
Abstract
Aim
Nursing work has historically been difficult to specify. This has led to difficulties in determining safe staffing requirements and adequately supporting safe patient care. The aim of this qualitative interview study was to explore how nurses understand their work.
Design
Qualitative interview study, using the interpretive description methodology.
Methods
Twenty registered nurses and nursing students completed semi-structured interviews about their work. The researcher drew on the interpretive description methodology to analyse interview data and create a model that interprets participants’ experiences of their nursing work.
Results
Nurses understand their work by its role in the healthcare system, rather than by the tasks or activities they complete. This understanding is significant because nurses adapt their work constantly, and rigid definitions of working would not support safe adaptation. Nurses report working across three broad roles: clinical work, which is patient-facing; managing work, which sustains the care environment; and enabling work, which provides supports like research and education that make nursing a profession.
Conclusions
Clinical, managing and enabling work have different aims, but all serve the purpose of supporting safe patient care and sustaining healthcare systems. Adaptation is a constant feature of each of these roles. This model may be useful for nurses in structuring and explaining their work and informing nursing workforce policy.
Keywords
Introduction
Nursing is an important profession that makes a crucial contribution to patient safety and high-quality healthcare. Nursing work has historically been difficult to specify, as it has numerous unrecognised aspects (Nelson and Gordon, 2006; Perry and Fairbanks, 2015). When nurses’ work has been neglected or diminished, there are negative outcomes (Afolabi et al., 2019). These include patients’ care being missed (Ausserhofer et al., 2014; Ball et al., 2014; Bittner and Gravlin, 2009; Cho et al., 2016; Recio-Saucedo et al., 2018) and medical errors (Abbasi et al., 2016; Cramer et al., 2013; Potter et al., 2005; Wears and Sutcliffe, 2015). There have also been claims that nurses are over-educated (Chapman and Martin, 2013), which devalues the skill and expertise of nurses (Gillett, 2012).
Attempts to shape nursing work have lacked understanding of how nurses contribute to healthcare, with negative consequences. For example, the recent introduction of Nursing Associate roles (Department of Health and Social Care, 2017) in the UK, ostensibly to be a compassionate, patient-facing role and reduce costs, overlooks evidence that replacing registered nurses with other providers leads to higher patient mortality (Aiken et al., 2011). Nurses may be distinguished through their caring role, but focussing on care tasks alone does not fully capture nursing work or recognise the role of healthcare environments in supporting nurses’ ability to provide care (Maben, 2008; Maben et al., 2009; Smith, 2012). A new model of nursing work is needed to fully capture the expertise of nurses. This paper reports a qualitative interview study exploring how nurses perceive their roles in modern healthcare work.
Background
It is important to re-evaluate what nurses do and how they conceptualise their work in modern healthcare, so that nurses can be better recognised, resourced and supported. A meta-narrative review (Jackson et al., 2021) was undertaken to inform this study. There were three main findings from this meta-narrative review that (a) nursing work has been studied as separate domains of labour, (b) that nursing work is not always caring for patients – it can also be in response to other types of demand and (c) nursing work is influenced by the gendered expectations of women and caregiving.
This review showed that nursing work includes cognitive, physical, emotional and organisational labour, all of which create a complex series of activities that cannot be understood using a reductionist focus on tasks. These domains of labour illustrate many aspects of nurses’ work that are not immediately visible (such as a nurse’s thoughts), and may be difficult to recognise. While this review was helpful in establishing how researchers have studied different aspects of nursing, it is unknown whether these findings reflect nurses’ understandings of their own work.
Aims
The aim of this study was to a) understand how nurses conceptualise their work and b) develop a model of nursing work to inform the modern nursing role in healthcare systems.
Methods
Design
This qualitative, interview study drew upon interpretive description (ID) (Thorne, 2008) to understand nurses’ work. Research in ID describes and interprets a phenomenon, considers the meaning of related behaviours, and formulates a valuable clinical response (Thorne, 2008). The product of an ID study is a new understanding of a complex phenomenon, with a focus on its practical implications.
Sample
Nurses were recruited to the study through Twitter, employing convenience sampling (Green and Thorogood, 2018; Richards and Morse, 2012). The inclusion criteria were that participants needed to be Registered Nurses or nursing students currently working or studying in the UK, in any clinical setting. Tweets included hashtags to reach the UK nursing community, including #WeNurses. Tweets included a link to a digital information sheet. Potential participants were invited to signal their interest by contacting the researcher via email.
Data collection
Nurses completed semi-structured qualitative interviews. During an interview, the participant was invited to meet with the researcher either in person or online by Skype. The interview began with opening questions about the participant’s work, after which they were invited to play the serious video game Resilience Challenge (Jackson et al., 2020) during the interview. Resilience Challenge presents scenarios relating to patient care, and is discussed fully elsewhere (Jackson et al., 2020). The game was used as an elicitation tool to prompt nurses to reflect on their work, with a discussion after each game scenario, and questions about the issues raised in the game. In the game, a player has to select a response to advance a patient’s journey through five scenarios. Each of the options presented in the game requires some type of compromise, based on real clinical examples. These examples created opportunities for nurses to share examples from their own work. Interviews took place in spring 2018, lasted 45–150 min, and were audio recorded. The interviews focused on how the nurses determined a course of action during their work, and how their roles supported patients across a continuum of care.
Data analysis
Data analysis was undertaken by coding transcripts to interpret participants’ experiences. Inductive coding was the hallmark of the coding process, consistent with ID (Thorne, 2008). Coding of interview transcripts began with short phrases in the text, where participants explained their roles, actions and decision-making while working. The coding gradually moved to larger portions of text, as overlapping experiences (Thorne, 2008) were identified.
Rigour
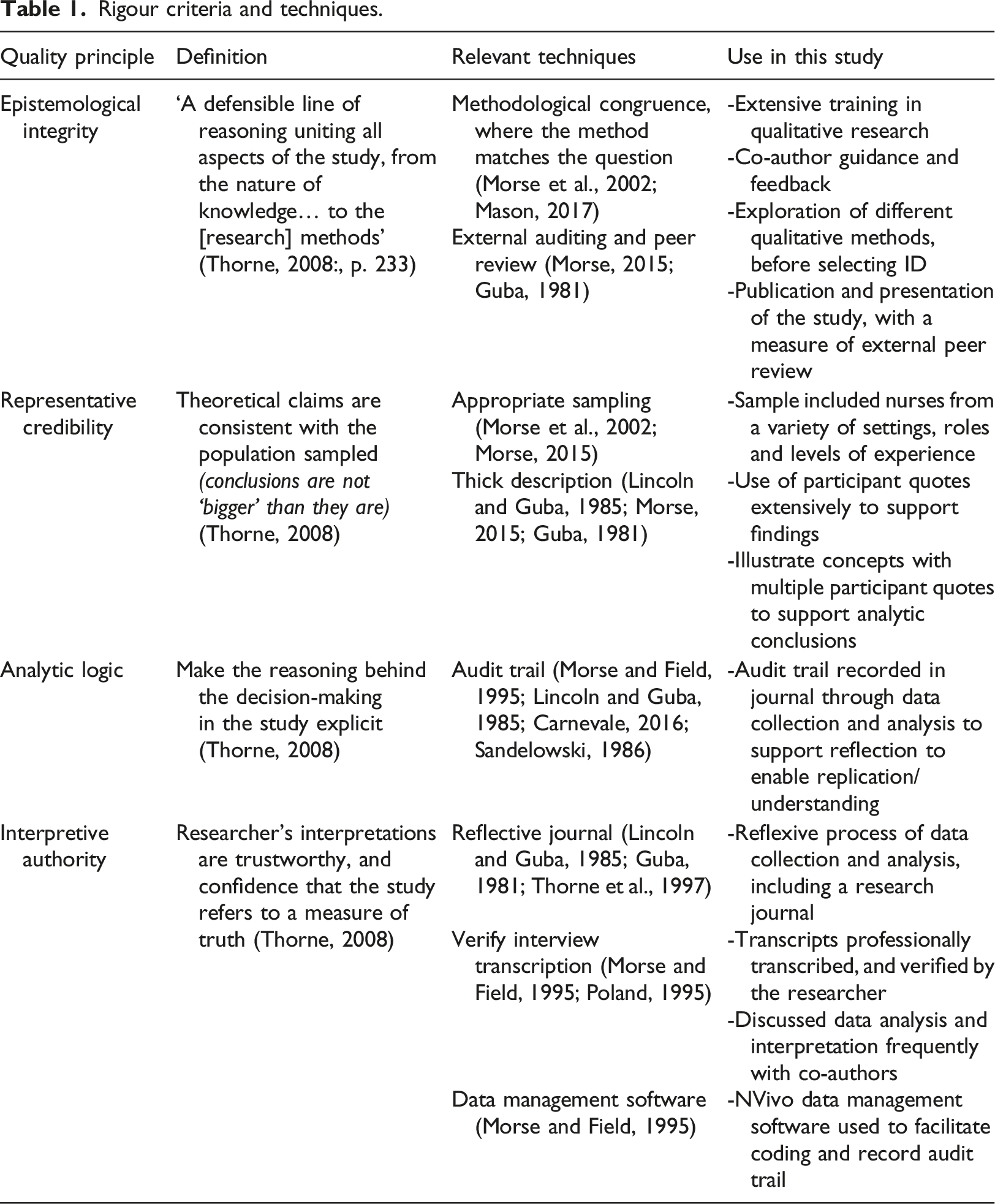
Thorne (2008) outlined a bespoke approach to rigour for interpretive description research. Thorne’s (2008) quality principles for interpretive description are presented in Table 1, with specific techniques for rigour that were used in this study.
Rigour criteria and techniques.
Ethical approval
Ethical approval for this study was obtained through the King’s College London Research Ethics Committee, protocol number RESCM-17/18-3787, on April 2, 2018. Informed consent was provided by participants, either in person by signing a consent form, or through a verbal consent via Skype. No participants withdrew from the study. The study findings explain how nurses understand their roles in healthcare, and are reported in the following section.
Findings
Demographic profile of participants
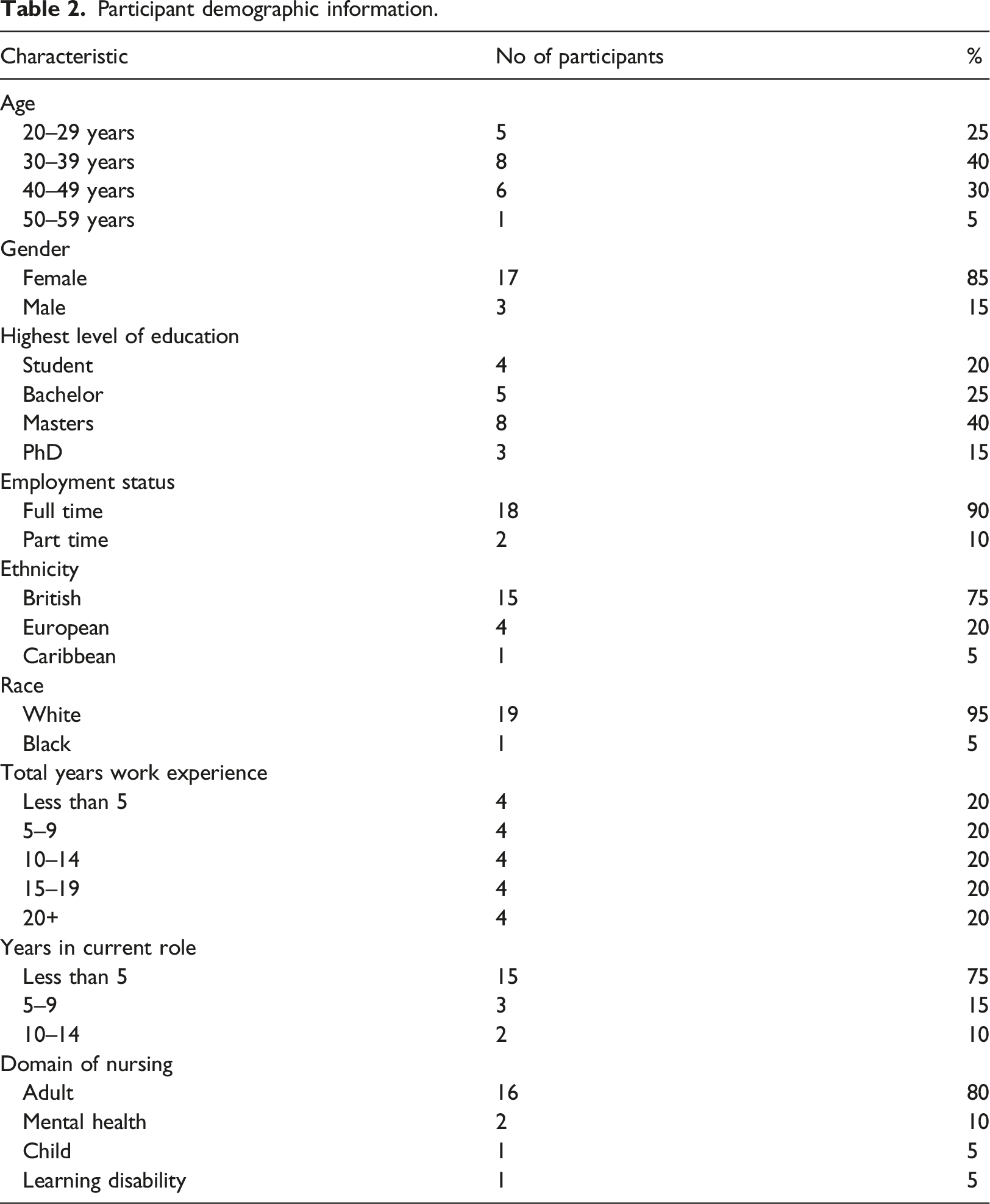
The demographic data for participants are listed in Table 2. The sample was evenly distributed across years of experience. The age range reflects an expected range for the nursing profession. There were more nurses with higher degrees, adult nurses and white nurses than expected, which may reflect the study’s recruitment using Twitter.
Participant demographic information.
Roles in nursing work
Nurses understood their roles by their broad goals and purposes, rather than by the specific nature of their activities. Nurses described their roles as a flexible framework that allowed adaptation in their work. Nurses indicated that they are required to adapt constantly, and understanding their work as a role (rather than a series of tasks) enabled them to adapt as needed. Nurses reported being at the centre of the patient, their family and the interdisciplinary team, working in service of both patients and the healthcare system (Figure 1).

Model of nursing work roles.
Participants understood their work as fulfilling roles, which were synthesised as clinical work, managing work and enabling work. Clinical work refers to work nurses undertake directly with, or in service to, patients and families. Managing work sustains the care environment, in physical spaces like a ward and broader spaces like a geographic area. Enabling work supports the nursing profession, and provides the scaffolding for the professional activities of nurses. These roles are presented separately for clarity, but are not mutually exclusive. For example, a nurse working with patients may do both clinical and managing work, but be primarily in a clinical role. Nursing role characteristics are outlined in Table 3.
Comparison of nursing work roles.

Clinical work
The first role nurses reported was clinical work, the most visible and well-known facet of nursing. Clinical work can occur in a range of settings, with a wide variety of patient populations. This participant illustrated how clinical work includes several overlapping activities, which may not be obvious to a casual observer. If you were bed bathing a patient, you’re not just actually washing that patient and looking at the skin, you’re obviously using that opportunity to have some conversation with them, depending on how they are, so that you’re actually building emotional support and assessment into the everyday tasks that you’re doing (P3. nurse educator, adult nursing).
Participants acknowledged that their work could go unnoticed or be devalued. For example, when a physician makes a decision, it needs to be communicated in order to happen (such as, changing the dose of a medication). However, a nurse does not necessarily need to report their decision-making, as they can implement changes in care directly. This participant explained how nurses’ actions were evidence-based, but this was not appreciated when a patient was waiting for an admission. The fact that we are moving the ward around and making that patient then wait for their bed space for 2 h while we deep clean two other rooms because they are a confused meningitic patient and we want to put them in a bed that is visible [to the nursing station]. The emergency department see us as just stalling. (P18. adult nursing, ward manager).
This participant explained how the actions that supported patient safety and infection control were dismissed as stalling by those who did not understand the intentions of the work.
Managing work
The second type of nursing role in this model is managing work, where nurses sustain care environments. Nurses’ managing work makes clinical work possible, for nurses and other healthcare professionals. Managing work is a unique contribution of nurses to healthcare settings, and is most visible in roles like a ward manager. Participants described managing work as a complex activity that serves patients, staff and the hospital as a whole. So, my nursing work would be keeping the department safe, making sure the staff are happy, making sure the patients are happy and making sure that we get doctors, get different specialities having to come and see the patients. (P8. adult nursing, ward manager).
This participant’s work created an environment where people doing clinical work could do so without unnecessary barriers. Nurses’ managing work supported the whole organisation, including multidisciplinary collaboration, patient flow, patient satisfaction and support for staff.
Generally, healthcare professionals such as physicians move around in a hospital, while nurses remain in a fixed location. Managing work can involve looking after a physical space like a ward, or be figurative, such as when nurses work in patients’ homes. For one participant, this work included managing resources in the community. I see my role as supporting people with learning disabilities to understand and manage their health needs and supporting other health services to understand and manage the health needs of people with learning disabilities (P16. learning disabilities nursing, clinical nurse).
This participant’s work ensured that her patients could access appropriate care from others, and navigate the healthcare system. Nurses’ managing work creates an environment that supports patients’ trajectories through the healthcare system.
Enabling work
The third type of work participants reported was enabling work, which sustains the nursing profession. Nurses who do enabling work are not directly patient-facing. Instead, they work in capacities like education, research, policy development and leadership. One nurse educator identified her work as preparing the next generation of nurses.
I don’t have a hands-on nursing role with patients, but ultimately I think the role that I do have can heavily influence the level of care that people do receive both now and in the future (P3. adult nursing, nurse educator).
This participant recognised that teaching nursing students would have far reaching implications for quality in nursing work. Enabling work has the broadest scope of nursing work, and maintains a pipeline of people to enter and evidence/information to support the profession.
Nurses reported that enabling work is often misunderstood. For example, a researcher stated that what she was doing was often seen as low priority by clinical colleagues, who privileged providing patient care over participating in research. If we want drugs approved so that millions of patients in the future can benefit from these drugs, we have to be very careful about the information that we are putting in and make sure it’s accurate. But they perceive you to be sitting at the computer doing nothing (P4. adult nursing, nurse researcher).
This participant felt enabling work was devalued by nurses who do clinical work, even though the enabling work had the potential for substantial impact. The participant reported that other nurses privileged clinical work unfairly. When I’m performing [clinical] tasks I’m seen to be a ‘real nurse’ (P15. adult nursing, nurse educator). Participants reported that enabling work was not recognised as real work by colleagues, and that visible clinical work was considered the true work of nurses. Participants were reconciled to the fact that their colleagues may dismiss enabling work as ‘not real nursing’. Participants held on to their personal knowledge of the significance of their work.
Adaptation
Within each type of work in the model, adaptation was a constant feature of nurses’ work, and it was supported by nurses understanding their work as a role, rather than a series of tasks. These adaptations occurred in any nursing role. The reason for the adaptations was to ensure patient needs were met, particularly patients experiencing vulnerability, whose needs may have existed outside existing policies or guidelines. Nurses’ adaptations also ensured that the healthcare system continued to function. I learned this very quickly in nursing is that you are navigating a very unideal world, and you do have to go with the programme fairly quickly (P1. adult nursing, clinical nurse). This participant explained that a large part of her role was to devise work arounds to ensure patient needs were met. Nurses also managed issues that ensured other professionals could continue to do their work without disruption. You hopefully are the firewall to prevent anybody else getting stressed (P8. adult nursing, nurse manager). Nurses applied their judgement and decisions to ensure patient care and hospital routines proceeded smoothly. Nurses would do whatever was required to create adaptations, without focussing on whether or not a task was outlined in their job description.
Adaptation is an important feature in nursing work, and it is made possible because of how nurses understand their roles. Participants used the framing of a role to support the safe adaptation of their work. Nurses reported that they did not focus on their stated job duties, but on fulfilling their role. This frame of reference meant that nurses could adapt their work. This participant explains how nursing work has changed in response to changing patient needs. The complexity of patients is just huge, it’s really increased even in this short space of time since I’ve started working in community. It’s a huge difference. And some of the care that we give is care that years ago I never would have thought we’d be giving, so it’s really changed unrecognisably in the last sort of five years or so (P13. adult nursing, district nurse).
This participant reported that her role was still to provide care for patients in the community, even though the scope of that care had changed dramatically. Understanding nursing work as a role meant that participants could adapt their work as needed, while retaining the mental model of their professional purpose. The finding that the frame of a nursing role supports adaptation in nursing work is novel, and is discussed in the following section.
Discussion
Debates about the work of nurses are as old as the profession (Goddard, 1953; The Standing Nursing and Midwifery Advisory Committee, 1955). At present, new models of nursing are much needed to address workforce challenges (Carryer, 2020; Clarke, 2011). The findings of this study may support a modern understanding of nurses’ work, and the importance of optimising nursing work across its continuum. In the current study, nursing work is understood as a role that supports adaptation to meet the needs of patients and the healthcare system. The model presented here may frame discussions about appreciating the value of the complex work of nurses.
There have been various other ways of modelling nurses’ work. Bottorff and Morse (1994) created a model of nurses’ work, but emphasised what nurses did, leading to a partial task focus. Other authors focused more broadly, including James (1992, p. 488), who reported her findings as ‘Care = organisation + physical labour + emotional labour’. The literature review informing this study expanded on James’ definition, characterising nursing work as cognitive, physical, organisational and emotional labour (Jackson et al., 2021). However, these models do not reflect how the participants in this study understand their own nursing work. This study illustrates nurses’ understandings as fulfilling roles, rather than completing designated activities.
The idea of nursing roles may be useful to help structure workforce policy, as nurses’ work across a variety of roles and settings may provide a unifying view of the profession. Other studies have identified nursing work as being broader than clinical work (Drevdahl and Canales, 2020). The model in this study may provide a common language for nurses in any field to explain how they contribute to care. It may also help other healthcare professionals understand the work of nurses. This study supports the finding that there is a lack of appreciation for nursing roles outside of clinical care (Drevdahl and Canales, 2020). Using language about roles across the profession may provide a more inclusive model of the nursing profession.
However, there may be a risk that understanding nursing work according to its role may lead to an overwhelming work allocation for nurses. Roles in traditionally female fields tend to have broader job descriptions than those of traditionally male fields (Ellemers, 2014). The findings of this study reflect this trend, with nursing roles being broad and encompassing many different activities, whether they are part of the nursing scope of practice or not. Other studies have found that nursing work can be characterised as doing tasks no one else will do (Bishop, 2007; Bogossian et al., 2014; Capri and Buckle, 2015; Ray, 2016), even though these tasks can be meaningful for nurses. Using roles as a framework may support nurses to advocate for appropriate staffing in each, acknowledging the importance of adequate management staffing to support patient care.
There are many aspects of nursing work that are hidden and underappreciated (Allen, 2014; Smith, 2012). This study also adds that nurses make a unique contribution to healthcare systems by sustaining the care environment. It would be useful for nurses to articulate this contribution clearly, and describe how nursing contributes to interprofessional teams. Adaptation has also received little attention from nursing authors. The findings in this study illustrate that adaptation is a central feature of nursing work, and that nursing roles are a mental framing that enable nurses to adapt their work in response to a variety of demands. Both sustaining care environments and adaptation create significant work burdens for nurses, and need to be considered as part of workload, in addition to patient acuity or census.
The implications of this study include the potential for a new conversation about how nurses understand their work, and language to highlight distinct aspects of nursing work, without diminishing other professional roles. Nurses can articulate their unique roles in healthcare systems, without devaluing the contribution of others. The findings may also be used to shift perceptions of nursing, and the idea that clinical work is the sole domain of the profession.
Limitations
The main limitation of this study is its sample, through study recruitment using Twitter. There is a lack of racial diversity and overrepresentation of graduate-educated nurses. It is possible that the use of Twitter-based convenience sampling may have produced a non-representative sample. This may be an example of ‘elite bias, a particular problem in qualitative research, because subjects who act as participants or informants in studies are frequently the most articulate, accessible, or high-status members of their groups’ (Sandelowski, 1986, p. 6). This sampling outcome contrasts with other studies, where online channels like Twitter were considered effective means of recruiting so-called hard to reach participants (Lane et al., 2015; O'Connor et al., 2014). However, there was consistency across the sample in the themes discussed and future studies could explore whether these views are shared by other groups of nurses.
Conclusion
Nurses reported their work as fulfilling a role, rather than defining their work through tasks or work settings. These roles encompass a wide variety of activities, that aim to provide clinical care, manage the context where care occurs, and enable nursing work as a profession through education and research. Adaptation is a constant feature of nurses’ work, as nurses meet complex needs in the healthcare system. Nurses need policy supports that recognise the totality of their contributions to healthcare, and careful consideration of what constitutes the full remit of nursing work.
• Nurses understand their work by its role, not by the tasks they complete • Nursing roles can be categorised as clinical work, managing work and enabling work, which all support patient care and sustain health systems • Nurses adapt their work constantly, to meet a variety of healthcare needs. This adaptation is unrecognised and unsupported. • Viewing nursing roles as a continuum can provide a cohesive view of the nursing profession.Key points for policy, practice and/or research
Footnotes
Acknowledgements
The authors would like to acknowledge the participants of this study, and Mathilde van der Merwe for her assistance in preparing this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received from the Canadian Institutes of Health Research, and King’s College London.
Ethical approval
Ethical approval for this study was obtained through the King’s College London Research Ethics Committee, protocol number RESCM-17/18-3787, on April 2, 2018.
Jennifer Jackson is a Registered Nurse and an Assistant Professor at the University of Calgary. She has had nursing experience in nephrology, intensive care, education, and management. She earned a PhD at the Florence Nightingale Faculty of Nursing, Midwifery & Palliative Care, at King's College London, supported by the Canadian Institutes of Health Research. Her research interest is supporting nurses and improving health systems, currently focusing on community based addiction services.
Jill Maben is currently Professor of Health Services Research and Nursing at the University of Surrey and Visiting Professor of Nursing at Murdoch University, Perth, Australia.
Janet E Anderson is now Professor of Human Factors in Healthcare, Monash University.