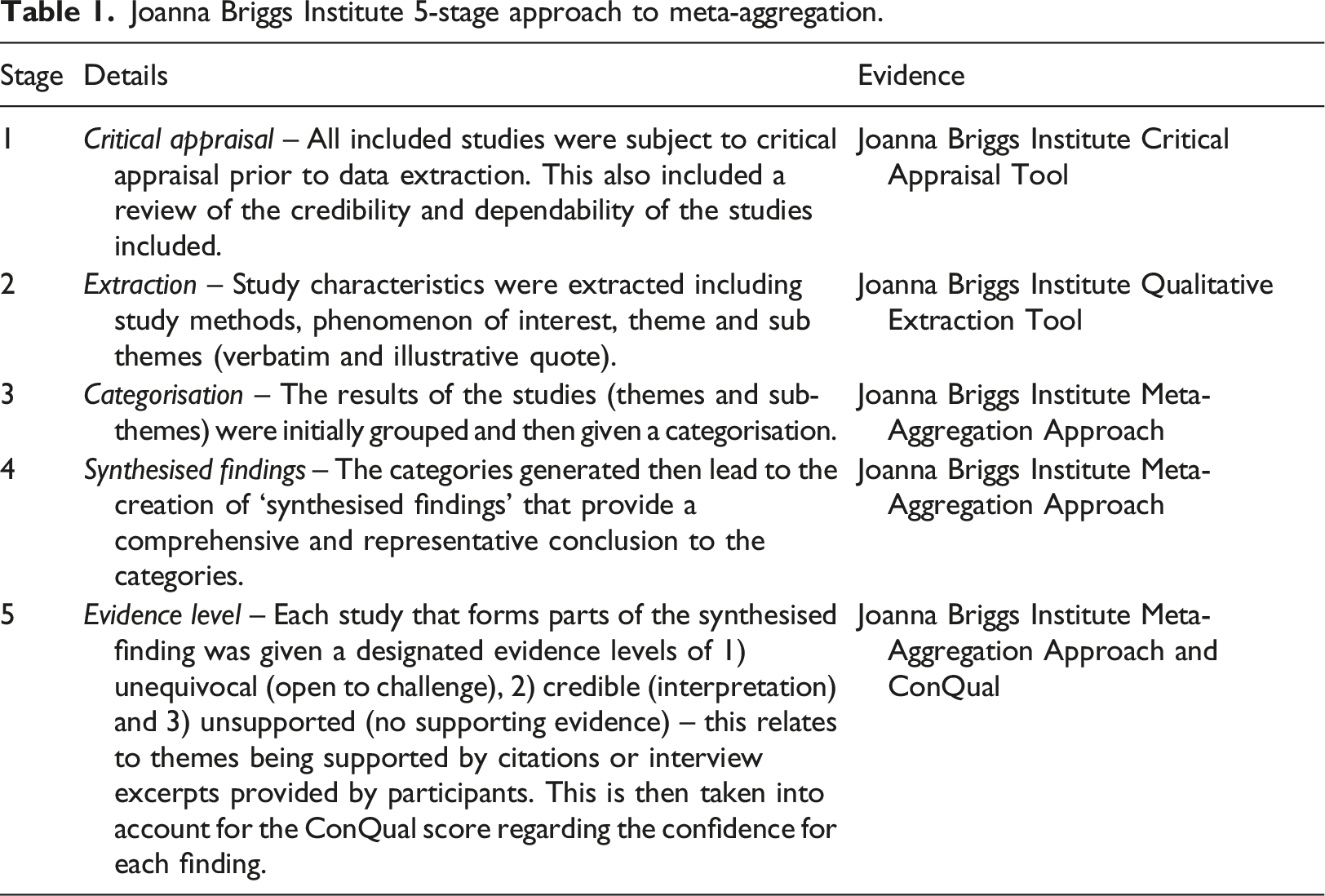
A qualitative review was undertaken using the Joanna Briggs Institute (JBI) meta-aggregation method. A search strategy was applied to 12 databases, from inception to February 2021, with 22 studies identified and appraised. The findings were extracted and synthesised via the JBI approach.
Results
Four synthesised findings were identified: (1) The ‘New Norm’, how diagnosis led to men being faced with a ‘new version’ of themselves; (2) ‘Journey into the Unknown’ relates to the unforeseen diagnosis of the condition; (3) ‘Access’ – challenge in receiving a diagnosis, and support; and (4) ‘Personhood’ – the impact of the condition upon external constructs and relationships.
Conclusions
Men are faced with similar challenges as women coupled with societal expectations with respect to gender identity and expression. This leads to those wishing to engage with men to adopt ‘gender-based tailoring’ within healthcare services, information and support.
Introduction
Chronic oedema is an umbrella term for what is a long-term condition (LTC), in which lymphoedema is a sub-category, with lymphoedema containing other categories, such as primary and secondary (Rankin, 2016). Primary (intrinsic) is due to developmental abnormalities within the lymphatics, such as Milroy’s or Turners; this condition is estimated to affect between one in 2763 and up to one in 8000 people in the United Kingdom (UK) (Cooper and Bagnall, 2016; ILF, 2006; Rankin, 2016). Secondary (extrinsic) is linked to damage to the existing lymphatic system, such as infection, cancer or surgery, with this representing the most reported diagnosis within lymphoedema caseloads (Cooper and Bagnall, 2016; ILF, 2006; Rankin, 2016). It is estimated that between 140 and 250 million people across the world are affected by lymphoedema, with this figure being up to four people per 1000 of the UK population, with 20% of cases involving men, with incidence increasing with age (Cooper and Bagnall, 2016; Moffatt et al., 2019b). This qualitative systematic literature review aims to address an imbalance in the current evidence base between men and women diagnosed with lymphoedema.
Methods
Joanna Briggs Institute 5-stage approach to meta-aggregation.
Search strategy and appraisal
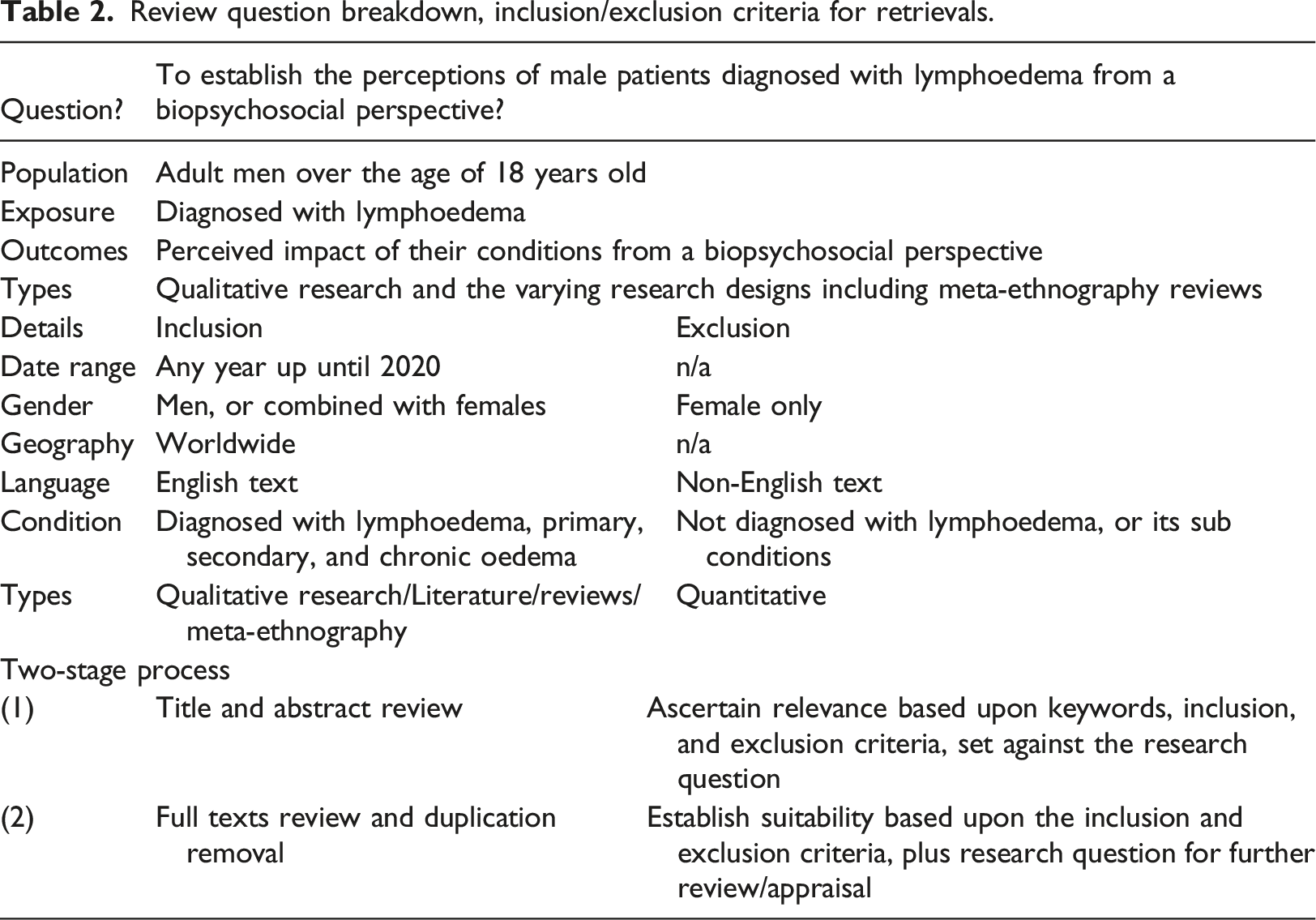
Review question breakdown, inclusion/exclusion criteria for retrievals.
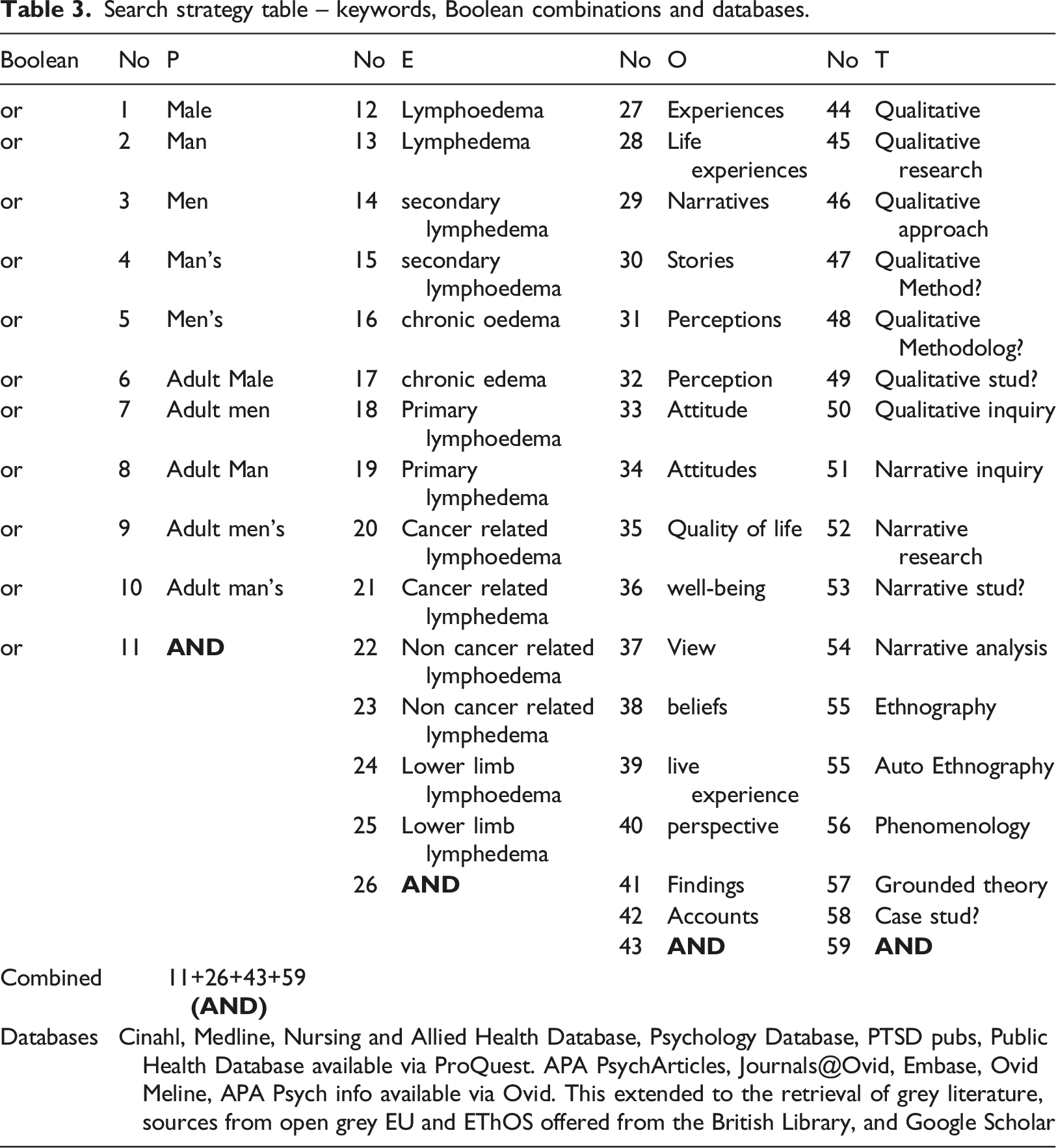
Search strategy table – keywords, Boolean combinations and databases.
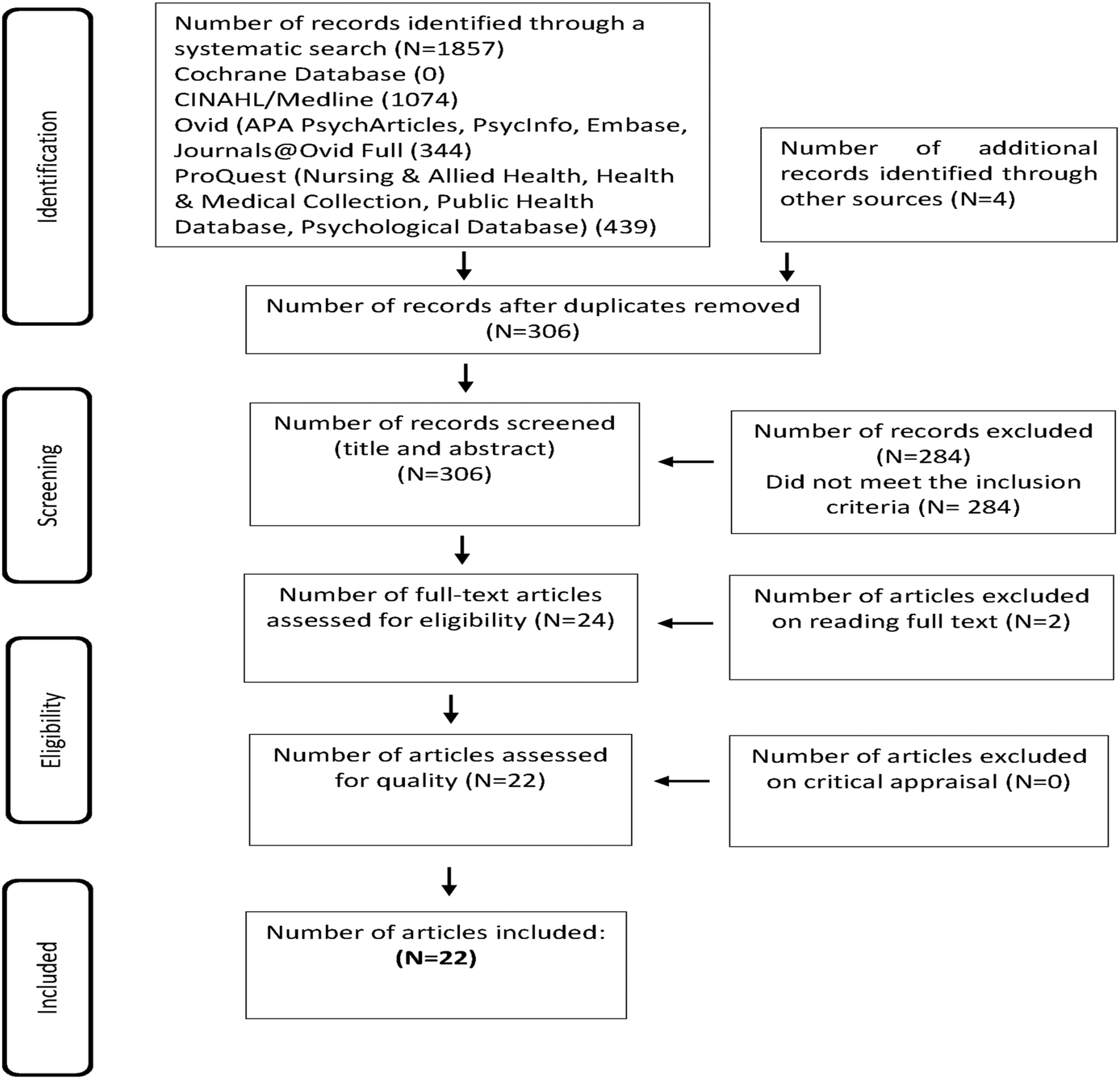
PRISMA flowchart indicating the phases that formed the systematic review
Data extraction table for included studies.

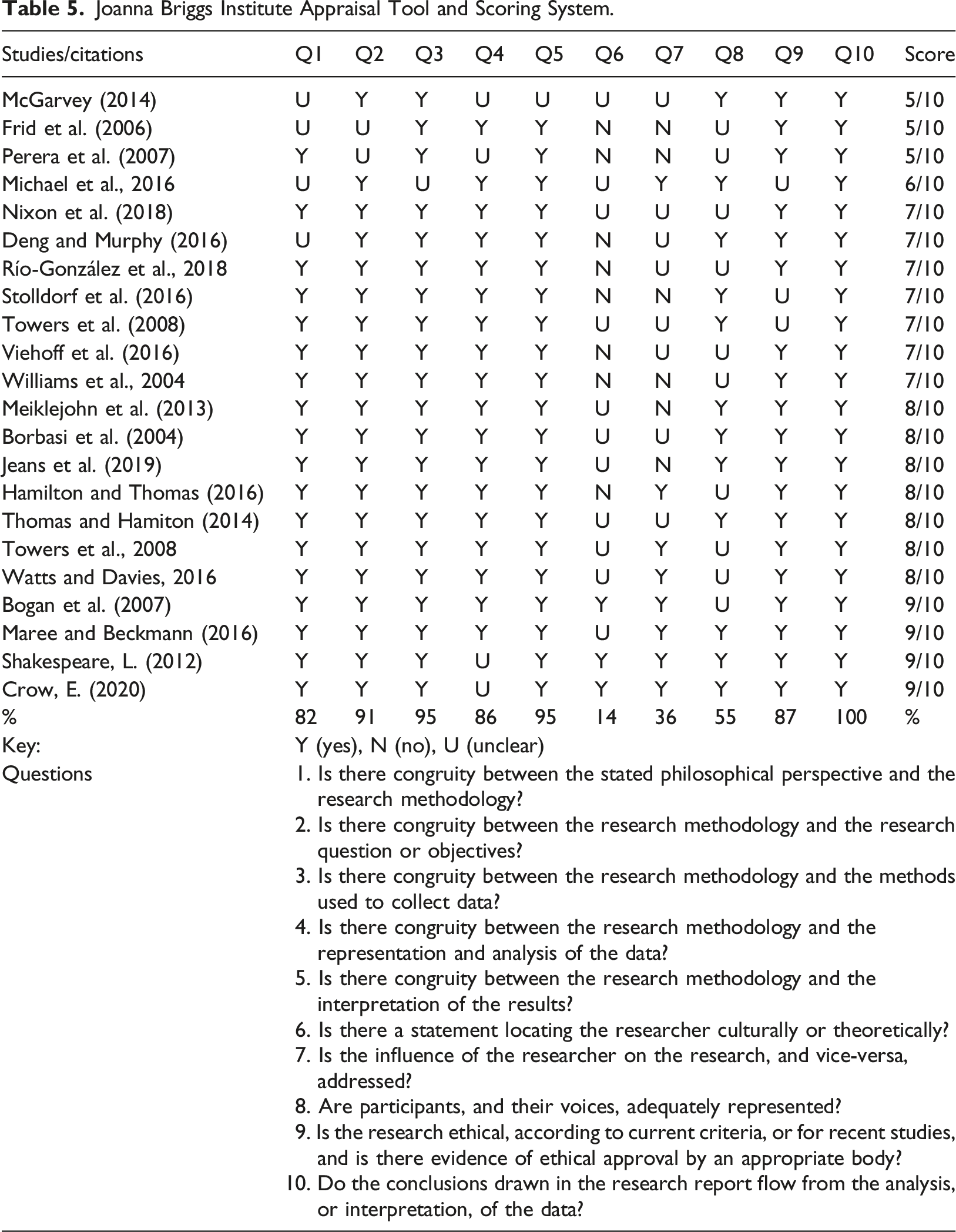
Joanna Briggs Institute Appraisal Tool and Scoring System.
Data synthesis
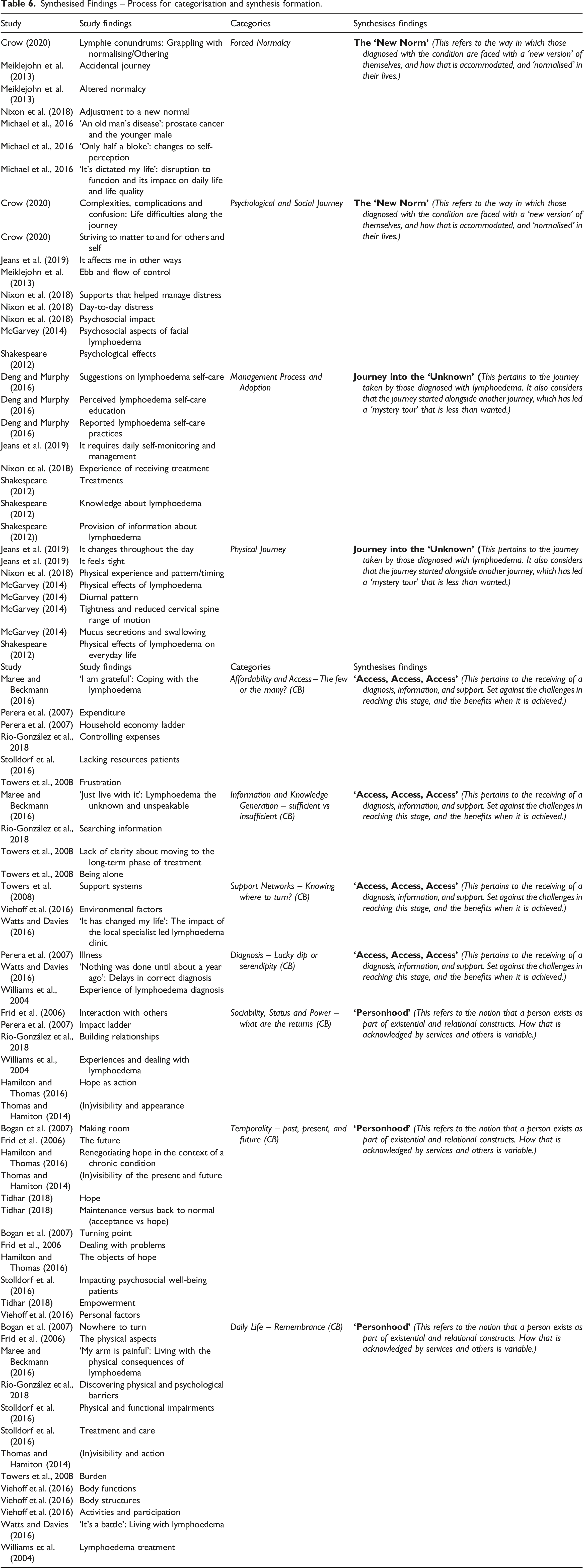
Synthesised Findings – Process for categorisation and synthesis formation.
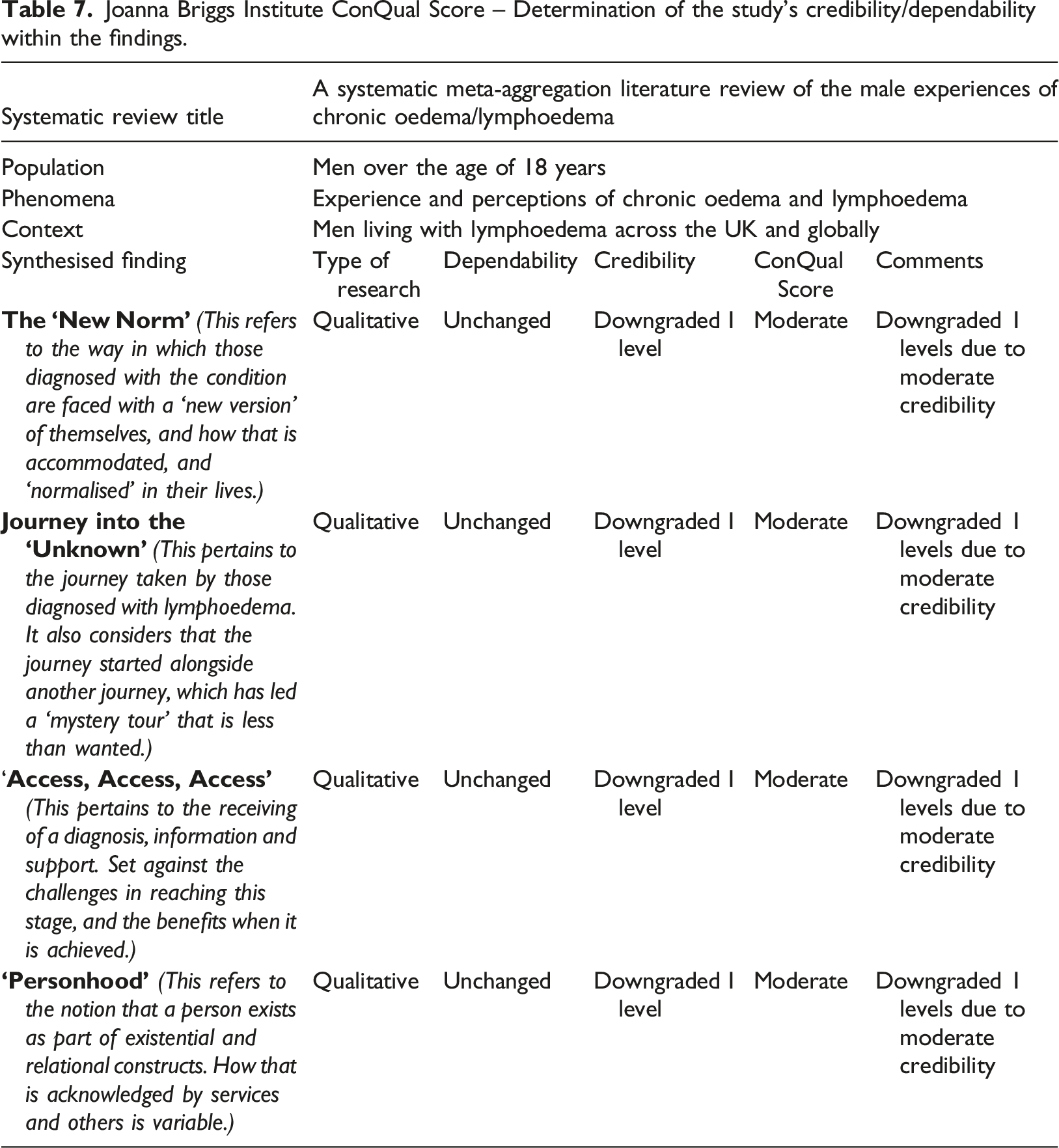
Joanna Briggs Institute ConQual Score – Determination of the study’s credibility/dependability within the findings.
Review finding results
Four synthesised findings were identified. The first two findings, (1) The ‘New Norm’ and (2) Journey into the ‘Unknown’, had a high representation of men and their accounts, which were constructed from eight studies, 32 findings and four categories. The remaining two findings, (3) Access and (4) Personhood, were constructed on 13 studies, 47 findings and seven categories. However, the sample of men and their accounts were smaller in representation or integrated into a single account:
Synthesised finding 1: The ‘New Norm’
The diagnosis of lymphoedema can have a negative impact upon men, with the need to meet other men like themselves
The baseline that men form of themselves which represent their perception of normal, alters when this is challenged by a new diagnosis especially one that is long-term. One man stated, ‘it’s dictated my life’, with another perceiving the condition as, ‘an old man’s disease’, reinforced by their contact with men, ‘You go to the support group…they are all elderly men, it felt old’ (Michael et al., 2016: 326, 325). The baseline of men was affected by their perceived vulnerability, between physical strength and its projection of manhood, ‘My legs ache,.., I don’t have the strength in my legs that I used to have.’, and its complications, ‘the most distressing part of…was cellulitis’ (Michael et al., 2016: 325; Nixon et al., 2018: 4). In the study by Crow (2020: 237) there was a perceived ‘feminisation’ of the condition by men, due to a perceived notion that body image was only a female concern, rather than being one that would affect both genders equally. This led to some men wishing to see, speak and interact with men like themselves, to lead to a ‘life calibration’, and to assist them to reconstruct their ‘new normal’ (Meiklejohn et al., 2013: 463; Nixon et al., 2018).
The psychological and social journey of men are not equal with the need for varied mechanisms to manage distress
It impacts upon the alterations to a man’s physical appearance, such as facial oedema, affected their expression of their masculinity, and led to social avoidance, such as recreational activities (McGarvey, 2014; Nixon et al., 2018). However, this was not homogenous, with some stating the effects of lymphoedema were ‘part and parcel of it’, which has been described as the ‘ebb and flow’ but can perpetuate notions of stoicism (McGarvey et al., 2014: 321; Meiklejohn et al., 2013: 463). This has also been noted as a potential transitional process similar to a grieving process with some men wishing to be ‘..re-diagnosed.’ (Meiklejohn et al., 2013: 463, Michael et al., 2016). Significant others were seen by men to play a key role within their lives, with this described as ‘supports that helped manage distress’ (Nixon et al., 2018: 21). Men also drew strength from their occupational identity, but this strength could lead men to prioritise work over their own health (Crow, 2020: 196–196; Nixon et al., 2018; Shakespeare, 2012).
Synthesised finding 2: ‘Journey into the unknown’
The physical manifestation of lymphoedema is the first challenge that men face but with limited knowledge and experience to manage it
This journey for some men occurred soon after treatment, such as cancer (Nixon et al., 2018). This led to experiences of physical discomfort and sensory changes, ‘. really tight around the bottom half of my chin’ and ‘It’s much firmer…’ (Jeans et al., 2019: 5). This rapid change did not allow time for preparation or even adaption for men, to the reduced range of movement, facial oedema, but also thick and viscous secretions, with one man stating, ‘It’s certainly affecting [me]’ (McGarvey, 2014: 320). The limited time led men to disengage from their recreational activities, due to limited knowledge and experience, of the ‘diurnal patterns’ within the presentation of their oedema (McGarvey, 2014: 320; Nixon et al., 2018). When this pattern was established, ‘..mainly there first thing in the morning…’, it led to men employing strategies to help them (Jeans et al., 2019: 5; McGarvey, 2014; Nixon et al., 2018; Shakespeare, 2012).
Self-management and the tools for educating men can be effective and empowering if tailored
The ability to undertake ‘self-monitoring’ and then implement strategies was seen as ‘empowering’ for men (Deng and Murphy, 2016; Jeans et al., 2019; Nixon et al., 2018). Expanding a man’s knowledge in this area can be received positively by men, but must equally be balanced against their specific condition, education and even their level of acceptance (Deng and Murphy, 2016; Nixon et al., 2018). This has led to words, such as being ‘fed up of it’, related to their perception of self-management and having, ‘no treatment at all, I just wear the elasticated stocking at work’, despite compression therapy representing the mainstay treatment option (Shakespeare, 2012: 136). Tailoring of education has been seen as requiring the understanding of the person’s learning style, access to peer support and even technological support in terms of self-care reminders to achieve empowerment (Deng and Murphy, 2016; Nixon et al., 2018: 20).
Synthesised finding 3: ‘Access, Access, Access’
Access to knowledgeable healthcare professionals and services can improve biopsychosocial outcomes for patients
The level of access to those with knowledge and expertise was filled with challenges from diagnosis to treatment (Perera et al., 2007). This has led to multiple referrals to receive a diagnosis, with some receiving this outcome via serendipitous events, thus increased levels of anxiety and risk of permanent physical changes (Perera et al., 2007; Watts and Davies (2016); Williams et al., 2004). Despite, reports of, ‘I went through several diagnoses’, this was compounded by the level of disinterest, but also observed lack of observed compassion, by being told, ‘just live with it’ (Maree and Beckmann, 2016: 82; Perera et al., 2007; Watts and Davies, 2016; Williams et al., 2004: 282).
Access to resources and support are affected by occupation and level of income
The type of support offered after a diagnosis was perceived as being affected by the level of household income examples (Perera et al., 2007; Río-González et al., 2018). This was linked to the ability to purchase aids for the donning or doffing of garments, or to buy shoes as a result of the oedema as examples (Perera et al., 2007; Río-González et al., 2018). In addition to the household income, the type of occupation and the tasks involved within it were seen to affect patient outcomes (Río-González et al., 2018). For example, low-income households engaged in more precarious work, that had a direct impact upon their condition, such as increased risk of trauma, or that an infection may lead to workplace disruption, such as sickness or absence (Río-González et al., 2018; Perera et al., 2007). This was associated with a level of ‘frustration’, due to the condition’s impact but also the perceived lack of financial support, such as from government to support as a result of their LTC (Stolldorf et al., 2016; Towers et al., 2008: 138).
Access to appropriate information can support a person to build their knowledge base surrounding lymphoedema
Limited access to appropriately tailored information led those affected to see information, but came across some that were not appropriate, such cancer-focused literature (Río-González et al., 2018). Shakespeare’s (2012) study connected with the notion that information needs to be understandable but also how it is related to its management (Tidhar, 2018; Towers et al., 2008). The absence of this being addressed led to feelings of loneliness, anger and disillusionment, ‘…haven’t had someone tell me, to give me a straight answer’. Whilst some suggest ‘the more I know, the more I will suffer’, acknowledges the individual concept of sufficient knowledge (Shakespeare, 2012: 139; Tidhar et al., 2018; Towers et al., 2008). Access to knowledge was also present when referring to effective support networks, such as significant others or peer support, who shared similar levels of knowledge and experiences to support their chosen strategies (Tower et al., 2004; Viehoff et al. (2016)).
Synthesised finding 4: ‘Personhood’
The diagnosis and development of lymphoedema was perceived as affecting the person’s past, present and future
The altered baseline of individuals was seen as a biopsychosocial shift, with the presence of grief alongside varying ‘turning points’ and the perception of ‘making room’ for what had occurred (Bogan et al., 2007: 219). However, within the studies this was not universal, with those that continued to ‘worry’, or were ‘waiting for a miracle to happen’, with the notion of ‘acceptance’ being a destination yet to be reached (Frid et al., 2006; Hamilton and Thomas (2016): 826; Towers et al., 2008: 41). In ‘dealing with problems’, such as the use of donning tools, patient education or support, the ability to accept led to choices focussing upon the future (Frid et al., 2006: 9). This represented ‘objects of hope’ (Hamilton and Thomas (2016): 826), but some were ‘not at that point yet’ (Bogan et al., 2007: 828; Stolldorf et al., 2016; Viehoff et al. (2016)).
Lymphoedema affects the person’s perception of power and status within their lives
‘Stigma’ was present within the study by Perera et al., (2007: 6), but also the reduced ‘social standing’ caused by the visibility and reaction to their lymphoedema. Williams et al. (2004) study commented on how the reactions and actions of those around them caused them distress. Thomas and Hamiton (2014) referred to the problem of having a condition that was ‘highly visible, while they live with a largely invisible or unknown condition’, due to the limited social awareness (Río-González et al., 2018; Thomas and Hamiton (2014): 4). The change in status and perception, altered existing relationships, such as caring duties, with others needing to be rebuilt even within themselves (Frid et al. (2006)). Especially when it affected their occupational identity, ‘The senior nurse took me off the ward and I was office based. I decided then I had had enough, and I just retired. I feel really grieved’ (Watts and Davies, 2016: 3151). This led to seeking of havens with those who held knowledge and experience to support them and to avoid feelings of loneliness (Thomas and Hamiton (2014), Williams et al., 2004).
The presence of lymphoedema acts as a constant reminder within a person’s daily life
The oedematous limb acted as a symbol, and a reminder of the changes that had occurred, but also led to a level of ‘discomfort’, beyond its physical appearance (Frid et al. (2006)). This affected the person’s constructed baseline (Viehoff et al. (2016)), in which there was a focus upon controlling the impact of the condition through strategies, until this was challenged by external forces. ‘..in the summer when it is hot, you get the feeling that your leg is swelling and you can’t move forward’ (Viehoff et al. (2016): 415). This loss of control acted as a reminder of what had come to pass, with refuge sought through hiding the condition even from themselves, ‘In winter it is a little better, I can hide it, but in summer it is very bad an emotional thing’ (Maree and Beckmann, 2016: 81). The relationship between the conditions and its presence in their daily lives was one that is contentious, and hard to resolve.
Discussion
The qualitative review provides one of the first collective insights of the daily lives of men diagnosed with lymphoedema. This resonates with the work by Monyihan et al. (2017) regarding men diagnosed with a LTC and the complexity that is added to a person’s life when faced with another LTC diagnosis. This is relevant when other international studies suggest that lymphoedema often co-exists with another LTC condition (Cosgriff, 2010; Moffatt et al., 2019b). Moniyan et al. (2017: 1988) goes on to suggest a LTC can cause a level of ‘Ambiguity in a masculine world’, in which vulnerability and weakness are associated with ill health by men and society (Moynihan et al., 2017: 1988). This feeds into the work by Leventhal et al. (2016) regarding a person’s existing prototype of themselves (baseline) and how this develops into their ‘illness representation’. This has been suggested as affecting masculinity and associated traits, such as older men and ‘stoicism’, but may also play a beneficial part in developing ‘optimism’ and even ‘self-determination’ (Moynihan et al., 2017: 1989). Masculinity is considered to have varying typology and expression, with some suggesting there are dominant versions (hegemonic) (Coles et al., 2012).
The changes to what is a perceived ‘norm’ and their masculinity is a challenging area for men, with them seeking a sense of control and empowerment to manage the LTC (Leventhal et al., 2016; Reigel et al., 2019; Zanchetta et al., 2017). This reflects other work regarding the need for appropriate access to information that is accurate and tailored (Deng and Murphy, 2016; Nixon et al., 2018). This not only takes into account how it is delivered, but also by whom, such as knowledgeable healthcare professionals, and the ability to interact with men similar to themselves (Flurey et al., 2018; Williams et al., 2004). This has the potential to change a man’s prototype of themselves (baseline), but also the strategies for the management of their condition, thus altering their ‘illness representation’ (Leventhal et al. 2016). However, this requires men to allow a level of vulnerability in seeking support, linked to their internal beliefs surrounding men and ill health (Dale et al., 2015; Robertson and Baker, 2017). This may be magnified, due to the suggested inequity of service provision to those affected by lymphoedema in the UK (Moffatt et al., 2019a).
Multiple referral and delays in the receipt of a diagnosis and treatment is a documented issue, leading to complications (Dale et al., 2015; Perera et al., 2007; Stolldorf et al., 2016). For example, persistent infections and sickness, leading to men to place ‘occupational demands’ ahead of their own health (Dale et al., 2015: 9). This was to project ‘strength’ within a workplace that considers ill health as unacceptable (Jønsson et al., 2020: 109; Zanchetta et al., 2017). This is alongside the deployment of ’push back’ as a tactic, to distance themselves from the condition, but to also create a sense of normality in their lives (Dale et al., 2015: 10). This reflects the notion of personhood in which there is ‘a moral and ethical category, tied to the concepts of autonomy, agency and self-determination’ (Sofronas et al., 2018: 407). This is caused by their perceived loss, but also the uncertainty of their role in future (Gentili et al., 2019; Persson et al., 2019). Gender-based delivery of services has been suggested as a means to remedy some of the aspects mentioned, whilst acknowledging men are one homogenous group (Robertson and Baker, 2017). Despite this approach being advocated, at the present time it has yet to be fully developed or delivered (Lönnberg et al., 2020; Robertson and Baker, 2017).
Strengths and limitations
The qualitative review is one of the first to identify, appraise and undertake a meta-aggregation in this area. This extended to the systematic review and process that was undertaken across the available databases. However, the study also has limitations by not including non-English studies caused by no access to translation services. Equally, there are several studies that did not present a clear separation between male and female accounts, thus making it challenging to ensure they fully represented men and their narratives.
Conclusion
Lymphoedema impacts widely across men within the studies retrieved. Studies with a higher representation, or had a clearer account of men, led to two synthesised themes, (1) ‘forced normalcy’ and (2) ‘journey into the unknown’, that identify the challenges men face in both accepting and managing their lymphoedema condition. Whilst still offering insight, the disruption faced by men was less apparent within the two remaining themes, due to the combination of men and women into one account, still offered insight. It equally took a different tone and focus, with the concept of having ‘access’, coupled with overall impact upon ‘personhood’. Appropriate knowledge information and access to expertise negated some of the biopsychosocial complications of lymphoedema. However, this was connected to their ‘personhood’, and the value they derive for themselves and from the wider society. The surrounding literature resonated with the findings of the review, and the way men engage within their health set against their perception of masculinity. This places a greater demand on services to consider intersectionality within the healthcare economy and requires further empirical research to be undertaken within men and lymphoedema. • The involvement of men within the design and commissioning of lymphoedema services to ensure that their needs are understood and met is crucial. • Men with lymphoedema require access to a wide range of sources of support, therefore policymakers should collaborate with these men, especially those with non-cancer related causes, and with representative organisations public, private and charitable. • Policymakers should recognise the importance of gender appropriate information resources and how these can be developed within existing services. • Policymakers should take into consideration that lymphoedema will exist alongside other Long Term Conditions.Key points for policy, practice and/or research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This was a systematic review and thus exempt from ethics approval.