
Abstract
As people with intellectual disability live longer, the number of people living with dementia is increasing, creating an imperative to implement tailored post-diagnostic supports that enable identity, self-determination, quality of life and well-being. To inform the development of post-diagnostic guidance for persons with intellectual disability living with dementia, a qualitative descriptive study was undertaken to understand experiences of accessing and using post-diagnostic supports and desired future supports. Four main themes resulted: 1. Being me: a sense of self through connection and valued life pursuits; 2. Meeting the social and personal needs of the person; 3. Formal processes that support people living with intellectual disabilities and dementia; 4. Challenges in supporting people living with intellectual disabilities and dementia. Findings identified areas of importance to living well, emphasising sense of self, social connectedness and meeting changing needs and care requirements in varied contexts through collaborative pre-emptive planning centred on the person.
Introduction
Life expectancy of people with intellectual disability has substantially increased over the past decades (McCarron et al., 2015) and is to be celebrated. However, concerns regarding the prevalence of dementia in this population have arisen, particularly in relation to people with Down syndrome (Bayen et al., 2018; McGlinchey et al., 2019). People with an intellectual disability particularly those with Down syndrome are at increased risk of developing dementia as they age (McGlinchey et al., 2019; Strydom et al., 2009). In a 20 year prospective follow up of 77 individuals with Down syndrome, McCarron et al. (2017) reported a risk of dementia of 23% in those age 50 years, increasing to 45% at 55 years and 88% in those aged 65 years. Clinical dementia was associated with cognitive and functional decline and new onset seizures activity.
The World Health Organization (2024) defines dementia as a term which refers to a number of conditions “affecting memory, other cognitive abilities and behaviour that interfere significantly with a person’s ability to maintain their activities of daily living”. Research has identified some of the impacts of dementia for persons with an intellectual disability as including: the loss of daily networks or limiting social participation; changing identities and relationships, including for some the disappearance of peers; loss of autonomy in decision-making; and concern for the future (Jacobs et al., 2023; Sheth 2019; Watchman et al., 2020). Watchman (2016) further highlighted the risk of a person being defined by a diagnosis of dementia and a need for effective person-centred post-diagnostic supports.
According to Gibb et al. (2019), the Irish Dementia Post-Diagnostic Steering Group conceptualises post-diagnostic supports as enabling and supporting individuals living with dementia and their families to live life with choice over the trajectory of the condition. An international consensus statement proposed a model for post-diagnostic supports for people living with intellectual disability and dementia with seven foci: quality of life, counselling, psychological and medical support, timely reviews of care plans, early identification of psychological and behavioural changes, reviews of care practices for advanced dementia and end of life care, and supports to carers and staff (Dodd et al., 2018). However, challenges have been identified in relation to the provision of services for older adults with intellectual disability living with age-related conditions including dementia. For example, Sheerin et al. (2024) noted difficulties in accessing mainstream services, accommodation, an appropriate staff skill-mix, and adaptations to changing needs. This despite ageing with intellectual disability being regarded as more complex than ageing in the general population and potentially involving “premature ageing” and “secondary conditions” (Alftberg et al., 2021, p. 192).
Literature has further highlighted a specific lack of awareness and knowledge of dementia among carers with a concomitant need for education and training in relation to caring for people living with the condition and an intellectual disability (Acton et al., 2023; Hughes et al., 2024). Key issues include the need for early and timely diagnosis of dementia, particularly in light of the risk of earlier age of onset (Watchman, 2016) along with advancing post-diagnostic supports to meet the complex needs of those with an intellectual disability and co-existing dementia (Begley et al., 2023; McCarron et al., 2002). While there is overlap in relation to post-diagnostic supports for those diagnosed with dementia in the general population, it is acknowledged that there are also sometimes higher and distinct needs for those with an intellectual disability, and that post-diagnostic support elements commonly necessitate adaptation (Begley et al., 2023; Dodd et al., 2018; Gibb et al., 2019). However, there is still limited evidence that includes the first-person experiences of those with intellectual disability and dementia despite the growth in the related evidence-base (for example, Jacobs et al., 2023; Sheth, 2019; Sheth, 2019; Watchman, 2016).
It is imperative that the voice and perspective of people with an intellectual disability and dementia inform post-diagnostic supports and any related guidance. Despite challenges to accessing the perspective of people living with intellectual disability and dementia in research (Watchman, 2016), guidance to support inclusive and ethical approaches to research inclusion and participation are widely available, many of which are grounded in researchers’ experiences and those of people with an intellectual disability and dementia (Collins et al., 2022; Novek and Wilkinson, 2019; Watchman et al., 2020). As such, post-diagnostic guidance should be informed by a variety of stakeholder perspectives including people living with an intellectual disability and dementia, alongside the available empirical evidence.
This paper presents the findings of a qualitative study to understand the lived experiences of accessing and using post-diagnostic dementia supports from the perspective of people with an intellectual disability and dementia, as well as of family members and staff carers supporting people with an intellectual disability and dementia. The research also aimed to understand future post-diagnostic supports that participants would like to have. The work reported here is a component of a large multi-stage mixed method research study informing the development of post-diagnostic dementia support guidelines for people with an intellectual disability (McCarron et al., 2023, 2024).
Methods
Research design
The study employed a qualitative descriptive research design, i.e., it was less theory driven than other research approaches thus enhancing its flexibility and utility in the conduct of healthcare research in diverse contexts and enabling researchers to remain close to participant experiences (Doyle et al., 2020; Kim et al., 2017). The study is reported with regard to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007).
Sample
Purposive sampling was employed to recruit participants with knowledge and experience of the research phenomenon. Services known to the research team as supporting people with an intellectual disability including an ageing population were approached to provide permission to conduct the research and provided with information regarding the purpose and nature of the study. The services were requested to act as gatekeepers to identify as potential study participants, people with an intellectual disability who had received a diagnosis of dementia, or family and staff carers (who had known the person for at least six months) for people with an intellectual disability with this diagnosis. Participant information leaflets were provided to gatekeepers to distribute, together with a consent form, or consent/agreement form to provide agreement on behalf of a person with an intellectual disability. To support inclusion and informed consent, these documents were made available in easy read versions as appropriate. Potential participants were given time to consider the information, and arrangements to conduct interviews were agreed between researchers and those who chose to participate.
Data collection
Data were collected via semi-structured interviews with the topic guides informed by the study aim, outcomes of a scoping review (Dennehy et al., 2023) and a focus group with providers of post-diagnostic dementia supports from earlier project work packages. Interview questions while addressing topic areas, were adjusted to meet the needs of individual participants, and employed inclusive and accessible language. Interviews were recorded with participant permission. Given the recent impacts of COVID-19 at the time of the study, and to support participant convenience, interviews were predominantly conducted online with four face-to-face interviews facilitated at participants’ request. Participants with an intellectual disability opted to have the support of a staff or family carer present during the interview to support them. To maximise the opportunity to share their perspectives and to accommodate participants who might have had difficulty with standard interview formats, an adaptation of photo/artefact elicitation techniques (Hergenrather et al., 2009; Kyololo et al., 2023; Wang and Burris, 1997) was employed in interviews with the person living with intellectual disability. Questions to support photo/artefact elicitation were incorporated into the interview guide (see Box 1 for examples of these questions). Two participants chose this option. Photo / Object: Can you tell me about this? What does this mean to you? Prompts: Describe your picture/object ➢ What is happening in your picture?/What does the object represent? ➢ Why is this important to you? ➢ What does this picture/object tell us about your life since the doctor told you have dementia?Box 1: Exemplar questions to support use of photo/artefact elicitation
Ethics
Ethical approval was obtained from the Faculty of Health Sciences Research Ethics Committee, Trinity College Dublin and service provider ethics committees, and a Data Protection Impact Assessment was completed and formally approved. To support inclusion of participants living with intellectual disability and dementia who might have an alteration in capacity to provide informed consent, a consent declaration was obtained from the Health Research Consent Declaration Committee (https://hrcdc.ie/guidance/). This supported the inclusion of one participant whose family member provided agreement to consent.
Analysis
The six phases of Reflexive Thematic Analysis (Braun and Clarke, 2022).

Two members of the research team generated initial codes having familiarised themselves with the data, through repeated reading of the transcripts. Critical to the aim of the study and to ensure the perspective of the person with an intellectual disability was central, a member of the research team with life experience of intellectual disability worked with one of the research team members during the coding process. As the analysis advanced through each phase of RTA, research team members met frequently to review, compare, agree and refine the write up of the thematic findings with recursive reference to participants’ primary data. NVivo software (QSR International (UK) Limited, 2022) was employed to facilitate the storage, organisation and analysis of the data.
Results
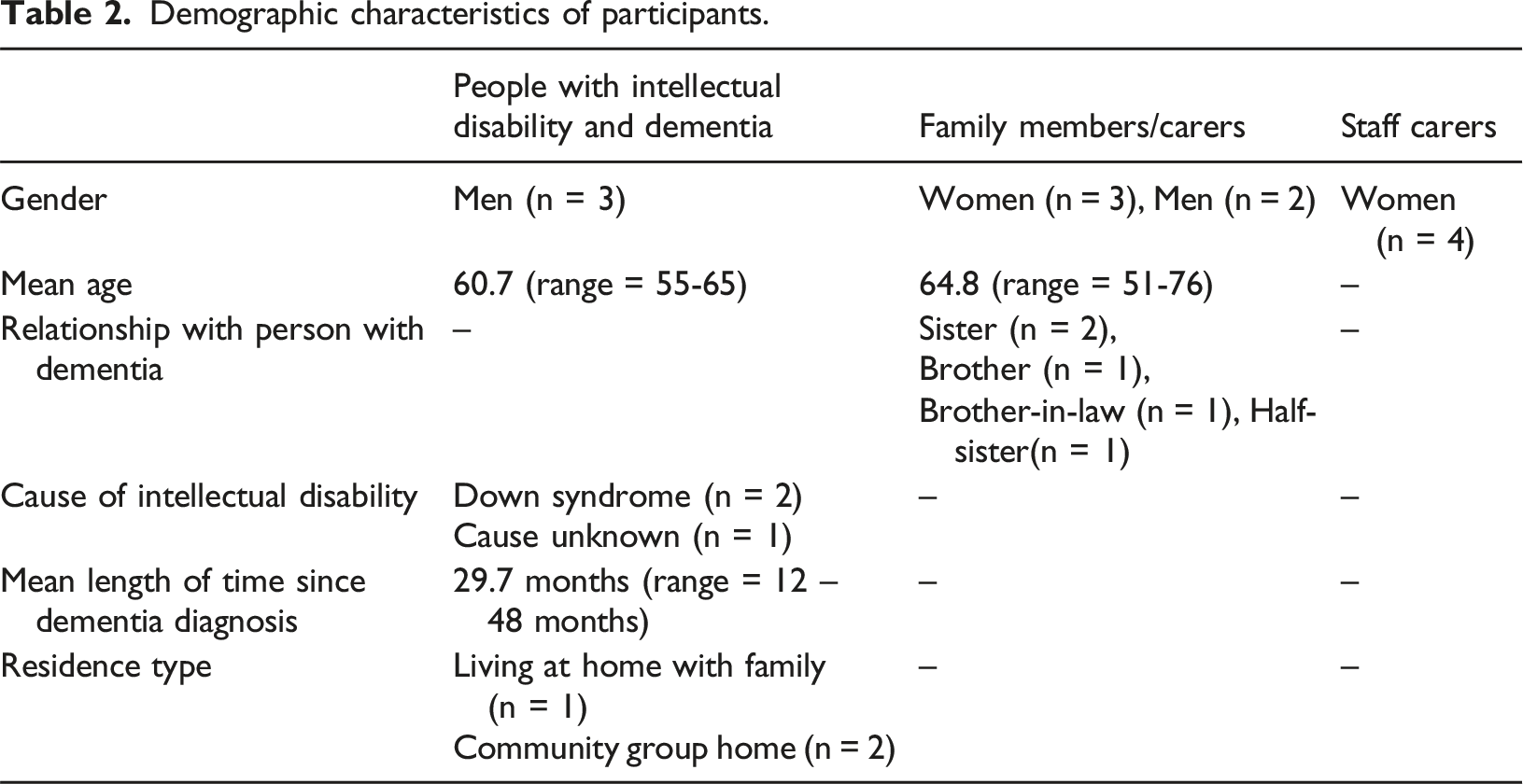
Demographic characteristics of participants.
The thematic structure identified through the process of RTA centrally positioned the focus on, and where possible the voice of, the person with an intellectual disability and dementia. The perspectives of family carers, family members and professional carers supported and/or elaborated the perspectives of those living with intellectual disability and dementia. Four main themes (with accompanying sub-themes indicated in italics in the presentation of findings below) were generated through the RTA process (Figure 1). The findings will be described with reference to these themes. Overview of the thematic findings.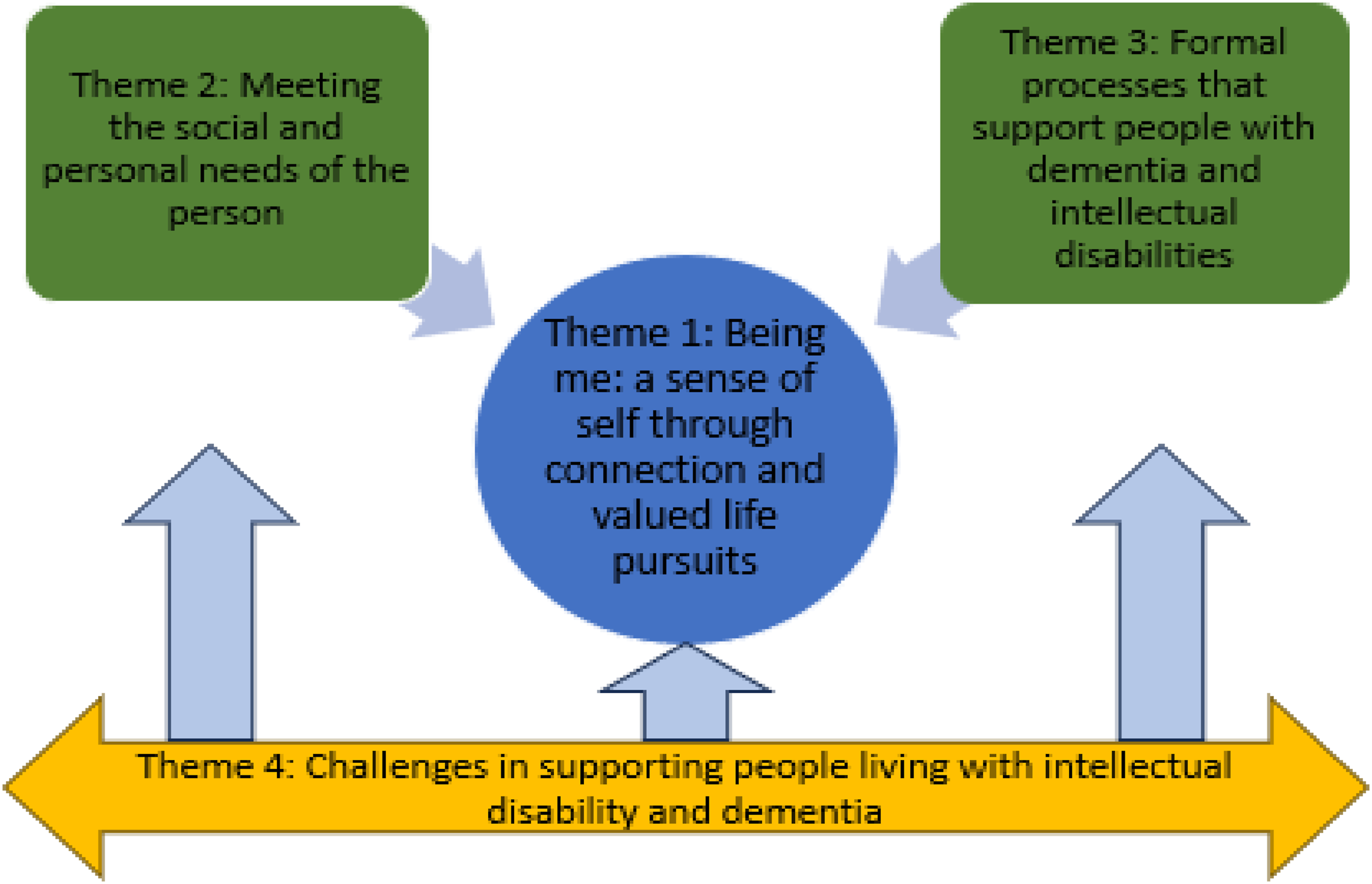
Theme 1: Being me: A sense of self through connection and valued life pursuits
The ‘importance of community and socialising’ was identified by those interviewed as central to supporting a sense of self and identity in the context of living with dementia. Participants further noted how conversing with people, and encountering helpfulness and caring enhances connectedness and belonging, and a perception of being known and valued in the context of local community: “They’re all good and very helpful and caring. Like the way that you are with me kind of stuff. And I felt happy about it” (Person with an intellectual disability and dementia) “There’s some [people] that she [person living with dementia] has established long-term relationships with you know. And because it’s a country place, everybody knows one another as well. So, there’s a good sense of community. And not only do they know her, they know me; they know my family do you know. So, there is this sense of community” (Family carer) “Yea and I do talk to the neighbours across the road there” (Person with an intellectual disability and dementia)
Participants further acknowledged that with progression of dementia, continued connection can require additional supports and an understanding of a person’s changing abilities, for example, when planning a social outing. This noted, carers emphasised that maintenance of social connection is important to quality of life and continued sense of self. However, carer participants acknowledged that where familiar surroundings or routines change, there may be a potential impact on a person’s daily living abilities, independence or life skills: “I think when they [persons with intellectual disability living with dementia] move out, they nearly go downhill quicker because they’re not, their surroundings is different and everything around them is different.” (Staff carer)
Thus, findings suggested that ‘connection through familiarity’ is an important consideration to sense of self. There was reference to familiarity with people, places and routines also being linked to perceptions of safety and knowing support is available in the context of change. For example, living where there is familiarity and ease of navigation was identified as important to life with dementia and a sense of reassurance: “Visiting people and the old people who I know locally, but not a stranger …” (Person with an intellectual disability and dementia)
A person’s home was identified as a place where valued interests and current skills could be supported. Familiar environments in general were identified as providing a context where activities and hobbies could be enabled and continued in tandem with connection to valued others. Thus, abilities can be supported and maintained for as long as possible upholding agency and self-efficacy. There was reference to activities and hobbies bringing joy, connection with others, sense of achievement or relaxation. Examples included gardening, nature, and music: “I do yea [name of a singer] is like first class. I do I like concerts and friends, yea. And the music society is my favourite as well.” (Person with an intellectual disability and dementia) “That garden, he loves it, he would sit out there in the garden all the time he loves. And planting flowers, and like he wouldn’t have been a big gardener, now he just it’s a new thing sort of with him.” (Staff carer)
Theme 2: Meeting the social and personal needs of the person
Findings suggested that care which supports quality of life and well-being for the person was understood to extend beyond functional supports by attending to the individual, their preferences, and desired activities in supporting identity, independence and personhood. Thus, the need for ‘creative and compassionate solutions in care’ were identified, as a one size for all approach is not possible in pursuit of these aims. To this end, carers indicated the necessity to be observant, to note subtle indicators of preferences and changing needs over time, which could then inform the creative meeting of person-centred care-related challenges, via appropriate adaptations and ensuring safety. Consequently, the need for fluidity or flexibility and an openness to try new things was common in participants’ narratives: “I find him [person living with intellectual disability and dementia] getting quite stressed out like. Or you know pulling at his clothes things like that. I’ll sit him down, we’ll turn the television off, you know we’ll put music on. And I’ll get him his blanket, and as I said sometimes it works and sometimes it doesn’t like you know… Everything that [name of person] used to do, we no longer do, or we do but we do it differently do you know?’ (Staff carer)
“… So, like the staff team here are quite good in recognising needs and kind of acting on them.” (Staff carer)
While it was highlighted that ‘good communication is key to good care’ and therefore meeting needs, and that it supports inclusion and belonging, carer participants noted challenges could be encountered in maintaining effective communication with the person, for example some family carer participants referred to difficulty in understanding what a person might be trying to communicate that could lead to “frustration” or “aggressive behaviour” (Family carer). Inferences in family and staff carer data noted communication breakdown could lead to the person living with dementia experiencing isolation leading to frustration. However, there were references to experiential, and for professional carers formal, learning in intellectual disability and dementia care as assisting in the redress of challenges to communication. For example, enhanced attention to non-verbal communication cues and the use of communication supports including visual aids, social stories and communication passports were highlighted: “I suppose I've just always been respectful of [name of person supported] …. no matter how much they can understand…. I still have to respect that he might understand some of it. So therefore, I would tell him the same as I'd tell anybody else, you know what I mean, I'll tell him about what my day has been, where I was, I'll tell him I'm back, you know, regardless of what he can and can't understand. You know, and I don’t talk to him in baby talk, I talk to him ordinary.” (Family carer) “I suppose staff would always like that now be very vigilant. Monitor her [person living with intellectual disability and dementia] facial expressions and stuff like that” (Staff carer)
While the previous theme highlighted the importance of familiarity in upholding the person’s sense of self, agency and belonging, here ‘familiarity in care as the foundation of a good life with dementia’ extends this from being known to highlighting the presence and involvement of familiar people in the provision of care. For example, the data evidenced professional staff experiences of noting change in the person in the presence of unfamiliar care staff, for example, upset. In contrast, where the carer knows the person, it was suggested they would be better placed to understand and document preferences and needs, and to ensure shared knowledge of this in support of continuity in care. As such, familiarity can support person-centred care planning, placing the person at the centre of a circle of support. Family carers also supported the centrality of familiarity in care, noting benefits in terms of social interaction and attention to their loved one’s preferred choices or needs: “So, you know it’s kind of what you call wraparound care. Or what I think of as wraparound care… what I would say is that the care is individualised in that if there’s a need they seem to respond.” (Family member) “But he [Person living with intellectual disability and dementia] really needs full-time staff that know him, you couldn’t have a stranger working with him…. But other than that, like, again it’s getting around to knowing him so well and the documentation in his files for staff when they come in.” (Staff carer)
Theme 3: Formal processes that support people with dementia and intellectual disabilities
Participants outlined forms of ‘multidisciplinary supports across the dementia journey’ that when and where available, timely and appropriate to preferences and needs, can support the maintenance of health and quality of life. Findings in this theme relate to evidence provided in the main by staff carers and family members whose relatives were in receipt of care within organisations. Professional carers spoke of access to multi-disciplinary teams, and family members noted the level of support offered to their family members who were being cared for in such settings. The benefits of access to professionals with expertise in both intellectual disability and dementia were identified, including the identification and resolution of issues as they unfold. There were also some references to the positioning of a multidisciplinary team [MDT] where a diagnosis of dementia was made. Where this was possible, actions by that team were indicated as working to ensure structural supports were made available to enable the possibility of ageing in place of choice or to avoid the need for transfer to a hospital or another setting as shown here: “Yea we have the CNS, [Clinical nurse specialist name] comes to him. Speech and language, dieticians, the dietician’s onboard with him actually at the moment. Because he had such a big weight loss when he was in and out of hospital. But oh, yea we’ve a full MDT so we have…. Oh [name of person with dementia] will stay here; there’d be no reason for him to go back down.” (Staff carer)
The data evidenced expressions of ‘satisfaction with the supports in place’ particularly from family members whose relatives were being cared for within an organisation and professional carers: “You could not buy the service she [person living with dementia] gets there. I mean really, she couldn’t, every last detail has been thought of.” (Family member) “Where she [participant’s sister] is now, has the best facilities that she’s ever encountered through the years. And obviously, her care since the onset of dementia has been much harder work for the staff concerned.” (Family member)
Professional carers linked to or within organisations that had built support structures to care for people with intellectual disability living with dementia referred to the convenience of having a team of skilled and relevant professionals at hand. However, some disparity was noted in the availability of such supports, which can impact on the person and carers, for example for those living outside of formal organisations, as will be evidenced as part of the following theme.
Theme 4: Challenges in supporting people living with intellectual disability and dementia
Participants elucidated ‘challenges when support is not available’ that impact on the provision of person-centred care with respect to enabling ‘Being me’ a sense of self through connection and valued life pursuits’ elucidated earlier. Family carers’ perspectives were particularly represented in this theme, although not exclusively. Such carers highlighted significant delays in receiving a diagnosis for the person and, for some, deficits in the following post-diagnostic supports. Examples cited included absence of or insufficient information, a lack of signposting to relevant supports with one family carer indicating she felt “invisible” (Family carer). In the absence of relevant information and where there was no help in managing needs, for example changes in communication, there was reference to breakdowns in communication or trying to search online for solutions. Such experiences were accompanied by expressions of inability to negotiate access to assistance and/or uncertainty about the future of a loved one: “And it was me complaining to him [doctor] that we have got no support. Why has he [person living with dementia] not seen somebody in a hospital? Why has nobody sent me a book to say here is information about dementia? But nobody did that.” (Family carer)
The availability of funding was commented upon. For example, family carers referred to encountering difficulties in relation to access to funding for home accessibility modifications leading to having to draw on pensions and savings: “The biggest thing that’s keeping us back at the moment, obviously, is finance because I have spent all my, all my retirement, most of my retirement money on doing up our kitchen and doing the bathroom upstairs to make it compliant and like because of the dementia I've had to paint the, the room a certain way, I've had the, I did the house in certain dark colours so that, you know, they stand out for him” (Family carer)
There was also some inference to financial issues being a consideration in some instances leading to decisions to a person having to move from their home within an organisation. Resourcing was also cited as a potential challenge in relation to being able to facilitate one-to-one care to support social and personal life, and maintenance of skills: “There's a lot of small little things like, you know, like digital life story books, putting things together, things like that. Staff on the floor struggle to find the time to be creating new stories or, you know, it's a very sad thing to say but that is the reality, one staff member on duty, you know. …That might just be attending to her activities of daily living. So, like I think, again, as I said, we could do with a support staff for [name of person living with dementia], if we did have a support staff we could, you know, have them doing all those types of things with [name of person supported], do you know.” (Staff carer)
Encountering ongoing challenges inherent in the experience of caring (including information, support and funding or resourcing) were linked to descriptions of ‘the impact of caring on carers’. Such impacts could include personal, physical, emotional and financial. For example, family carers indicated impacts on prioritisation of their own health needs, particularly in instances where there is an absence of support for the person living with dementia when a family carer is not there: “I can't get out for a walk every day like I had started there, I'm well over-weight, I'm now on [medication for a health condition] since the start of all this.” (Family carer)
Impacts on sleep and the need for ongoing vigilance and being on persistent high alert in relation to their loved one was an experience recounted by some family carers. Limitations on time and means to access professional support including emotional was indicated and the family carers highlighted having had distressing experiences as a carer which could lead to anxiety and frustration, impacts on relationships and isolation: “I honestly don’t think we can keep going, I think we’re already past burnout.” (Family carer)
Evidence from the professional carer data also suggested sadness or guilt for those who experienced challenges in care provision due to lack of available supports: “I find it sad that we don’t have time to do those types of things with her and like I feel guilty about it but I know people can only do like what they can in the short space of time that they're there and there's other people to support and look after as well, you know” (Staff carer)
Findings from professional carers, family members and family carers demonstrated ‘the need for appropriate and timely information and training’ considering gaps experienced in information flow and dementia specific care skills. Professional carers highlighted a desire for further education indicating that having more staff carers with dementia specific knowledge and skills could enhance the potential for people diagnosed with dementia to receive appropriate and timely support. Family carers also made some suggestions including having a point of access to information and experience about caring for someone with an intellectual disability, a plan put in place for living at home, peer support and signposting to relevant supports: “Well, I suppose it would be great to meet up with or connect to other people in similar situations because it's very, it's very isolating, you know, and especially now. Again, the support would be company. The support would be somewhere that we could access but we'd have to be able to access it” (Family carer)
Discussion
This study explored the experience of people with an intellectual disability and dementia in relation to accessing and using post-diagnostic dementia supports and desired future supports, as well as the related experiences of the family members and staff carers supporting these participants and other individuals with an intellectual disability and dementia. The study further aimed to position and respect participants living with an intellectual disability and dementia as active participants in their own lives, care and as research participants. Findings demonstrated that for the person living with dementia, sense of self was lived out through interests and activity enabling purpose, achievement and pleasure, and the maintenance of the familiar; an important goal post diagnosis of dementia identified by the majority of participants. In addition, the findings demonstrated the importance of personhood and inclusion and their ongoing support; good communication; and person-centred, timely post-diagnostic supports. The importance of ongoing and familiar relationships and routines to enabling engagement was similarly identified by Jacob et al. (2023), while Sheth et al. (2021) and Watchman et al. (2020) highlighted the importance of supporting peer friendship networks and their maintenance as dementia advances.
Participants with an intellectual disability and dementia in the current study referred to the importance of social connections and access to preferred hobbies and pursuit of interests and their connection to sense of agency and perceptions of feeling valued and belonging. There was also some reference to interdependence. Being known in and having continued connection with one’s community were highlighted as pivotal to the support of a person’s self-identity. These findings are important. In a systematic review, Jacobs et al. (2023, p.251) identified “narrowing of lives” as associated with changes in functioning particularly when discontinuance of work and leisure activities occurred. Sheth (2019) further highlighted self-limiting of participation by the person with dementia. Concepts such as belonging, friendships and reciprocity have been the focus of exploration in the field of intellectual disabilities more widely (McCausland et al., 2020). A systematic methodological review by Fulton et al. (2021) identified the importance of such concepts to social inclusion but concluded that clear conceptualisations of both belonging and reciprocity were lacking, and rarely centralised to the person in research. Fulton et al. (2021) consequently called for more nuanced understanding. Findings from the current study draw attention to these concepts for those living with dementia and shed additional light.
A need was also identified for pre-emptive planning and resources including funding to enable the person to continue to pursue interests and to age where possible in their home of choice. Evidence demonstrated that some intellectual disability services actively plan to support remaining in place of choice over the trajectory of dementia. Such findings resonate with other dementia research findings that support of social identity and social networks may contribute to conversations in relation to advance care planning (Nimmons et al., 2023). It further supports the importance of the person living with dementia being central to planning for their care and support, a finding reiterated by others such as Chapman et al. (2018) and Jacobs et al. (2023).
Participants’ narratives suggested that as dementia progresses and abilities and needs change, understanding, innovation and adaptation are required. Respect for personhood is heavily reliant on the availability of timely support to address health and well-being, living safely and having preferences met. This study supports that collaborative planning, and person-centred support of those with an intellectual disability and dementia (Cleary and Doody, 2017; Herron et al., 2020), involves a multifaceted team working in an interdisciplinary way, listening to the voices of individuals with intellectual disability, and their carers; with members familiar with the person, their changing needs and personal preferences and abilities. Access to post-diagnostic specialist dementia care and environmental supports were also identified as vital to the care provided by the different carer participants. The literature supports that perceptions of quality of service are reliant on family, paid carers and intellectual disability services having access to such professionals with dementia specific knowledge and skills (Acton et al., 2024). However, as in the current study, access to such expertise can vary.
Although findings are consistent with earlier research by Herron et al. (2020), reference to lack of information in relation to available supports and how to access them, along with carer knowledge on how to manage changing needs and care appeared to have impacts on all involved. This is not an isolated finding. Acton et al. (2024) identified that post-diagnostic supports for people with an intellectual disability and dementia should enable access to information and navigation of everyday challenges but found that this was often not the reality. Carers in the current study noted an absence of clear signposting to information, training and education. Hughes et al. (2024) in their systematic review similarly reported disparities in service access and challenges in service navigation. Thus, there is a pressing and critical need for information about dementia in the context of intellectual disability, available supports and how to access them, and education optimised to different carer group needs, a finding supported by others in the field (Acton et al., 2023, 2024; Cleary and Doody, 2017; Dicks et al., 2015; Herron et al., 2020; Hughes et al., 2024).
In the current study, a disparity was noted by some in relation to resources available to people living in the family home compared to those living within varied service provided settings. There were references to the particular challenges of providing quality care for the person without access to necessary supports and how the impacts lead to neglect of the person’s and family carers’ own social, physical and health needs. Carers referred to perceptions of not being seen and for some burnout impacted on the ability to provide continued care and on relationships including with the person with an intellectual disability and dementia. There was also some reference to these being compounded during the COVID-19 pandemic. Similar findings were highlighted by the Alzheimer Society of Ireland (ASI, 2023) and in a further report by the ASI and Family Carers Ireland (2023), which emphasised the disconnect of these experiences from the reliance of the health and social care system on family carers to provide the majority of care to those living with dementia. In those reports, financial aspects of caring are highlighted, as in this study, with respondent carers indicating that many had reduced working hours or withdrawn from their work to provide support and care. Again, similar to the current study, national (ASI 2023) and international studies (Lindeza et al., 2024) identify that while rewards and gratifications form part of the mosaic of the caring experience, carers of people living with dementia have more stress and burnout than the wider population alongside social, emotional and financial costs.
Strengths and limitations of the study
The research processes employed in the study contributed to credibility and the creation of an audit trail enhancing the trustworthiness of the research process with reference to the transferability, dependability and confirmability of its findings (Lincoln and Guba, 1985; Stahl and King, 2020). This noted, as with all research, this study has limitations. For example, despite the best efforts of the research team, only three participants living with dementia directly participated. However, consistent with Koppel and Dallas (2007) (referencing Smith et al. (1999)), a centralising textual focus was applied to their interview data, and to the perspectives of other participants providing richness and an enhanced understanding of variations in living environments, observations and experiences; an approach consistent with other research in this field (Manji and Dunn, 2010).
Conclusion
This study through its illumination of the experiences of accessing and using post-diagnostic supports, and understanding of desired future supports, provides evidence to inform the development of post-diagnostic support guidance for people living with an intellectual disability and dementia. As living with a diagnosis of dementia for a person with an intellectual disability can bring particular complexity, addressing resultant challenges requires creativity, compassion and knowledge of the person. The findings demonstrate that post-diagnostic dementia care is best experienced in a familiar environment, with familiar people who adapt support to a person’s preferences, abilities and changing needs using a person-centred perspective. Belonging, social connection, agency and personhood are maintained via communication, collaboration and individualised supports. However, the need for information, intellectual disability and dementia specific education and reduction of disparities in available services, needs to be addressed. All people living with intellectual disability and dementia require access to dementia specific post-diagnostic supports that uphold sense of self and identity, while meeting individual needs, regardless of place of residence.
Footnotes
Acknowledgements
We sincerely thank all of the study participants for giving so generously of their time in order to help us understand their experiences and perspectives.
Ethical considerations
Ethical approval for the study was granted by The Faculty of Health Sciences Research Ethics Committee Trinity College Dublin on 1st June 2021 and individual service providers where required. To support the inclusion of participants with intellectual disability and dementia who might have alteration in capacity to provide informed consent, a consent declaration was obtained from the Health Research Consent Declaration Committee (![]() ) on 30th July 2021. Participants provided informed consent or assent prior to participating in the research interviews.
) on 30th July 2021. Participants provided informed consent or assent prior to participating in the research interviews.
Author contributions
Authors listed on this manuscript were members of the research team who conducted the study and involved in preparing the content in the manuscript.
Funding
The research was funded by the Health Research Board of Ireland and the Alzheimer Society of Ireland, through the Health Research Charities Ireland – Health Research Board joint funding scheme (Grant number HRCI-HRB-2020-026).
Declaration of conflicting interests
The authors declared no potential conflicts of interest.