
Abstract
Vortioxetine is a multimodal antidepressant that potently antagonizes 5-HT3 serotonin receptors, inhibits the high-affinity serotonin transporter, activates 5-HT1A and 5-HT1B receptors, and antagonizes 5-HT1D and 5-HT7 receptors. 5-HT3 receptors largely mediate the hyperalgesic activity of serotonin that occurs in response to nerve injury. Activation of 5-HT3 receptors contributes to explain why selective serotonin reuptake inhibitors, such as fluoxetine, are not indicated in the treatment of neuropathic pain. Here, we studied the analgesic action of vortioxetine in the chronic constriction injury model of neuropathic pain in mice. Vortioxetine was injected once a day for 27 days at doses (10 mg/kg, intraperitoneally) that determine >90% 5-HT3 receptor occupancy in the central nervous system. The action of vortioxetine was compared to the action of equal doses of the serotonin-noradrenaline reuptake inhibitor, venlafaxine (one of the gold standard drugs in the treatment of neuropathic pain), and fluoxetine. Vortioxetine caused a robust analgesia in chronic constriction injury mice, and its effect was identical to that produced by venlafaxine. In contrast, fluoxetine was inactive in chronic constriction injury mice. Vortioxetine enhanced mechanical pain thresholds in chronic constriction injury mice without changing motor activity, as assessed by the open-field and horizontal bar tests. None of the three antidepressants caused analgesia in the complete Freund’s adjuvant model of chronic inflammatory pain. These findings raise the attractive possibility that vortioxetine can be effective in the treatment of neuropathic pain, particularly in patients with comorbid depression and cognitive dysfunction.
Introduction
A large body of evidence suggests that serotoninergic pathways descending from the rostral ventromedial medulla (RVM) to the spinal cord are involved in the top-down inhibitory control of pain (reviewed in Ossipov et al. 1 and Zhuo 2 ). However, the effect of serotonin on pain modulation in the spinal cord can be either inhibitory or facilitatory depending on the receptor subtypes that are preferentially activated. Pharmacological studies have shown that serotonin-induced analgesia is mediated by 5HT7 receptors, whereas hyperalgesia is mediated by 5HT3 receptors.3–6 While inhibition of nociceptive transmission by serotonin may prevail in conditions of acute pain, serotonin-induced hyperalgesia contributes to the development of chronic pain after tissue or nerve injury.6–9 Accordingly, shRNA interference-induced knockdown of the serotonin-synthesizing enzyme, type-2 tryptophan hydroxylase, in the RVM causes analgesia in the spinal nerve ligation (SNL) model of neuropathic pain in rats. 10 An elegant work shed light into the epigenetic mechanism underlying the hyperalgesic activity of serotonin in response to nerve injury. SNL in rats caused a downregulation of the gamma-aminobutyric acid (GABA)-synthesizing enzyme, glutamate decarboxylase-65, in the raphe magnus as a result of a reduced H3-histone acetylation at the gad65 gene promoter. 11 Disinhibition of serotoninergic neurons might drive maladaptive changes in serotonin descending pathways resulting into nociceptive sensitization and chronic pain. These findings contribute to explain why pure serotoninergic drugs, for example, selective serotonin reuptake inhibitors (SSRIs), are ineffective in the treatment of neuropathic pain. In contrast, drugs that also inhibit noradrenaline uptake, such as venlafaxine, duloxetine, and amitriptyline, show level A rating for efficacy in the treatment of neuropathic pain. 12
We reasoned that activation of 5-HT3 receptors could overcome a potential analgesic activity of serotonin in neuropathic pain. This gave us the impetus to examine the action of vortioxetine in a preclinical model of neuropathic pain. Vortioxetine is a new multimodal antidepressant drug, which inhibits the high-affinity serotonin transporter, and also interacts with different types of serotonin receptors. In particular, vortioxetine behaves as a full agonist of 5-HT1A receptors; a partial agonist of 5-HT1B receptors; and an antagonist of 5-HT1B, 5-HT3, and 5-HT7 receptors. Vortioxetine displays the highest affinity and central nervous system receptor occupancy for 5-HT3 receptors and is nearly as potent as the prototypical 5-HT3 receptor antagonist, ondansetron, in inhibiting the 5-HT3-dependent Bezold–Jarisch reflex.13–15 Owing to these characteristics, vortioxetine is clinically effective in improving cognitive dysfunction associated with unipolar depression (see “Discussion” and “References” therein). We hypothesized that vortioxetine could be beneficial in neuropathic pain by enhancing serotoninergic transmission and potently inhibiting 5-HT3 receptors at the same time. We tested this hypothesis by comparatively evaluating the effect of a chronic treatment with vortioxetine, the serotonin-noradrenaline reuptake inhibitor (SNRI), venlafaxine, and the SSRI, fluoxetine, in mouse models of chronic inflammatory and neuropathic pain.
Materials and methods
Animals
The experiments were carried out in two-month-old male CD1 mice (Charles River, Italy). Animals were housed three to four per cage in a controlled temperature room (21°C–23°C, humidity 40%–50%) maintained on a 12-h light/dark cycle (light on 07.00 am); food (Standard Diet Charles River 4RF21, Italy) and water were available ad libitum. All efforts were made to minimize the number of animals used and to alleviate their discomfort. All experimental procedures were performed in conformity with the European Union Directive (2010/63/EU) on the protection of animals used for scientific purpose and were approved by the Italian Ministry of Health (DDL 26/2014 and previous legislation; protocol number n° 882/2017-PR).
Drugs
Vortioxetine was provided by H. Lundback A/S (Denmark). Fluoxetine and venlafaxine were purchased from LKT Laboratories, Inc. (Saint Paul, MN). All drugs were dissolved in 5% of 2-hydroxypropyl-β-cyclodextrin and administered intraperitoneally (i.p.) at the dose of 10 mg/kg (50 µl/10 g, body weight). Control animals received the vehicle alone (50 µl/10 g, body weight). The fixed dose of 10 mg/kg for the three drugs was selected on the basis of previous studies using fluoxetine and/or venlafaxine in models of neuropathic pain.16–20 No studies with vortioxetine in pain models had been performed before. The dose of 10 mg/kg of vortioxetine is used in most of the studies on cognitive function and depressive-like behavior.21–24
Induction of chronic inflammatory pain
Tissue inflammation was induced by a single subcutaneous (s.c.) injection of 20 µl of complete Freund’s adjuvant (CFA; Sigma-Aldrich; 1 mg/ml) in the dorsal surface of the right hind paw. Control mice (n = 7) were injected s.c. with saline in the right hind paw. Three hours after CFA injection, mice were treated once a day (always at 2.00 p.m.) for 12 days with vortioxetine (n = 8), fluoxetine (n = 9), venlafaxine (n = 8), or their vehicle (n = 7). Tactile allodynia was assessed before the injection of CFA (day 0) to determine baseline thresholds and then 1, 3, 5, 7, 10, and 12 days after CFA (and drug) injections.
Induction of chronic neuropathic pain
Mononeuropathy was induced by the chronic constriction injury (CCI) of the sciatic nerve in mice 25 anesthetized by i.p. injection of tiletamine–zolazepam + xylazine (30 mg/kg + 10 mg/kg). The sciatic nerve was exposed, and three loose ligatures with 4-0 silk suture thread were made around the nerve with a 1.0- to 1.5-mm interval between each of them. In sham-operated mice, an identical dissection was performed on the same side, except that the sciatic nerve was not tied. Fourteen days after CCI (day 0), mice were daily injected with vortioxetine (n = 10), fluoxetine (n = 9), venlafaxine (n = 9), or vehicle (n = 8) for 28 days. All treatments were performed at 2.00 p.m. Tactile allodynia was measured prior to CCI to determine baseline thresholds, in the morning (10.00 a.m.) of the starting day of drug treatments, and then at days 1, 3, 5, 7, 12, 14, 16, 21, and 27 of antidepressant treatments.
Assessment of tactile allodynia
Tactile allodynia was assessed in the hind paws using calibrated von Frey filaments (two Biological Instruments, Italy) and the up-down method previously described by Chaplan et al. 26 Animals were placed in individual Plexiglas boxes on a raised metal mesh surface and allowed to acclimatize for 30 min before the test. Testing was initiated with a medium-sized filament, which was applied for 7 s to the plantar area (plantar territory of the sural nerve) until the filament bent slightly. If the mouse withdrew or lifted the paw, the response was considered positive, and a one size smaller filament was tried. Conversely, if no response was observed, a one size larger filament was tried. The protocol was repeated until five changes in behavior had been observed. The 50% paw withdrawal threshold (PWT) was determined according to the following equation: Xf + kD, where Xf is the value of the last von Frey filament used, k is the Dixon value for the positive/negative pattern, and D is the logarithmic difference between stimuli. 27 Tests were performed in the morning, before drug injections, thus reflecting the analgesic action of the previous treatment day.
Assessment of locomotor activity and catalepsy
Locomotor activity was assessed in an open-field apparatus in all mice used for the study of neuropathic pain (sham-operated mice and CCI mice treated with vehicle, fluoxetine, vortioxetine, and venlafaxine) at day 18 after the onset of drug treatments (between day 16 and day 21 of pain assessment). The open-field apparatus was a Plexiglas-squared arena (40 × 40 cm) with gray walls (40 cm high) and an open roof, located in a sound-attenuated and dimly illuminated room. Animals were individually placed in the center of the arena and allowed to explore for 10 min. The arena was cleaned with 50% ethanol solution before each test. The frequency of line crossing was used to assess total general motor activity. For this purpose, the floor was divided in nine virtual quadrants of equal size. A line crossing was considered when the animal entered another virtual quadrant with all four paws. Behavioral data were acquired and analyzed using an automated video-tracking system (Any-Maze, Stoelting, Wood Dale, IL).
Catalepsy was assessed in the same mice at day 19 after the onset of treatments by the horizontal bar test in which the fore paws of mice were placed on a 15-cm-long bar placed at 4.5 cm above the surface level. The center of the bar was marked to assure identical placement of the mice during the test. 28 The time in which the fore paws remained in the horizontal bar was recorded by an observer who was unaware of the treatments with a cutoff time of 60 s. If a mouse did not stay in the position after four attempts, the cataleptic response time was registered as 0 s.
Statistical analysis
Statistical analysis of the PWT was performed by two-way analysis of variance (ANOVA) for repeated measures followed by Bonferroni post hoc comparisons, where appropriate. Statistical significance was set at p < 0.05.
Results
No analgesic effect of the selected antidepressants in the CFA model of chronic inflammatory pain
A significant reduction in tactile withdrawal threshold was observed in the ipsilateral hind paw one day after unilateral CFA injection. In CFA mice chronically treated with vehicle, tactile allodynia remained unaltered in the first five days and then gradually decreased until the last day of pain assessment (12 days following CFA injection). None of the selected antidepressants, including vortioxetine, caused changes in tactile sensitivity in the hind paw ipsilateral to CFA injection (Figure 1(a)). No changes in paw withdrawal were found in the contralateral hind paw regardless of drug treatments (Figure 1(b)).
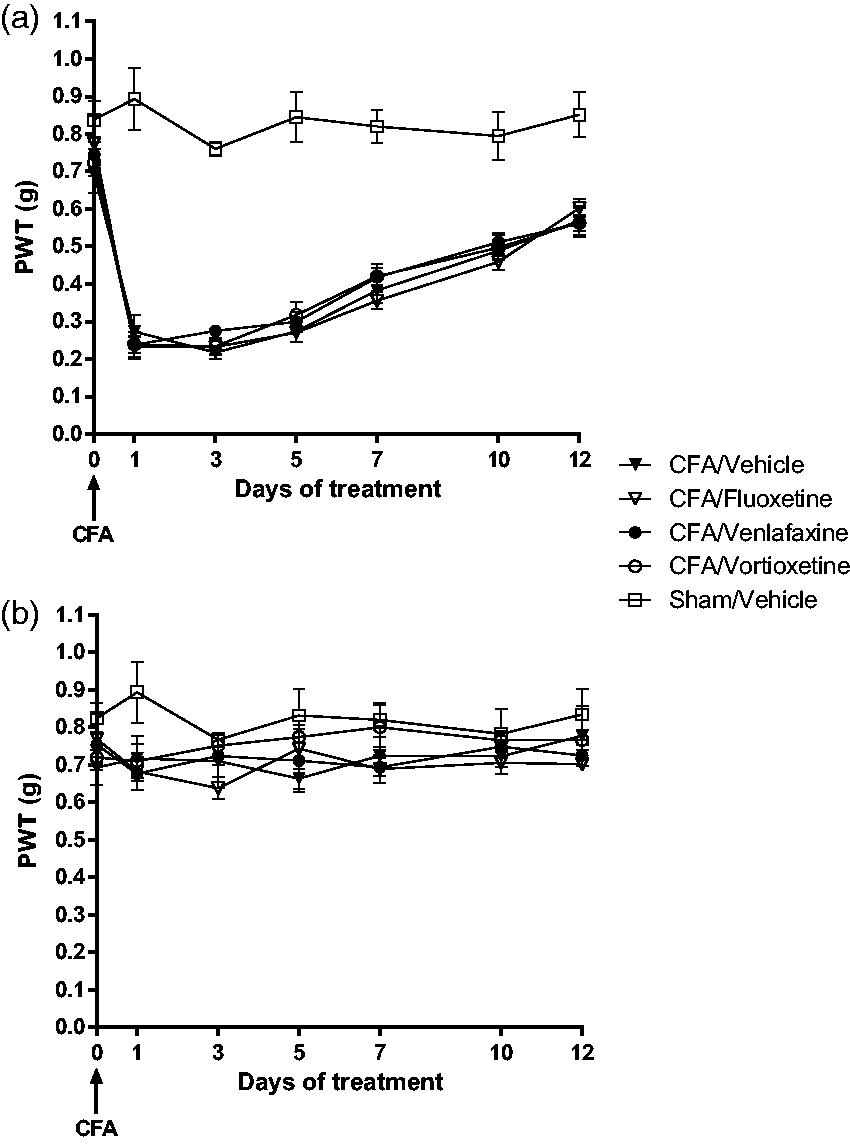
Chronic treatment with fluoxetine, venlafaxine, and vortioxetine did not cause analgesia in the CFA mouse model of inflammatory pain. Mice were injected with CFA in the right hind paw. Control mice received an equal volume of saline in the hind paw. In CFA mice, systemic treatments with fluoxetine (10 mg/kg), venlafaxine (10 mg/kg), or vortioxetine (10 mg/kg) started 3 h after CFA injection. All drugs were injected intraperitoneally once a day for 12 days. Tactile pain thresholds were assessed at days 1, 3, 5, 7, 10, and 12 after CFA injection. Pain threshold measured in the ipsilateral hind paw is shown in panel (a), where values are means ± SEM of 7 to 9 mice per group. In order to assess the inflammatory effect of CFA injection, we first compared each of the CFA-injected groups with the group of sham-operated mice treated with vehicle. Two-way ANOVA for repeated measures (treatment × days) indicated that all CFA-injected groups were statistically different from sham (CFA/vehicle vs. sham/vehicle: F1,98 = 79.76, p ≤ 0.05; CFA/fluoxetine vs. sham/vehicle: F1,103 = 16.36, p ≤ 0.05; CFA/venlafaxine vs. sham/vehicle: F1,97 = 12.39, p ≤ 0.05; CFA/vortioxetine vs. sham/vehicle: F1,97 = 11.99, p ≤ 0.05). Then, we assessed the treatment effect comparing all CFA-injected groups without the group of sham-operated mice treated with vehicle. Two-way ANOVA for repeated measure indicated a significant effect of the day (F3,199 = 98.29, p ≤ 0.05) but no effect of antidepressant treatment (F3,199 = 1.33, p = 0.3). Pain threshold in the contralateral hind paw is shown in panel (b). CFA: complete Freund’s adjuvant; PWT: paw withdrawal threshold.
Chronic treatment with vortioxetine caused analgesia in the CCI model of neuropathic pain
Unilateral CCI of the sciatic nerve caused the expected reduction in mechanical pain thresholds after 14 days with respect to basal thresholds and to thresholds detected in sham-operated mice. Daily treatments with fluoxetine, venlafaxine, vortioxetine (all at 10 mg/kg, i.p.), or their vehicle started at day 14 after CCI immediately after pain assessment (indicated as time 0 in Figure 2(a) and (b)). In CCI mice treated with vehicle, the reduction in tactile pain thresholds in the ipsilateral hind paw remained unchanged for the whole duration of the treatment (27 days, corresponding to 41 days after CCI) (Figure 2(a)). Fluoxetine treatment in CCI mice had no effect on tactile allodynia, and PWT values were indistinguishable from those detected in mice treated with vehicle (Figure 2(a)). In contrast, treatments with either venlafaxine or vortioxetine caused a robust analgesia that was initially observed at day 7 and became substantial at day 12 of the treatment (Figure 2(a)). There was no difference between the analgesic effect of vortioxetine and the effect of the venlafaxine (Figure 2(a)). No changes in mechanical thresholds were found in the hind paw contralateral to CCI regardless of drug treatments (Figure 2(b)).
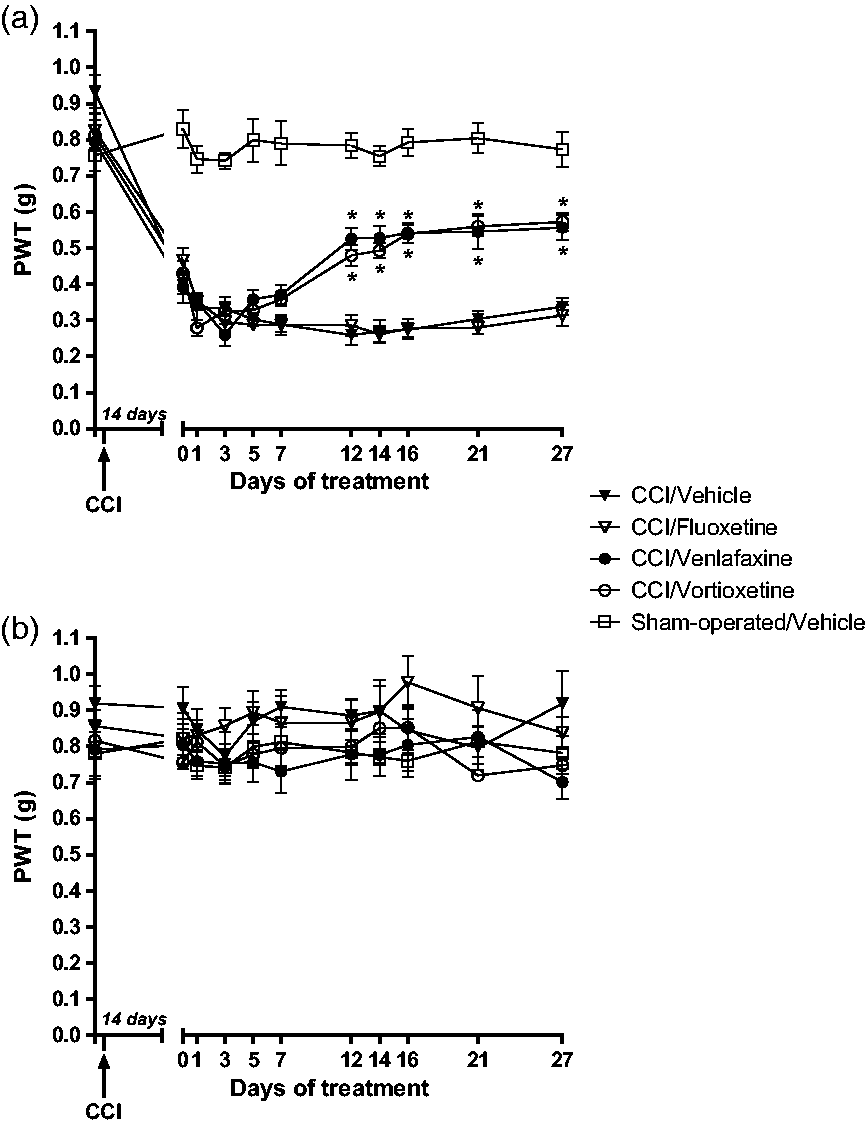
Analgesic effects of vortioxetine and venlafaxine in the CCI model of neuropathic pain. Mice were subjected to CCI of the right sciatic nerve and treated, after 14 days, with fluoxetine (10 mg/kg), venlafaxine (10 mg/kg), vortioxetine (10 mg/kg), or their vehicle. Treatments were performed intraperitoneally once a day for 27 days (i.e., up to 41 days after CCI). Tactile pain thresholds in the ipsilateral hind paw are shown in panel (a) where values are means ± SEM of 8 to 10 mice per group. In order to assess the induction of neuropathic pain after CCI, we first compared all CCI groups with the group of sham-operated mice treated with vehicle. Two-way ANOVA for repeated measures (treatment × days) indicated that each of the CCI groups was statistically different from the group sham-operated mice treated with vehicle (CFA/vehicle vs. sham/vehicle: F1,180 = 255.25, p ≤ 0.05; CFA/fluoxetine vs. sham/vehicle: F1,180 = 264.59, p ≤ 0.05; CFA/venlafaxine vs. sham/vehicle: F1,180 = 98.16, p ≤ 0.05; CFA/vortioxetine vs. sham/vehicle: F1,190 = 156.51, p ≤ 0.05). Then, we assessed the treatment effect comparing all CCI groups without the group of sham-operated mice. Two-way ANOVA for repeated measure indicated a significant effect of the day (F3,370 = 18.17, p ≤ 0.05), a significant effect of the treatment (F3,370 = 23.97, p ≤ 0.05) and an interaction between the two factors (F3,370 = 10.61, p ≤ 0.05). Values obtained in CCI mice treated with vortioxetine or venlafaxine were significantly different with respect to values obtained in CCI mice treated with vehicle or fluoxetine from day 12 of treatment (*p < 0.05, Bonferroni’s post hoc test). Mechanical pain thresholds in the contralateral hind paw are shown in panel (b). CCI: chronic constriction injury; PWT: paw withdrawal threshold.
Vortioxetine and the other antidepressants had no effect on spontaneous locomotor activity and did not induce catalepsy in sham-operated and CCI mice
To exclude that changes in motor activity could influence the evaluation of pain thresholds, we measured spontaneous locomotor activity in sham-operated mice, and in CCI mice treated with vehicle, fluoxetine, venlafaxine, or vortioxetine. Mice were evaluated in an open-field apparatus at day 18 after the onset of drug treatments (pain thresholds were measured at day 16 and day 21). Measurements of total distance traveled and number of line crossing showed that CCI itself (mice treated with vehicle) and drug treatments did not change spontaneous locomotor activity, as compared to sham-operated mice (Figure 3(a) and (b)). We also evaluated the ability of mice to remove their fore paws from a horizontal bar (a test for the assessment of catalepsy) at day 19 after the onset of drug treatments. All mice (sham-operated mice or CCI mice treated with vehicle, fluoxetine, venlafaxine, or vortioxetine) showed no cataleptic behavior and immediately removed both fore paws from the horizontal bar (not shown).
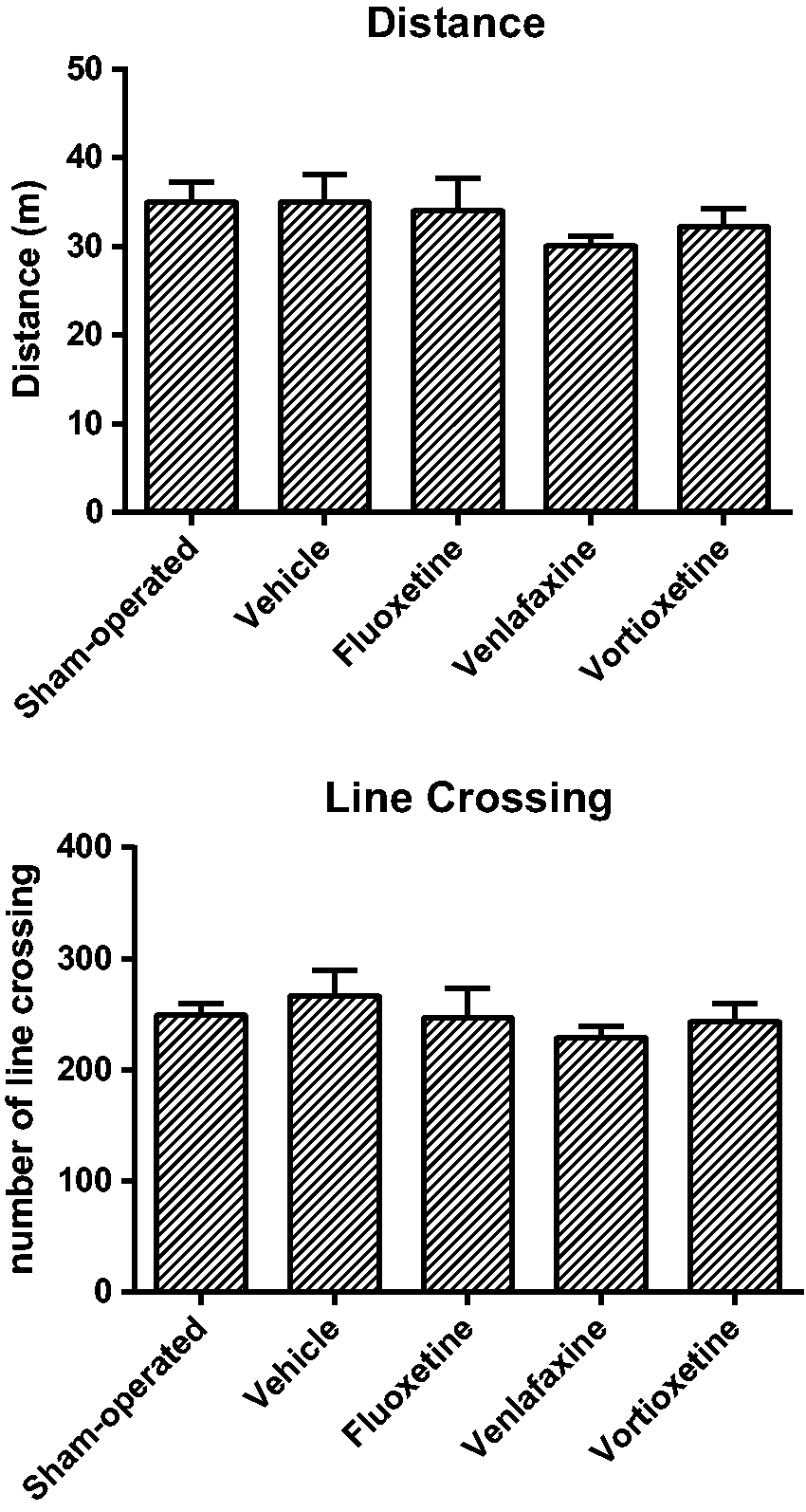
Antidepressant treatment did not cause changes in spontaneous locomotor activity in mice subjected to CCI of the sciatic nerve. Spontaneous locomotor activity was assessed in mice subjected to CCI of the right sciatic nerve treated with antidepressants or their vehicle (see legend of Figure 2) and in sham-operated mice at day 32 after surgery (day 18 of treatments in CCI mice). Distance traveled (in meters) (a) and numbers of line crossing (b) were determined in an open-field apparatus (10 min of total observation). Values are means ± SEM of 8 to 10 mice per group.
Discussion
Full functional recovery in patients affected by unipolar depression relies on the control of residual symptoms and comorbid disorders. Cognitive dysfunction, which occurs in a significant proportion of depressed patients, has a negative prognostic value and is refractory to the majority of antidepressant medications. Depressed patients with cognitive dysfunction, characterized by impairment in executive functions, speed of processing, and working and episodic memory, often relapse in spite of continuous medication, and this leads to a marked reduction in the quality of life.29–32 The multimodal antidepressant, vortioxetine, has shown a remarkable efficacy in improving cognitive dysfunction associated with unipolar depression.33–40 In a network meta-analysis of 12 clinical trials made uniform by the use of the digit symbol substitution test as a measure of cognitive function, vortioxetine has shown a large superiority with respect to all other antidepressants drugs such as SNRIs, SSRIs, monoamine oxidase inhibitors, and tricyclic antidepressants. 41 This unique property of vortioxetine largely depends on its ability to potently antagonize 5-HT3 receptors in the prefrontal cortex and hippocampus, a mechanism that restrains the inhibitory activity of selected populations of GABAergic interneurons on pyramidal cells.42,43 Despite this remarkable feature, vortioxetine is not yet considered as a first-choice drug in patients with depression associated with comorbid neuropathic pain because the action of vortioxetine on pain transmission is still unknown. In contrast, antidepressants that inhibit both serotonin and noradrenaline reuptake, such as duloxetine, venlafaxine, amitriptyline, are gold standard drugs in the treatment of neuropathic pain. 12 Using an established mouse model of neuropathic pain, we have shown here for the first time that vortioxetine displays a strong analgesic activity, which is indistinguishable from the activity exhibited by venlafaxine. To our knowledge, this is the first example of a pure serotoninergic drug showing analgesic activity in a model of neuropathic pain. In contrast, chronic treatment with the SSRI fluoxetine did not cause analgesia in the CCI model of neuropathic pain (see Hu et al. 44 for similar data obtained in rats).
As outlined earlier, the serotonergic pathway descending from the lower brainstem to the dorsal horns of the spinal cord becomes hyperalgesic under conditions of neuropathic pain because of epigenetic processes developing in the raphe magnus and other mechanisms (see “Introduction” and “References” therein). Serotonin-induced hyperalgesia is mediated by the activation of 5-HT3 receptors, which counteract the analgesic activity of 5-HT7 receptors (reviewed in Ossipov et al.
1
). Vortioxetine acts as a multimodal serotonergic antidepressant, behaving as an inhibitor of the high-affinity serotonin transporter, a full agonist of 5-HT1A receptors, a partial agonist of 5-HT1B receptors, and an antagonist of 5-HT1D, 5-HT3, and 5-HT7 receptors (reviewed in Sanchez et al.
39
). Measurements of target occupancy in mice showed that 10 mg/kg of vortioxetine (the dose used in this study) nearly saturates 5-HT3 receptors and the serotonin transporter but recruits only 20% to 30% of 5-HT7 receptors.
45
Thus, under conditions of serotonergic hyperactivity, as occurs in neuropathic pain, vortioxetine will efficiently antagonize 5-HT3 receptors leaving the vast majority of 5-HT7 receptors unoccupied and, therefore, available for activation by serotonin. On the basis of these findings, we could predict that SSRIs could be effective as analgesic drugs in neuropathic pain if combined with a potent 5-HT3 receptor antagonist. This interesting hypothesis warrants further investigation.
Because antidepressant drugs have intrinsic anti-inflammatory effects, 46 we cannot exclude that vortioxetine causes analgesia by restraining neuroinflammation associated with neuropathic pain. Along this line, increasing evidence suggests that pain-associated neuroinflammation is gender-dependent, with a greater involvement of microglia in males and T lymphocytes in females (reviewed by Coraggio et al. 47 ). Sex steroids are known to affect neuroinflammation by modulating microglial responses to injuries.48–50 Here, we examined the analgesic activity of vortioxetine only in males to avoid heterogeneity caused by the ovarian cycle. It will be interesting to extend the study to nonsynchronized, synchronized, and ovariectomized female mice (with/without hormonal replacement therapy) to gain insights into the influence of gender and sex steroids on the analgesic activity of vortioxetine in models of neuropathic pain.
None of the antidepressants used in the present study caused analgesia in the CFA model of chronic inflammatory pain. In a previous study, fluoxetine at the dose of 10 mg/kg was found to enhance mechanical pain thresholds in CFA-injected rats. 51 To our knowledge, fluoxetine has never been tested in the CFA model in mice, except in one study in which fluoxetine had no effect on CFA-induced edema, but pain thresholds were not determined. 52 High doses of venlafaxine (50 and 100 mg/kg) were reported to enhance mechanical pain thresholds after intraplantar injection of carrageenan in rats, 53 but the drug has never been tested before in CFA mice. The lack of effects of venlafaxine and vortioxetine on pain thresholds in CFA mice supports the hypothesis that the molecular and transsynaptic mechanisms underlying nociceptive sensitization in inflammatory and neuropathic pain are different. We have shown recently that a seven-day treatment with the antidepressant, amitriptyline, is effective in causing analgesia in the CFA model of inflammatory pain in mice. 54 Although amitriptyline shares with venlafaxine the ability to inhibit both serotonin and noradrenaline reuptake, other mechanisms, such as inhibition of neurotransmitter receptors or voltage-sensitive sodium channels, may contribute to the analgesic effect of amitriptyline and account for the different actions of amitriptyline and venlafaxine in the CFA model of pain.
Our findings suggest that vortioxetine may enrich the therapeutic armamentarium in patients affected by major depression associated with comorbid neuropathic pain. If confirmed in clinical studies, the analgesic activity of vortioxetine will be particularly helpful for patients with cognitive dysfunction in which the drug shows a greater efficacy with respect to all other classes of antidepressants. Another advantage is the good profile of safety and tolerability of vortioxetine, which does not causes significant increases in body weight and sexual dysfunction (as opposed to SSRIs) or cardiovascular adverse effects (as opposed to SNRIs).55–57 The analgesic effect of vortioxetine in the CCI model paves the way for clinical studies in which vortioxetine should be compared to gold standard antidepressants in the treatment of neuropathic pain.
Footnotes
Authors’ Contribution
ARZ performed pain experiments and contributed to write the manuscript; DM, FDM, and RL performed pain experiments; SA performed experiments on motor behavior; and PC and FN planned research and wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by an unrestricted grant from Lundbeck, Italy and by Lundbeck Denmark for the pure ingredient.