
Abstract
Background
The aim of this study was to assess whether the genotype of the serotonin transporter-linked polymorphic region (5-HTTLPR) in gastric cancer patients is associated with postoperative pain and pain threshold.
Methods
We conducted a prospective cohort study of 251 patients scheduled for gastrectomy from May to September 2019. All patients enrolled in the study were asked to complete the Hospital Anxiety and Depression Scale questionnaire. Heat pain threshold (HPT), cold pain threshold (CPT) and Pressure pain threshold (PPT) were measured for all participants one day prior to surgery. Blood samples were collected for genetic testing. All patients were connected to a patient-controlled intravenous analgesia (PCIA) pump at the end of the surgery. After exclusion of 15 patients, the postoperative conditions of 236 patients were recorded.
Results
Distribution of homozygous long (L/L), heterozygous (L/S), and homozygous short (S/S) 5-HTTLPR genotypes among participants were 26 (11.0%), 91 (38.6%), and 119 (50.4%), respectively. Heat pain threshold (P = 0.038) and Numerical rating scale (NRS) in the 1st postoperative 24 h (P = 0.026) were significantly different between long (L/L) and short (S/S) genotype carriers.
Conclusions
In patients with gastric cancer, heat pain stimulation is associated with 5-HTTLPR polymorphism, and postoperative pain may be related to 5-HTTLPR polymorphism.
Introduction
Management of postoperative pain in gastric cancer patients following gastrectomy is a major concern. Individuals vary in their sensitivity to specific harmful stimuli. Serotonin (5-hydroxytryptamine, 5-HT) has been identified as one of the neurotransmitters involved in the modulation of different types of pain. 1 The 5-HT transporter (5-HTT) has a high affinity for 5-HT and plays an important role in clearing extracellular 5-HT from the synaptic cleft, which is closely related to the amount, effect and duration of 5-HT receptors. 2
The gene encoding the human 5-HT transporter, SLC6A4, is located on chromosome 17 and contains a common polymorphism in the upstream transcriptional control region. This serotonin transporter-linked polymorphic region (5-HTTLPR) consists of a 44-bp insertion or deletion involving repeat elements 6 to 8 resulting in long (L) or short (S) alleles, forming three genotypes: L/L, L/S, S/S. The S allele variant has been associated with reduced transcription efficiency resulting in reductions in 5-HTT expression and 5-HT re-uptake.3–5
Postoperative pain mainly occurs within the first 24–72 hours after surgery. There is large inter-individual variation in the intensity of postoperative pain, and poor pain management may increase postoperative complications, which can influence rehabilitation. 6 Postoperative pain is reportedly influenced by a variety of factors including age, gender, depression and anxiety symptoms, pain threshold, type of procedure, range of gastrectomy, and response to analgesics.6–8
A recent study indicated that the preoperative pain response to heat stimulation may predict the intensity of postoperative pain in patients following arthroscopic knee surgery. 9 While one report has associated heat pain threshold and cold pain threshold with polymorphisms in the serotonin transporter gene, another study of healthy non-depressed individuals appears to show that variability in genotypes associated with the serotonin transporter does not play a major role in heat or pressure pain thresholds.10,11 Thus, the relationship between 5-HTTLPR polymorphisms, individual pain thresholds, and the intensity of postoperative pain is unclear and requires additional study. The aim of this prospective cohort study was to assess the association between 5-HTTLPR genotype and pain thresholds, anxiety and depression scores, and postoperative pain following gastrectomy in gastric cancer patients.
Methods
Participants
The study was approved by the Ethics Committee at the Peking University Cancer Hospital & Institute. The protocol number is LGH2019068. The trial was registered with the Chinese Clinical Trial Registry. The registration number is ChiCTR 1900023080. Written informed consent was obtained from all the participants.
Consecutive patients with gastric cancer, aged 18–80 years, with an American Society of Anesthesiologists (ASA) physical status of I to III, scheduled for gastrectomy at the Peking University Cancer Hospital from May 2019 to September 2019 were enrolled in the study. All patients were native Chinese. Exclusion criteria included: (1) repeated gastrectomy and conjoined surgery; (2) multiple primary malignant tumors; (3) current and chronic use of analgesics, psychotropic medications, hormones, or non-steroidal anti-inflammatories; (4) history of chronic pain, schizophrenia, epilepsy, dementia; (5) hepatorenal dysfunction; (6) unable to complete preoperative assessment due to dementia or language barrier; (7) Preoperative pain score >3 using Numerical Rating Scale (NRS) (ranging from 0 to 10, 0 = no pain, 10 = the worst imaginable pain). Of the 251 total patients enrolled in this study, 236 patients completed the trial, and 15 patients dropped out.
Preoperative data collection
Demographic details including gender, age, history of tobacco and alcohol use, body mass index (BMI), education level and the grade of ASA were collected. Patients were asked to fill out the Hospital Anxiety and Depression Scale questionnaire one day prior to surgery.12,13 The questionnaire consists of 14 items comprising two subscales for anxiety and depression, with 7 items per subscale. Scores for each subscale range from 0−21 indicating the level of anxiety and depression. Scores between 0 and 7 indicate a normal state of the patient, while scores between 8–10, 11–14 and 15–21 indicate mild, moderate and severe degrees of anxiety and depression, respectively.14,15 The anxiety and depression scores were recorded.
Measurement of pressure pain threshold (PPT)
The pain threshold of pressure pain stimuli was assessed by means of Von Frey hairs of different strengths (0.16, 0.4, 0.6, 1,1.4, 2, 4, 6, 8, 10, 15, 26 g; Aesthesio®, UgoBasile, Comerio, Italy). Subjects were in a seated position with their eyes closed to avoid visual feedback. Von Frey hairs were placed on the palmar skin of the forearm and bent slightly to apply pressure. Subjects had to give a clear verbal signal of “yes” or “no” to indicate whether or not the stimulus was painful. Each Von Frey hair was used three times with an interval of 10 seconds each time. PPT was defined as at least two of three stimuli causing pain, and the weight of Von Frey hair was recorded as the PPT.
Measurement of cold pain threshold (CPT)
A cold pain threshold test device (TAWA Q-18, Beijing, China) is a temperature-controlled water bath with a maximum temperature variance of ±0.5°C. Subjects placed their non-dominant hand in a cold water bath (5°C) with their fingers spread apart and without touching the bath wall. They were asked to keep their hands still in the water for as long as possible. CPT was defined as the time (seconds) when the subject began to feel pain, with 60 seconds set as the maximum to ensure safety.
Measurement of heat pain threshold (HPT)
A heat pain threshold test device (YOONING GH-100, Hangzhou, China) is a computer-controlled thermostat. Study subjects placed the thenar eminence of their non-dominant hand on a 10 × 7.5 cm metal plate, which was maintained at 47.5°C ± 0.1°C. Subjects were asked to keep their hands on the metal plate for as long as possible. HPT was defined as the time (seconds) when the subject could not keep their hands on the metal plate, with 60 seconds set as the maximum to ensure safety. Three consecutive tests with an interval of 10 seconds were conducted to determine the HPT. All pain threshold measurements were performed one day prior to surgery.
Anesthetic and analgesic techniques
All patients received general anesthesia induced by intravenous administration of 2 mg/kg of propofol and 0.4 μg/kg of sufentanil. Endotracheal intubation was facilitated by intravenous administration of 0.2 mg/kg of cisatracurium. Anesthesia was maintained by inhalation of sevoflurane and intravenous administration of remifentanil and propofol. Bispectral index values between 40 and 60 were maintained. Intravenous sufentanil (10 µg) was administered 30 minutes before the end of the surgery.
Following surgery, all patients were connected to a patient-controlled intravenous analgesia (PCIA) pump containing 100 ml of 3 μg/kg of sufentanil, 10 mg tropisetron, and 0.1 mg dexmedetomidine in 0.9% sodium chloride solution. The PCIA pump was programmed to deliver a loading dose of 2 mL, a 1 mL/h basal infusion, a 2 mL bolus dose with a lockout interval of 10 minutes, and a maximum dose of 13 mL/h. The type of procedure, operative duration, range of gastrectomy, blood loss, and transfusion volume were recorded.
Postoperative data collection
Postoperative pain was assessed using the Numerical Rating Scale (NRS) (ranging from 0 to 10, 0 = no pain, 10 = the worst imaginable pain). Patients received 0.1 μg/kg of sufentanil administered by an anesthesiologist to achieve an NRS score ≤3 prior to discharge from the post-anesthesia care unit. If the NRS score >3, 0.1 μg/kg sufentanil was given repeatedly in intervals of at least 15 minutes until the NRS score ≤3. Postoperative visits were performed by the same researcher. Additional analgesic drugs (primarily intravenous morphine) were given by surgery whenever the NRS score >3 after pressing the PCIA pump. NRS scores, sufentanil consumption of PCIA, and the use of additional analgesic drugs were recorded every 24 hours from the time the patient was discharged from the post-anesthesia care unit to the removal of the PICA pump.
Measurement of 5-HTTLPR genotyping
All patients were native Chinese. Whole blood samples were collected from study subjects prior to surgery. DNA was extracted and 5-HTTLPR genotype was determined by polymerase chain reaction (PCR) with the following primers: Forward: 5′-
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics (Version 22.0; IBM Corp., New York, USA) and Origin 2019 (Version 9.6; OriginLab, Massachusetts, USA). Continuous variables with normal distribution were presented as mean ± standard deviation (SD). Non-normal variables were presented as median (interquartile range), and enumeration data were presented as the percentage (%). One-Way ANOVA, Kruskal-Wallis H test and Pearson X2 test were used to compare the differences in normal distribution data, non-normal distributed data and categorical data, respectively, among the three groups. The independent sample t-test, Mann-Whitney U test and Pearson X2 test were performed for between-group analysis of normal distribution data, non-normal distributed data and categorical data respectively. A two-sided P value of <0.05 was the statistical significance level.
Multivariate linear regression analysis was used to identify risk factors correlated with postoperative pain, with NRS score in the first postoperative 24 hours as the dependent variable. Gender, age, BMI, tobacco use, alcohol use, education level, preoperative anxiety score, preoperative depression score, type of procedure, range of gastrectomy and 5-HTTLPR genotypes were included as independent variables in the model.
Multivariate binary logistic regression analysis was performed to identify variables associated with heat pain threshold. Heat pain threshold was the dependent variable, and values were separated into two categories by interquartile range. Gender, age, BMI, tobacco use, alcohol use, education level, preoperative anxiety score, preoperative depression score, and 5-HTTLPR genotypes were included as independent variables. The same multivariate binary logistic regression model was used to identify variables associated cold pain threshold, or pressure pain threshold.
Multivariate binary logistic regression analysis was performed to identify variables associated with preoperative anxiety score. Gender, age, BMI, tobacco use, alcohol use, education level and 5-HTTLPR genotypes were included in the model. The same multivariate binary logistic regression model was used to identify risk factors associated with preoperative depression score.
Results
3.1. Of the 251 patients enrolled in the study from May 2019 to September 2019, 5 were removed due to refusal to complete the Hospital Anxiety and Depression Scale questionnaire, 6 were removed due to refusal of preoperative pain threshold measurements, and 4 were removed due to change in type of procedure. In total, 236 patients were included in the statistical analysis (see Figure 1).
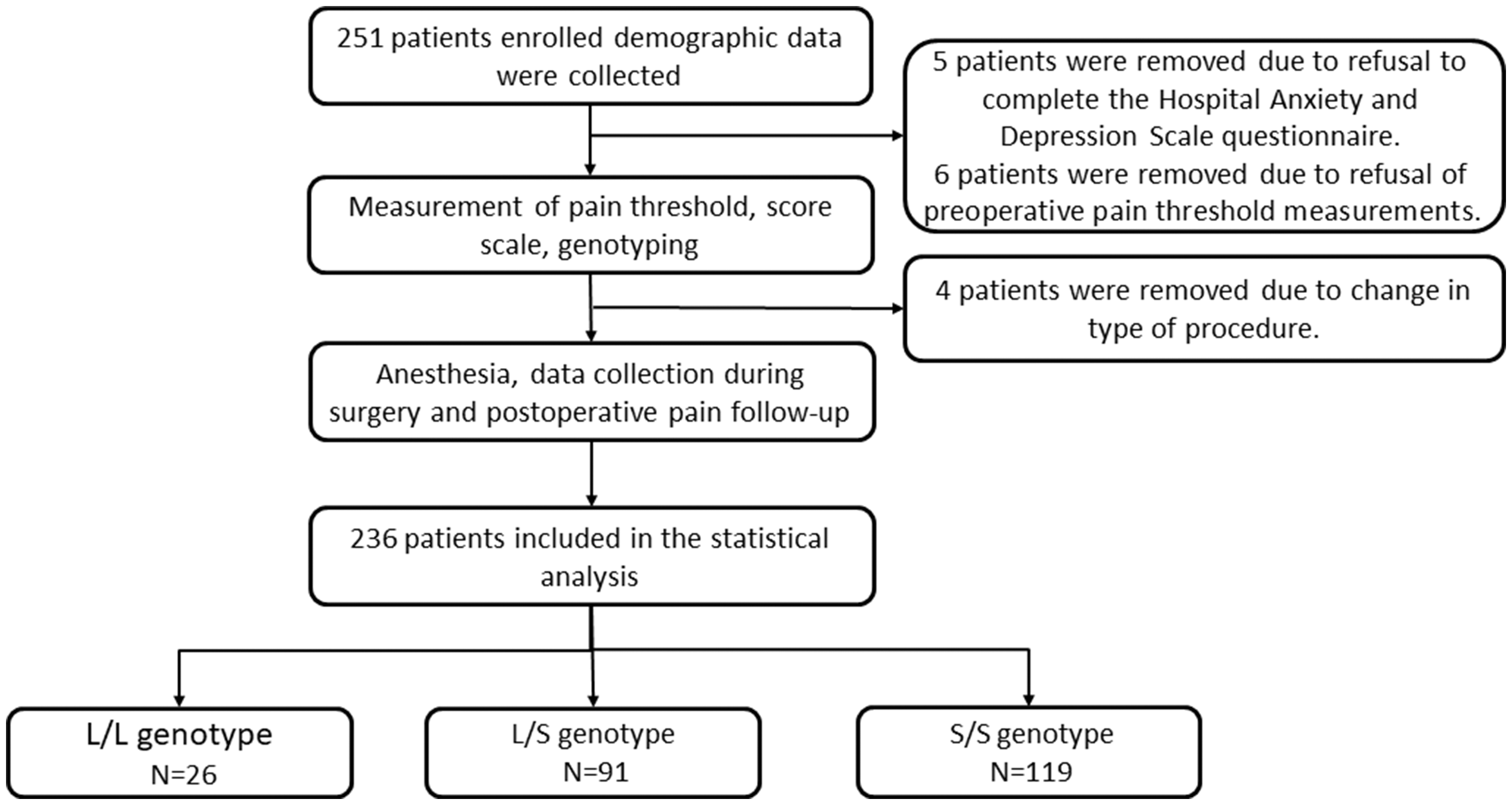
Flow chart of study.
3.2. 5-HTTLPR polymorphism in study participants consisted of homozygous long (L/L), heterozygous (L/S), and homozygous short (S/S) genotypes (Figure 2), with a distribution of 26 (11.0%), 91 (38.6%), and 119 (50.4%) respectively. The Sanger sequencing results were consistent with the L/L, L/S and S/S genotype sequences in the NCBI database. Patient characteristics, including demographic details, intraoperative data, and postoperative pain data are shown in Table 1. With the exception of type of procedure, no significant differences were observed in any parameters among carriers of (L/L), (L/S), and (S/S) genotypes.
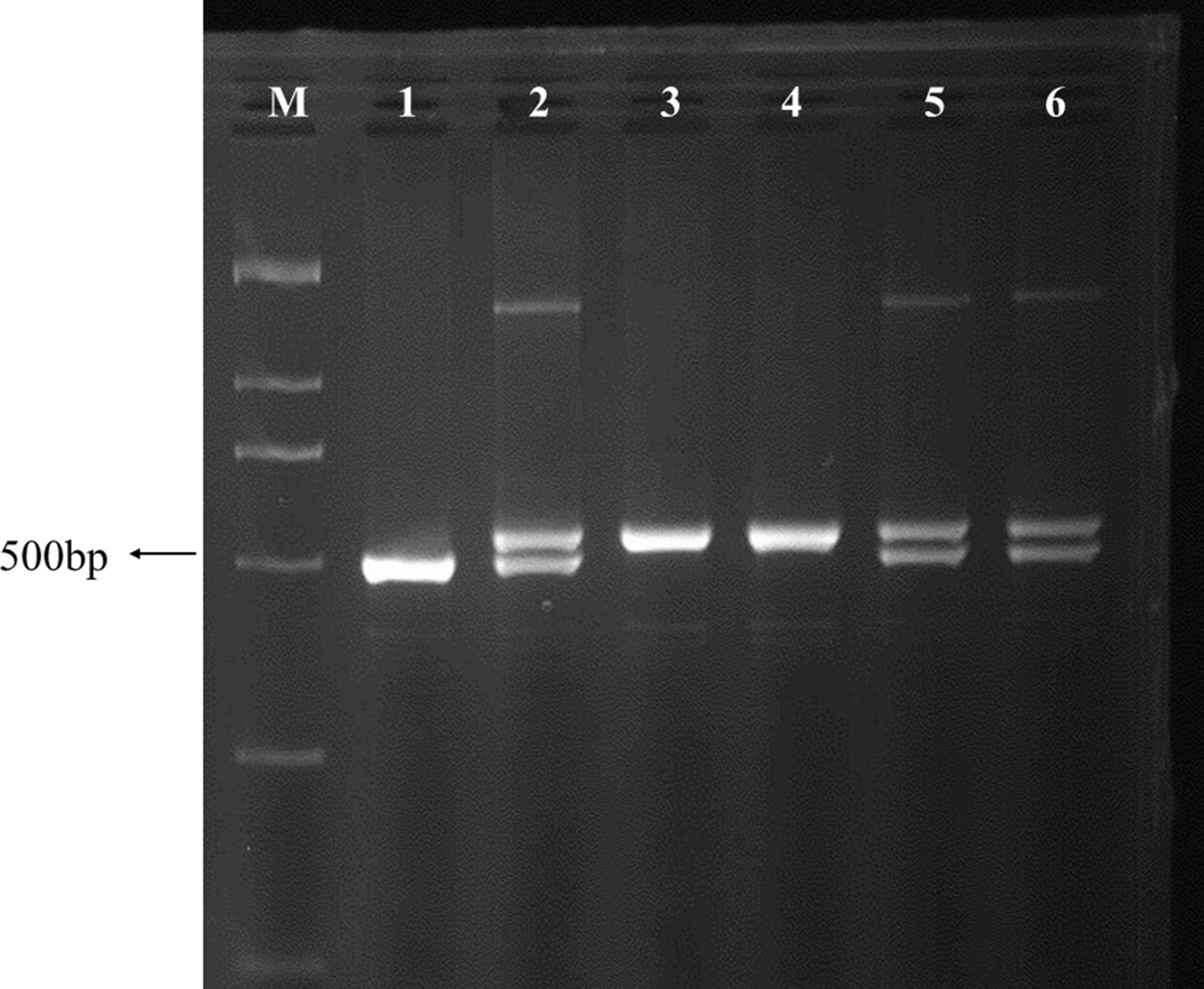
5-HTTLPR genotyping gel electrophoresis map.
Demographic details, intraoperative data, and postoperative pain data for overall.

Data presented as mean ± SD, median (interquartile range), or n (%). BMI: body mass index; ASA: American Society of Anesthesiologists.
aKruskal-Wallis H test.
bMann-Whitney U test.
cPearson X2 test.
dOne-Way ANOVA.
eThe independent sample t-test.
P1 Value: comparison between the three groups of carriers of (L/L), (L/S), and (S/S) genotypes. P2 Value: comparison between the two groups of carriers of (L/L), and (L/S) genotypes. P3 Value: comparison between the two groups of carriers of (L/L), and (S/S) genotypes.
3.2. Preoperative anxiety scores and preoperative depression scores are shown in Tables 2 and 3, respectively. A preoperative anxiety score higher than 8 was reported for 41 (17.4%) patients, and a preoperative depression score higher than 8 was reported for 24 (10.2%) patients.
Preoperative anxiety score.

Preoperative depression score.

3.4. As data associated with the L/L, L/S, and S/S genotypes was not statistically different, 3 we further compared the data associated with the L/L and S/S genotype carriers, and L/L and L/S genotype carriers separately. Compared to L/L genotype carriers, the S/S carriers showed a higher NRS score in the first postoperative 24 hours (Figure 3(a)). The preoperative heat pain threshold in S/S genotype carriers was lower than that of L/L and L/S genotype carriers (Figure 3(b)). There were no significant differences in pressure pain threshold (Figure 3(c)), cold pain threshold (Figure 3(d)), sufentanil consumption of PCIA in the first postoperative 24 hours (Figure 3(e)) between the L/L and L/S, or L/L and S/S genotypes (see Table 1 for details).

(a) NRS score in 1st postoperative 24 hours. (b) Heat pain threshold. (c) Pressure pain threshold. (d) Cold pain threshold. (e) Sufentanil consumption of PCIA in the first postoperative 24 hours.
3.5 The results of the linear regression analysis showed that age, tobacco use, 5-HTTLPR genotypes, and total gastrectomy were statistically associated with post-operative pain, as shown in Table 4.
Multivariate linear regression of risk factors for NRS score in the first postoperative 24 hours.

3.6 The results of multivariate binary logistic regression analysis indicated S/S genotype carriers (S/S vs. L/L, odds ratio (OR): 3.836, p = 0.044), high education level (odds ratio (OR): 1.147, p = 0.002), female (odds ratio (OR): 1.858, p = 0.078) and high preoperative anxiety score (odds ratio (OR): 1.082, p = 0.070) were associated with a lower heat pain threshold (see Table 5). No significant association was found between 5-HTTLPR genotypes and cold pain threshold or pressure pain threshold (see Table 5).
Multivariate logistic regression analysis of risk factors for heat pain threshold, cold pain threshold and pressure pain threshold.

3.7 There was no association between 5-HTTLPR genotypes and preoperative depression score or preoperative anxiety score (see Table 6).
Multivariate logistic regression of risk factors for preoperative anxiety score and preoperative depression score.

Discussion
The study results suggest that 5-HTTLPR polymorphisms are associated with heat pain threshold. Patients homozygous for the short 5-HTTLPR allele (S/S) were more sensitive to heat pain stimulation at 47.5°C, relative to patients homozygous for the long allele (L/L) (OR = 3.836). The regulation of 5-HT in pain involves descending 5-HT inhibitory and facilitation pathways depending on the type of pain and the type of receptor acting on it.17,18 Lindstedt et al. 10 reported an opposing result that S/S carriers with low expression of 5-HTT were less sensitive to heat pain and cold pain than L/L carriers. Heat pain threshold in that study was measured used a baseline setting of 32.0°C with a change rate of 1.5°C/s and a return rate of 8.0°C/s. In contrast, we used a constant temperature of 47.5°C and asked subjects to keep their hands on the metal plate for as long as possible. HPT was defined as the time (seconds) when the subject could not keep their hands on the metal plate. Other studies have also found that 5-HTTLPR genotype does not affect the sensitivity to thermal pain, including heat pain and cold pain, among healthy individuals and patients with fibromyalgia syndrome.11,19 However, the enrolled population and the methods of measuring pain thresholds were diverse in these studies, particularly the temperature and methodology used to determine heat pain thresholds.10,11,13,16,19 The values obtained for heat pain threshold may therefore be highly variable between studies and are likely a source of inconsistent results.10,11,19
We found that the heat pain threshold, but not pressure pain or cold pain threshold, was associated with 5-HTTLPR polymorphism. Studies in mice have shown that heat, cold and mechanical stimulation activate thermo- and mechano- specific neurons diversely. Therefore, different types of pain caused by heat, cold and pressure may transmit to different thalamus functional areas and cortical circuits. 20 Other polymorphisms within the 5-HTTLPR loci may further impact pain thresholds. A single nucleotide polymorphism (rs25531) leading to an A-allele or G-allele has been associated with the transcriptional efficacy of 5-HTTLPR. 21 Pain sensation is affected by multiple genes as well as gene interactions. Genetic variations of the serotonin transporter and different subtypes of serotonin receptors have also been related to the regulation of pain.11,22 Thus, further research is needed to indicate the possible mechanism for the differential effect of the 5-HTTLPR polymorphism in the SLC6A4 gene on heat pain, cold pain and pressure pain thresholds.
In the present study, carriers with the 5-HTTLPR S/S genotype had significantly higher NRS scores in the first postoperative 24 hours relative to patients with the L/L genotype. 5-HTTLPR polymorphisms were statistically associated with post-operative pain. Thus, we conclude that postoperative pain may be related to 5-HTTLPR polymorphism. Although the median NRS score of L/L and S/S genotype carriers differs by 1 point, and neither exceeds 3 points, it is worth noting that all the patients in this study received additional analgesic drugs when their NRS score was above 3. Both sufentanil consumption of PCIA and the use of additional analgesic drugs in the first postoperative 24 hours were increased in S/S genotype carriers, although the data was not statistically significant, suggesting that S/S genotype carriers may experience more postoperative pain.
A search of the PubMed database for the key words “serotonin transporter polymorphism, postoperative pain”, failed to find strong clinical results that support or conflict with our conclusions. 5-HT dysfunction is considered a common mechanism of emotion and pain pathology. 12 The S allele variant has been associated with reduced transcription efficiency resulting in reduced 5-HTT expression and 5-HT reuptake. 23 This may be the reason that 5-HTTLPR polymorphism affects pain.
5-HTTLPR polymorphism is the result of a 44 base pair insertion/deletion resulting in a long (L) and short (S) allele and three genotypes- homozygous long (L/L), heterozygous, (L/S), and homozygous short (S/S). The distribution of these genotypes among the 236 gastric cancer patients in our study were 11.0% (L/L), 38.6% (L/S), and 50.4% (S/S). Previous reports indicate that the frequency of the L/L genotype is 24%–38% and 10–28% in European and Chinese populations, respectively.24–26 While these frequencies are quite variable among different populations, our results are consistent with these reports, as all study participants were native Chinese.
Preliminary findings have suggested that 5-HTTLPR variants may influence depressive symptoms and stress conditions among patients with CHD, chronic pain, or papillary thyroid carcinoma.27–29 In the present study, neither preoperative anxiety nor depression score were associated with 5-HTTLPR polymorphism. Only 24 (10.2%) patients had a preoperative depression score higher than 8, with the highest preoperative depression score being 13. However, patients that required psychotropic medication for the treatment mental health conditions were excluded from the present study and may explain these discrepancies.
There are two potential limitations to this study. First, some patients (15) pressed the PCIA pump more than 24 times during the first postoperative 48 hours and depleted the 100 ml PCIA solution. These patients did not continue to use the PCIA pump and so the sufentanil consumption during the 2nd postoperative 24 hour may not be accurate. Therefore, we only compared data from the first postoperative 24 hours. Second, patients in this study underwent either open procedure or laparoscopic elective gastrectomy. Our results indicate a significant difference in the type of procedure between the L/L, L/S and S/S genotypes, but no difference when comparing only the L/L and S/S groups. The relationship between type of surgical procedure and postoperative pain is not clear.30,31 Our sample size is insufficient for propensity score matching analysis to reduce bias in the study.
Conclusion
In summary, our study provides evidence that 5-HTTLPR polymorphism is associated with heat pain stimulation and may be related to postoperative pain in gastric cancer patients.
Footnotes
Authors' Contributions
LY and SL conducted the study, analyzed the data, and wrote the manuscript. JW, HWS, CXY helped conduct the study. HYT helped design the study, conducted the study and co-wrote the manuscript. All authors read and approved the final manuscript.
Ethics Approval and Consent to Participate
We declare that this study has obtained the report of ethics board approval and written informed consent was obtained from each participant before surgery. The study was approved by the ethics committee of Peking University Cancer Hospital & Institute, Beijing, China in April 2019. The protocol number is 2019YJZ22.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Peking University Medicine Seed Fund for Interdisciplinary Research (BMU2020MX028) (the Fundamental Research Funds for the Central Universities). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.