
Abstract
The impact of the COVID-19 pandemic on the health and wellbeing of social workers working with people with learning disabilities has not been fully explored. This paper reports findings from a large United Kingdom study that surveyed health and care workers in six phases of the pandemic and shortly thereafter (2020-23) relating to 310 social workers who worked with people with learning disabilities. Mann-Whitney U tests revealed that these social workers experienced a decline in wellbeing over the pandemic period, but this lessened as time passed. Logistic regression showed that social worker wellbeing predicted intentions to leave their profession. This study offers an evidence-based foundation to guide retention policies in learning disability social work, aiming to stabilise the sector and preserve essential experience for workforce planning.
Background
The regulated profession of social work in the United Kingdom (UK) is generally organised around children’s and adults’ services, with some social workers’ main, or sole service user group being people with learning disabilities either children and/or adults. It worth noting that in this paper the term learning disability is used reflective of UK legislation and services. Elsewhere the terms intellectual disability, intellectual and developmental disability or intellectual impairment are used. Most of the social workers employed to work with this service-user group work in local government (in England, Scotland, and Wales) or integrated Health and Social Care (HSC) Trusts combining health and social care (especially in Northern Ireland), with a minority working for the National Health Service (NHS) or independently. Their role often centres around assessments of need and risk, care planning and monitoring with people in complex situations or multiple and/or severe disabilities including work with carers and families. They practice within legal frameworks and principles of human rights. However, in England a statement of capabilities for social workers working with adults with learning disabilities, published by the Department of Health and Social Care (DHSC) and the British Association of Social Workers (BASW), proposed distinctive skills needed for this practice area. It noted: Social work with people with a learning disability differs from generic adult social work… With people with learning disabilities the social worker gets much more involved in the person's life, dealing with the small stuff, as well as the main issues/concerns/ area of need…. (DHSC/BASW, 2019, p. 10)
Despite this, a recent study of family carers of people with learning disabilities noted: ‘Attendees discussed current pressures within social work, including poor pay and conditions and how the role has become one of reactive practices largely focused on crisis management’ (Ryan et al., 2024, p. 72). This echoes previous concerns that social work practice in this area is undertaken ‘with a cohort that often achieves poor outcomes and for whom complex systems, processes and resource pressures can supersede person-centred and asset-based support’ (SCIE & Innovation Unit., 2018, p. 47). These concerns prompted a short-lived government funded experiment of appointing ‘named social workers’ for specific groups of adults with learning disabilities (e.g. with complex or multiple needs) giving these social workers a protected or very limited caseload (ibid). Such specific roles were envisaged as having the potential to be the main contact points for individuals and carers, combined with being a professional voice to advocate for them across agencies (James et al., 2018).
Practice guidance also exists in England for social work with adults with complex needs which encompasses people with learning disabilities who may be eligible for publicly funded social care support and social work interventions (NICE, 2022). The overall population of people with learning disabilities is sizeable, with 1.3 million people with learning disabilities in England alone, of whom, 950,000 are aged 18+ years (Public Health England, 2023). However, not everyone with a learning disability in the UK has a social worker, named or otherwise, or complex needs.
Evidence of the serious impact of the COVID-19 pandemic and its legacy on many people with learning disabilities is emerging internationally (see Lunsky et al., 2022). Their increased risks of hospital admission and mortality during this period (Tromans et al., 2020; Williamson et al., 2021) were highlighted in the context of people with learning disabilities being more likely to experience poor health and wellbeing, loneliness, and poverty than England’s general population (Flynn et al., 2022). As Alma Economics (2023) summarised ‘Covid-19 led to losses of routine, activities, and contact with family and carers, with the death rate for people aged 18-34 with learning disabilities 30 times higher than that of non-disabled people of the same age group. The impacts of social restrictions aimed at curtailing transmission of the virus were reported to be particularly profound for people with learning disabilities’ (see also Courtenay and Perera, 2020; Murray et al., 2021). Specific to social care, a survey in the early months of the pandemic by MENCAP (2020) (n = 1069) reported 69 percent of people with learning disabilities had their care cut or reduced since the pandemic; most (79%) families were providing more care for their relative, and many (72%) families feared further cuts.
While there are several studies of direct care and support staff working with people with learning disabilities during the pandemic (e.g., e.g.Linehan et al., 2022), the impact on social workers working with people with learning disabilities is less evident. One probable reason is that this is a small specialism numerically. For example, in NI, only 338 (5.1%) of its 6628 social workers were primarily working in Adult Learning Disabilities in 2023 (NISCC, 2023) while in Children’s Learning Disabilities there were 73 (1.1%). Social Work England (2023) reported 3373 (3.4%) of its 100,654 registrants worked with Adults with Learning Disabilities and 2514 (2.5%) with Children with Disabilities (physical and/or learning disabilities). In Wales 110 (1.8%) social workers from a total of 6241 have recorded their primary service-user group as learning disabilities (anecdotally reported by Social Care Wales). Data from Scotland was unavailable.
Despite these small numbers of social workers, the population of people with learning disabilities is sizeable, with 1.3 million people with learning disabilities in England alone, of whom, 950,000 are aged 18+ years (Public Health England 2023). Local government adult social care expenditure was £28 billion in 2022/23 (The King’s Fund 2024) with most being spent on support for working-age adults with learning disabilities and physical support for disabled people (NHS Digital, 2022). While people with learning disabilities constitute five percent of England’s disabled population, they receive 43 percent of net state current expenditure on long- and short-term care (NHS Digital, 2022). Social workers are the main professionals undertaking social care assessments, making decisions around planning, budgets and co-ordination, as well as monitoring and review of these processes, and undertaking liaison with carers, family and other professionals (they are also a central part of statutory based mental health assessments for non-voluntary assessment and treatment). Thus the impact of the pandemic on this group has wide implications if it includes a loss of experienced professionals making key decisions or if they are working sub-optimally.
The pandemic’s impact on social workers has been studied internationally (see Harrikari et al., 2023) and in the UK (Owens et al., 2024), often in relation to psychological distress and resilience. Its effects on social work specialisms have also been explored (e.g., Ross et al., 's 2021 study of paediatric hospital social workers). Other studies observed the impact on social workers’ wellbeing, mental health, stress, and burnout but not client group effects (e.g. Ashcroft et al., 2022; Maddock, 2024; UNISON, 2022). Several focused on changing practice, such as increased online communications with colleagues and service users (McFadden et al., 2020; Mishna et al., 2021), use of professional judgement (Manthorpe et al., 2021) and responses to pandemic-related legal, ethical or employer changes (Baginsky et al., 2023; Banks et al., 2020). However, the small numbers of social workers specialising in learning disabilities mean that their views and experiences may be subsumed by general studies.
The pandemic’s impact on the social work profession needs to be set in context. UK social work employers prior to the pandemic have long been experiencing staff shortages and high turnover (e.g. Wiseman and Davies, 2013). Ravalier and Walsh (2018) found half (50%) of UK social workers (n = 3421) were dissatisfied with their role with 60 percent considering leaving their jobs. Comparing UK social workers working with adults with learning disabilities (n = 77) to those working in child protection (CP) (n = 358) using the Maslach Burnout Inventory, McFadden et al. (2018) found high levels of emotional exhaustion (EE) co-existing with high levels of personal accomplishment (PA) in both practice areas (CP 75%; learning disabilities 69%), while less depersonalisation (DP) was reported among both groups (CP 32.4%; learning disabilities 15.5%). The proportion of social workers working with adults with learning disabilities who scored highly in DP was lower than social workers in other user group specialisms. Levels of PA were high among the learning disabilities group despite high levels of EE, but very similar to other respondents. In summary, EE levels were high in 2018 indicating that social work with adults with learning disabilities was a stressful occupation prior to the pandemic but possibly mediated by lower DP (often attributed to good relationships with clients/service users).
Study aims
As noted above, few studies have investigated the health and wellbeing of UK social workers working with people with learning disabilities during the pandemic. This study aimed to assess the impact of the COVID-19 pandemic on the wellbeing of this group at six different time points between May 2020 and February 2023, made possible by the large numbers of responses to our surveys. We hypothesised that their wellbeing would decline as the pandemic progressed. Additionally, we examined whether factors such as wellbeing levels, age, gender, sick days, and country of work predicted intentions to leave the profession. The study also sought qualitative data to provide context to the quantitative findings which were analysed with the aim of providing insights into these social workers’ perspectives on how the pandemic affected their practice, themselves and their working conditions (for full study details see McFadden et al., 2020).
The timeline of pandemic restrictions in the UK were fairly common across all four countries and aligns with the same global timeframes that impacted the international community (Harrikari et al., 2023). In March 2020 they began to affect the general population with lockdowns and changes to service provision in line with government rules and legislation (The Coronavirus Act, 2020). By May and June 2021, schools reopened and limits on attendance at weddings and funerals were removed. By July 2021 all restrictions were removed. However, the pandemic’s legacy continues to affect the workforce and care services long after restrictions ended, as our study demonstrates.
Materials and methods
Design and participants
This paper employs a mixed methods approach to highlight the experiences of social workers specialising in learning disabilities. It was a component of a broader, ongoing multi-phase programme, entitled ‘Health and Social Care Workers’ (HSC) quality of working life and coping whilst working during the COVID-19 pandemic (McFadden et al., 2020). We investigated how delivering health and social care during the pandemic had affected UK nurses, midwives, allied health professionals, social care workers and social workers, working in various settings including hospitals, care homes, community, and day services. By employing both qualitative and quantitative methods, the study explored mental wellbeing, quality of working life, coping mechanisms, and burnout during and after the pandemic (McFadden et al., 2023a).
The study had a cross-sectional design, gathering data at roughly six-month intervals: Phase (P)1 (May - July 2020), P2 (November 2020 - February 2021), P3 (May - July 2021), P4 (November 2021 - February 2022), P5 (May - July 2022) and P6 (November 2022 - February 2023). Our online survey included reliable and validated measures, with each survey featuring a few open-ended questions to capture respondents’ experiences and perspectives. An opportunity sample was recruited through social media platforms (Facebook, Twitter/X) and professional associations, unions, communications, employers, and regulatory bodies. For this paper, we analysed data exclusively from social workers who reported working primarily or exclusively with children and/or adults with learning disabilities.
Ethical approval was attained from the Research Ethics Filter Committee of the School of Nursing Ulster University (Ref No: 2020/5/3.1, 23 April 2020, Ulster University, IRAS Ref No. 20/0073) for the study and Trust Governance approval (for Northern Ireland only) was gained from the Health and Social Care Trusts for Phase 2. Permission for the use of the scales used in the questionnaire was provided by the original authors, and consent and confidentiality were addressed in Participant Information Sheets provided at the start of the survey.
Measures
Demographic and work-related variables
The survey obtained demographic and work-related information. Variables comprised gender, age category (21–29, 30–39, 40–49, 50–59 and 60+), ethnicity, country of work (NI, Scotland, England, Wales), place of work (hospital, community, primary care or GP practice, care home, day care, and other), sick days taken over the previous year (none, less than 10, 11–20 and 21+), and intentions to leave their profession (yes and no).
Mental wellbeing
Mental wellbeing was assessed using the seven-item Short Warwick Edinburgh Mental Wellbeing Scale (Stewart-Brown et al., 2009). Respondents rated their feelings over the past two weeks on a five-point Likert scale from 1 to 5. Item scores were summed and then converted to metric scores for comparison with other samples. Scores ranged from 7 to 35, with higher scores indicating better mental wellbeing. This scale is known for its excellent psychometric properties (Stewart-Brown et al., 2009). In this study, the internal consistency coefficient, as measured by Cronbach’s alpha, was α = 0.89.
COVID-19 related working conditions
Working conditions were assessed with one open-ended qualitative question in P2 to P5: ‘What was the impact of COVID-19 on your specific place of work, so far, in relation to patient/user numbers and service demand?’. Other open-ended responses were also optional for respondents to explain or detail particular impacts of the pandemic on health and wellbeing. The qualitative data helped ensure that the quantitative survey results were rooted in respondents’ experiences.
Data analysis
Collected data were coded, cleaned, and prepared for analysis. Responses were filtered to include only those from social workers working primarily or exclusively with people with learning disabilities (n = 310). To ensure accuracy, a pre-analysis check was conducted to identify any missing data and extreme values. Descriptive statistics were generated using SPSS-28. Qualitative responses were analysed through reflective thematic analysis, following Braun and Clarke’s six-phase framework (Braun and Clarke, 2021). This flexible methodology offered a comprehensive understanding of the survey data.
Findings
Demographics
Sociodemographic details of social workers working with people with a learning disability (n = 310).
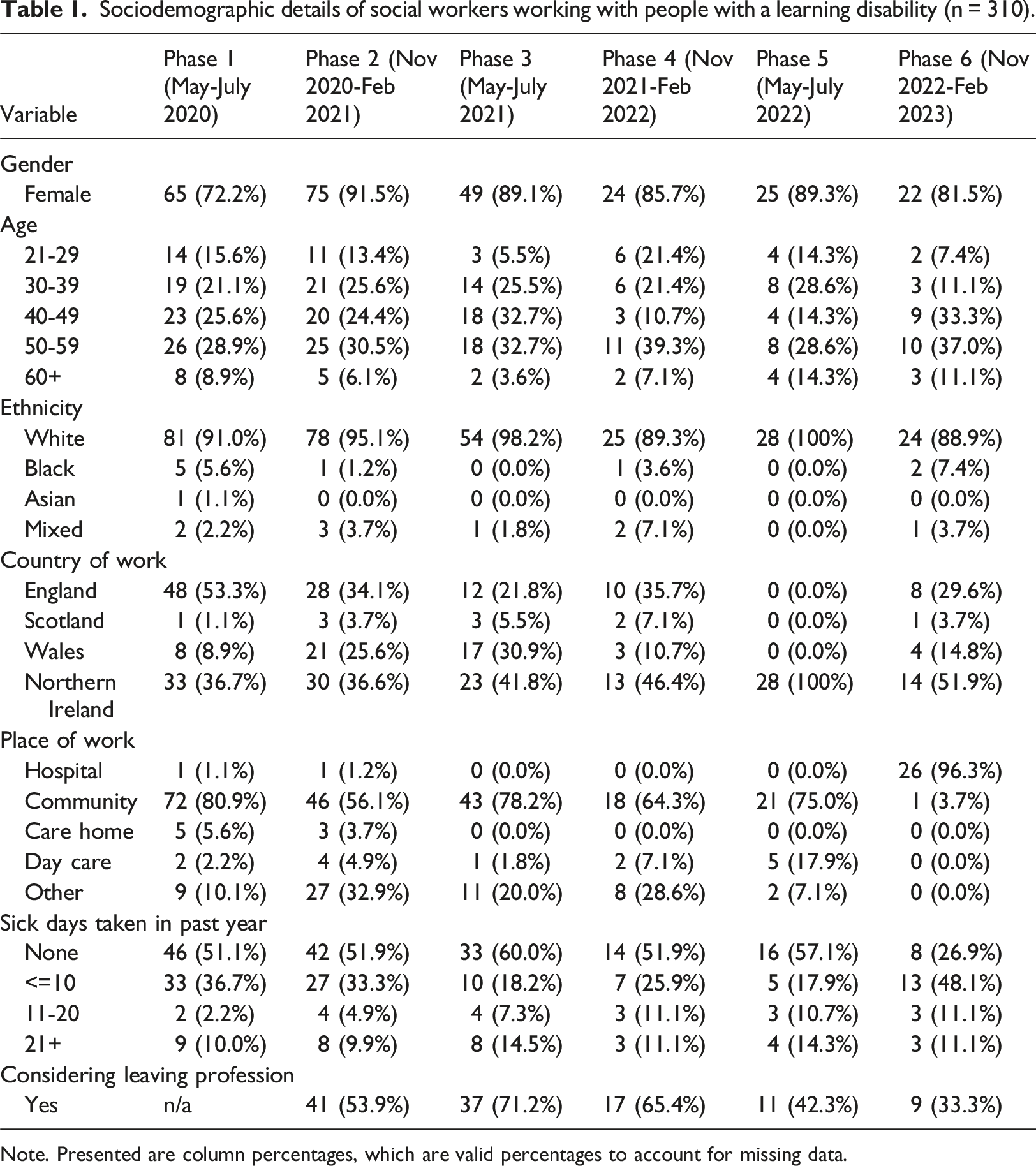
Note. Presented are column percentages, which are valid percentages to account for missing data.
Quantitative findings
A series of Mann-Whitney U tests examined differences in wellbeing scores between each of the six phases (see Figure 1) among the social workers working with people with learning disabilities. There was a significant negative decline in wellbeing scores from P1 (Md = 19.98, n = 70) to P3 (Md = 18.59, n = 51), U = 1154.50, z = −3.32, p < .001, with a moderate effect size r = 0.30, then a significant increase in wellbeing from P3 (Md = 18.59, n = 51) to P5 (Md = 20.73, n = 23), U = 312.00, z = −3.31, p < .001, with a moderate effect size r = 0.38, however, mental wellbeing declined in P6 though not significantly Overall Wellbeing Scores by Study Phase and Country among social workers working with people with learning disabilities Note: 23.6 population norms for wellbeing (Ng et al., 2017).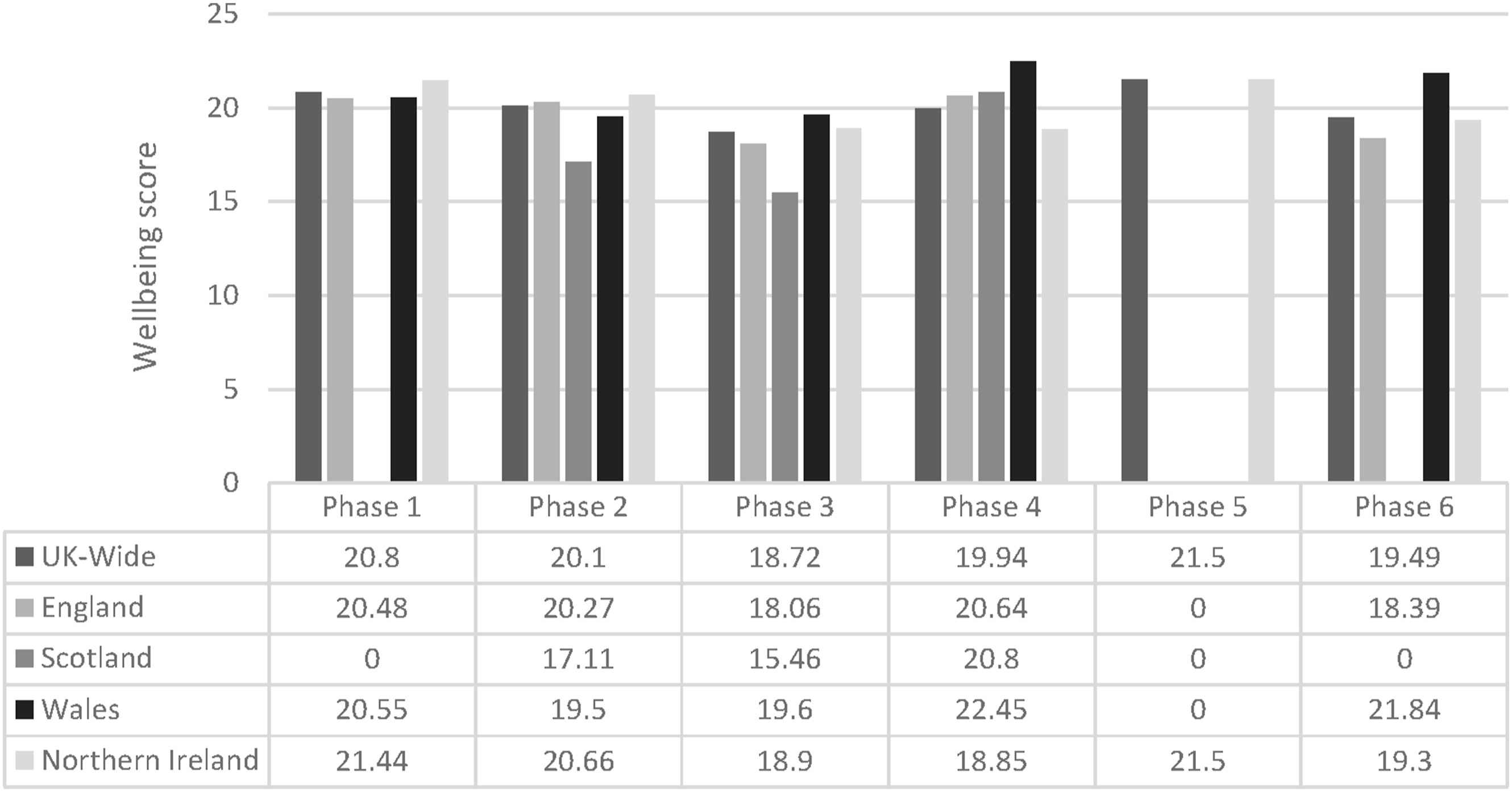
Logistic regression. Mental wellbeing on intention to leave social work.
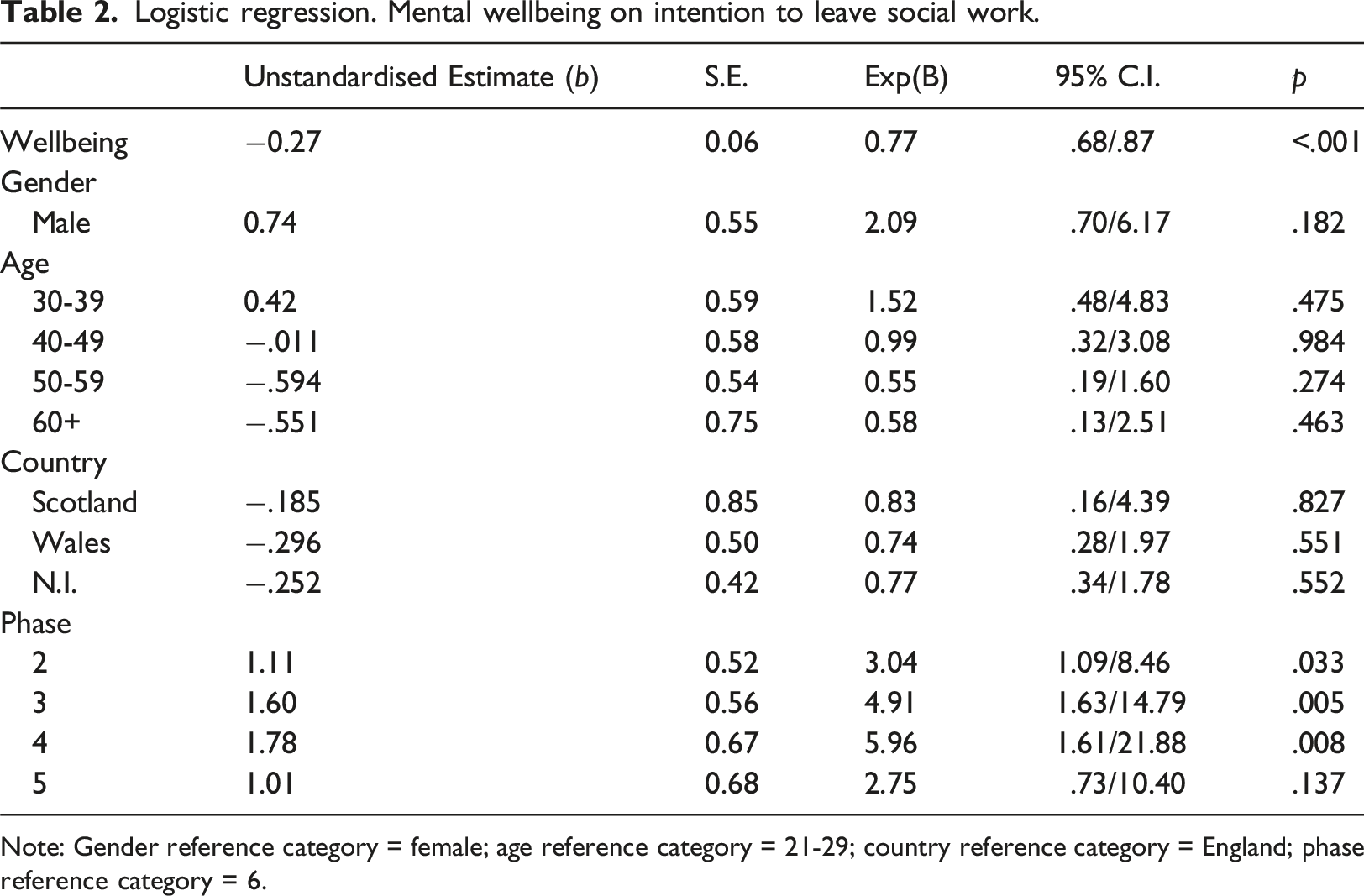
Note: Gender reference category = female; age reference category = 21-29; country reference category = England; phase reference category = 6.
Thematic analysis
Qualitative analysis, themes.

Changing working conditions
Some of the qualitative data are presented here to illustrate the impact on the pandemic on respondents’ work, often in relation to the move to home from office working and stopping home visits to service users other than in rare circumstances. As one respondent (177; P3, female, 40-49, community-based, England) observed, ‘I miss seeing my allocated cases’. Another (155) noted that practice with people with learning disabilities in particular, was often helped by face-to-face encounters rather than online contact: I have found it very frustrating not being allowed to visit service users, I do my work by phone, and I feel that a lot can be missed when talking to people, i.e. facial and body language can tell a lot especially with people with learning disability. They can have difficulties communicating and if not seeing a person (social worker) they need someone to be with them to pass on how they are feeling, the things they miss, things that are important to them. On a positive note, I have taken the time to read their history, and to really listen and hear what they say and/or their carers say (155; P2, female, 21-29, community-based, NI).
Some reported that the impact of social restrictions on their clients’ social networks was profound, especially if they had little other support. It was not simply that formal or paid services such as day centres had been shut but that voluntary and community groups also had to suspend their activities. Respondent 141 outlined the difficulties of severe and sudden changes to social networks and routines which meant substantial administrative work trying to find some service or support that might be available to service users in the new context: It’s been so difficult to see those we support have little else around them with all their social activities/groups and days services closed. Every phone call or meeting with a service user ends up being a new package of support therefore a new assessment, care plan, panel application. The paperwork is never ending. It’s been so difficult doing assessments over the phone or Teams when they have a disability and can struggle to communicate. As there is little third (voluntary) sector support about, more people are looking to social care for support, when in “normal” times they would not meet criteria for support as it would be provided elsewhere (141; P2, female, 21-29, day care, Wales).
Social work was the main human service profession to move from office to home working in the UK (Baginsky and Manthorpe, 2020; UNISON, 2022). Those working with people with learning disabilities shared similar experiences and feelings about this move with other social workers, providing various comments about good or bad managerial support, general positive views about the availability of IT and equipment for them, and reflections on the difficulty experienced by some of managing their work/life balance, particularly if they were juggling child/family care and work. Across the profession positive points were made about talking to colleagues, working with other agencies and practicing some self-care by taking breaks and seeking support. However, there were some differences in emphasis among the learning disabilities group in terms of the pandemic’s impact on learning disability community-based services (many were closed) and the consequent effect on their communications with people with learning disabilities and their families. As two respondents admitted, they felt personally stressed by enquiries they could not resolve: In relation to my role, I found the most difficult the lack of information to those working on the ground. As we are the contact person for the service user and their family we are contacted regularly regarding questions about the reopening/closing of services however, it felt that we had little information to share with the families. This had an emotional impact on workers such as feeling helpless but also emotionally draining as each call was emotion and stress filled and we felt we had no resolution to offer (153; P2, female, 21-29, community-based, NI). One of the biggest problems for us is the constant staff absences due to stress, psychosomatic stress, isolating, childcare whilst trying to provide a day service. Also, the level of stress trying to accommodate the most needy and vulnerable service users and realising the difficulty of not or providing only a limited service. A small number of carers have presented (us) with a legal challenge to the partial closure of day care which has been very difficult for staff trying to do their utmost best (156: P2, female 60+, day care, NI).
Intentions to leave
For respondents who commented on intentions to leave, a variety of reasons were provided. Some had considered moving jobs but thought that any form of social work would be as stressful (285; P6, female, 50-59, community-based, England). Some were considering early retirement (159; P2, female, 50-59, not specific location, NI), others had intentions to leave ‘before it gets any worse’ (284; P5, female, 50-59, day care, NI). While some valued social work’s job security (92; P2, female, 50-59, not specific location, England) others commented that leaving seemed impossible owing to geography. Even among those new to the profession there were indications of thinking of moving on: ‘I am newly qualified, but I have had difficulties coming to terms with knowing this will be my work life for a long period of time, if not forever’ (241, P4, female, 21-29, community-based, Wales).
Discussion
Our analysis of the responses from social workers working with people with learning disabilities chimes with other UK reports of social workers’ reactions to the pandemic and their working experiences (see Foley and Foster 2022). Their responses were similar in terms of wellbeing and changes to working life to those of other UK social workers in our wider study. Our hypothesis that their wellbeing would decline as the pandemic progressed was partially upheld but the upturn after P3 may indicate that the lessening of social restrictions affected their client group positively and thereby their own feelings and work pressures.
It may seem surprising in light of the profound impact of the pandemic on people with learning disabilities and their carers in terms of mortality and wellbeing that the learning disability respondents had similar levels of reduced wellbeing and intentions to leave their profession as other areas of practice such as children’s services (McFadden et al., 2023b) and older people (MacLochlainn et al., 2023) The overall picture is that of a profession that generally moved rapidly from office to home working and increased its online and telephone communications with colleagues, other agencies, service users and carers. The profession had assurances that it was in accord with the ethical framework for practice with adults (BASW, 2020) and this is likely to have informed their activities directly or indirectly in terms of reducing risks of virus transmission among their vulnerable client group. That our respondents were able to withdraw from much face-to-face contact reflects the structure of much UK social work during the pandemic. Other services, for example, social care direct support and personal contacts for adults, and the primacy of health and education services for children and young people with learning disabilities, often needed to maintain direct contact. This was reflected in our study’s responses from social care practitioners such as those working in care homes. None of our respondents reported holding a role similar to that of a named social worker (James et al., 2018) with the implications of high levels of contact which such a restricted caseload might imply. A minority who had face-to-face contact prior to the pandemic, for example, in a day service, moved to home working, which impacted on routine face-to-face interactions. Contact with family and some service users was reported as personally stressful by some who felt unable to change social restrictions or resolve pandemic uncertainties. Difficulties in communications that were not face-to-face were reported but not confined to this service user group.
Regarding support from managers and employers this was variably experienced. There are several implications overall for employers in terms of changing this variability and, of course, in planning for emergencies. The lack of planning by English local authorities and social care services for a pandemic or similar crisis necessitated rapid responses (see Baginsky et al., 2023) and this was indirectly acknowledged by a few of our respondents as a continued source of stress or irritation in terms of lack of access to resources such as Personal Protective Equipment.
It is important to note what we did not find referenced to in the data. We found no mention of consulting specific guidance such as the ethical framework for social care (BASW, 2020) as helpful or otherwise and none of the specific legal guidance for mental health, learning disabilities and autism, and specialist services (NHS England 2020) produced for social workers as well as other professionals. Qualitative research would be helpful in asking about these resources directly to assess whether such publications are used and by whom. Other studies have focussed more on specialist services, such as schools, where social workers are not the major professional group, whose staff reported major challenges in maintaining school activities from wider social restrictions (Challenging Behaviour Foundation 2021). However, our respondents seemed to have more casework concerns, often about their administrative work in revising assessments, care plans and budgets. It may be surprising to some that the learning disability respondents felt as overwhelmed than those working with children in our wider survey (McFadden et al. 2023a), but the reasons for this may not relate to the service user or client group. In any event, if this translates to exit from the profession, there may be shortages of learning disability experience to inform holistic social care assessments and imaginative planning and to educate future cohorts. The Local Government Association (LGA) foresaw the importance of retaining and employing specialist staff trained to work with people with learning disabilities early in the pandemic (LGA 2021) and specific efforts might need to be developed to attract new recruits or encourage existing social workers to transfer to this area of practice.
Strengths and limitations
This study reports on a specific professional role that has been under-explored in relation to the COVID-19 pandemic. Data were collected over six phases from 2020-23 and were mixed methods, allowing for standardised measures of wellbeing and intention to leave as well as qualitative more in-depth information about social workers’ views during the pandemic. There are limits to the study from the small numbers overall and declining numbers of respondents. While this was a UK wide survey, by P4, P5 and P6 the numbers of learning disability social workers participating had reduced considerably (in P5 all were from NI). Comparing findings between different phases proved difficult due to sampling bias and therefore was a limitation of this study. A further potential limitation was convenience sampling using online recruitment via Twitter/X and Facebook as well as professional networks which may increase the risk of bias. In the context of the pandemic however, it reached respondents who would have been practically difficult to access otherwise in real time during the various time-periods of the pandemic. Collecting cross-sectional data at each phase of the study was a further decision based on practical considerations. The study design also offered anonymity.
Conclusion
Our study provides an evidence-base to inform retention policies in learning disability social work for workforce planning and efforts to stabilise this sector and retain vital experience. The quality of services and safeguarding needs of people with learning disabilities, their carers and families, have been notoriously neglected as evidenced in criminal proceedings and convictions relating to high profile Serious Case Reviews such that of as Winterbourne View Hospital and others (Manthorpe and Martineau, 2015). Future research on social worker wellbeing in learning disability services should aim to examine factors which would retain staff and implement those with the most persuasive evidence. Sustaining high-quality experience in learning disability social work is critical to maintaining an empowering human rights approach for social work interventions for this essential service.
Footnotes
Acknowledgements
We thank all who participated in this research. The views expressed are those of the authors and not necessarily those of the funders.
Authors’ contributions
All authors contributed to the study conception and design. Data analyses were performed by Justin MacLochlainn (JML) and John Mallett (JM). The first draft of the manuscript was written by JillM, Paula McFadden (PMF) and JML all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Health and Social Care Research Division (HSC R&D Division) of the Public Health Agency, Northern Ireland (COVID Rapid Response Funding Scheme COM/5603/20), the Northern Ireland Social Care Council (NISCC) and the Southern Health and Social Care Trust and funding from England’s National Institute for Health and Care Research (NIHR) Policy Research Unit in Health and Social Care Workforce-PR-PRU-1217–21002.
Ethical statement
Institutional review board statement
Ethical approval was attained from the Research Ethics Filter Committee of the School of Nursing Ulster University (Ref No: 2020/5/3.1, 23 April 2020, Ulster University, IRAS Ref No. 20/0073) for the study and Trust Governance approval (for Northern Ireland only) was gained from the Health and Social Care Trusts for Phase 2. Permission for the use of the scales used in the questionnaire was provided by the original authors, and consent and confidentiality were addressed in Participant Information Sheets provided at the start of the survey.
Disclaimer
The views expressed are those of the authors and not necessarily those of the funders, or the NIHR or Department of Health and Social Care.