
Abstract
Background
The main barriers to ‘vulnerable migrants’ receiving good quality primary care are language and administration barriers. Little is known about the experiences of healthcare discrimination faced by migrants from different cultural groups. The aim was to explore vulnerable migrants’ perspectives on primary healthcare in a UK city.
Methods
Three focus groups and two semi-structured interviews were aided by interpreters. These were analysed against a pre-developed framework based on national standards of care for vulnerable migrants. Recruitment was facilitated via a community organisation.
Results
In total, 13 participants took part, six women and seven men. There were five Arabic speakers, four Farsi speakers and four English speakers. Themes included access to primary care, mental health, use of interpreters, post-migration stressors and cultural competency.
Conclusion
Vulnerable migrants perceived high levels of discrimination and reported the value of a respectful attitude from health professionals. Appointment booking systems and re-ordering medication are key areas where language barriers cause the most disruption to patient care. Medication-only treatment plans have limitations for mental distress for this population. Community-based therapies which manage post-migration stressors are likely to enhance recovery.
Introduction
People migrate to the UK for diverse reasons, including to seek asylum from forced displacement due to war or persecution, making migrants a very heterogeneous group (Hannigan et al., 2016). In the year to March 2018, there were 14,166 grants of asylum, alternative forms of protection and resettlement in the UK (Office for National Statistics, 2020). ‘Vulnerable migrants’ is a collective term for all asylum seekers, refugees and undocumented migrants, although there are differences between these groups in terms of the challenges they may face, for example, benefit entitlements (Refugee Council, 2020). The term ‘vulnerable’ refers to those adversely affected by circumstances leading to or resulting from migration, rather than an attribute of people themselves (The Faculty of Inclusion Health, 2018). Further definitions of these terms are in Supplemental Material.
Those seeking asylum often face adversity before, during and after arrival in the UK which can result in complex health and social needs (Centre for Health Services, 2014) and poorer health than the general population (UK Border Agency, 2010). Socio-economic needs include financial difficulties, with asylum seekers in the UK living 74% below the poverty line (Asylum Matters, 2018), combined with the stress of the asylum process itself (Almoshmosh et al., 2019). They have higher rates of pre-existing infectious disease (Clark and Mytton, 2007) and non-communicable diseases which may worsen during migration (Amara and Aljunid, 2014). One in five has mental health disorders (Mental Health Foundation, 2016), including post-traumatic stress disorder due to torture and witnessing atrocities (Almoshmosh et al., 2019).
Vulnerable migrants may use different support systems compared to the host population. This often includes the family doctor as the first and often only resource for help (Maier and Straub, 2011). Good basic primary care is fundamental and poor access can lead to poor health outcomes (Kang et al., 2019).
A brief review of the evidence surrounding best practice in UK primary care for vulnerable migrants demonstrated a high degree of agreement between studies on the barriers to receiving good quality primary care (Nellums et al., 2018), for example, lack of awareness of NHS structure (Bhatia and Wallace, 2007). Despite primary care being free for all, regardless of immigration status (NHS England, 2019), vulnerable migrants can struggle to access services which may be ill-equipped to provide appropriate care (Cheng et al., 2015). This can be due to issues within the healthcare encounter, the system and within the wider resettlement processes (Robertshaw et al., 2017). Patients may avoid using primary care for fear of arrest and of personal data being shared with the Home Office (Nellums et al., 2018).
A previous service evaluation of a local nurse-led vulnerable migrant service highlighted the need to evaluate the barriers to accessing primary care (Clark, 2018). The aim of this study was therefore to explore vulnerable migrants’ perspectives on access to primary healthcare in a UK dispersal city and by mapping these experiences to best practice guidelines to identify key areas for improvement.
Methods
The study setting was a UK city with around 150 residences for asylum seekers and approximately 50 families from the Syrian Resettlement Scheme (UK Government, 2020). The health provider was a nurse-led primary healthcare service for up to 200 asylum seekers and undocumented migrants, providing initial health assessments, immunisations and support to register with a local GP (Clark, 2018).
This study used qualitative methods. Firstly, to give a theoretical underpinning for our design and analysis, we developed a framework of best practice for provision of primary care to vulnerable migrants. These were identified by searching government websites, national bodies such as the Royal College of GPs and the Equality and Human Rights commission and multi-disciplinary bodies such as the Faculty of Inclusion Health, shown in the Supplementary Material. This framework informed the topic guide and was used to analyse our data against. The protocol was refined by consulting an ‘expert-by-experience’ patient from the migrant community and an experienced volunteer working with vulnerable migrants on the participant burden of the methodology, logistics of recruitment and topic guide suitability.
The lead author (EGC) is a GP with a specialist interest in migrant health and the second investigator (AW) is a retired health visitor. Both had skills and experience working with vulnerable migrants and interpreters. Participants met the above definition of an adult vulnerable migrant, resident in the UK for less than 5 years and spoke Farsi, Arabic and English, which are the most common languages spoken by migrants across the city (Clark, 2018). The topic guide and sample questions are appended.
Recruitment was facilitated by a community organisation, supporting recently settled migrant families to increase community cohesion, by offering free English classes and advice. Many participants had no prior concept of research, which made them cautious about consent processes and audio recording. Trusted senior staff at the organisation discussed the study with eligible participants. One week later, the two investigators attended to answer questions and provide practical information and take informed written consent. In total, 13 participants took part; five Arabic speakers, four Farsi speakers and four English speakers who were from Sudan and Kurdistan. Eleven took part in focus groups. Two semi-structured interviews were conducted with individuals who were keen to participate but felt uncomfortable in a group. There were six women and seven men across the focus groups and interviews.
Each group lasted 1–2 hours, conducted at the community organisation premises, a familiar place for participants. They were facilitated by the lead investigator and notes were taken by the second investigator. Sessions were audio recorded and transcribed. After analysis, audio recordings were destroyed. No participant identifying information was included.
The study participation leaflet and consent statement were translated into Arabic and Farsi. Face-to-face volunteer interpreters, who were health professionals with no connection to the participants and fluent in the languages, were present during focus groups. Interpreters’ experience can influence the quality of the interpretation (Larkin et al., 2007), and hence were requested to avoid misinterpretation or rewording and checked the transcripts with the audio-recordings for accuracy (Kirkpatrick and Van Teijlingen, 2009). Interpreters signed a confidentiality agreement.
Data analysis
The principles of framework analysis (Ritchie, 2014) were followed to categorise the themes against the framework of best practice that we developed at the first stage of our research. The manuscripts for each of the groups and interviews were coded for each of the six categories of best practice. Themes were developed by interrogating the data and comparing vignettes for similar and contrasting views. Then, in a more inductive way, we analysed the data for new concepts. Within each category we then grouped the themes into sub-themes.
Results
The tree diagram in Figure 1 summarises the themes and sub-themes. Our findings fall into two major themes of primary care and mental health. Within primary care, there were subthemes of access, consultations, interpretation, advocacy, costs, staff skills, knowledge and cultural competence. Within mental health, there were subthemes around symptoms, post-migration stressors and treatment. This tree diagram summarises the themes and sub-themes.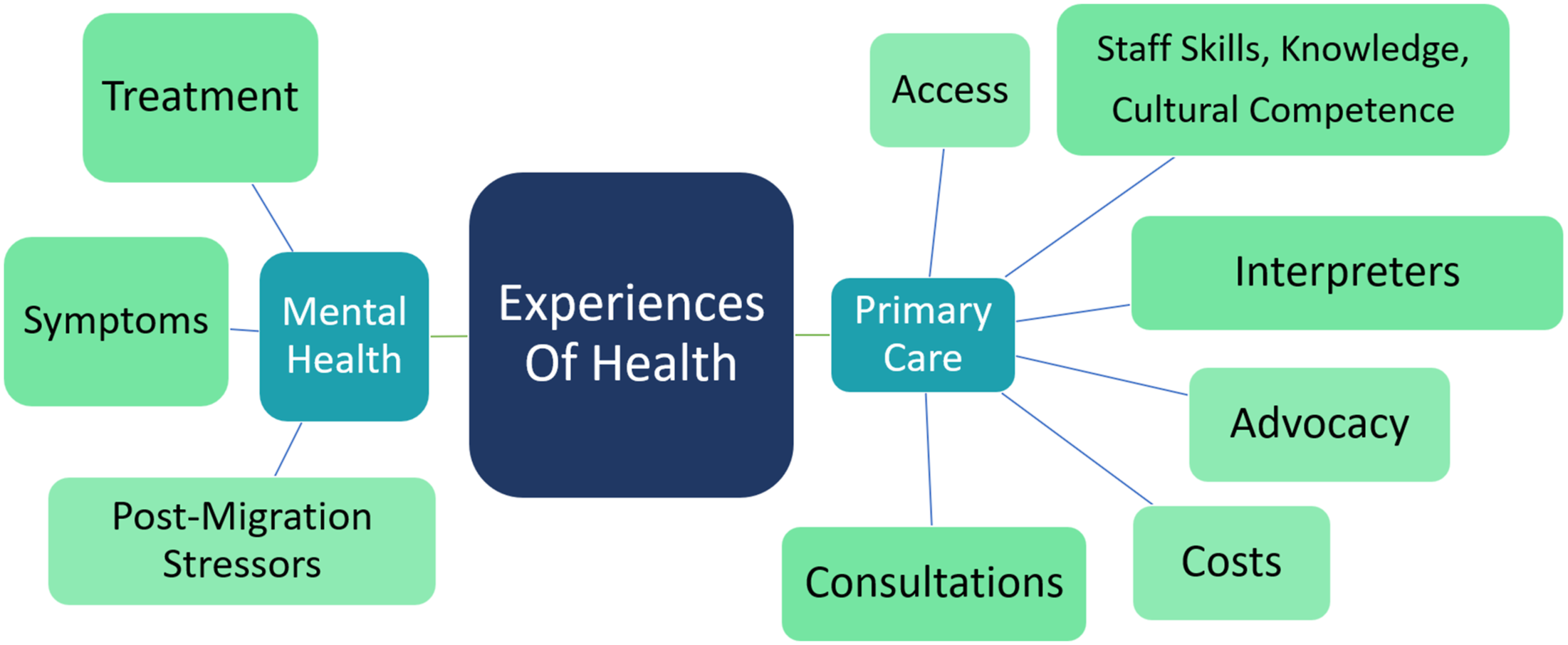
Primary care
Access
Access was hindered at several points in the patient’s care including at registration, booking registration and re-ordering medication. Most participants had not experienced difficulties registering with a GP as they had received prompt support by the nurse-led service for asylum seekers, as this Iranian lady reported. ‘A lady came to us, brought some basic hygiene things ….and took us to the doctors to register’ (p. 6). However, some were aware that registration processes could be difficult for migrants, ‘You can’t register straight away, you need some documents or form of ID and if you lack that due to the asylum process that may raise difficulty’ (p. 3).
On a system level, all groups showed insight into the challenges of the NHS ‘As we know NHS is underfunded’ (p. 3). However, on a personal level, they expressed difficulty getting timely appointments with GPs for acute problems, particularly those that required an interpreter. This lady from Iran stated ‘days ago, I had a miscarriage. Massive bleeding. I called the GP and was given an appointment for 2 weeks… We don’t have these kind of things in Iran. We get seen’ (p. 6). Difficulties were expressed around ordering medication ‘my last time to GP was about maybe 4-5months ago, they prescribed me some tablets… Promethazine firstly, then Sertraline... but I never have got them, I haven’t taken’ (p. 9).
Good practice dictates longer appointments should be given when interpreters are needed or there are mental health problems. This woman, with a history of trauma, confirmed the limitations of a 10 min appointment ‘Because my GP was very good, but every time she can see just 10 minutes… it’s no good’ (p. 10) and that warmth, patience and longer consultations were vital to enhance understanding for patients and clinicians. ‘The GP should give people a nice face… Sometimes people really don’t understand anything, and maybe say something wrong. So give time when he needs help’ (p. 12).
Consultations
Personal experiences of primary care consultations varied greatly. Participants valued the diversity of the NHS enabling an accepting attitude of staff ‘Health professionals are quite friendly and helpful. Even the health care professionals themselves are from different backgrounds’ (p. 3). Kindness and respect were also valued, ‘she (the GP) is very understandable, respectful. And then she at least looks that she believes her. And that I think this makes her to be the best doctor for her’ (p. 9). Some felt their asylum status was overshadowing their care. ‘I prefer to die than to hear about GP again. Everyone say you’re asylum seeker and waiting for paper’ (p. 9).
Interpreting
Most reported good access to telephone interpreting. However, there were some concerns over confidentiality, quality and access. Confidentiality was a concern when the interpreter came from the same community, ‘Phone is good, for me face-to-face is not. I don’t trust them’ (p. 10). One patient was unsure if the interpreter had accurately reported their words into English, and another had difficulties organising an interpreter for each appointment ‘At the GP, if I didn’t specify that I will need an interpreter [in the next appointment], they wouldn’t book an interpreter’ (p. 4). Two groups agreed that different dialects can impair the quality of interpretation. ‘Iraqi dialect is different from Algerian Arabic’ (p. 1).
Costs
Discussion was limited on this area. No participant disclosed inappropriate charging for healthcare, apart from one gentleman who was charged for a dental visit. ‘Dentists sent a bill of £80, because we ticked the wrong box …so we had to go to Red Cross’ (p. 7).
Advocacy
There was unanimous consensus of the benefit of the support of the nurse-led service, particularly in advocacy. ‘The staff are so approachable, whilst the GP surgery are not. So they [the nurse-led service] will contact the GP…and make an appointment’ (p. 4). There was consensus that the nurse-led asylum seeker service provided succinct, accessible information about the NHS. This woman from Kurdistan also had her GP advocate for her, as her partner explained ‘She provides good treatment for her… she provides some letters in regard to her mental health issue’ (p. 9).
Staff skills, knowledge and cultural competence
There was great contrast between the different ethnic groups. Overall, Sudanese, Syrian and Iraqi individuals were satisfied with the NHS, perhaps due to the contrast with health system in their countries of origin, as this Sudanese gentleman states ‘(laughs) we have never seen before healthcare in my country. So it’s different… There are no GPs. Where I was living in the countryside – mountains, jungle…farmers’ (p. 12).
The Iranians all felt the NHS was worse than the private system in Iran, where the patient dictates treatment. ‘In Iran, you have a problem, you go to the doctor and they sort it, there is no messing about’(p. 5). Language barriers may have fuelled this disappointment and these patients disengaged with the NHS, seeking treatment by having medication sent from abroad.
Participants felt that professionals did not have in-depth knowledge of the asylum process or individual cultures, but this did not negatively impact on care if they felt respected. This Muslim woman describes a male doctor attempting to shake her hand. ‘I don’t think [they disrespect our culture]. Because they don’t know my culture, this is not intentional’ (p. 2).
Mental health
A dominant feature of all focus groups’ discussion was around mental health, including symptoms and treatment.
Post-migration stressors
When migrants arrive in resettlement countries, the new challenges they face were well described. For example, some felt discrimination from local population ‘I saw a lot of people in the street… some people look at you like you are a stranger….it is not nice’ (p. 12) and some felt rejection from their own community ‘Just English people and Christian help me. Muslim people tell you ‘you are no good, you need scarf’ (p. 10).
Boredom and isolation were described ‘One gets bored… hide yourself, hate the life… if you come from where people live in community, and you come to lock your door, four walls all day…’ (p. 11). In contrast, a protective factor for this woman was her family ‘I didn’t experience isolation because I had my children’ (p. 4).
Asylum seekers are unable to work and have limited access to financial support, as this gentleman describes ‘The problem is you don’t have enough money… just have £37 a week….I used to be a construction man for many years. And it’s my job satisfaction. So I would really like to be involved with construction… it makes me forget about the past’ (p. 9).
The asylum process can take years and involve multiple claims, which can cause distress and may ease once the process concludes ‘Later, Alhamdulillah (thanks be to god), the crisis passed when I got the refugee status, my situation got better and my family joined me’ (p. 1). However, once leave to remain is granted, asylum seekers have 28 days to arrange new accommodation, claim benefits and find employment. This can be a time of great vulnerability, as this gentleman describes. ‘Once you get recommendation for legal paper, you are not able to live in the house, you must register with job centre… I was homeless and stayed in YMCA’ (p.12).
Symptoms
Mental distress was expressed in different ways by participants. This lady suffered poor sleep and appetite, both physical symptoms of depression. ‘I’m not sleep well, and every night I have bad dream… I have a problem for eat. Never no hungry’(p. 10). She also had recurrent unexplained abdominal pain, which was eventually concluded to be somatisation of her mental distress. Other patients experienced conflicting emotions ‘…you need to be with others to overcome the loneliness, but at the same time… you want to be alone’ (p. 1). Withdrawal may be a maladaptive coping mechanism. Others felt a loss of control and despair ‘I was twice suicidal, not just attempt I really did that. It’s a miracle I’m still alive. When I think about that I’m a mess and I might lose my control’ (p. 9).
Treatment
There was a consensus that medication for distress was only one approach to mental health and had limitations, ‘I told him [the GP] that I am not feeling well mentally. He gave me tablets… they made me .crazy’ (p. 1). Other approaches which could be explored were psychological therapy ‘I’m looking for an alternative way to make me forget about the past.. for some people who are really experienced, to teach us how to do this’ (p. 9). Again, some felt the mental health treatment offered was being overshadowed by their asylum status ‘I am asking them to help me… they keep remind us that you are asylum seeker and need paper to provide proof to home office… that makes me really disappointed’ (p. 9) which would perhaps suggest an element of inequitable healthcare based on immigration status.
Participants were unanimously positive about the role of community organisations in reducing post-migration stressors by providing a sense of community and meaningful activities ‘Support regarding asylum, socialising, networking, getting a career …mentorship programmes’ (p. 3).
Discussion
Many migrants face language barriers, exacerbated by the systems in place, such as telephone or internet booking for appointments (Nellums et al., 2018). This can lead to frustration, misunderstandings and ultimately poor engagement (Poduval et al., 2015) as demonstrated particularly in the Iranian group in our study. Our study revealed that patients may prefer telephone interpreters rather than face-to-face if they come from the same small community.
Migrants face discrimination due to their immigration status in host countries (Nellums et al., 2018), and previous studies called for closer examination of whether this occurs in healthcare (Kang et al., 2019). Evidence was found in our study, particularly regarding mental health, where immigration status was perceived by patients to be overshadowing care received. Providers often lack knowledge about migrants' rights and entitlements (Poduval et al., 2015), fuelling discrimination. Online resources are a good source of basic information to support healthcare staff caring for this group (Doctors of the World, 2020).
Mental health issues and distress dominated our findings, demonstrating the challenges migrants can face in addition to physical health issues (Almoshmosh et al., 2019). It clearly demonstrated that a lack of meaningful activities and a sense of community can be particularly distressing. This is particularly notable in Syrian women in this study, where social networks provide coping mechanisms (Almoshmosh et al., 2019).
Advocacy from charities and healthcare staff improves access (O’Donnell et al., 2007) and helps migrants build ‘social mastery’ by rebuilding relationships and community to restore wellbeing (Van de Kolk, 2015). This study demonstrated the vital advocacy role of health professionals in negotiating the health system, which should be recognised in training of staff (Robertshaw et al., 2017). Liaison with community organisations can support patients to tackle these post-migration stressors to reduce mental distress. Other studies have shown an overreliance on the charitable sector (Nellums et al., 2018) to do this, but this study showed that these stressors were not being tackled locally by mental health services so individuals were forced to access such support from the charitable sector.
Previous studies have shown that 10 minute GP appointments are too short, particularly when dealing with trauma (Kang et al., 2019), which is prevalent in this group. Our study demonstrates that this group needs longer appointments to achieve shared understanding when dealing with somatisation and health beliefs. Approximately a quarter of vulnerable migrants who access primary care use somatisation to express distress (Aragona et al., 2012), and this phenomenon was described by some of our participants with unexplained physical symptoms. Previous studies have shown that responsiveness to health beliefs and cultures increases engagement of minority populations with healthcare (Szczepura, 2005). Cheng et al. (2015) called for studies of this group to focus on specific ethnic groups to elucidate cultural differences. In our study, experience and usage of primary care varied depending on country of origin, with those from resource poor settings such as Sudan having greater satisfaction compared to those from more resourced health systems such as Iran.
Mental distress does not necessarily indicate mental illness so less clinical approaches may be beneficial, particularly as there is stigma associated with psychiatric medication in some migrant groups (Almoshmosh et al., 2019). Our study demonstrates that negotiating medication use with migrants requires careful explanation of side effects and modes of action.
Several strengths of our study included partnering with a community organisation to engender trust, making a concerted effort to ensure accurate translation and using interpreters specifically from the same culture as participants (Alzubaidi et al., 2015). Single ethnicity groups (i.e. Iranian) provided more free flowing conversation and consensus. Inclusion of non-English speakers led to challenges at every stage, from recruitment through to analysis, but the authors negotiated these challenges to ensure their views were included. The small sample size limits generalisability with men and women combined into groups, altering group dynamics. Barriers to access are more pronounced in migrant women (Nellums et al., 2018) and future research could explore their experiences specifically.
There may have been bias towards more empowered participants as those facing the greatest vulnerabilities were perhaps not engaged with the community organisation or unable to fully verbalise their experiences.
Conclusions
This study gives insight into particular aspects of primary care that language barriers impact on, mainly accessing emergency appointments, use of telephone systems and re-ordering medication. The authors have recommended that an important first step is for surgeries to sign up to the ‘Safe surgery’ campaign, where practices commit to tackle the barriers faced by many migrants accessing healthcare (Doctors of the World, 2020). This study supports the role of specialist nurses for vulnerable migrants within primary care, for example in advocating for patients and providing clear and succinct information on the NHS. Working with local pharmacies on medication compliance would be an opportunity to improve care of chronic conditions.
Professional interpreters facilitate shared understanding in the consultation (Faculty of Inclusion Health, 2018). Interpreters should have the same language, dialect and origin of country as the patient (Hadziabdic and Hjelm, 2014). It is recommended that health professionals should reassure patients on interpreter confidentiality, offer the choice of telephone or face-to-face interpreters and flag interpretation needs on the medical record. Longer appointments are essential to complex needs, often involving prior trauma and the extra time that interpretation takes (NHS England, 2018).
Discrimination can stem from a place of fear and misunderstanding. It is vital to train all health professionals on cultural awareness and humility, to ensure health workers remain cognisant of biases that may impact on their ability to fulfil their fundamental duties to provide good quality care for all, regardless of culture or immigration status (Robertshaw et al., 2017). Providing clear and accessible information to this group in a way that improves patient’s understanding of their rights to access health services can dispel fear of discrimination (Nellums et al., 2018).
Our study shows that medication-only treatment plans have limitations for patients with mental distress. We suggest that community-based, culturally appropriate interventions could be utilised to tackle post-migration stressors and rebuild their lives using the resilience, strength and skills acquired on their journeys (Faculty of Inclusion Health, 2018; Refugee Council, 2021). Health professionals have signposting and advocacy roles and should liaise with community organisations (Faculty of Inclusion Health, 2018). Where medication is indicated, health beliefs and stigma should be directly tackled (Szczepura, 2005).
Accessing emergency appointments, use of telephone systems and re-ordering medication are the key areas where language barriers cause the most disruption to patient care. Specialist nurses for vulnerable migrants within primary care have an important role to play in supporting access to the NHS. Vulnerable migrants may perceive that immigration status impacts on primary healthcare offered; is it therefore vital to train health professionals on cultural competence, including guidance on advocacy and sign-posting. Medication-only treatment plans have limited benefit for mental distress for this population. Community-based therapies which include dealing with post-migration stressors are likely to enhance care. Vulnerable migrants are hard to recruit into research studies, with many of the same barriers faced in accessing services. Future primary care research must make concerted efforts where possible to include non-English speakers, engender their trust and make appropriate arrangements to ensure their views are heard.Key points for policy, practice and/or research
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871211043754 – Supplemental Material for Scarred survivors: Gate keepers and gate openers to healthcare for migrants in vulnerable circumstances
Supplemental Material, sj-pdf-1-jrn-10.1177_17449871211043754 for Scarred survivors: Gate keepers and gate openers to healthcare for migrants in vulnerable circumstances by Emily Clark, Nicholas Steel, Tara Berger Gillam, Monica Sharman, Anne Webb, Ana-Maria Bucataru and Sarah Hanson in Journal of Research in Nursing
Supplemental Material
sj-pdf-2-jrn-10.1177_17449871211043754 – Supplemental Material for Scarred survivors: gate keepers and gate openers to healthcare for migrants in vulnerable circumstances
Supplemental Material, sj-pdf-2-jrn-10.1177_17449871211043754 for Scarred survivors: gate keepers and gate openers to healthcare for migrants in vulnerable circumstances by Emily Clark, Nicholas Steel, Tara Berger Gillam, Monica Sharman, Anne Webb, Ana-Maria Bucataru and Sarah Hanson in Journal of Research in Nursing
Footnotes
Acknowledgements
Norwich Integration partnership. Adam Wagner, Research Fellow (support with methodology). Mike Clemo, volunteer at vulnerable migrant service (support with facilitation and recruitment). Hesam Safari, expert patient (support with reviewing methodology). Yasir Hameed, consultant psychiatrist (interpreter – Arabic). Keivan Maleki, GP (interpreter – Farsi). Research participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is a summary of research funded by the National Institute for Health Research (NIHR) Applied Research Collaboration East of England (ARC EoE) Programme. The views expressed are those of the author(s), and not necessarily those of the NHS, NIHR or Department of Health and Social Care.
Ethics
Ethical approval was granted from the University of East Anglia Faculty of Medicine and Health Sciences Research Ethics Committee reference 201819 – 137 on 16.7.19, with the amendment of including semi-structured interviews approved on 24.10.19.
ORCID IDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.