
Abstract
Background
Nurses need to exhibit stronger leadership by taking more responsibility and accountability to improve healthcare quality and patient safety.
Aims
The aim of this study was to determine the association between quality of care and leadership styles and practices, and whether the characteristics of nurses influence this interaction.
Methods
We conducted a multicentre cross-sectional survey of 655 nurses working on clinical wards in Dutch university medical centres in 2018.
Results
Transformational leadership was significantly associated with quality of care which explained 5.9% of the total variance (R2 = 0.059 F = (11,643) = 3.726, p = 0.011), and the nurse characteristics gender, profession and type of practice area were significant influencing factors. Nurses rated the quality of care (mean (M) = 7.7, standard deviation (SD) = 1.3) as moderate and they showed moderate levels of transformational leadership style (M = 3.7, SD = 0.5) and transformational leadership practices (M ≥ 6.2 and ≤ 7.6).
Conclusions
When considering quality improvement on clinical wards strategic managers need to be aware of the fact that leadership is associated with quality of care and that nurse characteristics influence this association. The findings indicate a pressing need for education and training for nurses in how to develop leadership and raising the awareness among strategic managers about the importance of leadership in health care is recommended.
Introduction
Although nurses make up 59% of the global health workforce, global reports claim that they are not visible in strategic planning or decision making of healthcare, and nurses’ lack of leadership was identified as an important challenge for health care (Sigma Theta Tau International, 2018; Klopper et al., 2020; IOM, 2011). Strengthening leadership of nurses, both as current and future leaders, to ensure that nurses have an influential role in health policy formulation and decision-making, and to contribute to the effectiveness of health and social care systems was called upon by the first State of the World’s Nursing Report recently published by the World Health Organization (WHO, 2020).
Despite the many definitions of leadership, the definition most often used in nursing is from Northouse (2013), who described leadership as a process whereby an individual influences a group of individuals to achieve a common goal. This definition explains leadership as a practice accounting for everyone, independent of professional position or social status. Among the different leadership styles and practices, the leadership style most used in nursing is transformational leadership (TL): a relational leadership style in which professionals have trust and respect for the leader and are motivated to do more than is formally expected of them to achieve organisational goals (Afsar and Umrani, 2020). Bass (1990) described a transformational leader as someone who builds trust, acts with integrity, encourages others, encourages innovative thinking and coaches and develops people. Based on years of research, Kouzes and Posner (2016) identified five important TL practices of exemplary leaders which include: (a) challenge the process by being open to innovation and change; (b) inspire a shared vision by formulating a certain vision or goal, and make colleagues enthusiastic about it; (c) enable others to act by creating a safe, trusted environment in which everyone can work well together; (d) model the way by being an example for colleagues; and (e) encourage the heart by acknowledging and recognizing everyone's contribution. Other leadership styles are transactional leadership (TAL) that occurs when a leader monitors deviations and mistakes and rewards achievements (Bass, 1990) and laissez-faire leadership (LFL) that occurs when a leader is passively avoidant of issues and provides follower feedback only when problems need to be corrected (Bass, 1990).
What type of leadership styles and practices are needed to address the challenges faced by nursing must be informed by current empirical findings of the impact of nursing leadership on patient, nursing and healthcare outcomes. There is well-documented evidence for leadership impacting nursing outcomes and various patient outcomes (Cummings et al., 2018; Wong et al., 2013). Findings showed relational leadership styles of managers are positively associated with nursing workforce outcomes and related organisational outcomes, whereas task-related leadership of managers is negatively associated with nursing outcomes (Cummings et al., 2018). Findings also showed relational leadership styles of managers are positively associated with patient satisfaction, patient safety outcomes and lower patient mortality (Wong et al., 2013). TL of managers was found to be positively associated with patient safety culture, patient safety outcomes, continuous quality improvement initiatives and improved quality processes (McFadden et al., 2009, 2015).
Nurse-reported quality of care (NRQC) is a well-known measure, which focuses on the quality of care (QoC) as perceived by nurses (Aiken et al., 2002). Nurse perceptions develop over time through a series of interactions and direct observations and are not based on short-term observations (McHugh et al., 2012). Therefore, these perceptions and NRQC is considered to be a reliable and valid way of measuring QoC (Aiken et al., 2017; Stalpers et al., 2016).
Despite the importance of leadership in healthcare, there is a lack of studies investigating the association between the leadership of nurses working on clinical wards and QoC. Studies have shown that nurse characteristics, such as years of nursing experience and nurse education, influence QoC (Blegen et al., 2013; Stalpers et al., 2016). Other characteristics, such as age, years of nursing experience and nurse education, also influence leadership (Doran et al., 2004; Raup, 2008). Although nurse characteristics may influence the association between leadership and QoC (Fitzpatrick, 2017), which characteristics these may be is still not known.
The aim of this study was to determine the association between QoC and leadership styles and practices and whether the characteristics of nurses working in Dutch university medical centres (UMCs) influence this interaction.
Method
Sample and data collection
A cross-sectional survey was conducted among nurses working on clinical wards in Dutch UMCs between February and May 2018. The population included 7250 nurses working on clinical wards, on inpatient or outpatient wards, of five Dutch UMCs, and nurses who were contracted in these wards were included in the study. The sample size was calculated for the outcome of QoC. Initially, we assumed a response distribution of 50%. The eligible population size was 7250. To obtain a 5% margin of error and a confidence level of 99%, a sample size of 608 nurses was needed (Raosoft, 2004).
Nursing councils and the board of directors approved participation in the study. The Medical experts at a certified translation agency translated the questionnaires into Dutch using the back-and-forward method. The online survey was tested by a group of experts of all the UMCs. A total of 3470 nurses were approached for participation. The potential participants received an email informing them of the study purpose and inviting them to participate anonymously. The invitation included a link to the online survey. As customary, informed consent was inferred when participants completed and returned the survey. Completing the survey required a maximum of 30 minutes. All the nurses received an email reminder after two or three weeks, and the survey was closed after 10 weeks. Participants could only return the survey after completing all the questions, which prevented the occurrence of missing data.
Measures
Nurse characteristics
The following data were collected: nurse’s age, gender, highest nursing degree, profession, weekly working hours, years of nursing experience and type of practice area. Practice areas were grouped into 10 categories based on specialisation and further divided into three groups for the analyses: (a) acute and intensive care includes traumatology, operating room, intensive care, high care and medium care, cardiac care unit, thorax, gynaecology and obstetrics; (b) clinical care includes all surgery wards, rheumatology, rehabilitation, neurology, long, internal medicine, oncology wards, paediatrics; (c) outpatient clinics and mental care includes all outpatient clinical care and all psychiatric care.
Leadership
Leadership styles were measured using the validated and reliable Multifactor Leadership Questionnaire (MLQ), version MLQ-6S (Bagheri et al., 2015), which is a short self-assessment (SA) that measures different components of TL, TAL and LFL. This 21-item questionnaire is a 5-point Likert-scale (from 1 = ‘not at all’ to 5 = ‘frequently, if not always’). The MLQ includes seven subscales: idealized influence, inspirational motivation, intellectual stimulation, individualized consideration, contingent reward, management by exception and laissez-faire. Management by exception is a subscale that is part of TAL as well as LFL and is thereby used twice in the outcome of the questionnaire (Bass, 1990). The level of leadership was considered ‘low’ when the score was between 1 and 3, ‘moderate’ when the score was between 3 and 4, and high when the score was between 4 and 5. Cronbach’s α was 0.86 for this study.
TL practices were measured using the validated and reliable Leadership Practice Inventory (LPI), which is a 360° instrument that includes SA and observer-assessment (OA). The LPI is commonly used in research to measure leadership of managers or other professionals (Cummings et al. 2018). In this study we measured personal TL practices with the LPI SA as years of research has showed that the LPI SA is sufficient to measure personal leadership of professionals (Kouzes and Posner, 2016). The LPI includes 30 items, categorised into the five practices: challenge the process; inspire a shared vision; enable others to act; model the way and encourage the heart. Each practice includes six items scored on a 10-point Likert scale (from 1 = ‘almost never’ to 10 = ‘almost always’). The level of TL practice was considered ‘low’ when the score was between 1 and 6, ‘moderate’ when the score was between 6 and 8, and ‘high’ when the score was between 8 and 10. Cronbach’s α was 0.94 for this study.
QoC
We used the four-item NRQC questionnaire developed by Aiken et al. (2002) to measure QoC. The first two items refer to the QoC on their ward and each item is scored on a 4-point Likert scale (from 1 = ‘poor quality’ to 4 = ‘excellent quality’). The third item refers to the improvement of QoC in the hospital over the past year, and each item is scored on a 3-point Likert scale (from 1 = ‘deteriorated’ to 3 = ‘improved’). The total score of NRQC is calculated as the sum of the first three items, ranging from 3 to 11. The level of NRQC was considered ‘low’ when the score was between 3 and 6.9, ‘moderate’ when the score was between 7 and 9.9, and ‘high’ when the score was between 10 and 11. The fourth item is an extra item referring to the confidence nurses feel about the ability of their patients to manage after hospital discharge, and each item is scored on a 4-point Likert scale (from 1 = ‘very confident’ to 4 = ‘not at all confident’). Cronbach’s α for the three items in this study was 0.61. However, this value was reduced due to the short length of the questionnaire and therefore, the reliability was acceptable (Tavakol and Dennick, 2011).
Statistical analysis
The data were analysed using IBM SPSS Statistics, version 24 (Armonk, New York, USA). Descriptive statistics were calculated for all the parameters. Univariate linear regression was used to determine the association between QoC as dependent variable and independent variables leadership styles and practices and influencing nurse characteristics. Preliminary analyses were conducted to ensure no violation of the assumptions. Each independent variable of the univariate association with a p-value < 0.20 was included in hierarchical multiple regression analyses to determine the association and influencing nursing characteristics (Pallant, 2010).
Results
Nurse characteristics
Nurse characteristics (n = 655).
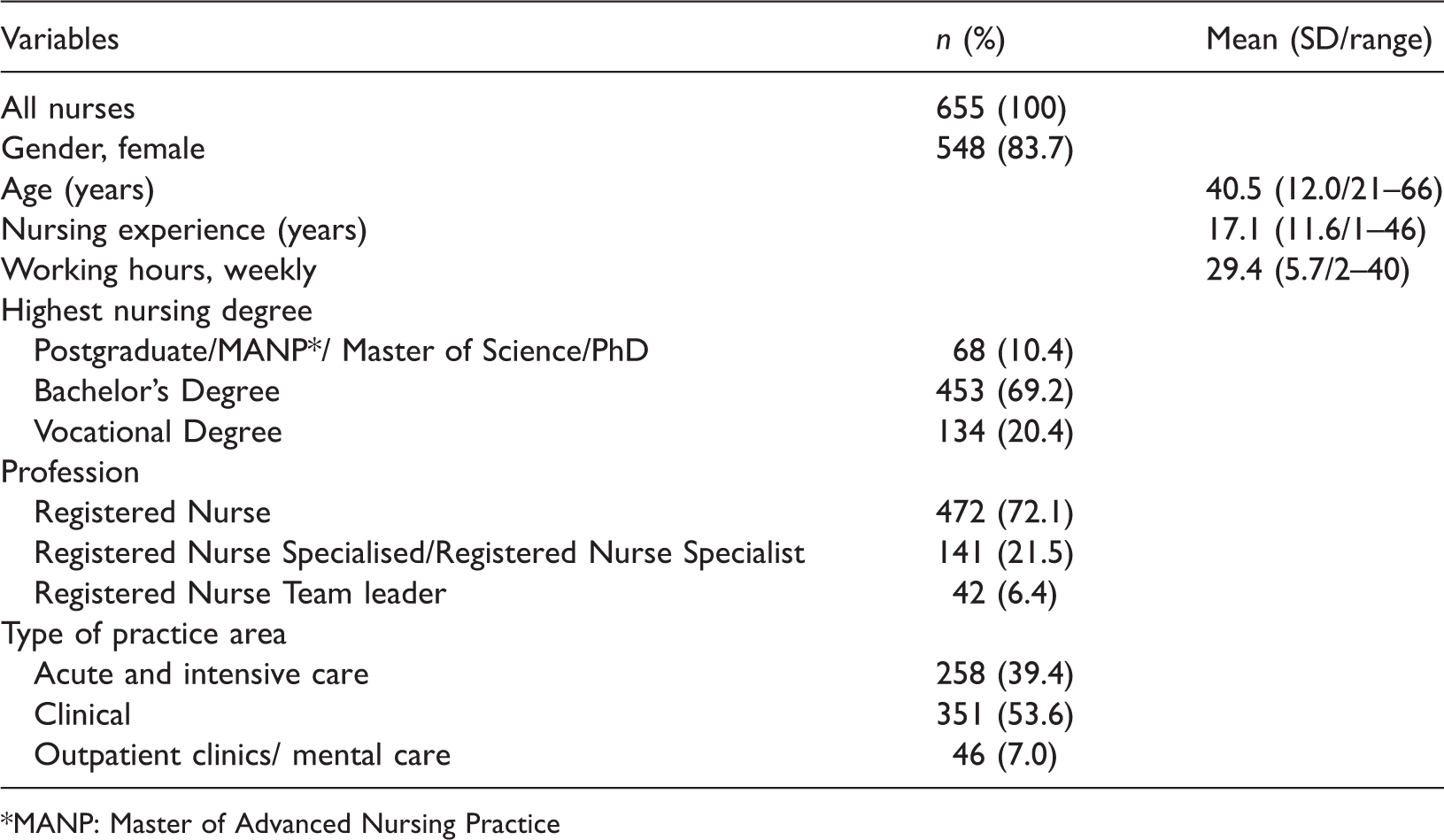
*MANP: Master of Advanced Nursing Practice
Leadership
Leadership styles and practices.
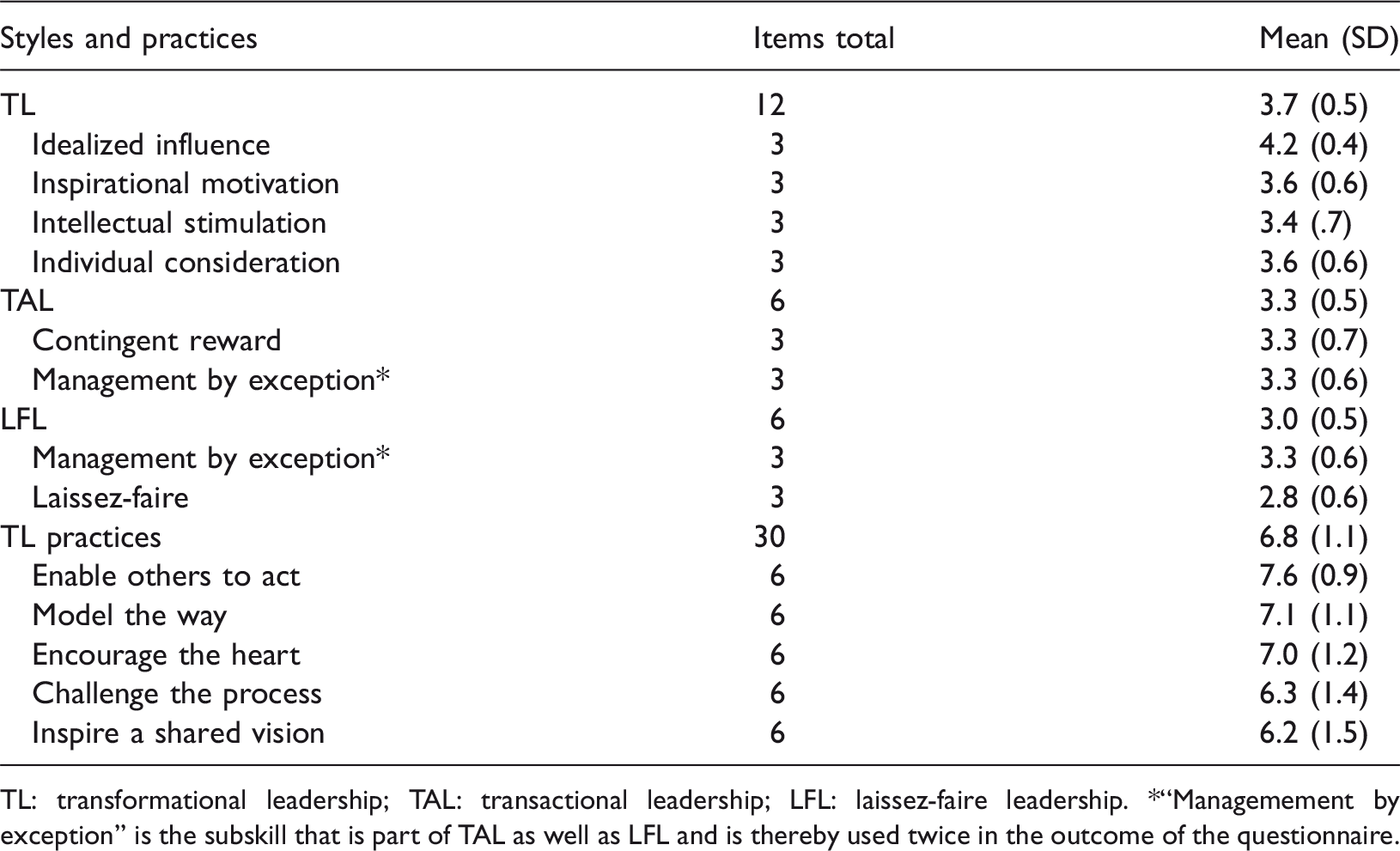
TL: transformational leadership; TAL: transactional leadership; LFL: laissez-faire leadership. *“Managemement by exception” is the subskill that is part of TAL as well as LFL and is thereby used twice in the outcome of the questionnaire.
QoC
Nurse-reported quality of care (NRQC).
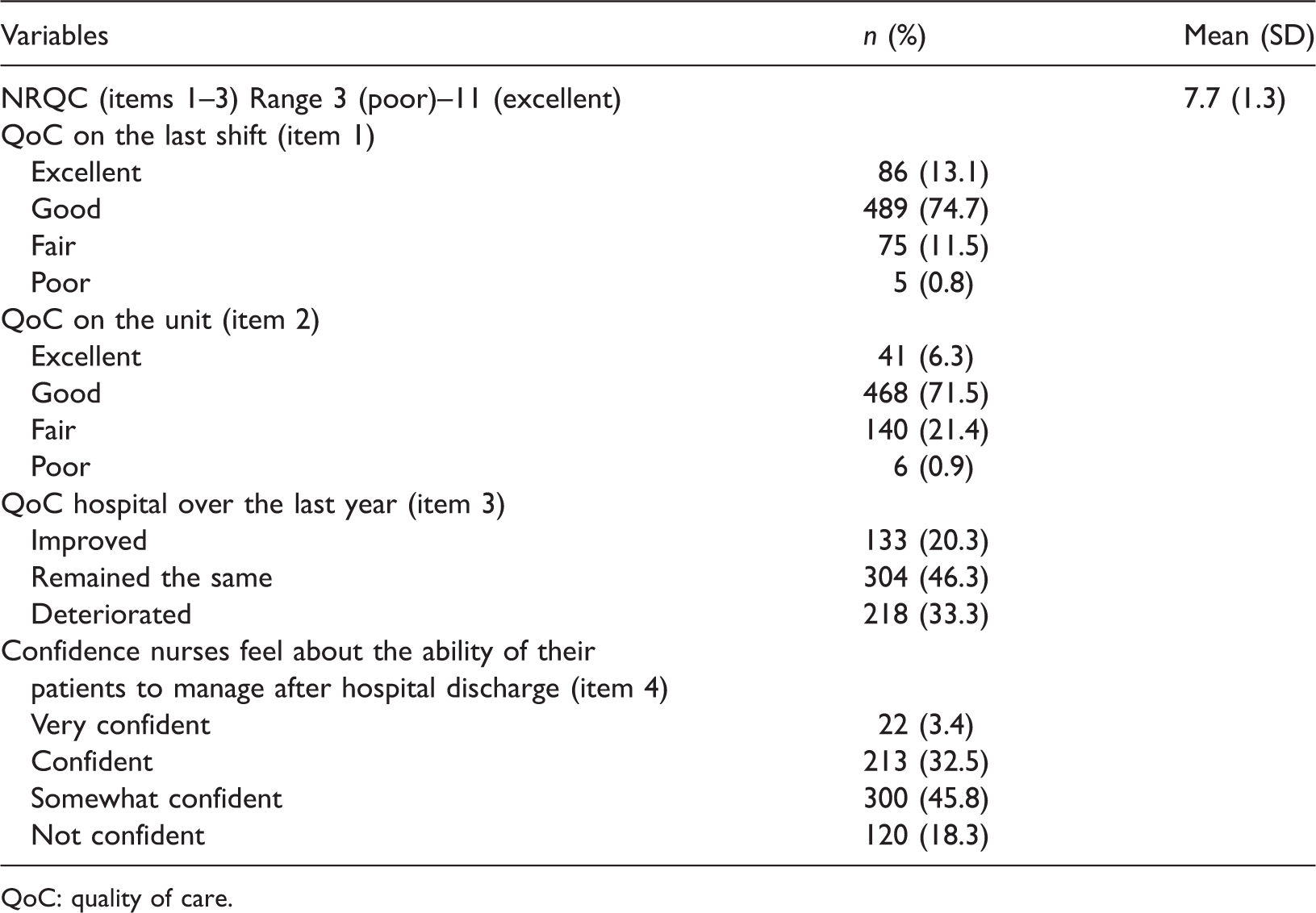
QoC: quality of care.
Association between leadership and QoC
Leadership styles and practices and influencing nurse characteristics associated nurse-reported quality of care.
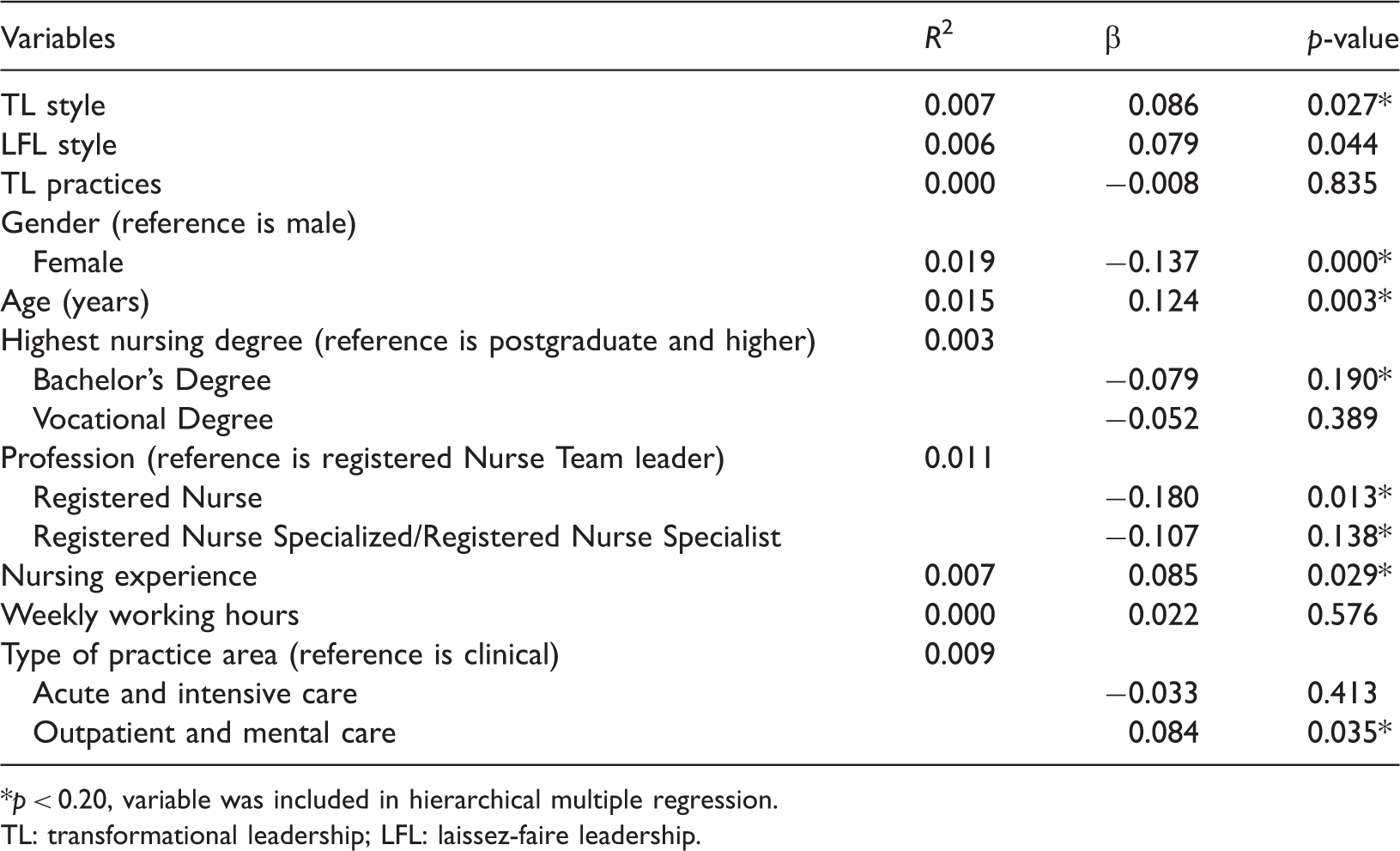
p < 0.20, variable was included in hierarchical multiple regression.
TL: transformational leadership; LFL: laissez-faire leadership.
Influencing nurse characteristics
Univariate linear regression analyses were carried out to predict the QoC based on separate associations with nurse characteristics. The independent variable age was excluded because of its multicollinearity with nursing experience. Independent variables with a p-value < 0.20 were gender, nursing experience, nursing degree, profession and type of practice area (Table 4).
Nurse characteristics influencing the association between leadership styles and practices and quality of care.
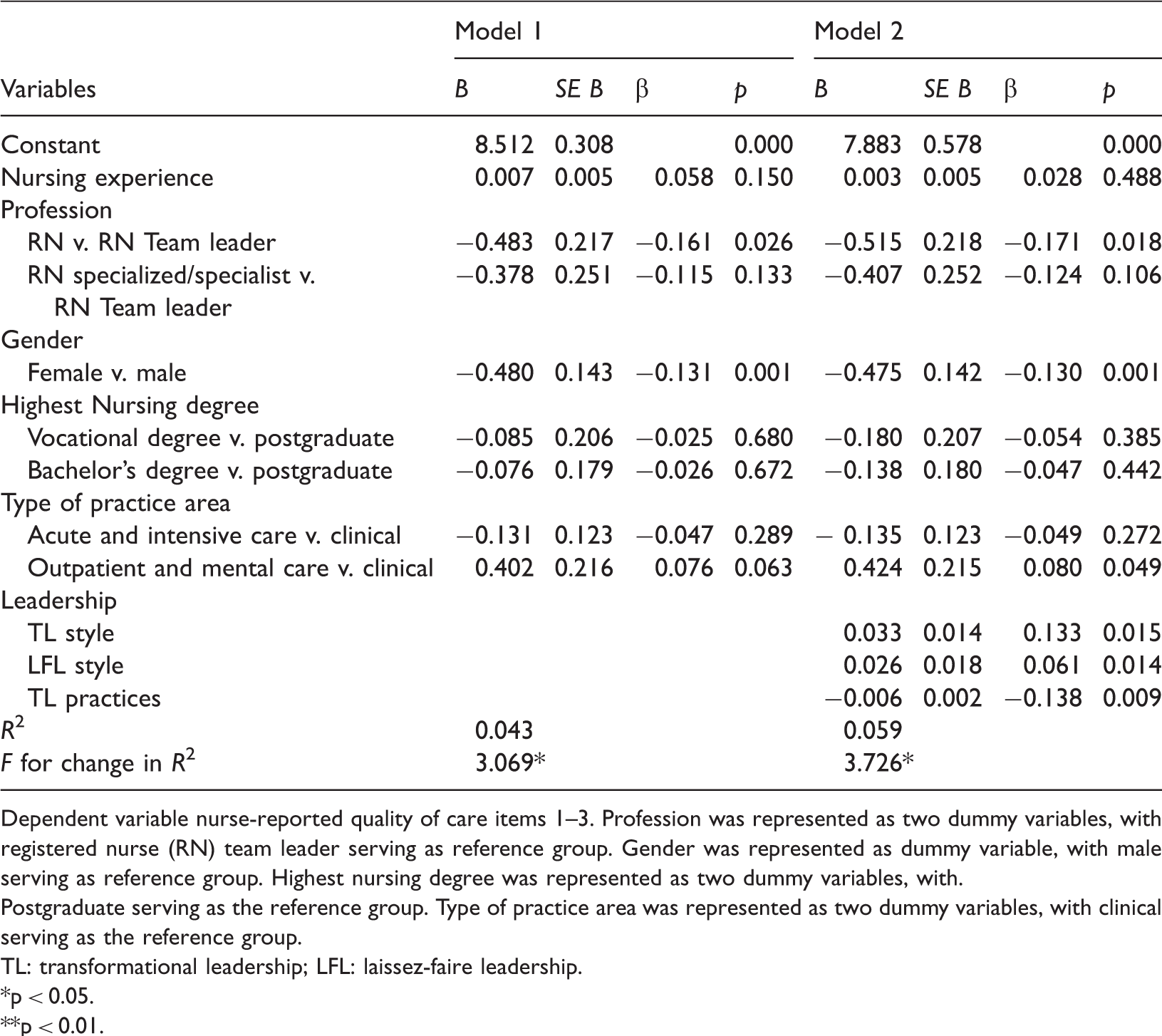
Dependent variable nurse-reported quality of care items 1–3. Profession was represented as two dummy variables, with registered nurse (RN) team leader serving as reference group. Gender was represented as dummy variable, with male serving as reference group. Highest nursing degree was represented as two dummy variables, with.
Postgraduate serving as the reference group. Type of practice area was represented as two dummy variables, with clinical serving as the reference group.
TL: transformational leadership; LFL: laissez-faire leadership.
p < 0.05.
p < 0.01.
Discussion
This study revealed that leadership styles and practices of nurses working on clinical wards are positively associated with QoC, and that nurse characteristics gender, profession and type of practice area significantly influenced this association.
The findings in relation to leadership showed nurses working in daily patient care on clinical wards scored highest on TL, indicating a moderate level of TL practices. Earlier reviews have shown a growing evidence for relationship-focused leadership of nurses, like |TL, impacting nursing outcomes, organisational outcomes, patient outcomes and quality and safety outcomes (Cummings et al., 2018; McFadden et al., 2009, 2015; Wong et al., 2013). However, the studies included in these reviews mainly investigated leadership of nurse managers and not nurses working in clinical practice. To our knowledge this is the first study in Europe to examine the leadership of nurses working on clinical wards. Most studies on the leadership of nurses working in clinical practice were conducted in Canada (Boamah, 2018, 2019) and the USA (Abraham, 2011; Douglas Lawson et al., 2019; Fardellone et al., 2014; Krugman et al., 2000; Shapiro, 1998). This is, to our knowledge, also the first study to measure the level of leadership with the MLQ and the LPI among nurses working on clinical wards. However, a Canadian study showed that nurses scored considerably higher on the clinical leadership scale compared to our results (Boamah, 2018, 2019). This difference may be explained by the fact that leadership has for a long time been recognised as important and is well integrated in the curriculum of Canadian nursing educational programmes (Lavoie-Tremblay et al., 2016). The importance of leadership was only recognised in recent years in the Netherlands and is now being integrated into curricula of some nursing educational programmes. Therefore, due to the longer tradition for leadership training in Canada one can expect the leadership of nurses working in direct patient care in Canada to show stronger leadership than nurses in the Netherlands. Strong TL also motivates colleagues and students to reach their highest potential (Kim, 2020). Therefore, by developing leadership of nurses working on clinical wards, more nurses will reach their potential, which may improve quality and safety.
Our findings in relation to QoC showed that nurses in our study rated the NRQC in their hospital as moderate. Earlier studies conducted in Europe, showed somewhat similar QoC scores (Aiken et al., 2002, 2012; Chevalier et al., 2017; Westerbert and Tafvelin, 2014). Aiken et al. (2012) conducted their study in 12 European countries and showed that 27% of the nurses in Europe reported QoC as ‘poor to fair’; 35% of nurses in the Netherlands and 16% of the nurses in the USA (Aiken et al. 2012), compared to 22.3% of the nurses in our study. Overall, previous studies from Canada and the USA showed higher NRQC scores, compared to our study (Aiken et al., 2012; Spence Laschinger and Fida, 2015; Wong et al., 2010). The differences can be explained by the fact that nurses in Canada and the USA are trained in continuous QoC improvement, also known as part of Quality and Safety Education for Nurses (QSEN, 2013), and thereby have more influence in decision-making concerning QoC compared to in Europe. McFadden et al. (2015) showed the importance of continuous quality improvement to improve the quality of patient safety. Continuous quality improvement is being implemented and the expectation is that the NRQC on clinical wards in the Netherlands will improve as well. However, in order to strengthen quality and safety in healthcare in general, Philipps et al. (2016) emphasised the importance of integrating leadership skills with systems thinking, and QSEN competencies (QSEN, 2013), in curricula of bachelor programmes.
Although our findings strengthen the evidence that the QoC provided by nurses working in direct patient care is influenced by their level of leadership, the association we observed was weak. Our findings are consistent with those of Boamah, who found an association of 23% between the clinical leadership of nurses working on clinical and nurse-reported QoC (Boamah, 2019), which is a considerably stronger association than we found in our study. This difference may be explained by the fact that different instruments were used to measure the same concepts. Our findings showed that the association between leadership and QoC was significantly influenced by gender, profession and type of practice area, which explained 5.9% of the total variance in QoC. The significant influence of profession, nurses in direct patient care (B = –0.515, β = –0.171, p = 0.018), could be explained by the additional training and tasks of team leaders, specialised nurses and nurse specialist. The significant influence of type of practice area, outpatient and mental care practice (B = 0.424, β = 0.080, p = 0.049), could be explained by the individual characteristic of outpatient care, as compared to the team effort on clinical departments, and by a higher degree of standardisation in mental health care. The significant influence of gender, female nurses (B = –0.475, β = –0.130, p = 0.001), could be explained by the fact that of the small group of men (16.3%) participating in our study, most were team leaders. More research is needed to fully ascertain if gender really influences the association with a more equally gender balanced sample of female and male nurses. However, the explanation of the significant association between the leadership of nurses and QoC remains incomplete and further research is needed before practical implications can be made. le May (2020) noted that both QoC and leadership are highly complex concepts, which is difficult to fully capture in one instrument, both concepts are in fact measurable and immeasurable at the same time (le May, 2020). This study used two different instruments to measure leadership and showed the indirect association between leadership of nurses working in daily patient care and QoC. Further research is needed to investigate the association between leadership and QoC in nursing in the various settings of health care. Also research is needed into the training of nurses, especially how they can develop personal leadership and become empowered strong leaders able to influence decision-making to improve patient care, which will likely improve the QoC.
The findings of our study indicate that there is a pressing need for further leadership-training opportunities of nurses working in clinical practice. Strategic managers and team leaders need to understand the importance of leadership in relation to QoC and the need for formal leadership programmes to support nurses working on clinical wards to improve in their leadership development. Also, it is important to integrate leadership education and training in the nursing curriculum of bachelor and post-graduate educational programmes. The type and nature of leadership programmes may vary depending on the nurse’s educational level and specialty area. Leadership programmes for nurses may include the following elements: (a) an opportunity to develop personal leadership development plans, based on key themes of self-acceptance, self-management and self-development, founded in theoretical underpinnings of transformational leadership; (b) theoretical and practical tools, frameworks and practices to help nurses to navigate workplace challenges and to further their abilities to lead, negotiate and influence with impact; (c) an opportunity to develop a self-reflective understanding and acceptance of one’s own unique leadership style and strengths; (d) mentorship with mentors highly experienced in specific specialty or content area; (e) focus on research and translation of evidence into clinical practice to optimise the quality of clinical care; (f) to emphasise the importance of joining national, regional and global nursing networks of like-minded nurses striving to drive gender balance in leadership positions in healthcare. Leadership programmes generally are long-term programmes of 1.5 to 2 years and are increasingly provided through online modules or combination of online with face-to-face opportunities. Examples of leadership programmes for nurses include the National Leadership Mentoring in Nursing Research programme for postdoctoral nurses, which was set up with the aim of increasing the cadre of nurse scientists in the Netherlands (Hafsteinsdóttir et al., 2020) and the Nursing Leadership Educational Program (Nurse-Lead) for doctoral nursing students and postdoctoral nurses in Europe (NurseLead, 2018).
Strengthening leadership development of nurses through leadership education in formal curricula will not be enough because personal leadership practices are learned and developed through intensive training and through daily practice. Personal leadership, like leading, is a craft that needs skills which can be developed through continuous practice. Strategic managers need to support, encourage and motivate nurses working on clinical wards to strengthen their leadership to improve the QoC. Postdoctoral nurses, and master’s educated nurses, the experts in the field of research and evidence-based practice (EBP), are imperative to ensure the empirical foundation informing clinical practice to enhance QoC. Therefore, more advanced career pathways and joint clinical academic positions for these nurses are needed to work on clinical wards to support nurses in translating evidence into clinical practice to strengthen their influence in healthcare quality and safety. Today, nurses, especially postdoctoral nurses and master’s educated nurses, however, lack career perspectives and access to decision-making positions to make the positive changes so badly needed (de Lange et al., 2019). In the recent State of the World’s Nursing Report only 30% of responding countries in Europe reported to have existing advanced nursing roles, compared to 50–75% in other parts of the world (WHO, 2020). Indeed, there seems to be a pressing need both for leadership development opportunities and for the development of advanced positions like combined joint positions combining clinical academic positions and career pathways to provide more career opportunities for master’s educated and postdoctoral nurses.
Strengths and limitations
To appreciate the findings of this study, some limitations must be considered. The different manners of recruitment may have caused selection bias. In two of the UMCs, the nurses were approached directly by a contact person, in the other three UMCs, the contact persons emailed the division managers, followed by an email to middle managers, who emailed the nurses. The latter procedure may have caused some delay and resulted in nurses not receiving an invitation to participate. Although the response rate (18.9%) in our study may be considered as low, it is acceptable in surveys as prior studies on nurses’ attitudes showed a comparable response rate ranging between 11 and 27% (Fink et al.,2005; Hafsteinsdóttir et al., 2013). It is important to note that some of the wards participating were confronted with intense workload due to unprecedented nursing staff shortages and some wards went through organisational changes during the time of the study. However, the characteristics of nurses in our sample are similar to the characteristics of the nursing workforce in Dutch hospitals in general (CBS, 2019; Meza et al., 2014).
Strength of this study was the use of validated and reliable instruments, and all the questionnaires were translated using the back-and-forward method and had a high Cronbach’s α. Also, we used two instruments to measure leadership, namely the MLQ measuring leadership styles and the LPI, measuring TL practices, contributing to a comprehensive measure of leadership. Indeed, the role of leadership is more complex than assessing it for an individual in isolation, since leadership as measured in our study depends on the role of the person concerned and the dynamics with others in the team. To our knowledge, the LPI and MLQ have never been combined in one study, and the combination of both instruments gave more insight into the leadership of nurses.
Conclusion
This study demonstrates that nurses exhibited a moderate level of transformational leadership and rated QoC as moderate. A significant association was found between leadership and QoC, and it explained 5.9% of the total variance with gender, profession and type of practice area as the significant influencing nurse characteristics. Further research on the association between leadership and the QoC is recommended. The findings indicate a pressing need for formal leadership programmes to educate and train nurses working in the clinical arena in further developing their leadership. Also, more emphasis is needed to integrate leadership in the formal curriculum of nursing education. Strategic managers need to support, encourage and motivate nurses working on clinical wards to strengthen their leadership to improve the QoC. Advanced nursing positions and roles are needed to improve QoC. Thereby postdoctoral nurses, and master’s educated nurses, the experts in the field of research and EBP, are imperative to ensure the empirical foundation informing clinical practice to enhance QoC. Therefore, it is imperative that governments and universities provide structural funding for the development of execution of leadership programmes for nurses to secure optimal evidence-based and high-quality and safe care to patients.
Key points for policy, practice and/or research
To strengthen the leadership development of nurses in the clinical arena, the formal support, stimulation and motivation of strategic managers and team leaders is recommended. Joint positions are needed where nurses combine work in clinical practice, research and education to strengthen their influence in healthcare quality and safety. It is imperative that governments and universities provide structural funding for the development and execution of leadership programmes for nurses to secure optimal evidence-based and high-quality care to save patients. Further research is needed to investigate the association between leadership and QoC in nursing in the various settings of health care. Also research is needed into the training of nurses, especially how they can develop personal leadership and become empowered strong leaders able to influence decision-making to improve patient care, which will likely improve the QoC.
Footnotes
Acknowledgements
We would like to thank the nurses for participating in the study and the managers, contact persons, members of the nursing councils and the boards of directors of the UMC’s for their support and making this study possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
A medical research ethics committee confirmed that the study was outside the scope of the Dutch Medical Research Involving Human Subjects Act (Overheid, 2019) (reference number WAG/mb/18/004477) and therefore permission was not needed.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the participating hospitals. The study did not receive a formal grant from funding agencies in the public, commercial or not-for-profit sectors.