
Abstract
Chronic low back pain (CLBP) is often treated with opioid analgesics (OA), a class of medications associated with a significant risk of misuse. However, little is known about how treatment with OA affect the brain in chronic pain patients. Gaining this knowledge is a necessary first step towards understanding OA associated analgesia and elucidating long-term risk of OA misuse. Here we study CLBP patients chronically medicated with opioids without any evidence of misuse and compare them to CLBP patients not on opioids and to healthy controls using structural and functional brain imaging. CLBP patients medicated with OA showed loss of volume in the nucleus accumbens and thalamus, and an overall significant decrease in signal to noise ratio in their sub-cortical areas. Power spectral density analysis (PSD) of frequency content in the accumbens’ resting state activity revealed that both medicated and unmedicated patients showed loss of PSD within the slow-5 frequency band (0.01–0.027 Hz) while only CLBP patients on OA showed additional density loss within the slow-4 frequency band (0.027–0.073 Hz). We conclude that chronic treatment with OA is associated with altered brain structure and function within sensory limbic areas.
Introduction
Chronic low-back pain (CLBP) is a leading cause of disability worldwide and its prevalence is on the rise.1–3 OA are commonly prescribed for the management of CLBP4,5 and the most frequent indication for the use of prescription opioids in primary care settings 6 is for CLBP. Opioids pose a high risk for addiction because their analgesic effects are mediated primarily via binding to the µ-opioid receptor. 7 Once started on these medications, CLBP patients frequently continue using opioids for years 8 and long-term opioid use for non-cancer pain dose-dependently increases the risk of overdose, misuse, and addiction.9–13 The misuse of prescription opioids contributes significantly to the public health crisis that we now face.14–16 In fact, a majority of today’s heroin abusers were introduced to opioids via medical prescriptions. 17 Despite their widespread use and associated morbidity/mortality, an understanding of how opioids affect brain circuitry in chronic pain patients is lacking. Such knowledge is crucial for a full understanding of the neurobiology of opioid addiction and identifying predictors of the risk of opioid misuse and addiction.
Short-term administration of increasing doses of OA in healthy humans undergoing fMRI shows that the limbic brain (amygdala, para-hippocampal area, and anterior insula) is exquisitely sensitive to low doses of opiates, 18 while higher doses decrease the perception of acute pain with a corresponding decrease in brain activity in the thalamus, primary and secondary somatosensory areas, insula, and anterior cingulate cortex (ACC).18–20 Collectively, these areas are consistently active in response to acute pain.21–23
However, the effects of chronic µ-opioid agonists on brain activity, network topology, and structure in chronic pain patients are largely unknown. Younger et al. 24 studied the brain structure in 10 CLBP patients before and one month after the administration of morphine and identified a decrease in amygdala volume and increase in the ACC, hypothalamus and prefrontal cortex volumes relative to placebo. Martucci et al. 25 investigated the effect of OA on reward-related decision making and brain circuitry in a cohort of fibromyalgia patients taking a stable dose of OA. Interestingly, they observed that the brain response during reward anticipation in medicated patients was not different from that of healthy controls in the nucleus accumbens and medial prefrontal cortex. Only unmedicated patients showed abnormal responses to reward anticipation in the medial prefrontal cortex. These results, unexpectedly, demonstrate a “normalization” of neural responses to rewarding stimuli in chronic pain patients medicated with OA.
In this article we study the brain structure and function of CLBP patients medicated with OA with no evidence of misuse and compare them to unmedicated CLBP patients and healthy controls. Given that the limbic system is rich in opioid receptors26–32 and the recent evidence supporting the critical role of the limbic system in chronic pain,33–36 our starting hypothesis was that the limbic brain of medicated patients should be significantly altered compared to non-medicated patients and healthy controls.
Material and methods
Participants
Eleven chronic low-back pain patients treated with opioid analgesics (CLBP-op), 30 chronic low-back pain patients not medicated with opioid analgesics (CLBP-no-op), and 30 healthy controls (HC) participated in this study. All CLBP patients reported low back pain of at least 30 out of 100 on the visual analogue scale (VAS; 0–100, where 100 = maximum imaginable pain and 0 = no pain) for at least 1 year. All CLBP-op patients were prescribed OA by their physicians for at least 1 year, except one patient who had been taking them for 4 months at the time of the study. Patients’ prescription were confirmed online using the Connecticut Prescription Monitoring and Reporting System (https://connecticut.pmpaware.net/login). Participants were excluded if they reported aberrant drug taking behavior at the intake visit, pain at other locations, systemic illnesses, psychiatric diseases, history of traumatic brain injury, or if they tested positive on a urine toxicology test for drugs other than opioid analgesics. All patients reported no or less than mild depression (i.e. Beck’s Depression Inventory (BDI) scores between 14 and 19) except 3 CLBP-op and 3 CLBP-no-op patients who reported moderate depression (BDI
Demographic and clinical variables.
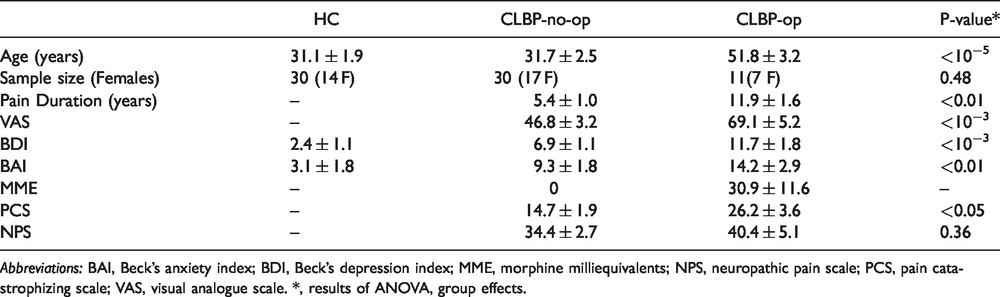
Abbreviations: BAI, Beck’s anxiety index; BDI, Beck’s depression index; MME, morphine milliequivalents; NPS, neuropathic pain scale; PCS, pain catastrophizing scale; VAS, visual analogue scale. *, results of ANOVA, group effects.

Sub-cortical volumes in CLBP patients. CLBP-op patients chronically treated with opioids show significantly smaller nucleus accumbens and thalamus volume (p-value was obtained from GLM analysis, corrected for age, gender and intracranial volume). Volumes were extracted using FIRST. #, p < 0.05; post-hoc analysis comparing CLBP-op, CLBP-no-op to healthy controls; *, p < 0.05; post-hoc analysis comparing CLBP-op and CLBP-no-op.
Magnetic resonance imaging
Participants underwent an anatomical T1-weighted scan and two-consecutive 6-minute long resting-state functional (fMRI) scans. All imaging data was collected on a Siemens 3 T Trio magnet equipped with a 32-channel head-coil. The T1-weighted acquisition used a 3 D MPRAGE sequence with the following parameters: TR/TE = 1900/2.52 ms, flip angle =9°, matrix = 256 x 256 with 176-1mm slices acquired in the same orientation as the functional data. During the functional scans, participants were asked to stare at a fixed cross hair. The fMRI sequence had the following parameters: TR/TE = 1000/30.0 ms, flip angle = 60°, matrix = 110 x 110 x 60 with 2-mm isotropic voxels, and an acceleration factor of 4.
Subcortical volume calculations
Structural data were analyzed with the standard automated processing stream of the Functional Magnetic Resonance Imaging of the Brain’s (FMRIB) software library (FSL), version 5.0.10, which shows high reliability across laboratories. 37 The processing sequence includes skull removal, a two-stage linear subcortical registration, and segmentation using FMRIB’s Integrated Registration and Segmentation Tool (FIRST). 38 The volumes of the right and left nucleus accumbens (NAc), amygdala, hippocampus and thalamus were calculated for each participant and normalized to standard Montreal Neurologic Institute (MNI) space. The normalization coefficient was calculated using FSL’s SIENAX. 39 Quality control included: (i) visual inspection of subcortical segmentation to identify gross mismatches between underlying anatomy and FIRST output; (ii) identification and exclusion of outliers defined using Tukey’s method; 40 and (iii) comparison of signal-to-noise ratio (SNR) within each subcortical structure across groups. SNR was calculated as the mean signal within a certain structure minus the mean signal outside the brain divided by the standard deviation of the signal outside the brain. Outliers were defined independently for each structure. One participant’s data was excluded as such; importantly, removing this individual did not change our statistical results.
Functional MRI preprocessing
Two 6-minute long resting-state fMRI scans were acquired consecutively while participants stared at a fixed cross hair. The preprocessing of each participant’s fMRI time series was performed using FSL’s Expert Analysis Tool (FEAT). Preprocessing included skull removal using Brain Extraction Tool (BET), motion correction, 41 band pass filtering (0.008–0.2 Hz), and spatial smoothing (5-mm full width at half maximum Gaussian blur). Several sources of spurious variance were removed from the data with linear regression. The 6 parameters obtained by rigid head motion correction along with their temporal derivatives and 10 components derived from noise regions of interest (ROIs) were regressed out from the data. The latter components were identified following an anatomical approach as described previously. 42 Briefly, cerebrospinal fluid and white matter average time series were extracted from each subject’s fMRI data based on masks derived from the high-resolution anatomical image using FSL’s FAST. 43 Next, principal component analysis was applied to obtain the first 5 white matter and first 5 CSF components. After preprocessing, the functional scans were registered into the MNI space. Registration to high resolution structural and/or MNI images was carried out using FLIRT.41,44 Registration from high resolution structural to MNI space was then further refined using FNIRT nonlinear registration. 45
Spectral analysis
Spectral analysis was performed using custom Matlab (The MathWorks, 2018) routines and is similar to previously reported methods. 46 The frequency power of the BOLD signal was determined voxel-wise using Welch's method and normalized by dividing by total power. This normalization was necessary as the absolute power of BOLD remains unknown simply because the absolute intensity of BOLD signal in time space is also unknown and assigned an arbitrary value in all standard fMRI analyses. The average power of each frequency band, 47 slow-5 (0.01–0.027 Hz), slow-4 (0.027–0.073 Hz), slow-3 (0.073–0.198 Hz) and slow-2 (0.198–0.5 Hz), was calculated at each voxel and converted into 4 different maps for each subject. Individual subjects ’ maps were transformed into standard space as described in the preprocessing section and multiplied by a standard gray matter mask. Subject-level maps were transformed to z-score maps by subtracting the mean voxel-wise power for the entire brain and dividing by the standard deviation. Group differences were generated using permutation based inference (p< 0.05) 48 . They were tested against 10,000 random permutations, which inherently corrects for multuple comparisons. Clusters were identified using threshold-free cluster enhancement method(TFCE) 49 .
Statistical analyses
Statistical analyses of demographic and clinical variables and of extracted sub-cortical volumes were performed using Statistica Software (TIBCO, Inc.). Between-group analysis was performed using general linear model or ANOVA. We used linear regression analyses to investigate the relationships between reported pain according to VAS scores or levels of inflammatory markers and brain measures
Results
Demographic and clinical variables
CLBP-op patients were significantly older (p < 10−3, ANOVA post-hoc comparisons) than CLBP-no-op and HC subjects. The 3 groups did not differ in terms of the distributions of genders. Clinically, CLBP-op reported significantly larger (p < 10−3) BDI depression scores and larger (p < 0.01) BAI anxiety scores. CLBP-op patients experienced a significantly higher pain intensity than CLBP-no-op (CLBP-op VAS = 69.1 ± 5.2 (mean ± SEM); CLBP-no-op = 46.8 ± 3.2; p < 10−3, unpaired t-test) for a longer duration of time (CLBP-op = 11.9 ± 1.6 years; CLBP-no-op = 5.4 ± 1.0, p < 0.01). CLBP-op patients also demonstrated significantly more pain catastrophizing (p < 0.05). These results are summarized in Table 1.
Nucleus accumbens and thalamic volumes are compromised in CLBP patients on opioids
We compared subcortical volumes between the groups extracted using FIRST after correcting for age, gender, and intracranial volume. Group effects were significant for the NAc (p = 0.014, effect size partial-η 2 = 0.12) (adding left and right) and close to significant for the thalamus (p = 0.06, partial-η 2 = 0.07) (Table 2). Post-hoc comparisons showed that both CLBP-op (p = 0.004, Cohen’s d = 0.83) and CLBP-no-op (p = 0.018, Cohen’s d = 0.67) had a significantly smaller NAc compared to healthy controls, while only CLBP-op patients exhibited a significantly smaller thalamus relative to both CLBP-no-op patients (p = 0.01; Cohen’s d = 0.56) and healthy control subjects (p = 0.0014;Cohen’s d = 0.83) . Amygdala and hippocampus volumes did not show any group effects. We repeated the volumetric comparisons after including potential confounders in our model like measures of depression, or anxiety which can be independently associated with cortical and sub-cortical changes. 50 Table 2 shows that results remain practically the same. Importantly, SNR group comparisons revealed a significant drop in SNR in all structures examined in the CLBP-op group (Figure 3). This observation prompted us to repeat our volumetric comparisons after correcting for SNR in our GLM model, but group differences presented in Figure 1 persisted, if not, slightly increased (Table 2). We also examined the relationship between clinical variables and volumetric measures in medicated and unmedicated patients separately using correlation analyses to check whether observed group differences scale with pain intensity or duration or measures of depression or anxiety. Table 3 shows that none of the clinical measures showed significant correlation to the volumetric measures .
Sub-cortical volumes in centimeter cubes.
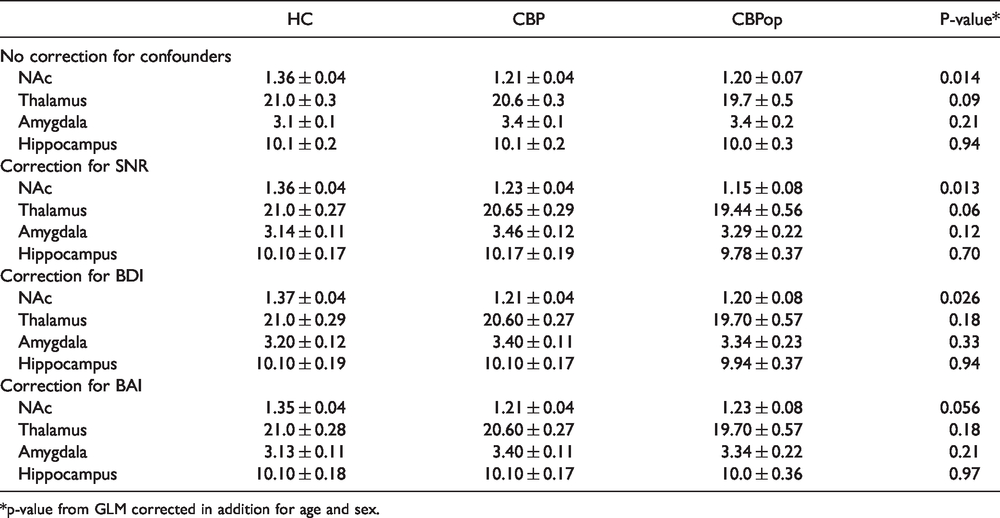
*p-value from GLM corrected in addition for age and sex.
Correlation analysis* between clinical variables and volumetric measures.

*None of the correlation analyses survived p-value threshold < 0.05.

Signal to noise ratio differs by medication status. CLBP-op patients chronically treated with opioids have a significant drop in signal to noise ratio (SNR) in all the structures examined. (p-value was obtained from GLM analysis, corrected for age, and gender).

NAc PSD. (A) CLBP-no-op and (B) CLBP-op patients show loss of slow-5 (0.01–0.27 Hz) PSD within the NAc compared to healthy controls (p < 0.05, ROI corrected). No significant difference was observed between medicated and unmedicated CLBP. C, Histogram plot illustrates slow-5 PSD within the cluster shown in A&B. D and E, NAc slow-4 (0.027–0.073 Hz) PSD is significantly decreased in CLBP-op patients only. Heat map, T-score.
CLBP-op have a different pattern of power spectral density changes
We also wanted to examine whether structural changes observed in CLBP-op patients is accompanied by altered brain activity dynamics collected during resting state scans. Therefore, we calculated the voxel wise power amplitude of spectral density (PSD) normalized by the sum across the whole frequency range.
46
The amplitude of PSD of BOLD signal exhibits consistent regional distribution across studies,46,47,51 and moderate-to-high intra-subject reliability.
47
In addition, it has been repeatedly shown to identify specific changes in clinical populations,
52
including chronic pain patients.53–55 Germane to the current study, we recently identified that loss of PSD within the slow-5 (0.01–0.027 Hz) frequency band of the NAc is a reproducible signature of CLBP.
36
Therefore, we wanted to test whether long-term exposure to opioid analgesics changes this signature. This is an important question given that the NAc is rich in opioid receptors,
56
which are directly involved in rewarding and aversive learning, and both acute and chronic pain in humans.57–60 Slow-5 frequency maps from the 3 groups were entered into an ANCOVA (corrected for age, gender) within the bilateral NAc ROI and the differences between the groups (i.e. F-test) were significant (p < 0.05, ROI corrected).
Discussion
CLBP patients medicated with opioid analgesics are at an increased risk for developing long-term misuse, dependence, or addiction. 61 The neurobiological determinants of this risk are still unknown. Our data suggests that chronic treatment with opioid analgesics is associated with significant alterations in the structure and function of the limbic brain and thalamus before the appearance of any aberrant medication taking behavior. As such, both CLBP-no-op and CLBP-op patients exhibit decreased NAc volumes compared to healthy controls. In addition, only CLBP-op group exhibited a significant drop in thalamic volume compared to CLBP-no-op and healthy controls. Altered subcortical volume was accompanied with a loss of NAc PSD in the slow-5 (0.01–0.027 Hz) frequency band of all CLBP patients and a loss of PSD in the slow-4 (0.027–0.073 Hz) frequency band only in CLBP-op cohort.
This is one of the very few studies 24 examining the long term effects of opioid analgesics on the brain of CLBP pain patients. Both prescription and illicit opioids (e.g. heroin) exert their analgesic and addictive effects primarily through the µ-opioid receptor.7,62 The binding of opioids in the limbic circuitry plays a critical role in analgesia, 32 learning and value-based decision making,63,64 and hedonic processes.65,66 For example, the infusion of naloxone, a µ-opioid receptor antagonist, into the basolateral amygdala decreases lever pressing for food in deprived rodents previously trained to associate lever pressing with delivery of a sucrose reward. 67 On the other hand, infusion of a µ-opioid receptor agonist into the ventral striatum, which encompasses the NAc, leads to analgesia and increased palatability (i.e. hedonic value) of food. 68 In humans, µ-opioid receptor agonists enhance the pleasantness of drinks with high levels of sweetness. 69 It is widely argued that the ventral striatum and medial prefrontal cortex encode the subjective value of all aversive and rewarding stimuli on a common scale.70–73 Specifically, ventral striatum and medial prefrontal cortex responses to rewards including food, money, and addictive substances, correlate with subjective ratings of reward value in humans such as food liking and magnitude of drug craving,74–83 and their activity tracks also back pain intensity.84–86 Importantly, one recent study showed that increased medial prefrontal cortex activity in response to alcohol cues predicts the risk of relapse in abstinent alcohol-dependent individuals. 87 Our results suggest that, consistent with the distribution of opioid receptors in the brain and the role of these receptors in these areas in value-based decision-making and pain, treatment with opioid based medications in chronic pain might exert its long-term effects on behaviors such as aberrant drug use via action within the limbic brain.
We also determined that long-term treatment with opioid-based medications did not alter the NAc slow-5 PSD in CLBP patients. This is an important observation given that the loss of slow-5 PSD within the NAc is a robust signature of CLBP. 36 It implies that chronic opioid agonists binding in the NAc may not be able to reverse a central nervous system functional signature of the state of being in chronic pain. Nevertheless, patients chronically treated with opioids showed loss of slow-4 PSD, suggesting that this latter frequency band is sensitive to OA treatment.
Opioid agonists can reduce water content in brain slices 88 hence decreasing the number of protons and leading to a weaker T1 signal. 89 The effect of opioid agonists on water movement may therefore explain the consistent drop in SNR across all studied subcortical areas observed in CLBP-op patients. Young et al. 24 reported a drop in amygdala volume following the long-term administration of prescription opioids compared to placebo in CLBP patients using tensor based morphometry, which is different from the subcortical extraction technique we used in this manuscript. While Upadhyay et al. 90 reported also that opioid dependent individuals exhibit decreased amygdala volumes, Seifert et al. 91 reported only a drop in left NAc volume. Chronic morphine administration in animals have been shown to reduce the size but not the number of dopaminergic neurons in the ventral tegmental area, 92 induce remodeling of dendritic spines in the NAc 93 and medial prefrontal cortex, 94 and disinhibit mesolimbic dopaminergic firing. 95 The effect of chronic morphine administration on thalamic structure is still unclear. However, neurochemical studies show that acute morphine administration decreases glucose utilization 96 and the BOLD signal, 97 while chronic administration decreases the level of glutamate, an excitatory neurotransmitter, in the thalamus 98 hence inducing a generalized decrease in activity. Whether this decrease in activity is reflected by the volumetric shrinkage we observed remains to be determined. Interestingly, a projection from the paraventricular thalamus to the NAc has been shown to be necessary and sufficient for opioid withdrawal induced physical signs and aversive memory in rodents. 99 Taken together, this structural brain data points to an association between thalamic and limbic brain changes and opioid use or misuse. It is still however unknown whether these changes are induced by chronic intake of opioid analgesics or predate the start of treatment. Well powered longitudinal within-subject studies using different structural analysis algorithms100,101 are needed to form a complete picture of the brain of chronic pain patients prescribed opioid analgesics.
Our study had some limitations, most notably the sample size of CLBP-op patients. Despite the modest number of CLBP-op patients, we were still able to observe the loss of NAc slow-5 PSD that we previously reported. 36 It also remains unclear whether the functional (i.e. loss of slow-4 PSD) and structural changes (i.e. loss of thalamic volume) observed in chronically medicated patients relate to chronic back pain or to the effects of long-term OA use. Future within subject OA treatment studies are needed to test the reproducibility of the results, and to incorporate a placebo (or active control) arm to corroborate or not the specificity of the results observed in this investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.G. has filed a patent application for the frequency analysis signature of chronic pain used in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from the National Institute on Drug Abuse (NIDA: 5K08DA037525) and from the Psychiatry Department at the Yale School of Medicine.