
Abstract
Keywords
Introduction
Challenging behavior occurs in approximately 10–15% of people with an intellectual disability, with severity and frequency increasing with the severity of the intellectual disability (Holden and Gitlesen, 2006). The concurrence of severe to profound intellectual disabilities and persisting challenging behavior results in a vulnerable group of people with intense and complex support needs which vary strongly within and between clients (Dutch National Disability Care [VGN], 2014). They experience limited intellectual and communicative abilities, which means that they need intensive guidance in their lives.
These support needs are often difficult to interpret and meet due to the communicative difficulties that are associated with the severity of the intellectual disability and challenging behavior, and common comorbid challenges (e.g. autism, hypersensitivity to stimuli, psychological or psychiatric problems; Schuengel et al., 2010; VGN, 2014). To experience well-being, people with severe to profound intellectual disabilities and challenging behavior are highly dependent on the support of professional caregivers. Enthusiastic and professional supervisors, family and other stakeholders commit themselves every day, despite and thanks to the complexity that these people entail. The guidance of these people requires a continuous quest that requires the dedication, wisdom, knowledge and expertise of all involved.
High-quality interpersonal relationships between staff and clients are essential to the quality of this support as well as to clients’ quality of life (Hermsen et al., 2014). However, little is known about factors that promote building high-quality interpersonal relationships between staff and people with severe to profound intellectual disabilities and challenging behavior.
High-quality interpersonal relationships can be characterized as secure attachment relationships in which clients use others as a secure base and safe haven to pursue a feeling of emotional security and well-being (Schuengel et al., 2010). Although discussions on attachment are often limited to early childhood, people seek support from attachment figures from early childhood to old age (Schuengel et al., 2010; Schuengel and Van IJzendoorn, 2001). Actually, adults with severe to profound intellectual disabilities are highly dependent on the support from attachment figures to experience well-being throughout life (Schuengel et al., 2010). People with severe to profound intellectual disabilities are less adept to cope with stressful situations, and without the support of important others stressors often result in challenging behavior (De Schipper and Schuengel, 2010; Janssen et al., 2002). The level of cognition plays an important role in the development of attachment relationships. Due to the low level of cognition and associated complex life histories of people with severe to profound intellectual disabilities (e.g. overstrained parents, institutionalization, lack of continuity), they are at risk of developing insecure attachments in childhood, putting people at risk for developing challenging behavior and complicating interpersonal relationships later in life (Janssen et al., 2002). For people in residential settings, access to common attachment figures, such as parents or friends, is often limited. According to attachment theories, people will seek for support from new attachment figures when experiencing a long-term unavailability of existing attachment figures (Schuengel and Van IJzendoorn, 2001). Accordingly, people with severe to profound intellectual disabilities and challenging behavior in residential settings are predisposed to display attachment behaviors towards staff (Janssen et al., 2002; Schuengel et al., 2010), such as monitoring the staff’s availability and seeking support under stress (De Schipper and Schuengel, 2010). Nonetheless, building secure attachment relationships is complicated by the often subtle, difficult-to-interpret cues used by people with severe to profound intellectual disabilities to communicate (emotional) needs and responses (Janssen et al., 2002; Schuengel et al., 2010). To perceive and interpret cues correctly and match support efforts to clients’ needs, staffs’ interest, sensitivity and attunement are key to build interpersonal relationships (Reinders, 2010).
People with severe to profound intellectual disabilities and challenging behavior experience significant challenges in relation to communication. They experience restraints in speech and communication at pre-symbolic or proto-symbolic levels (Bellamy et al., 2010; Iacono et al., 2009; Maes, et al., 2007). The development of communication is important to understand challenging behavior. From unintentional and intentional non-symbolic communication, communication progresses to language. Learning to communicate is influenced by children participating in play, interactions with other children, interactions with adults through daily routines, and activities that are repeated over and over. Children with disabilities often have difficulty with many of these things. They are often not provided with as many opportunities to engage language and communication rich environments as their peers without disabilities. Children with severe cognitive deficits may not have the cognitive abilities to become symbolic communicators independently, and may remain dependent on non-symbolic behaviors such as crying, facial expressions, or problematic behavior such as hitting to communicate (Chatwick et al., 2018).
Besides the level of cognition of people with severe to profound intellectual disabilities, clients’ severe and enduring challenging behavior has been shown to impact interpersonal relationships. On the one hand, the unpredictable and/or negative client reactions to staff behavior hinder meaningful interactions (Willems, 2016). On the other hand, poor staff-client interactions have been mentioned as important correlates of the origin and maintenance of challenging behavior (Hastings and Remington, 1994). It has been generally acknowledged that challenging behavior results from the interplay between individual and environmental factors (Hastings et al., 2013). That is, the (mis)match between personal capacities or disabilities and environmental possibilities or demands impacts the occurrence of challenging behavior and challenging behavior is often a way of communicating a mismatch (Nijs et al., 2019). Staff behavior can contribute to managing as well as triggering or maintaining challenging behavior. The impact of intrapersonal (e.g. attributions, attitudes, emotions), interpersonal (e.g. client behaviors) and environmental factors (e.g. team climate) on staff interpersonal behavior have been extensively studied (Van Den Bogaard et al., 2019; Willems, 2016). For people with severe to profound intellectual disabilities, interpersonal relationships with staff are essential to prevent harmful situations following challenging behavior to people with severe to profound intellectual disabilities themselves or others, and to prevent challenging behavior from severely diminishing the quality of life of these people.
In previous research on how to support people with intellectual disabilities and challenging behavior, clients have consistently indicated the importance of a good relationship with staff (Dodevska and Vassos, 2012; Griffith et al., 2013; Nijs et al., 2019; Roeleveld et al., 2011; Van Den Bogaard et al., 2019). In a study by Nijs et al. (2019) exploring aspects to improve residential support, people with intellectual disabilities even assigned the highest priority to establishing high-quality relationships with staff. Besides people with intellectual disabilities and challenging behavior themselves, their parents as well as staff members have expressed the importance of positive staff-client relationships (Hermsen et al., 2014; Nijs et al., 2019; Sohier et al., 2011). Qualities that were highly valued in the relationships included trust, respect, sincere interest and attention, a balance of power, and acknowledgement of one’s possibilities and needs (Dodevska and Vassos 2012; Griffith et al., 2013; Hermsen et al., 2014; Nijs et al., 2019; Roeleveld et al., 2011; Sohier et al., 2011; Van Den Bogaard et al., 2019).
It is clear that interpersonal staff-client relationships are particularly important for people with severe to profound intellectual disabilities and challenging behavior to experience well-being; unfortunately, these people are at high risk of lacking such relationships and the residential settings most clients reside in form risky environments to build interpersonal relationships due to staff’s high workload, work schedules and turn-over (De Schipper and Schuengel, 2010; Schuengel et al., 2010). Several studies have reported shortcomings in staff-client interactions in people with severe to profound intellectual disabilities and challenging behavior, including a lack of responsivity to clients’ needs and abilities (De Waele and Van Hove, 2005; McConkey et al., 1999); a focus on practical and physical care (De Waele and Van Hove, 2005); and a low level of staff contact (Mansell et al., 2001). The necessity to improve interpersonal relationships arises. Although previous research has indicated some important aspects of relationships between staff and people with an intellectual disabilities and challenging behavior, the specification to people with severe to profound intellectual disabilities is essential as the level of cognition plays an important role in establishing interpersonal relationships. In addition, a focus on factors that affect relationships specifically rather than aspects of good support (staff) in general is essential to promote building high-quality interpersonal relationships. The present study explores the perspectives of professionals and relatives on what affects interpersonal staff-client relationships in people with severe to profound intellectual disabilities and challenging behavior.
Methods
Approach
Design
Focus groups and individual interviews were combined. The qualitative method triangulation contributes to the richness of the data by generating complimentary views on the research topic (Lambert and Loiselle 2008).
Participants
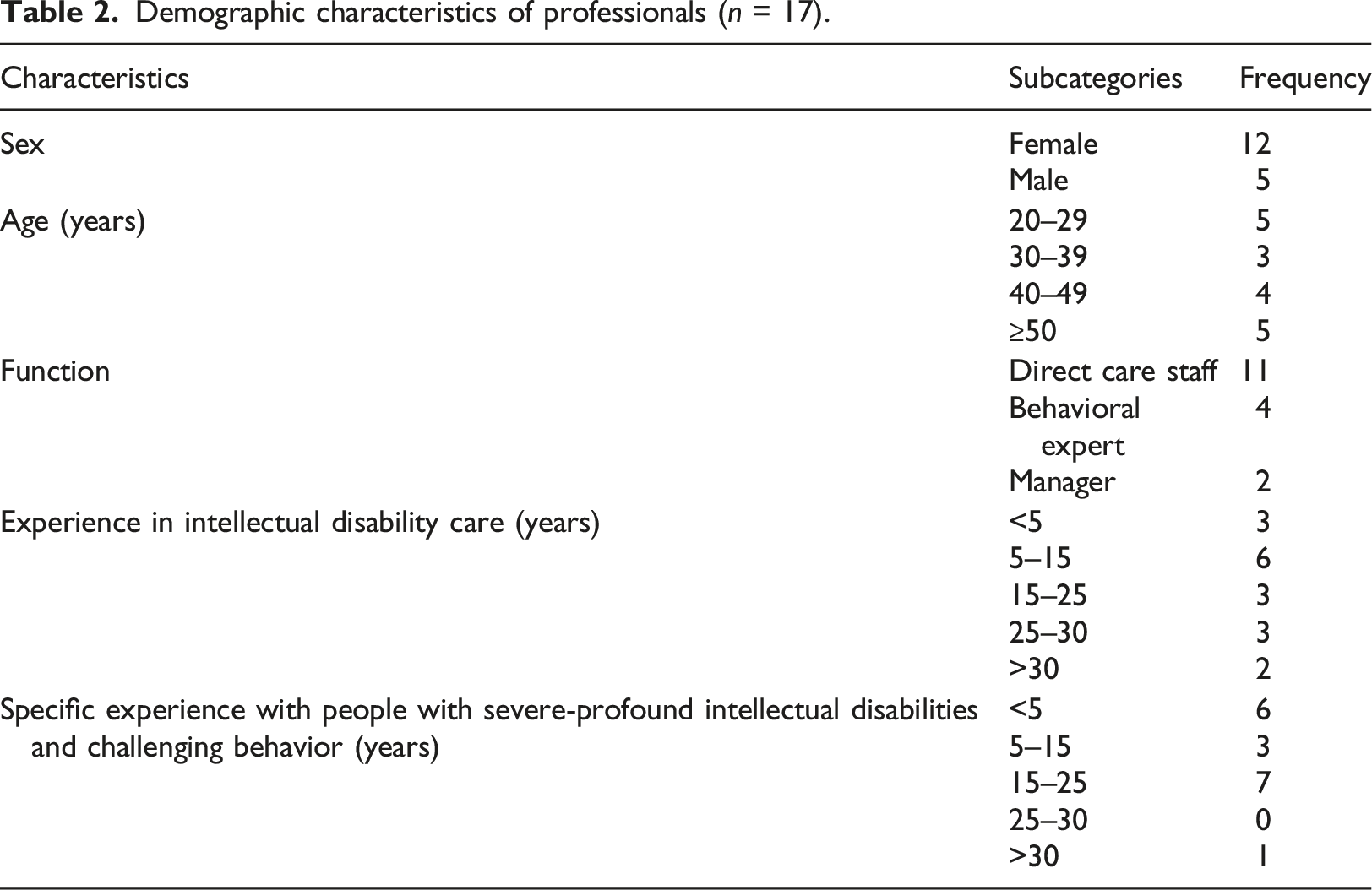
In total, 11 relatives and 17 professionals employed at 11 Dutch residential care organizations took part in this study. Relatives included parents, siblings and a cousin. Professionals included direct care staff, behavioral experts and managers. In this research, we focused specifically on the perspectives of professionals and relatives because they play a role of importance in building interpersonal relationships and in interpreting symptoms and signs with regard to the wellbeing of their family member or client. Relatives and close professionals seem the preferred persons to respond on behalf of the client or family member. The group findings have been approved by means of an advisory board of relatives and professionals.
Demographic characteristics of relatives (n = 11).
Demographic characteristics of professionals (n = 17).
Data collection
Three focus groups were conducted in May-June 2019. The focus groups took place at three locations in the south, east and middle of the Netherlands. The focus groups were heterogeneous, ranged in size from 7 to 10 participants, and included a total of 17 professionals and seven relatives. There were too little people willing to participate in a focus group in the north of the Netherlands, and professionals were overrepresented within the focus groups compared to relatives. Three additional semi-structured telephone interviews with four relatives (in one interview both the mother and father of one person participated) living in the north of the Netherlands were conducted in September-October 2019.
Procedures
A co-researcher with a mild intellectual disability contributed to the preparation, execution and analyses of the focus groups. The co researcher was recruited through his work in the clients-participation-council of one of the participating organizations and because of his former experience in contributing in research projects. The research team was trained in the so called CABRIO training. In this training we learned from doing research as a joint learning route. We were coached as inclusive team in organizing collaboration in the different stages of our research project.
The co-researcher had some experience in conducting scientific research by being an advisor in a previous research project, and had aspirations to develop his research skills. First, the co-researcher and the first author got to know each other and shared expectations and objectives regarding the research project. Thereafter, they discussed the focus group method and which role during a focus group would fit the co-researcher’s skills and preferences. Next, they discussed which questions were important to include in the focus groups and interviews. A semi-structured interview guide was developed, which was evaluated in a meeting including the other members of the research team (MH, HvV, AP, LR). The interview guide was used for both the focus groups and the interviews and included the following main themes: 1) experiences with high-quality staff-client relationships, 2) factors facilitating and hindering interpersonal relationships, and 3) essential staff skills to build interpersonal relationships. The focus groups started with each participant sharing an example of a high-quality staff-client relationship they had experienced. For the second and third theme, participants first thought about the subject themselves and wrote important factors down on a post-it note. Subsequently, the factors were divided in facilitating and hindering factors and discussed within the group. Participants of the interviews shared personal stories and examples of their relative regarding the three themes. Focus groups were moderated by the co-researcher and two alternating teacher-researchers 1 with experience in managing group discussions. The teacher-researcher asked the main questions from the interview guide and the co-researcher stimulated participants to explain and elaborate stories when necessary. The first author acted as an observer for group dynamics and non-verbal communication and managed the time. The interviews were conducted by the first author via telephone due to geographical barriers to conduct face-to-face interviews. Focus groups lasted approximately 2.5 h, and interviews lasted approximately 45 min. The focus groups and interviews were audio recorded and transcribed verbatim.
Data analysis
A thematic inductive analysis was performed together with the co-researcher in the inclusive research team. Analysis was undertaken to identify patterns (themes) within the data using the software program ATLAS.ti 8 (Braun and Clarke, 2006). The focusgroups and interviews were audio recorded and transcribed verbatim. The analysis of the data was both inductively as deductively oriented. We analyzed in an interpretive way through the lens of the interview guide (top down) as well as bottom up from the collected data.
First, the researchers immersed themselves in the data by repeatedly examining the transcripts of both the focus groups and interviews. Second, significant statements within the data were assigned a code with the purpose of data reduction. Codes were derived from the data (i.e. inductive approach). Two authors (MS, LR) independently coded the transcripts and the co-researcher coded 25% of the transcripts supported by the first author. The co-researcher and first-author followed the following steps to code the data: 1) the co-researcher read a statement of a participant out loud and marked pieces of the statement that were important to the research question – the first author supported the co-researcher by explaining difficult pieces of text; 2) the co-researcher paraphrased the meaning of the statement and interpreted what the statement tells us about interpersonal relationships– the first author helped to bring his thoughts into words by asking questions and summarizing his interpretations; 3) the co-researcher assigned one or more codes to the statement to capture the meaning of the statement - the first author helped the co-researcher to create the codes. The three sets of initial codes were collated by discussion. Third, the codes were combined in (sub)themes by joint discussion sessions within the research team. Fourth, the research team refined and defined the (sub)themes. A member check was conducted by presenting the (sub)themes to participants as well as to an independent advisory board 2 consisting of five professionals, two relatives and one teacher. No one of the participants of the advisory board had substantive additions. To increase the trustworthiness of the results, we used an interview guide. The focusgroups were moderated by the researcher, co-researcher and two teacher-researchers. The evaluation moments at the end of each meeting were also recorded and transcribed.
Findings
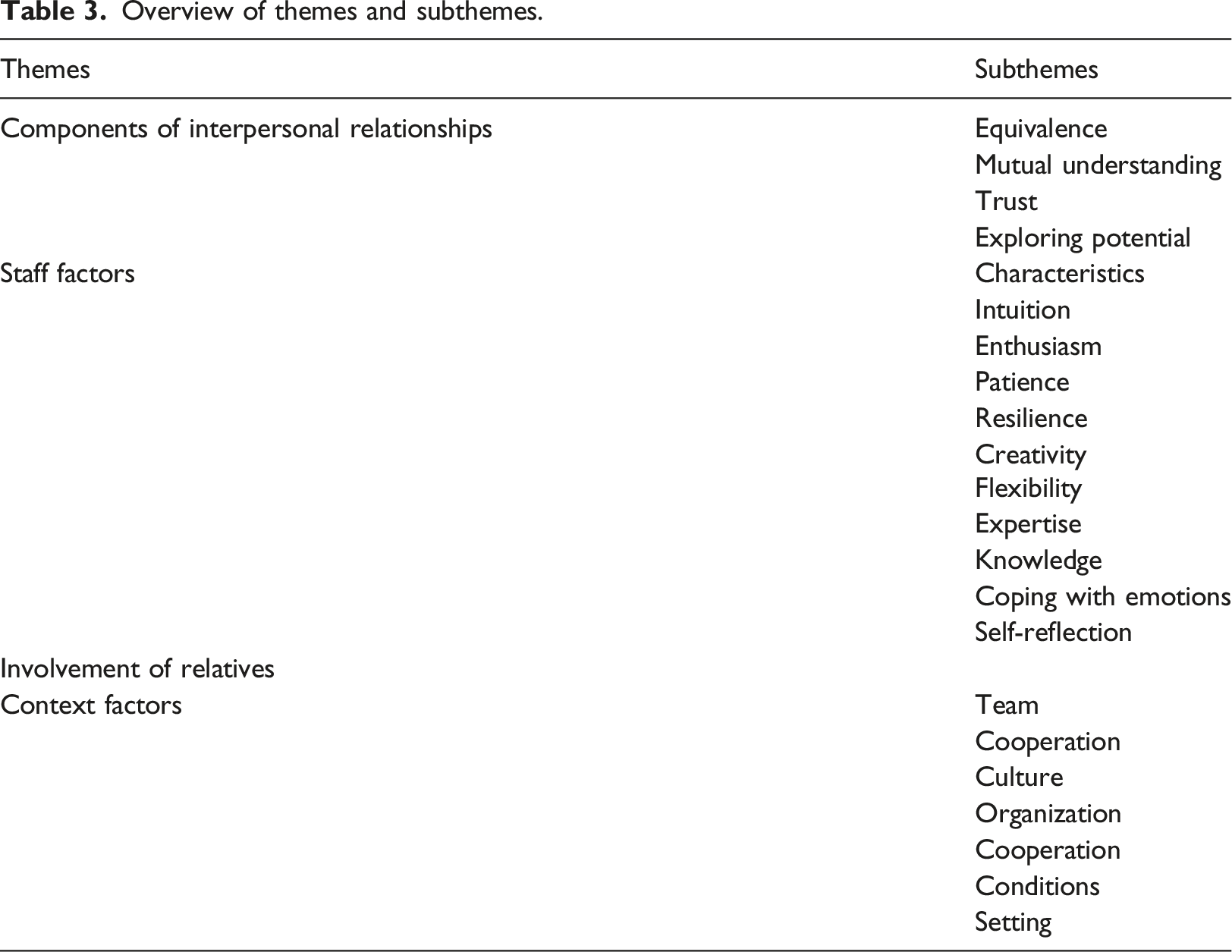
Overview of themes and subthemes.
Theme 1: Components of interpersonal relationships
The first theme describes four components that constitute high-quality interpersonal relationships in people with severe to profound intellectual disabilities and challenging behavior according to the participants, including equivalence, mutual understanding, trust, and exploring potential.
Equivalence
Participants emphasized the importance of equivalence in staff-client relationships as opposed to compulsion, power or coercion. Equivalence is characterized by staff that treat clients as human beings with common human needs, by respect and acceptance, and by attending to clients’ positive aspects (e.g. giving compliments). Following clients’ challenging behavior, attending to positive aspects includes not focusing on clients’ behavior, or giving a neutral reaction when behavior requires attention, while simultaneously focusing on more positive things, rather than controlling behavior by coercion or restricting freedom. Until a year ago, staff mainly focused on stopping the behavior, by saying: ‘No, stop that, look at me’. Now we focus on drinking coffee, offering her a cup, rather than paying attention to the behavior. (F2, P)
Equivalence is enhanced if staff provide clients with more autonomy and look for opportunities to let clients make their own choices. Empty room, bolted bed, empty walls […]. We went to the store and let him choose stuff for his room with the idea that he would destroy it rather soon, as he did before with all decorations we chose. To this day, he never destroyed anything again. (F1, P)
For people with severe to profound intellectual disabilities and challenging behavior, autonomy only has a positive effect when choices are offered with clear limits and adequate support, and when choices fit clients’ capacities to reduce the risk of inducing stress and challenging behavior with offering choices that are too big or too small. She could always choose from two sets of clothes. But she started to act out in the morning. We decided to let her choose from the whole wardrobe, and it appeared she was perfectly capable of making that bigger choice! No more acting out in the morning. (F1, P)
Mutual understanding
According to the participants, interpersonal relationships are characterized by striving for mutual understanding between interaction partners. Even though (verbal) communication is difficult with the clients, staff continuously search for the meaning of clients’ communications and behaviors. These searches were often referred to as a ‘puzzle’ that takes time to find the pieces, met with enthusiasm and motivation when ‘a piece of the puzzle is completed’. In addition, staff try to communicate in ways that are understandable for a client by adjusting to clients’ abilities. For example, providing ‘subtitles’ of events in the environment, providing clients with sufficient time to process communication, and visualizing communication. Being explicit was important as well. ‘I’ll be right there,’ what does that mean? – But if you tell a client ‘I’ll be there in 5 minutes,’ that often doesn’t mean anything to them as well. – No, but you can be more explicit; for example, ‘We will leave when I finish my cup of coffee.’ (F1, P-R-P)
Spending (one-on-one) time together enhances mutual understanding by getting to know and understand each other. Participants emphasized the benefits of video interaction training to enhance understanding.
Trust
According to participants, trust is an essential component of interpersonal relationships. Trust entailed clients’ belief that staff proximity is continuously and unconditionally available, and that challenging behavior does not harm their bond. He knows he is not allowed to do something and may regret doing those things. It helps him to know that you are still there afterwards and can hug each other. (F1, R).
Staff may gain clients’ trust by offering proximity, especially when a client is anxious or insecure. While proximity enhances trust, a balance with offering space and privacy was crucial.
Exploring potential
Clients not merely have disabilities, but also have the potential to learn and develop. Recognizing clients’ capacities and potentials while guarding clients’ well-being and safety promotes relationships. Participants mentioned staff’s tendency to keep situations that are going well stable while adapting routines and taking risks are necessary to explore clients’ potentials. Staff tend to think ‘We found something that works, it is okay as it is’. But I think if you keep searching for their beautiful aspirations or desires, you will always find new things to stimulate them. (F1, P)
Importantly, it was only possibly to adapt routines in relationships build upon trust.
Theme 2: Staff factors
Participants described staff factors that enable staff to build interpersonal relationships with people with severe to profound intellectual disabilities and challenging behavior, which are divided into characteristics (personal traits) and expertise (competencies learned through training or experience).
Characteristics
Certain characteristics (i.e. personal traits) enable staff to build relationships with clients. Besides specific traits, staff’s intuition and instinct were important to build relationships.
First, enthusiasm and passion are essential. According to participants, intrinsic motivation is important to persist in relationships and showing sincere interest, empathy, and compassion promotes relationships. Without passion for those people, if you don’t do it with love, it seems quite impossible to me to get it [building interpersonal relationships] done. (I1, R)
Second, a patient nature enables staff to build relationships by following a client’s pace, not expecting too much, and noticing and appreciating very small successes. Getting to know a client and win their trust takes time. Clients’ contact initiatives or positive reactions to staff behavior following a long period of difficulties indicate that a relationship is being build. In addition, the process of learning new skills to clients is long with small steps, asking for a patient approach.
Third, staff’s resilience, described as the ability to let go and continue following a negative event, is an essential trait to build relationships. Keeping some professional distance, putting clients’ behavior into perspective, and not letting the behavior affect oneself too personally (e.g. believing that clients’ challenging behavior is not directed at oneself personally, not taking work home) are essential for enduring relationships. That is one of the hardest ones, I think, but very important. That a client knows that no matter what happens, you are available. […] You need to be able to let go and continue. (F1, P)
Fourth, creativity and humor are helpful to distract clients and avert an impending incident. Humor commonly involves ‘mirroring’ clients’ behaviors.
Fifth, staff’s flexibility enables interpersonal relationships. According to the participants, people with severe to profound intellectual disabilities and challenging behavior are characterized by large interpersonal and intrapersonal differences. Therefore, being able to let go of routines and agreements when necessary, and adjusting behavior and activities to differences in abilities, needs and preferences within and between clients are necessary to build relationships. Sometimes the client completes 80% of a task, while on bad days the client does 10% and we do 90%. […] For example, when we are doing the dishes, he might only touch the plate and I put the plate in the dishwasher, but we will always perform the task together. (F1, P)
Expertise
Expertise includes staff members’ professional competencies acquired during training and on the job that facilitate relationships. First, general knowledge about clients with severe to profound intellectual disabilities and challenging behavior, according to participants mainly concerning (potential discrepancies between) social-emotional and cognitive development and additional problems (e.g. autism or attachment issues), promotes relationships. Theoretical underpinnings of why something is effective help staff to translate successes to other situations and clients, and to understand and accept clients’ behaviors. Moreover, knowledge about an individual client (e.g. life histories, interests, support agreements) promotes relationships. A professional staff member keeps developing knowledge and skills and is open to others’ feedback.
Second, vulnerability and sincerity, which involve acknowledging emotions to oneself, colleagues, and clients, enable staff to build relationships. Participants described that negative emotions (e.g. anxiety, insecurity) are common in staff supporting the clients. While negative emotions could complicate relationships if they hinder staff from offering proximity or when clients take over staff’s negative emotions, emotions mainly hinder relationships when staff does not effectively cope with emotions. On the one hand, effective coping strategies include acknowledging emotions, guarding personal boundaries, and asking colleagues for support. On the other hand, being straightforward and showing emotions towards clients is important, as clients have a great sense of others’ emotions. When a staff member is not sincere, a client is unable to trust him. Nevertheless, clients cannot cope with intense staff emotions. Establishing clear boundaries with clients can help to restore a situation; if this is not possible, a colleague should take over. I think it is a good thing to tell them how you feel, not pretend, and set boundaries. Enough is enough. Now we move on. (F1, P)
Whether staff is able to show vulnerability and cope with emotions is, besides staff’s professional stance, to a great deal dependent on team culture (see team factors).
Third, expertise includes staff’s ability to self-reflect. Participants stated the importance of knowing yourself and reflecting on your actions when building relationships with clients. A professional staff does not just act out of impulse but reflects on the impact of his behavior, emotions and values. Participants noticed the benefits of video interaction training to promote self-reflection.
Theme 3: Involvement of relatives
Participants advocated the importance of involving relatives to build interpersonal relationships. Relatives may help staff to get to know and understand clients and make care decisions, as they have insights in clients’ needs and the meaning of their behaviors. Their knowledge about a client’s life history can be of great importance and triggers for challenging behavior might be found in past events. He likes bathing in the evening, but he was tensed at first, which we didn’t understand. When I asked his sister, she told me they used to live in a farm with a very old bathtub which gave a small shock if the water level was too low. That used to scare him. (F3, P)
The reciprocity between staff and relatives was important as well. Sometimes, relatives help staff to understand a client while in other instances staff help relatives understand their family member. A reciprocal, positive collaboration between staff and relatives contributes to a positive atmosphere within a residence, promoting interpersonal relationships. Relatives may also be important advocates of clients’ well-being. We do not know her very well or visit her a lot, but we do make sure that the process goes well. Her caregivers ask us if they are doing a good job and discuss care decisions. Sometimes if they propose more pills or restrictions, we say: ‘That’s enough.’ And that is helpful, as they have to think again about how to support her. (F3, R)
However, relatives felt that some staff members think that input from relatives is redundant as staff members are ‘the experts’. Importantly, relatives differ in the extent to which they want to be involved. Relatives might be less involved due to experiences in the past. What they have been trough as a brother or sister.. There can be so much sorrow in those relationships that it might be broken for good. We can’t change the past, but we can take it into account in the way we approach relatives. (F3, P)
Staff may engage relatives by actively inviting them to contribute to care decisions, by being aware of making requests that might be too demanding, and by expressing appreciation regarding relatives’ support.
Theme 4: Context
Participants discussed factors in teams, organizations and settings that affect relationships.
Team factors
First, successful teams have a common vision and support clients in a similar manner. According to the participants, predictability is important to people with severe to profound intellectual disabilities and challenging behavior to engage in interpersonal relationships. Clear routines enhance predictability (e.g. consistency among different staff members in performing daily tasks like tooth brushing). In addition to these routines, challenging and meaningful activities are important, as a lack of stimulation may trigger challenging behavior and hinder relationships. Nevertheless, too many or overly strict agreements hinder relationships. Successful teams enable staff to be flexible when an agreement does not fit the momentary capacity or preference of a client. Support agreements should be adapted to match clients’ needs; it hinders relationships if agreements are changed for the staff’s own benefit or to address practical issues. Moreover, successful teams appreciate staff’s personal input.
You are more than just a caregiver, you also have your talents. For example, you are athletic, creative or like gardening. You should be able to put that in your work, your authenticity. To be allowed to be yourself. (F3, R)
Second, successful teams have an open culture in which staff members can openly express emotions, set boundaries and ask for support from colleagues and supervisors. Support entails exploring what someone needs to cope with emotions and taking over from others when personal boundaries are reached. In closed ‘macho’ cultures, teams interpret negative emotions as a failure, hindering effective coping and therewith relationships. Everyone is afraid at times. There used to be a macho culture; it was cool to say that you were not afraid. But staff should be open about anxiety. If you dare to acknowledge emotions, you can cope with them. Thus, I think anxiety as such does not hinder staff. But what do you need? And are your emotions acknowledged and accepted? (F2, R)
In addition, in open team cultures there is room for mistakes and to learn from one another without criticism, enabling staff to explore clients’ potential.
Organizational factors
Organization-wide cooperation enables relationships, including a common vision and communication between managers, day-care centers and residences, as well as organization wide support for staff to cope with emotions following an incident of challenging behavior. In addition to cooperation, participants considered several boundary conditions in organizations affecting relationships. First, frequent staff changes decrease clients’ feeling of trust and hinder mutual understanding. Second, while money was mentioned as a prerequisite for adequate support, participants noted that money is not essential to stimulate staff approaches that promote relationships. Third, time pressure hinders relationships, for example due to administration or staff shortages. Staff should be able to follow a client’s pace rather than being imposed a strict time planning. In the morning, we let go of time. […] The client’s pace leads rather than the clock in caretaking. But that means that you have to cooperate with the day care center, that they will welcome clients at any time. (F1, P)
Moreover, enough time for a client to get to know and trust new employees and for staff to transfer knowledge to new colleagues is important to building relationships.
Setting
Participants discussed the importance of predictable environments to interpersonal relationships, affected by group composition and -size. That is, groups of approximately four clients who get along improve predictability and tranquility in residences. Nevertheless, clients with similar problems often live together as support needs are similar while people with severe to profound intellectual disabilities and challenging behavior create a lot of stimuli and do not handle stimuli well themselves, causing unpredictable environments and thus hindering relationships. In addition, interior and atmosphere affect opportunities to build relationships. Interiors should only deviate from other people’s living standards to benefit clients’ needs. Organizations should consciously consider what benefits a client could gain from adaptations in the environment. We ordered a new closet, so we’ll put locks on it.’ Well, that is not always necessary. […] Of course, some doors are locked in residences for safety or clarity. […] But, for example, toys, why should those be locked away? I don’t have to ask for everything I want, do I? And what is the worst that can happen? That the toys will be spread around the room. Well, then you should tidy up a bit. (F1, P)
Discussion
The present study reports the perspectives of professionals and relatives on what affects interpersonal staff-client relationships in people with severe to profound intellectual disabilities and challenging behavior. The research makes implicit, practice-based knowledge of professionals and relatives explicit and scientifically underpinned. A thematic analysis of focus groups and interviews with professionals and relatives identified four principal themes: 1) components of interpersonal relationships, 2) staff factors, 3) involvement of relatives, and 4) context.
First, according to the participants, high-quality interpersonal relationships between staff and people with severe to profound intellectual disabilities and challenging behavior constitute the following components: equivalence, striving for mutual understanding, trust, and exploring clients’ potential. While equivalence was an important aspect of interpersonal relationships, previous research has shown that people with severe to profound intellectual disabilities and challenging behavior experience more coercive staff behavior and less autonomy than do clients with less severe intellectual disabilities or without challenging behavior (Knotter et al., 2013; Stalker and Harris, 1998; Stancliffe, 2000). Therefore, attention to equivalence is warranted. Knotter et al. (2013) showed that coercive staff behavior and restrictions on clients’ freedom are mainly determined by contextual factors, and team cultures rather than individual staff factors should be targeted to promote equivalence. Opportunities for autonomy are small, banal and present in everyday choices (e.g. deciding how much to fill a cup of coffee, when to refill it or how many cups to drink) and the risk of overlooking these opportunities and focusing on the more substantial, bigger life choices (e.g. where or with whom to live) arises naturally (Finlay et al., 2008). As the results show that making choices can be stressful for clients, especially when they do not fit clients’ capacities, offering clear limits and support are prerequisites when pursuing autonomy. Accordingly, in accordance with Willems (2016), staff controlling and autonomy-giving interpersonal behavior should be balanced. In case of severe challenging behaviour or lower levels of intellectual functioning, professional long-lasting support has not been an autonomous choice of the person himself. This dependency means that professional caregivers need to be reliable for, sensitive and attuned to, compassionate with, and interested in the people they care for (Willems, 2016).
This compassionate and sensitive attitude means that a careful approach of the other person is necessary. Challenging behaviour can possibly be prevented or regulated by inviting the other to make his or her own choice e.g. the example of choosing from a whole wardrobe.
Second, staff factors included characteristics and expertise. The combination of characteristics and expertise enables staff to build interpersonal relationships. It is generally acknowledged that staff need training to provide adequate support (Van Oorsouw et al., 2013). Previous research has shown the potential of training to improve staff’s expertise, including staff’s knowledge (e.g. Lowe et al., 2006) and emotional intelligence (e.g. Zijlmans et al., 2011). While self-reflection has been shown to be the most influential psychological resources for staff interactive behavior (Willems et al., 2016), it has not been included in research regarding staff training (Van Oorsouw et al., 2013).
Third, the findings showed the importance of involving clients’ relatives when building relationships. Relatives are experts due to practical knowledge from their lifetime involvement with their family member (De Geeter et al., 2003; VGN, 2014). In past decades, the involvement of relatives has changed. Formal and informal care used to be strictly segregated and professionals were the experts, best informed to make care decisions. Today, families’ expertise is increasingly recognized and formalized in policies. Hence, staff’s professionalism includes cooperating with relatives. According to De Geeter and colleagues (2002), this cooperation includes ‘providing information’, ‘mutual decision-making’ and ‘keeping relatives up to date’. Additionally, the present study points out the importance of reciprocity between staff and relatives to promote staff-relatives and staff-client relationships.
Fourth, context factors included team, organization and setting conditions. From previous research, we know that team cultures have a stronger impact on staff-client interactions than do organizational cultures (Hastings, 2002). Knotter et al. (2013) showed that the impact of team factors is three times greater than that of individual staff factors when considering staff interactive behavior toward aggressive clients. In the present study, team cultures were particularly important for staff to cope with emotions. In accordance with Willems et al. (2016), an avoidance-focused coping style (i.e. seeking distraction or company with others) was identified as an effective way to prevent negative emotions from hindering relationships with clients. In accordance to participants’ views that coping with emotions is to a great deal dependent on team cultures, several studies have indicated that contextual factors, including a lack of support from colleagues and management, are more strongly related to staff well-being than is challenging behavior (Chung et al., 1996; Hastings, 2002; Robertson et al., 2005).
Study strengths, limitations and implications
A strength of the present study was its inclusive nature; collaborating with people with an intellectual disability is shown to promote the quality of research (Frankena et al., 2015). A co-researcher provides insights based on personal experiences with the issues explored. Previous research indicates difficulties for people with mild intellectual disability to empathize with people with more severe intellectual disabilities (Bigby and Frawler, 2010). At first, the co-researcher in the present study mainly applied the data to his own experiences, but he was able to empathize with people more severe intellectual disabilities and challenging behavior when encouraged by the academic researcher by the following steps: 1) the first author and co-researcher talked about the own experiences of the co-researcher, 2) the first author asked the co-researcher to think about how a similar situation would look like for someone with severe to profound intellectual disabilities and challenging behavior, and 3) the co-researcher read the piece of data again and tried to apply it to people with severe to profound intellectual disabilities and challenging behavior. The challenges in including the co researcher in the research team were the lack of time and rest in the cooperation. Researcher were not used to take time and to re consider the results again and again.
Besides, afterwards we should have taken more time to reflect on the specific talents and skills of the co researcher. He cooperated in the flow of the research team. Maybe we did not make use of all talents (Bigby et al., 2019).
While people with severe to profound intellectual disabilities and challenging behavior could not participate due to shortcomings in (communicative) skills to participate meaningfully in interviews (Stancliffe, 2000), relatives seem the preferred persons to respond on behalf of them (Andresen et al., 2001). However, the question remains to what extend the insights from relatives reflect clients’ experiences. Both agreement and disagreement between relative and client ratings have been reported (Stancliffe, 2000). It is recommended to explore methods to meaningfully include people with severe to profound intellectual disabilities and challenging behavior in scientific research. Time-consuming observational work is required, including dialogue and close cooperation with all communication partners (Chadwick et al., 2018). An example of a method used in practice that could be applied in research is ‘Talking Mats’ 3 ; a method using picture communication symbols to help clients with (severe) communicative difficulties to express their feelings about a topic. In addition, it is recommended to use communication passports with important information about the person with severe to profound intellectual disabilities which can be easily shared with other people (Goldbart and Caton, 2010). Other examples of methods which promote the communication are Intensive Interaction (Nind and Hewett, 2006) and cause and effect activities such as the use of switches (Mansell, 2010).
Focus groups and interviews were combined in the study design. While the triangulation of qualitative methods in a single design may be a topic of debate, it does contribute to the richness of the data by generating complimentary views on the research topic (Lambert and Loiselle, 2008). In the present study, focus groups provided an overview of factors that affect interpersonal relationships for people with severe to profound intellectual disabilities and challenging behavior; interviews provided rich and personal stories of individual clients, representing detailed examples and elaborations of some factors mentioned in the focus groups (that is the factors that were most important to the person that was the subject of an interview: the participants’ child or sibling). No factors were mentioned in the interviews that were not identified by the focus groups.
A limitation of the present study is that due to use of a convenience sample the possibility exists that the sample has particular characteristics. A purposeful sample would contribute to the scientific rigor and generalizability of future research. A great proportion of direct care staff with long-term experience was noticed in the sample (i.e. merely 3 out of 11 direct care staff had less than 5 years of experience), while the inclusion of relatively inexperienced staff members in future research might increase insights into building relationships with ‘new’ staff members. In addition we probably included care givers and parents who were (already) highly involved with the target group. This could interfere with the quality of the interaction. People who are less involved might experience more difficulties in building a good relation with a client. However they did not participate so we do not know if outcomes would be different with for instance less involved care givers.
Footnotes
Acknowledgements
The authors thank the participants for their time and energy and for sharing personal stories. We would also like to thank the members of the advisory board for their continued support throughout this and other projects.
Author contribution
All authors have contributed to, seen, and approved the manuscript and agree to the order of authors as listed on the title page.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ZonMw (The Netherlands Organisation for Health Research and development), under Grant 845004012.