
Abstract
Background:
Primary headache and psychiatric diseases are bidirectional correlated. The real-world data of depression and anxiety in Chinese patients hospitalized for primary headache, considering all subtypes, remain unclear.
Methods:
This study enrolled patients attending eight Chinese headache centers from October 2022 to September 2023. A WeChat mini-program was designed to collect data. Headache was diagnosed and confirmed by two headache specialists. The Patient Health Questionnaire-9 and Generalized Anxiety Disorder-7 were used to assess depression and anxiety.
Results:
Overall, 1963 patients with primary headache were analyzed; the prevalence of depression and anxiety was 20.1% (396/1963) and 14.8% (290/1963), respectively. Of the 1963 patients, 217 (11.1%) had history of anxiety or depression and 184 (9.4%) had undergone assessments. Patients with both primary headache and depression were more likely to be women (77.8% vs 71.9%), experience more severe headache (numerical rating scale; 6.2 ± 1.9 vs 5.7 ± 1.9) and greater impacts on quality of life (Headache Impact Test-6; 65.3± 8.5 vs 58.1 ± 11.5). Those with both primary headache and anxiety exhibited similar results and were less educated. Depression and anxiety were more prevalent in chronic migraineurs (CM) than in episodic migraineurs (36.8% vs 16.9% and 28.9% vs 12.3%, respectively) and in those with chronic (CTTH) than in those with episodic tension-type headache (30.6% vs 15.1% and 20.1% vs 12.8%, respectively).
Conclusion:
Depression and anxiety are inadequately diagnosed and strongly associated with sex, severe headache, chronification and disability in patients with primary headache in China. To improve the health of patients with primary headaches, early screening for depression and anxiety is important.
Introduction
Headache disorders are very common. The global prevalence of active headache disorders is 52.0%, and these disorders are among the top five causes of disability-adjusted life years (DALYs).1,2 Primary headache, a dysfunctional disorder includes migraine, tension-type headache (TTH), trigeminal autonomic cephalalgia (TACs), and other primary-headache disorders. 3 Migraine and TTH are the most common forms of primary headache, with prevalences of 9.3% and 10.8% respectively, in China. 4 In the 2019 Global Burden of Disease Study, migraine was reported as the second greatest contributor to neurological DALYs. 5 Chronic headache, is defined as having headaches (TTH episodes and/or migraine attacks) on more than 15 days per month for over than 3 months, leading to higher comorbidity rates and significantly impacting disability scores.3,6 Chronic migraine (CM) is defined as having the features of migraine headache at least 8 days per month. 3
Depression is a common mental disorder, affecting an estimated 322 million people (4.4% of the global population) and accounting for 6.2% of the total disease burden in 2017. 7 A cross-sectional epidemiological study in 2019 found a weighted prevalence of depression at 6.8% in China. 8 Globally, depression was among the top ten causes of disability among individuals aged 10–49 years. 1 According to the World Health Organization, anxiety disorders are prevalent psychiatric disorders, affecting approximately 264 million people (3.6% of the global population) in 2017. 9 In China the weighted prevalence of anxiety was 7.6%. 8 Anxiety disorders have debilitating effects on daily function and well-being and were the sixth greatest contributors to DALYs among individuals aged 10–24 years. 1
The association between primary headache and depression/anxiety is well-established. A meta-analysis showed that the most frequent psychiatric comorbidities in participants with primary headaches were anxiety and depression. 10 Most of the included studies were recruited patients with only migraine. A bidirectional and dose relationship between migraine and depression/anxiety was also identified. Depression and anxiety tends to be more common in patients with migraine than in healthy controls. 11 Data from the population-based Korean Headache-Sleep Study showed that participants with depression are at increased risk of migraine compared with that observed in participants without depression. 12 A cross-sectional study in Taiwan found that higher migraine frequency correlates with higher anxiety and depression symptom scores. 13 Few studies have reported on psychiatric comorbidity in TTH and TACs. Anxiety-related scores tend to be higher in children with TTH than in healthy controls. 11 A cross-sectional, web-based, study using a validated questionnaire study found that cluster headache (CH) is associated with nearly three-fold increased odds of lifetime depression. 14
However, the prevalence and clinical features of depression and anxiety in Chinese patients hospitalized for primary headache, considering all subtypes, remain unclear. We hypothesized that comparing patients with primary headache with and without depression/anxiety might reveal differences in some clinical features and that depression/anxiety might be more common in patients with chronic headache compared to those with episodic headache. This study provided a more comprehensive understanding of depression and anxiety in primary headache, thus helping to guide clinical practice.
Methods
Study design, registration, and patient consent
From October 2022 to September 2023, all consecutive patients with a diagnosis of primary headache attending one of eight China headache centers for the first time were invited to participate in the study. These headache clinics are located in the central, eastern, southern, and western parts of China. The selection method was voluntary enrollment. The study was approved by the Medical Ethics Committee of the Chinese PLA General Hospital (approval number: S2022-302-01) and all participants gave informed consent.
Inclusion criteria were patients aged 18–75 years with primary headache with or without medication-overuse headache (MOH) providing informed consent. Exclusion criteria were secondary headaches except MOH and an inability to answer the questionnaire.
Clinical evaluation
A WeChat mini-program was designed to collect data via a questionnaire. The mini-program contained a computerized clinical decision support system (CDSS) based on the criteria of the International Classification of Headache Disorders, 3rd edition.3,15 Before enrolling patients, doctors in all study centers were trained regarding the mini-program to ensure homogeneity of data entry. The questionnaire covered biographic data, headache symptoms, quality of life (Headache Impact Test-6, HIT-6), symptoms of anxiety and depression (Patient Health Questionnaire-9, PHQ-9 and Generalized Anxiety Disorder-7, GAD-7), sleep quality (Pittsburgh Sleep Quality Index, PSQI), acute headache and prophylactic medications history, psychological history, anxiety/depression assessment, and treatment history.
Headache was diagnosed through CDSS and further confirmed by two headache specialists. The categories included migraine (migraine without aura, MO; migraine with aura, MA; chronic migraine, CM; probable migraine, PM), TTH (episodic tension-type headache, ETTH; chronic tension-type headache, CTTH; probable tension-type headache, PTTH), TACs and other primary headache disorders. Depression was defined as score of ≥10 on the depression items of the scale (PHQ-9), and anxiety as a score of ≥10 on the anxiety items (GAD-7). 16 Insomnia was evaluated using PSQI, chose 5 as the cut-off. 17
Evaluation of sample size
The sample size was estimated using confidence intervals for one proportion in the PASS 15 (NCSS, LLC, Kaysville, UT, USA). According to the previous studies globally, we estimated the prevalence of depression and anxiety with primary headache in China were about 23% and 25%. At 95% confidence level, confidence interval width of 5%, a cross-sectional study comorbid depressive would require at least 1127 patients. The proportion of patients with anxiety in primary headache should be investigated at least 1191. Considering the 90% questionnaire response rate, a total of at least 1324 people should be investigated.
Statistical analysis
Results
In total, 2177 patients were screened at the eight study centers. Of these, 56 patients were age <18 or >75 years, 15 patients did not fully understand the informed consent form because of their education level/language, eight patients were unwilling to participate, and data were lacking for 135. Ultimately, 1963 participants were analyzed.
Baseline characteristics
The characteristics of individuals with primary headache are shown in Table 1. The patients had migraine (1297, 66.1%), TTH (546, 27.8%), TACs (84, 4.3%), and other headaches (36, 1.8%). The mean age of all patients was 39.9 years and 1435 (73.1%) were women. Regarding education level, 937 (47.7%) participants had high school or less. The headache duration was 9.2 ± 9.0 years. The severity (pain score on a numerical rating scale, NRS) of headache was 5.9 ± 2.0. There was a family history of headache in 687 (35%) participants. The mean HIT-6 score in all patients was 58.8. There were 528 (26.9%) patients with mild (5 ≤ GAD-7 score ≤ 9), 168 (8.6%) with moderate (10 ≤ GAD-7 score ≤ 14), 93 (4.5%) with severe (15 ≤ GAD-7 score ≤ 19), and 29 (1.5%) with extremely severe (≥20) anxiety. Based on GAD-7 ≥ 10, the prevalence of anxiety in primary-headache patients was 14.8% (290/1963). The corresponding rates of depression were 29.2%, 12.7%, 5.4%, and 2.0%, respectively. As depression was defined as PHQ-9 ≥ 10, its prevalence in primary-headache patients was 20.1%. 217(11.1%) had anxiety/depression history and 184 (9.4%) patients had anxiety/depression assessments previously (See the Table 1 for further details).
Characteristics of individuals with primary headache.

TTH: Tension-type headache; TACs: Trigeminal autonomic cephalalgias, NRS: numerical rating scale; MOH: Medication overuse headache; HIT-6 Headache Impact Test.
New daily persistent headache two cases, Nummular headache 1 case, Primary stabbing headache1 case.
Data are missing for 369 (18.8%) patients.
Prevalence and clinical features of depression/anxiety in primary headache
Compared to primary-headache patients without depression, those with both were more likely to be women, to accept prophylactic treatment, and to have more severe headache, higher HIT-6 scores, and comorbid insomnia (see Table 2 for details). The same was true for those with headache and anxiety, except those patients were also less educated (Table 3). No significant differences were found in the primary classification of headache between those with/without depression and those with/without anxiety (Figure 1).
Characteistics of depression in primary headache.
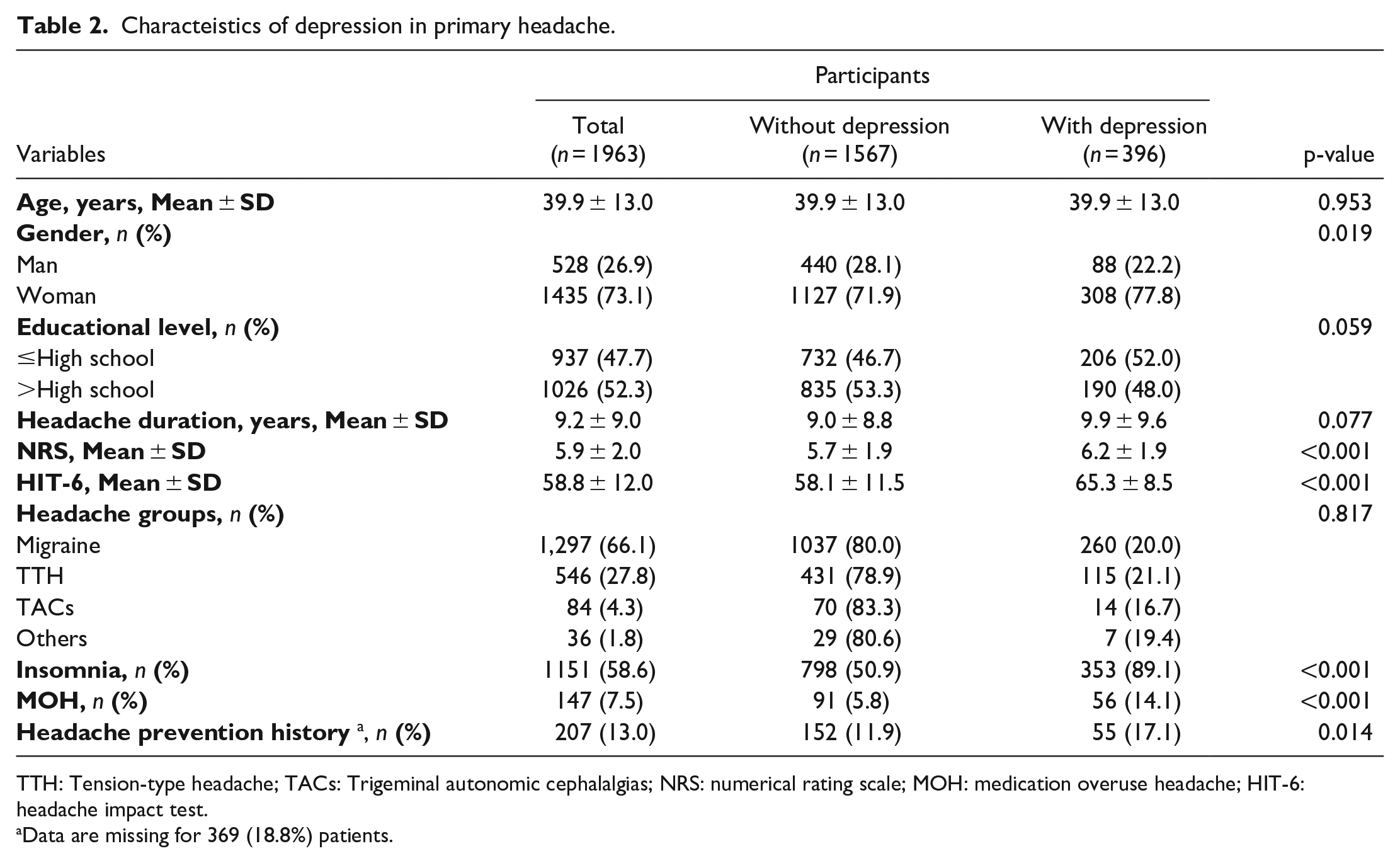
TTH: Tension-type headache; TACs: Trigeminal autonomic cephalalgias; NRS: numerical rating scale; MOH: medication overuse headache; HIT-6: headache impact test.
Data are missing for 369 (18.8%) patients.
Characteistics of anxiety in primary headache.

TTH: tension-type headache; TACs: trigeminal autonomic cephalalgias; NRS: numerical rating scale; MOH: medication overuse headache; HIT-6: headache impact test.
Data are missing for 369 (18.8%) patients.

Differences in the prevalence of depression and anxiety among groups by headache subtype. a.Differences in the prevalence of depression among groups by headache subtype. b. Differences in the prevalence of anxiety among groups by headche subtype.TTH: tension-type headache; TACs: trigeminal autonomic cephalalgia.
Next, based on the criteria of the International Classification of Headache Disorders, 3rd edition, we subdivided migraine and TTH by their frequency into episodic (EM) versus chronic (CM) migraine and chronic (CTTH) versus episodic (ETTH) TTH and compared their respective associations with depression/anxiety. The prevalence of depression did not differ between the EM and ETTH, CM and CTTH, and migraine and TTH groups. However, depression was significantly more common in the CM group vs the EM group (36.8% (75/204) vs 16.9% (185/1093)) and in the CTTH vs the ETTH (30.6% (64/209) vs 15.1% (51/337), both p < 0.001). See details in Figure 2.

Differences in the prevalence of depression between groups by headache type and frequency. a. Compared the prevalence of depression between groups by headache type. b. The difference in the prevalence of depression between groups by headache frequency.
Figure 3 compares the corresponding results for those with/without anxiety. The rate of anxiety was significantly higher in the CM versus the CTTH group (28.9% (59/204) vs 20.1% (42/209), p < 0.05), the CM vs the EM (28.9% (59/204) vs 12.3% (134/1093), p < 0.001) group, and the CTTH vs the ETTH (20.1% (42/209) vs 12.8% (43/337), p < 0.05) group. There were no other associations.

Comparison of the prevalence of anxiety between groups by headache type and frequency. a. Comparison of the prevalence of anxiety between groups by headache type. b. The differences of the prevalence of anxiety between groups by headache frequency.
Prevalence of primary headache subtypes depending on the presence of depression/anxiety
Of 396 participants with both headache and depression, 157 had MO, 75 had CM, 10 had MA, 18 had PM, 50 had ETTH, 64 had CTTH, 1 had probable TTH, 14 had TACs, and 7 had other primary headache disorders. The prevalences of both CM and CTTH were significantly higher, whereas those of MO and ETTH were significantly lower, among depressive participants (Figure 4).

Differences in headache type according to the presence of depression/anxiety. a. Differences in headache type according to the presence of depression. b. Differences in headache type according to the presence of anxiety.
Of the 290 participants with anxiety, 112, 59, 7, 11, 46, 42, 1, 9, and 3 had MO, CM, MA, PM, ETTH, CTTH, probable TTH, TACs, and other primary headache disorders, respectively. CM and CTTH were again more prevalent, whereas MO was less common, in patients with both headache and anxiety (Figure 4).
Discussion
This study explored the prevalence and clinical features of depression and anxiety in patients with primary headache who visited eight Chinese headache centers. Our main findings are as follows. First, the prevalence of depression and anxiety in patients with primary headache was 20.1% and 14.8%, respectively. Second, patients with both headache and depression or headache and anxiety were more likely to be women, have more severe headache, experience greater impacts on quality of life, undergo prophylactic treatments, and have comorbid insomnia and MOH; those with anxiety were also less educated. Third, depression and anxiety were more common among those with CM than among those with episodic migraine (EM), and more common in those with chronic TTH (CTTH) than among those with episodic TTH (ETTH); anxiety was also more common among those with CM than those with CTTH. Finally, CM and CTTH were more prevalent in participants with depression/anxiety than in those without these conditions.
To the best of our knowledge, this study is the first to investigate the prevalence of depression and anxiety in patients hospitalized for all subtypes of with primary headache in mainland China. In the Eurolight project, gathered population-based data on headache disorders and psychiatric disorders from 6624 participants of 10 EU countries, depression and anxiety were present in 6.9% and 19.1% of the subjects with migraine, respectively, while we found respective prevalences of 20% and 14.9% in migraine. 18 The prevalences of depression and anxiety in patients with TTH in the Eurolight project were 4.5% and 12.1%, respectively; in our study, the prevalences were 21.1% and 15.6%, respectively. 18 A cross-sectional study on comorbidities in patients with migraine in Japan shown depression and anxiety comorbidity rates of 22.2% and 14.6% respectively, which is similar to our study. 19 A meta-analysis reported depression and anxiety comorbidity rates of 23% and 25% respectively, in patients with primary headache patients; whereas the rates were 20.1% and 14.8% in our study. 10 Most studies on the co-prevalence of primary headache and psychiatric comorbidities have focused on migraine. Previous studies have summarized the literature, citing depression to be 2.2- to 4.0-fold more likely to occur in patients with migraine compared with the general population. 20 Consistent with their results, we found depression to be 2.9-fold more prevalent in patients with migraine (20%) compared with the general population (6.8%). Anxiety disorders are 2.0- to 5.0-fold more prevalent in patients with migraine than in the general population. 21 In this study, anxiety was approximately 2.0-fold more prevalent in patients with migraine (14.9%) compared with the general population (7.6%). A study of 10 Italian Headache Centers found that the prevalences of depression and anxiety in patients with TTH were 36.4% and 52.5%, respectively; in our study, the prevalences were 21.1% and 15.6%, respectively. 22 A previous study reported that the the rates of depression and anxiety were 6.3% and 15.6%, respectively in episodic CH, and were both 11.8% in chronic CH. In our study, the prevalences of depression and anxiety in patients with TACs were 16.7% and 10.7%, respectively. 23 The differences among studies may result from differences in ethnicity, sample sizes, the inclusion and diagnostic criteria, and heterogeneity among the studies.
We found that only 11.1% of the participants with primary headache had a history of anxiety or depression and 9.4% of the participants had undergone previous psychological assessment, indicating that primary headache with comorbid depression/anxiety was often overlooked. Cross-sectional and longitudinal studies have reported mood disorders, especially depression, as an independent risk factor for early migraine development and as presenting with worse prognosis. 24 Meanwhile, depression and anxiety significantly impact the quality of life and increase the financial burden on patients with episodic and chronic headaches.25,26 Early detection and intervention for depression and anxiety are essential for managing patients with headache. Antidepressants have proven effective and are first-choice drugs for the prophylactic treatment of patients with primary headache with comorbid depression.27,28
We also found that females with primary headache were more susceptible to depression or anxiety. This finding aligns with the general epidemiology of depression and anxiety, which indicates that these conditions are more common among women than among men. 8 Depressive disorders ranked among the top ten causes of DALYs for females but not for males aged 10–74 years. Anxiety disorders are among the top ten causes of DALYs for females aged 10–49 years. 1 The underlying biological factors and mechanisms contributing to these differences remain largely unknown. Psychopathological findings suggest that brain structure and function vary with naturally-cycling ovarian hormones.29,30 Additionally, anxiety was strongly associated with education level, with those having less education being more susceptible. While some studies have found a positive impact of education on mental well-being, this impact is potentially mediated through better physical health and improved health behavior and knowledge. 31 Furthermore, we found that those with headache concomitant with depression or anxiety tended to have more severe headaches and a greater headache impact compared with those without these comorbidities. These results are consistent with population-based studies and findings from patients with headache referred to headache specialists.12,32
Notably, the rate of comorbid depression and anxiety was higher in patients with CM or CTTH than in those with EM or ETTH, suggesting that there is a dose–response relationship between the two disorders and indicating that severe primary headache is associated with a more robust association with depression/anxiety. This finding is consistent with previous studies. The Migraine in America Symptoms and Treatment Study indicated that increasing monthly migraine frequency days was associated with increased risks of anxiety and depression, and higher headache frequency and severity correlate with a heavier burden of psychiatric comorbidities in migraineurs.33,34 A population-based study of TTH found that mental health component scores were lower in patients with pure CTTH, followed by chronic coexisting headache, EM with or without ETTH, and pure ETTH compared to those without headache. 35 We also found that patients with CM had a higher comorbid anxiety rate than those with CTTH. Similar to our findings, a study comparing the quality of life in patients with CM and CTTH showed that somatic anxiety subscale score of the Hamilton Anxiety Rating Scale was higher in the migraine group than in the TTH group. 36 Simultaneously, depression and anxiety group had a higher ratio of patients with CM and CTTH. Depression and anxiety are associated with more severe symptoms, more frequent attacks, and chronic headaches, and a higher tendency of medication overuse.37,38
The comorbidity between depression/anxiety and chronic headache indicates that the pathophysiology of these disorders may share several, common mechanisms. The anterior cingulate cortex (ACC) is a key structure involved in various higher brain functions, such as nociception, chronic pain, cognition, and emotions. 39 Increasing evidence from both clinical and rodent studies revealed that ACC activation contributes to chronic migraine. Atypical functional connectivity is found between ACC and pain-facilitating, pain-inhibiting regions in CM and rat model of recurrent headache. 40 The synaptic plasticity that may underlie this effect is one form of long-term potentiation (LTP) in the ACC which is triggered by the activation of N-methyl-D-aspartate (NMDA) receptors sustains the affective component of the pain state and another form of LTP which is triggered by the activation of kainate receptors may contribute to pain-related anxiety. 41 Neuroimaging studies have also implicated the dysregulation of both hypothalamic and thalamic pathways as a possible cause of this comorbidity. 24 Similarly, the altered hypothalamic–pituitary–adrenal axis and neurolimbic network may also contribute to this comorbidity. 38 In addition, migraine can be treated with drugs acting on the serotonin system, such as triptans (i.e. painkillers), serotonin and noradrenaline reuptake inhibitors, and tricyclic antidepressants. 38 This suggests that neurotransmitters may play a key role in the pathophysiology of such comorbidity.
This study has several strengths. First, we included a large sample from eight Chinese headache centers. Second, a uniform questionnaire was administered in the clinic by trained doctors. However, our study also had some limitations. Firstly, as the patients seen at the clinics were not selected based on random sampling, they may not be representative of all patients with primary headache in China. Second, a diagnosis focusing on the most problematic headache features may neglect combinations of multiple headache types within the same patient cohort. Finally, the PHQ-9, GAD-7, and PSQI are screening instruments for depression and anxiety rather than diagnostic tools, which may lead to underestimation of the prevalences of both disorders.
Conclusions
The prevalence of depression and anxiety in Chinese patients hospitalized with primary headache was 20.1% and 14.8%, respectively. Depression and anxiety in primary headache were strongly associated with sex, severe headache, being on disability, insomnia and MOH. Depression and anxiety were more common in patients with chronic than episodic headache, and more chronic headache contained in the comorbid depression/anxiety group. Depression and anxiety in primary headache disorders are inadequately diagnosed in China. To improve the health of primary headaches, screening for depression and anxiety should be performed early.
Footnotes
Acknowledgements
We thank all patients who took part in the study.
Abbreviations
DALYs: disability-adjusted life years;TTH: tension-type headache; TACs:trigeminal autonomic cephalalgia; CM:chronic migraine; EM: episodic migraine; CH: cluster headache;MOH: medication-overuse headache; CDSS: clinical decision support system; HIT-6: Headache Impact Test-6; PHQ-9:Patient Health Questionnaire-9, GAD-7: Generalized Anxiety Disorder-7; PSQI: Pittsburgh Sleep Quality Index; MO: migraine without aura; MA: migraine with aura; PM: probable migraine; ETTH: episodic tension-type headache; CTTH: chronic tension-type headache; PTTH: probable tension-type headache; NRS: numerical rating scale.
Authors contributions
Zhihua Jia collected, analysed and interpreted the data and results, and drafted the manuscript. Dongjun Wan, Zhiliang Fan, Peng Xu, Xueqian Yuan, Min Chen, Dan Wang, Hebo Wang, Hui Su, Xun Han, Zhe Yu, Yingji Li collected and organized the data of patients. Ruozhuo Liu, Xiaolin Wang, Rongfei Wang analysed the data and visualized the results. Ziming Yin, Shuhua Zhang, Shengshu Wang analyzed and modified the questionnaire. Shengyuan Yu and Zhao Dong proposed the concept and design of the study and revised manuscript for critical intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (grants 2023YFC2508701), and the Natural Science Foundation of Gansu Province (grants 21JR1RA187).