
Abstract
People with severe/profound intellectual disability experience challenges in communicating and require their communication partners to adapt to their means of communication. Augmentative and Alternative Communication (AAC) is recognised as a potential means to meet their communication needs. Interventions need to be aimed at both the individual and their communication partners. We conducted a mixed methods systematic review of the literature to synthesise evidence on communication partners experience of communicating with adults with severe/profound intellectual disability through AAC. Eight publications met the inclusion criteria, they underwent thematic synthesis where four themes emerged. A shared commitment to communication partnership is fundamental for the effective and efficient use of AAC. However, there was a disconnect between communication partners perceptions of their roles and responsibilities. This review prompts further research to explore communication partners perceptions of their roles and responsibilities in the use of AAC with people with severe/profound intellectual disabilities.
Keywords
Introduction
Communication is a basic human need and human right (Williams, 2000). Communicating effectively is a fundamental life skill (Fulya Sen, 2015) central to most life activities and impacts the quality of life (QoL) of individuals (Bennett et al., 2016). Powell (2008) describes communication as a complex process that involves the interaction of the cognitive-linguistic and motor systems. Similarly, Friedman and McNamara (2018) describe communication as “a series of complex and fluid interactions” (p.111) inclusive of, but not limited to the use and understanding of facial expressions, body language, gestures, reading, writing, speaking and listening.
The terminology and definition of intellectual disability has evolved over time (Brady et al, 2016). These changes represent the move from a medical oriented approach to disability, to a more person-centred perspective, focusing on the individual and their interaction with their environment (Brady et al., 2016). There is agreement that intellectual disability is characterised by substantial limitations in intellectual functioning and adaptive behaviour originating during the developmental stage (ICD-11, 2022; Schalock et al., 2021a). The 11th edition of the International Classification of Disease definition of intellectual disability was used and should be taken to include all individuals with severe/profound intellectual disability, including those with profound intellectual and multiple disability, which is a term used to describe persons with severe to profound intellectual disability as well as substantial physical impairment (Lyle, 2019; Nakken and Vlaskamp, 2007). Individuals with severe/profound intellectual disability experience significant communication difficulties (van Der Gaag, 1998) which can impact their wellbeing and QoL and tend to communicate at the earlier developmental stages. Therefore, strategies must be provided to ensure their communication needs are met. The focus of this review is on individuals who communicate at earlier developmental stages. Therefore, persons with severe/profound intellectual disability and persons with profound intellectual and multiple disability were included. Terms such as profound intellectual and multiple disabilities, severe/profound intellectual and multiple disabilities and complex disabilities are used in the literature. For accuracy and to remain true to the original work, the terminology of cited authors is being used in this review.
Individuals with severe/profound intellectual and/or multiple disability tend to function at pre-intentional communication stage and may experience sensory and physical disabilities and health issues (Coupe O'Kane and Goldbart, 1998; Erickson and Quick, 2017; Sigafoos et al., 2021; van Splunder et al., 2006). Expressive communication tends to involve a range of subtle and idiosyncratic behaviours that may be individual to the person or context (Stillman and Siegel-Causey, 1989) such as eye gaze, body language and movements, changes in muscle tone, facial expressions, vocalisation (Brady et al., 2016; Coupe O’Kane and Goldbart, 1998; Parry Hughes et al., 2011; Petry and Maes, 2006). Their communication attempts can go unnoticed (Munde and Vlaskamp, 2015; Wilder and Granlund, 2003) or may be misunderstood (Grove et al., 1999). It is difficult to place meaning on an individual's communicative behaviour, especially when these are idiosyncratic and therefore, communication breakdowns are common (Keen, 2014; Sigafoos et al., 2021). Efforts must be taken to ensure an individual’s communication attempts are recognised and understood.
Communication partners need to be sensitive to individuals with severe/profound intellectual disability subtle behaviours to interpret these behaviours and respond, thus facilitating a two-way process of communicating (Coupe O’Kane and Goldbart, 1998). In the context of this review, communication partners include persons who have social relationships with AAC users (e.g., parents, siblings) and educational or care relationships with AAC users (e.g., teachers, health care professionals, residential staff members) (Kent-Walsh and McNaughton, 2005). Communication partners have a fundamental role in assessing adults with severe/profound intellectual disability. They observe and interact with the person over an extended time and across different environments. Such experiences enable them to share their knowledge of the person's abilities (Cascella, 2004). Acknowledgement that all people can communicate creates a sense of responsibility for everyone who interacts with persons with severe/profound intellectual disability to recognise and enhance the individual’s communication methods and opportunities (Brady et al., 2016).
The right of people with intellectual disability to have a means to communicate is recognised internationally (United Nations (UN), 2006). Augmentative and Alternative Communication (AAC) is recognised as one method of facilitating and supporting communication with persons with complex communication needs (Beukelman and Light, 2020). AAC is defined as “an area of clinical practice that addresses the needs of individuals with significant and complex communication disorders characterized by impairments in speech-language production and/or comprehension, including spoken and written modes of communication” (ASHA, 2019). Typically, forms of AAC are divided into unaided and aided forms of communication. Unaided communication includes gestures, facial expression, eye gaze, body postures and signs (Pino, 2014). Aided forms of communication include approaches which require some form of external support including physical objects or equipment such as symbol charts or books; it also refers to computer-based systems or Voice Output Communication Aids (VOCAs) (Pino, 2014). The goal of AAC intervention is to empower individuals to engage and participate in a variety of interactions and activities of their choice (Beukelman and Mirenda, 2005). However, learning to communicate through AAC is a complex process for both the AAC user (Bailey et al., 2006; Rackensperger et al., 2005) and their communication partners.
Given the complex communication needs of individuals with profound intellectual and multiple disability, it can be challenging to provide effective AAC interventions (Sigafoos et al., 2021). The four components of communicative competence for AAC users include linguistic, operational, social and strategic competence (Light, 1989; Light et al., 2003). Individuals who require AAC need support from their communication partners for successful communication as communication competence relies on both the AAC user and factors related to their communication partners and environment (Blackstone et al., 2007). Individuals are likely to interact with a range of communication partners, who have various roles in their lives (Kent-Walsh and McNaughton, 2005). Therefore, successful communication through AAC depends on both the individual and their communication partners using the AAC (Kent-Walsh et al., 2015). However, communication partners approach to communication may negatively impact upon AAC use. For example, communication partners have been found to control interactions, ask close ended questions, provide little opportunities for AAC users to start conversations or to respond and often interrupt the AAC users’ utterances (Blackstone, 1999; Light et al., 1985). In addition, and more generally, Bradshaw (2001) discusses how communication partners may overestimate their use of nonverbal communication and underestimate their use of verbal communication. Therefore, they may not adapt their communication to the individual’s understanding (Bradshaw, 2001). Attitudinal barriers where people presume individuals with complex communication needs cannot learn to use AAC also pose as challenges to successful AAC provision and use (Sigafoos et al., 2021). In addition, several studies have reported unmet needs of persons with intellectual disability and complex communication in relation to AAC provision (Siu et al., 2010; Sutherland et al., 2005; Sutherland et al., 2014). The absence of AAC for this population may be due to a possible lack of awareness or training (Sigafoos et al., 2021) and lack of access to professionals with expertise in AAC (Siu et al., 2010; Sutherland et al., 2005; Sutherland et al., 2014).
Professionals must be mindful of the impact of AAC on both the user and their communication partners. The introduction of AAC impacts both the AAC user and their family (Angelo, 1997; Parette and Angelo, 1996; 1998). Therefore, professionals need to understand the affect AAC has on the family members (Angelo, 2000). More than half of families in a study by Angelo (2000) reported improvements in their child’s QoL, communication and independence. Communication partners have expressed frustration towards AAC device malfunctions (McCord and Soto, 2004; Kulkarni and Parmar, 2017) and difficulty understanding the AAC system (McCall et al., 1997). Despite these findings, it has been found that AAC has the potential to support individuals' complex communication needs (Beukelman and Mirenda, 2005). With encouragement, support, instruction and practice AAC users can transition from AAC novices to competent AAC communicators (Beukelman and Mirenda, 2005). Similarly, individuals with profound intellectual and multiple disability may develop intentional or functional communication skills when an AAC mode is suitably developed with a systematic instructional program that is well designed (Reichle et al., 1991).
Internationally, The United Nations Convention on the Rights of Persons with Disabilities (UN, 2006) provides a framework to promote, protect and ensure the rights of all people with a disability and encourages equal rights in all parts of life. The United Nations Convention on the Rights of Persons with Disabilities advocates accepting and facilitating the use of AAC. However, people with severe/profound intellectual disability continue to have unmet communication support needs (Brady et al., 2016). Changes in policy, legislation and regulation have transformed the approach to services for individuals with intellectual disability. People with severe/profound intellectual disability are more present and visible today than they were ever before (Brady et al., 2016) and the increase in the population of adults with an intellectual disability is expected to have an impact on the need for services and supports (Oulette-Kuntz et al., 2016). In addition, individuals with complex communication needs and their families have greater expectations to take part in a range of environments (Light et al., 2019). Increased expectations have led to a greater demand for access to AAC. To meet these individuals' variety of needs, service providers must consider new AAC supports, improved skill instruction and partner supports (Light and McNaughton, 2014; Light et al., 2019).
Given the potential of AAC to meet individuals with severe/profound intellectual disability complex communication needs, the challenges to successful AAC use and the significant role of communication partners in successful AAC provision and use, there is a need to explore communication partners experiences of using AAC with adults with severe/profound intellectual disability. The aim of this review was to explore communication partners’ experience of communicating with adults with severe/profound intellectual disability through AAC with a view to identifying potential barriers and facilitators to successful AAC use. Such knowledge may be of value when planning AAC support for persons with severe/profound intellectual disability and implementing AAC with them and their communication partners.
Methods
Protocol and Registration
A review protocol was developed by the authors. However, it was not published.
Design
The Joanna Briggs Institute (JBI) guidelines for mixed methods systematic reviews (MMSR) were followed. MMSR combine the findings of effectiveness from quantitative research and participants' experiences from qualitative research to increase the helpfulness of findings for decision makers (Bressan et al., 2016). Both perspectives are increasingly required to inform clinical, policy or organizational decisions (Lizorando et al., 2020). The universal steps of undertaking a systematic review apply to MMSR (Lizorando et al., 2020). However, there are differences in combining and integrating data. This MMSR followed a convergent integrated approach in keeping with the JBI methodology for MMSR. Specifically, this approach is a process of combining the data that was extracted from quantitative, qualitative and mixed methods studies. Data transformation was required to allow for the integration of qualitative and quantitative data.
Search strategy
A preliminary scoping search was undertaken with a specialist health sciences librarian. Databases were then selected based on the ‘fit’ with the topic area and return of relevant results.
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) (Moher et al., 2009), a literature search of seven databases was conducted including CINAHL, Scopus, Academic Search Complete, PubMed, ERIC, Cochrane, and Linguistics Collection in January 2020 and reviewed again in January 2021. No new literature was identified. These databases are comprehensive for health, social care and education; areas of practice commonly supporting people with intellectual disability. English language was the only database filter applied. As per PRISMA (2009) guidelines one full electronic search strategy has been presented in this review (Supplementary Table 1).
The following key concepts were searched and combined: search terms referring to severe/profound intellectual disability
The inclusion of the key concept relating to caregivers resulted in a limited number of hits in CINAHL and Academic Search Complete. Therefore, a second search was completed in these databases without that search string to identify potential literature relevant to this topic.
Study Selection
Inclusion and Exclusion Criteria
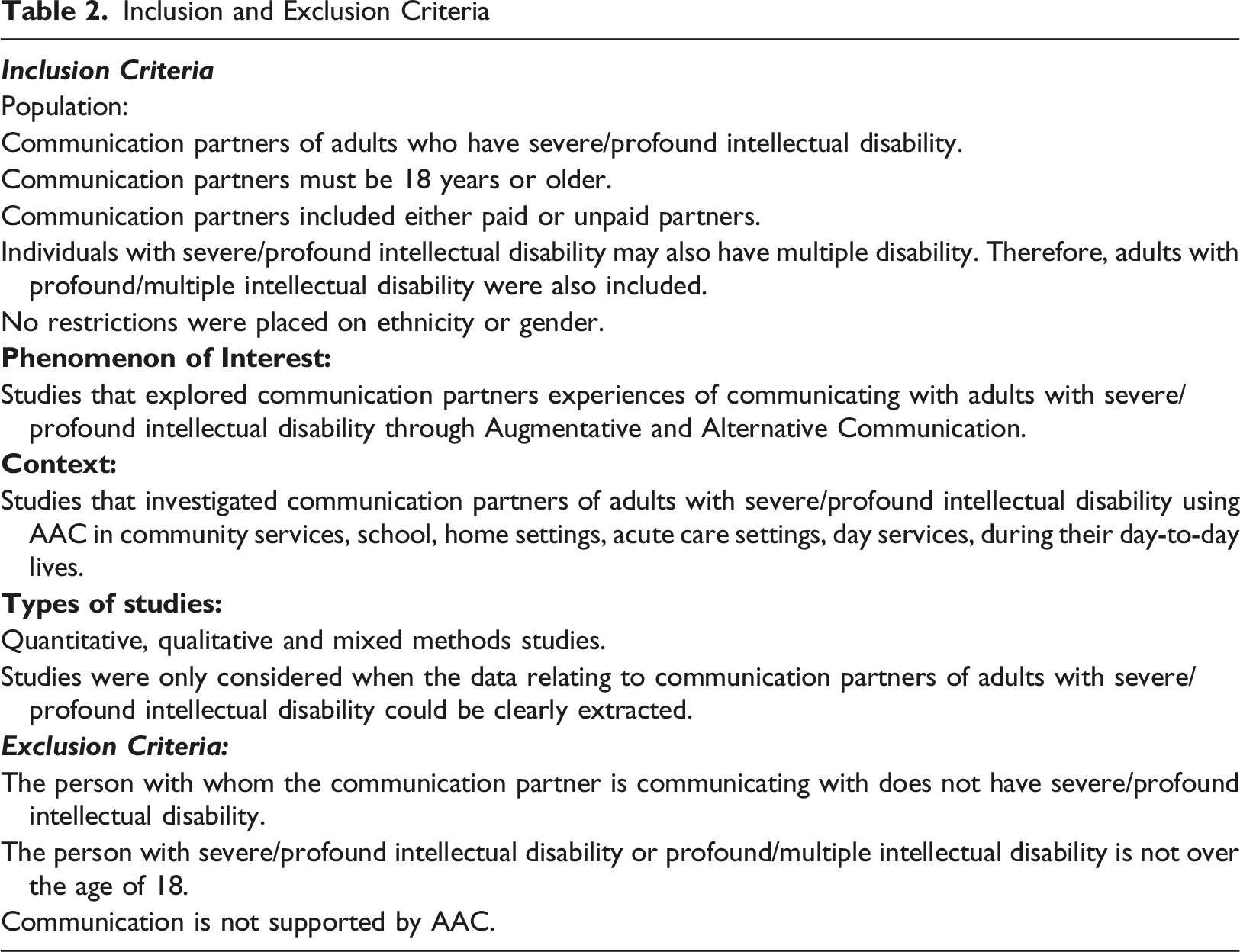
The full text of the remaining 99 articles were assessed for eligibility. Eight of these 99 articles met the inclusion criteria. The rationale for excluding 91 full-text records is detailed in the PRISMA Flow diagram (Figure 1). Any disagreements that arose between the authors were settled through discussion PRISMA Flow Diagram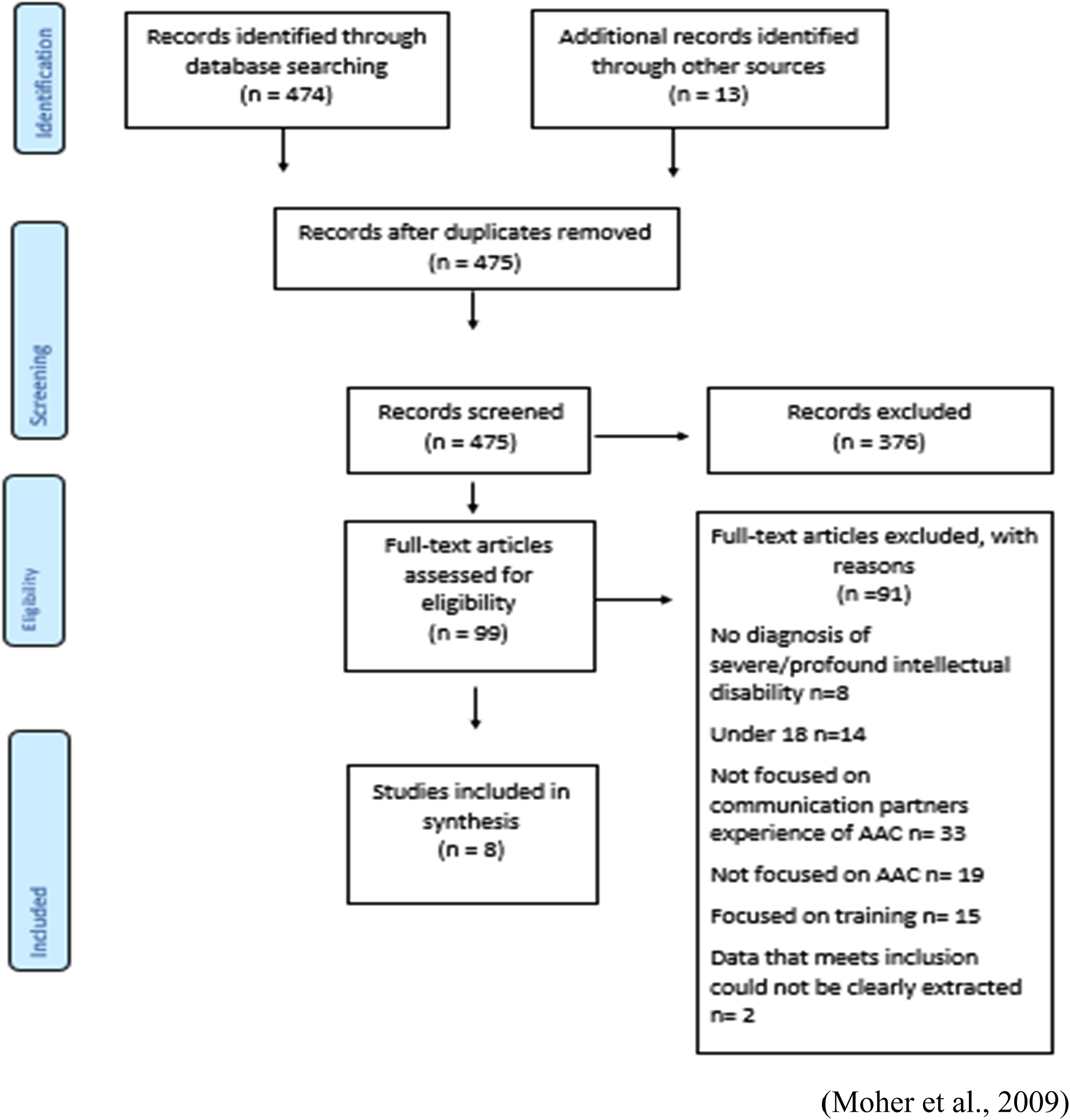
The studies that met the inclusion criteria were assessed for methodological quality using the Mixed Methods Appraisal Tool version 2018 (MMAT; Hong et al., 2018). The MMAT includes a total of 25 criteria and 2 screening questions. The MMAT was developed to appraise qualitative research, randomized control trials, non-randomized control trials, quantitative descriptive studies and mixed methods studies. The scoring system was removed from the 2018 version of the MMAT as it is advised to provide a more detailed presentation of the ratings of each criterion (Hong et al., 2018). Exclusion of papers with low methodological quality is not encouraged. Therefore, before screening, the authors agreed that all studies regardless of the results of their methodological quality would undergo extraction and synthesis. The MMAT was applied by the authors (EH, AMM, CD, EL). Any disagreements were discussed as a group. To improve the transparency in reporting the appraisal process, a summary of the MMAT results is included (can be seen in Supplementary Table 3).
Data Extraction
Summary of Data Extraction
Data Transformation
Following the JBI convergent integrated approach for MMSR, the quantitative data was ‘qualitized.’ The quantitative data was ‘qualitized’ as codifying the quantitative data has a lower risk of errors compared to applying numerical values to the qualitative data (The Joanna Briggs Institute, 2014). ‘Qualitizing’ the quantitative data was achieved by extracting data from quantitative studies and translating quantities into textual descriptions (Lizorando et al., 2020). Once extracted, the quantities were translated into individual sentences to answer the research question. This was then pooled with the data that was directly extracted from qualitative studies (Stern et al., 2020). This allowed the quantitative and qualitative data to be combined (Hong et al., 2017).
Data Synthesis
Thematic synthesis was undertaken manually (Thomas and Harden, 2008). The synthesis of the results was carried out in three stages; (1) free line by line coding of the extracted data followed by (2) grouping of these codes into related areas to develop descriptive themes, then (3) developing analytical themes (Thomas and Harden, 2008). The assembled data were categorized and pooled together based on similar meanings to produce a set of integrated findings to answer the review question.
Research Integrity
Each researcher has the responsibility to make ethical decisions at each stage of the review process. Wager and Wiffen (2011) outline practical and ethical issues that need to be considered when planning and publishing a MMSR. These include avoiding plagiarism, providing transparency and ensuring accuracy.
In this review other people’s words are indicated using double quotation marks and citation. It is acceptable to describe a person’s work in your own words. To ensure transparency, those who worked on the review are acknowledged and statements regarding information about funding and competing interests are provided (Cochrane Collaboration, 2011). Each researcher has the responsibility to ensure accuracy in data extraction. The results are presented without bias and review limitations outlined. Data extraction was clearly planned, disagreements were resolved through discussion and all authors agreed on which data was to be included (Wager and Wiffen, 2011). This MMSR followed the JBI convergent integrated approach according to the JBI methodology for MMSRs.
Results
Background of included studies
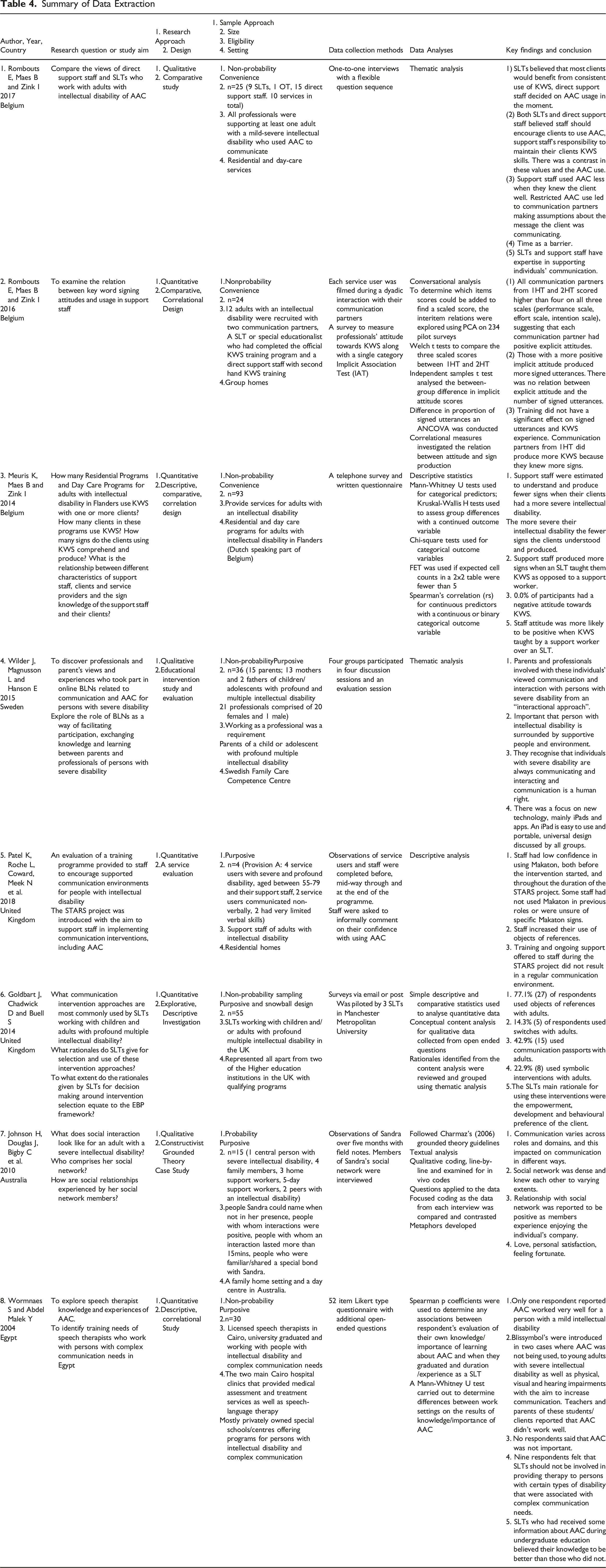
Eight studies met the inclusion criteria. Three of these were qualitative (Johnson et al., 2010; Rombouts et al., 2017; Wilder et al., 2015) and five quantitative (Goldbart et al., 2014; Meuris et al., 2014; Patel et al., 2018; Rombouts et al., 2016; Wormnaes and Abdel Malek, 2004). Three studies were conducted in Belgium (Meuris et al., 2014; Rombouts et al., 2016; Rombouts et al., 2017), two in the United Kingdom (Goldbart et al., 2014; Patel et al., 2018) and the remainder were conducted in Australia, Sweden and Egypt (Johnson et al., 2010; Wilder et al., 2015; Wormnaes and Abdel Malek, 2004).
All studies considered the experiences of either support staff (i.e., support workers, teachers, personal assistants) or facilitators who supported communication partners and AAC users (I.e., Speech and Language Therapists (SLT) and Occupational Therapists) with a total of 256 professionals participating in seven of the eight studies selected. One study did not specify how many staff were included (Patel et al., 2018). Two (Johnson et al., 2010; Wilder et al., 2015) of the eight studies included both support staff and family members (n = 19) views and one study (Johnson et al., 2010) included two peers as communication partners.
Three studies used surveys and two studies used questionnaires as the data collection method. Meuris et al. (2014) used both written questionnaires and telephone surveys. Interviews were utilised by two studies. Observations were undertaken by two studies. Johnson et al. (2010) used both observations and interviews. Discussion sessions were held in one study (Wilder et al., 2015). Sample sizes ranged from 8 to 93 respondents.
Synthesis
Four major themes were identified relating to communication partners experiences of communicating with adults with severe/profound intellectual disability through AAC; (1) Knowledge of AAC, (2) Attitudes and AAC Use, (3) Shared Commitment to Communication Partnership, and (4) Suitability of AAC (Supplementary Figure 2).
Theme 1: Knowledge of AAC
Theme one captures the sources from which communication partners acquired information and knowledge about AAC, the impact of training on their knowledge and the value of having knowledge in AAC. Four articles reported on knowledge of communication and AAC (Meuris et al., 2014; Rombouts et al., 2016; Wilder at al., 2015; Wormnaes and Abdel Malek, 2004)
Acquiring Knowledge about AAC
Communication partners acquired their information and knowledge about AAC through several resources.
Training provided by SLTs to support workers increased knowledge and use. Support staff knew and produced more signs when trained by an SLT (Meuris et al., 2014; Rombouts et al., 2016) or at an official training program (Rombouts et al., 2016) rather than a support worker. However, there were mixed reports about SLTs preparedness to provide such training, where SLTs wanted more knowledge and training in AAC. Wormnaes and Abdel Malek (2004) reported that SLTs within their study wanted further training and education in AAC to support persons with complex communication needs. Thirty per cent (9/30) of their respondents suggested a need for training about signs or symbols (Blissymbol’s, sign language, Makaton, pictures, tangible symbols) for SLTs who wanted to support people with little or no functional speech. SLTs within this study introduced Blissymbols to individuals with sensory impairments, which were reported to be unsuccessful. Introducing abstract symbols to such individuals highlights a lack of expertise (Wormnaes and Abdel Malek, 2004) as those who have significant cognitive and language limitations may find abstract symbols challenging to use. This suggests that SLTs within this study required further training and education in the selection of suitable AAC methods for persons with severe/profound intellectual disability.
Providing AAC information to SLTs during their education was beneficial to their knowledge level. SLTs received information about AAC through undergraduate education, postgraduate training, colleagues, books, journal articles, conferences, seminars, courses, workshops or television (Wormnaes and Abdel Malek, 2004). The value of providing information to professionals during their undergraduate education was highlighted where SLTs who had received this information evaluated their knowledge as greater than those who did not receive such information about AAC during their undergraduate education (Wormnaes and Abdel Malek, 2004). This suggests that more in-depth, extensive training may improve knowledge of AAC and result in professionals who feel knowledgeable in the field.
Knowledge and AAC Use
The relationship between knowledge and AAC use was captured by two studies. Communication partners knowledge about AAC could enhance or hinder AAC use (Rombouts et al., 2016; Wilder et al., 2015). A lower level of knowledge was considered a limiting factor to AAC use (Wilder et al., 2015). An enhanced knowledge of AAC led to increased use of AAC by communication partners (Rombouts et al., 2016).
To surmise, gaps in communication partners knowledge of AAC may result in unmet communication needs of persons with severe/profound intellectual disability. The importance of training and education around AAC use with persons with severe/profound intellectual disability to enhance the communication partners skillset is highlighted by the findings in this theme. SLTs have a fundamental role in facilitating AAC training. Therefore, they need to have sufficient training in and knowledge about AAC. Previous education about AAC may improve communication partners ability to communicate with persons with severe/profound intellectual disability who use AAC, potentially increasing the likelihood of meeting the individual’s communication needs.
Theme 2: Attitudes and AAC Use
This theme captures the interplay between communication partners attitudes towards AAC, their personal characteristics and the relationship between attitude and AAC use. This theme includes findings from six studies (Johnson et al., 2010; Meuris et al., 2014; Rombouts et al., 2016; Rombouts et al., 2017; Wilder et al., 2015; Wormnaes and Abdel Malek, 2004).
Available evidence indicates that communication partners attitudes towards AAC was positive overall or at least they did not have a negative attitude towards AAC (Meuris et al., 2014; Rombouts et al., 2016; Wormnaes and Abdel Malek, 2004). Those who has a more positive implicit attitude produced more signed utterances. However, there was no relation between explicit attitude and the number of signed utterances (Rombouts et al., 2016). Wilder et al, (2015) highlighted communication partners’ willingness to communicate as an important component in facilitating communication. Therefore, the available evidence would indicate that communication partners attitudes towards and willingness to use AAC may improve AAC usage.
Communication Partners Assumptions
While Johnson et al. (2010) found that knowing the individual with severe/profound intellectual disability was important to facilitate communication (Johnson et al., 2010), Rombouts et al. (2017) identified that it could be a potential barrier to communication when communication partners make assumptions about what the individual is communicating (Rombouts et al., 2017). When such assumptions were incorrect, the AAC user may not clarify their intended message resulting in misunderstanding (Rombouts et al., 2017). In addition, when support staff knew the AAC user well, they felt there was less of a need for communication support. Consequently, the perceived need to use AAC was lowered and AAC use was less frequent. Direct support staff mainly used KWS when there was an acute need for communication support depending on each person's individual needs (Rombouts et al., 2017). This could result in limiting AAC use (Rombouts et al., 2017).
To surmise, communication partners' attitude may enhance or hinder AAC usage with adults with severe/profound intellectual disability. Communication partners' personal characteristics may promote AAC use with the individuals that they support. Knowing the individual well was cited as an important factor in AAC use. However, this may also hinder AAC use should communication partners make assumptions about the intended message on the premise that they know what they are communicating. Such assumptions could pose as a potential barrier to communication opportunities for individuals with severe/profound intellectual disability.
Theme 3: Shared Commitment to Communication Partnership
The shared commitment to communication partnership is fundamental for the effective and efficient use of AAC with adults with severe/profound intellectual disability. There are various factors that can enhance or hinder this commitment, including uncertain ownership of AAC roles and responsibility, time constraints and the inclusion of communication partners in intervention planning.
Perceptions about Roles and Responsibilities
Communication partners have various roles and responsibilities in supporting persons with severe/profound intellectual disability communication through AAC (Rombouts et al., 2017; Wormnaes and Abdel Malek, 2004). Skilled communication partners were acknowledged as having additional responsibility within the individuals’ environment (Wilder et al., 2015).
Uncertain ownership of responsibilities was cited as a limiting factor to effective communication for AAC users (Wilder et al. 2015). Communication partners uncertain ownership could limit the individual’s communication goals and overall progress of these goals (Wilder et al., 2015; Wormnaes and Abdel Malek, 2004). There was a disconnect between SLTs perceptions of their roles, where some SLTs saw their role as supporting persons with severe/profound intellectual disability and complex communication needs while others did not (Wormnaes and Abdel Malek, 2004). More than half (52% n=15.6) of the SLTs provided speech therapy to people with severe intellectual disability and complex communication needs. However, 30% (9/30) of SLTs did not see the provision of therapy to persons with disabilities associated with complex communication needs as part of the SLT role (Wormnaes and Abdel Malek, 2004). The SLTs believed psychiatrists should be responsible for working with people with severe or multiple disabilities and that AAC specialists should be responsible for working with those who do not gain from speech training (Wormnaes and Abdel Malek, 2004). Therefore, to ensure individuals with severe/profound intellectual disability communication needs are met, there needs to be a clear outline of each communication partner's roles and responsibilities in AAC use. From a professional perspective a decision needs to be made regarding roles and responsibilities for training and knowledge about AAC and its use.
Professional and Family Members Input
Communication partners have different areas of expertise that contribute to the AAC intervention (Rombouts et al., 2017). Support staff shared their expertise with SLTs and SLTs viewed this contribution as crucial for AAC implementation (Rombouts et al., 2017). However, a gap in the inclusion of other communication partners was noted in two studies. SLTs worked with professionals and family carers but did not mention the views of these partners as often as expected when choosing an intervention (Goldbart et al., 2014) or co-operate with them to gather information as regularly as expected when developing supportive communication environments (Wormnaes and Abdel Malek, 2004).
Time
The importance of communication partners spending time with individuals with severe intellectual disability to learn how to interact with them was cited (Johnson et al., 2010). Therefore, partners need to have sufficient time to support individuals to communicate. However, time constraints were recognised to be a potentially limiting factor for effective AAC use with persons with severe/profound intellectual disability (Rombouts et al., 2017; Wilder et al. 2015).
Time constraints were related to communication partners workload, such as completing a range of tasks implemented by multiple stakeholders (Rombouts et al., 2017). They led to difficulty in detecting subtle communication signs, resulting in missed opportunities for communication (Patel et al., 2018). Patel et al. (2018) stated that the difficulty in detecting subtle communication signs may be due to the higher demands of providing physical care. Skilled interpretation was needed to understand the individual’s communication (Johnson et al., 2010) and it was a challenge to be persistent when communicating with individuals with delayed or subtle communication attempts (Wilder et al., 2015). Therefore, communication partners need sufficient time to recognise and interpret individuals' communication.
While SLTs understood that support staff had a high workload, they felt that their assessment of KWS and training as time demanding was unfair (Rombouts et al., 2017). Investing time into consistently using AAC would result in less deliberation in the future (Rombouts et al., 2017), resulting in time efficient supports for the future (Rombouts et al., 2017). In addition, the perceived time constraints were somewhat determined by the educational background of the staff. Support staff who had received care orientated education were not as involved in service users' communication needs, where a participant stated that carers viewed care as their primary responsibility. Therefore, pre-service education may provide support staff with guidance for their role as ‘aided language stimulator’ (Rombouts et al., 2017, p. 109) which may help to further enhance their understanding of the continued and consistent use of AAC.
Communication partners hold different roles and responsibilities in meeting the communication needs of a person with a severe/profound intellectual disability through AAC. However, lack of ownership of such roles and responsibilities may result in limited communication for persons with severe/profound intellectual disability. The inclusion of all communication partners in deciding on an intervention may lead to increased understanding and ownership of roles and responsibilities in AAC use. To strengthen the shared commitment to communication partnership it is important that each person is aware of their individual roles and responsibilities in the design, planning and use of AAC.
Theme 4: Suitability of AAC
Certain methods of AAC were deemed more suitable in meeting the complex communication needs of adults with severe/profound intellectual disability than others.
Promoting Acceptance
Two studies found that certain methods of AAC use were reported to encourage inclusion and participation (Goldbart et al., 2014; Wilder et al., 2015). For most respondents, switch use was a route to intentional communication for persons with severe/profound intellectual disability or increased participation and interaction (Goldbart et al., 2014). Similarly, iPads were discussed as being able to overcome boundaries as they are well known and can improve acceptance and encourage inclusion (Wilder et al., 2015). Introducing a method of AAC that improves acceptance could increase the use of AAC with the person with a severe/profound intellectual disability in different environments.
One study highlighted the suitability of objects of references for supporting individuals with severe/profound intellectual disability (Goldbart et al., 2014). Objects of reference were the most used method of AAC with adults with profound and multiple intellectual disability within one study (Goldbart et al., 2014). They were deemed important to support service users understanding and encourage choice making (Goldbart et al., 2014). The importance of objects of reference for people with sensory impairment, specifically visual impairment was mentioned by 25% (9/36) of SLTs (Goldbart et al., 2014).
Individuals Communication Needs
The importance of recognizing individuals’ communication needs emerged from five studies. The ability and needs of individuals with severe/profound intellectual disability needs to be considered when introducing AAC. This was evident where SLTs main rationale for the introduction of AAC was the ‘empowerment, development and behavioural preferences’ of the service user (Goldbart et al., 2014).
The more severe the level of intellectual disability the fewer KWS the person with the intellectual disability were estimated to understand and produce (Meuris et al., 2014). Despite this, signing systems were used with people with severe/profound intellectual disability in five studies (Goldbart et al., 2014; Meuris et al., 2014; Patel et al., 2018; Rombouts et al., 2017; Rombouts et al.,2016). In addition, support staff produced less signs when the service users had severe intellectual disability (Meuris et al., 2014). This impacts on the communication opportunities of persons with severe/profound intellectual disability who communicate through signs.
Symbolic approaches were reported as having the potential to be very motivating for persons with sufficient vision (Goldbart et al., 2014). However, Blissymbol’s were introduced to adults with severe intellectual disability and sensory impairments including visual impairments, teachers and parents reported AAC did not work well in these cases (Wormnaes and Abdel Malek, 2004).
The AAC chosen and used must be tailored and suitable to each person with an intellectual disability individual need.
Discussion
This review aimed to explore communication partner’s experiences of communicating with adults with severe/profound intellectual disability through AAC.
Findings suggest that increased use of AAC could be aligned with communication partners' increasing knowledge. Limited knowledge indicated lower usage. This finding is similar to Beukelman et al. (2008) where AAC success or failure was somewhat dependent on communication partners knowledge. In addition, in their Egyptian study, Wormnaes and Abdel Malek (2004) found that SLTs who received training during their undergraduate education felt more confident using AAC and those who believed they were more qualified in AAC supported more service users to use AAC (Wormnaes and Abdel Malek, 2004). In the hope of improving professional’s knowledge of AAC, training other professionals, such as teachers and healthcare professionals in AAC during their undergraduate education may further improve the provision and use of AAC with this population. The requirement for pre-service and in-service education in AAC has been repeatedly advocated in the literature (Balandin and Iacono, 1998; King, 1998; Simpson et al., 1998; Sutherland et al., 2005; Wormnæs and Abdel Malek, 2004). In addition, Lund and Light (2007) stated that knowledge barriers could be reduced by ensuring service providers are trained in AAC. By reducing knowledge barriers of service providers, persons with complex communication needs will have better access to experienced professionals (Lund and Light, 2007).
Similarly, communication partners need to have knowledge of AAC systems, services and a skillset in interaction strategies to provide suitable support (Kent-Walsh et al., 2010). A need for training relating to suitable methods of AAC for adults with severe/profound intellectual disability and complex communication needs was identified. This is reflected in SLTs introduction of Blissymbols to individuals with sensory support needs (Wormnaes and Abdel Malek, 2004). This highlighted a potential knowledge gap as some individuals who have significant cognitive and language limitations have difficulty using abstract symbols (Wormnaes and Abdel Malek, 2004). They benefit from expressing themselves using fewer abstract representations such as objects (Light et al., 2019). Objects of reference were reported to be successful when used (Goldbart et al., 2014). In addition, signing systems were used in five studies (Goldbart et al., 2014; Meuris et al., 2014; Patel et al., 2018; Rombouts et al., 2017; Rombouts et al.,2016). However, as severity of intellectual disability increased, communication partners estimated that fewer KWS were understood and produced by the individual (Meuris et al., 2014). This finding highlights the importance of having knowledge of AAC techniques that are individualized to each person and their needs. This concurs with the wider literature about feature matching, where team members work to match the individuals who require communication supports with the AAC (Ogletree, 2021). Having an awareness of individual’s complex communication needs may optimize the selection of suitable interventions that will offer each person the equal opportunity to communicate.
Individuals with severe/profound intellectual disability have complex and specific communication needs, therefore interventions should be specific to these needs. A person centred and individualised approach to supporting communication is recommended. One way of achieving this is to develop personal support plans to maximise individuals human functioning dimensions (Schalock et al., 2021b). In addition, the supports model concentrates on the match between individuals and their environments, whereby disability is “the expression of limitations in individual functioning within a social context” (Schalock et al., 2021b: p.6). In line with the supports model, strategies and resources need to promote individuals’ development and interests as well as enhance their well-being. Such support systems need to be person centred, outcome oriented, co-ordinated, comprehensive, include choice, inclusive environments and both generic and specialised supports (Coulter, 2005; Schalock et al., 2019; Shogren et al., 2018; Stancliffe et al., 2016; Thompson et al., 2014). In addition, support plans should match an individual’s needs (Schalock et al., 2018). It is recognised that it is challenging (Munde and Vlaskamp 2015) to develop interventions that match the individuals' abilities and needs. Therefore, the form of AAC used should be reflective of communication and functional needs of the individual AAC user.
The role of the SLT in training communication partners in AAC and improving their skillset was highlighted. Both support staff and service users knew more signs when they were taught by a SLT compared to a support staff. This is important as the success of interactions of persons using AAC is dependent on their own skills and that of their communication partners (Kent-Walsh and McNaughton, 2005).
There is agreement in the literature that AAC is a team approach that includes multiple stakeholders (De Paepe and Wood, 2001; Beukelman et al., 2008; Beukelman and Mirenda, 2005; Ogletree, 2021). Everyone who uses AAC with the individual should be involved in the team (ASHA, 2002). In addition, collaboration between team members can result in positive outcomes for AAC users and their family members (Lund and Light, 2007) and facilitate AAC success and implementation (Uthoff et al., 2021). The uncertain ownership of AAC roles and responsibility is a key finding of this review (Wilder et al., 2015; Wormnaes and Abdel Malek, 2004). This can lead to limited provision and use of AAC with adults with severe/profound intellectual disability. Firstly, SLTs uncertainty around providing support to persons with complex communication needs indicates that potentially, services may not be provided. This finding arose from an Egyptian study and therefore, should be considered within this cultural context. Furthermore, a participant in Lund and Light’s (2007) qualitative study discussed encountering a number of SLTs who did not think AAC was part of their profession. This suggests that a lack of clarity around professional responsibility may lead to inconsistency in access to certain services, which could result in unmet communication needs for persons with severe/profound intellectual disability. Therefore, all team members need to be aware of their own and other team members roles and responsibilities when supporting individuals with severe/profound intellectual disability to communicate through AAC.
The findings of this review indicate that collaboration between stakeholders is sub-optimal to what is recommended. Family views and wishes did not inform the rationale for certain AAC methods used by SLTs (Goldbart et al., 2014) and SLTs did not gather information from parents within natural settings (Wormnaes and Abdel Malek, 2004). This concurs with the literature that family carers felt that they were not included by professionals in decision making about their family members lives (Chadwick et al., 2013; Goldbart and Canton, 2010). In line with the recommended use of a holistic approach teams are required to ensure multiple perspectives are heard and included (Schalock et al., 2021b). In addition, the supports model actions outline the importance of working with the individual and their family to develop personal goals, support needs and strategies (Schalock et al. 2021b). Similarly, there is an increased recognition of the need to facilitate family centred care in the field of intellectual disability. The importance of collaborative, family centred AAC decision making is repeatedly documented within the literature (Angelo, 2000; Bailey et al., 2006; Sonnenmeier et al., 2005; Soto et al., 2001).
A greater number individuals are seeking and receiving AAC services than ever before due to more individuals presenting with complex communication needs and families and professionals recognizing the positive impact of AAC (Light et al., 2019). Therefore, it is important that family members and all other appropriate communication partners are involved in the design, planning and use of AAC with and for the person with severe/profound intellectual disability with the intention of increasing their awareness of its importance and their roles and responsibilities. Similarly, De Geeter et al. (2002) suggest that parents take on more responsibilities when they are actively involved in making decisions.
Including all appropriate communication partners in the decision-making process may further increase their understanding of their responsibilities, therefore leading to an increase in their ownership of such responsibilities and potentially facilitating a collaborative AAC approach. It is recognised that responsibilities of stakeholders can vary and be shared when a collaborative relationship is developed (Beukelman et al., 2008).
The findings of this MMSR indicate that clarity is required about the roles and responsibilities of all communication partners of individuals with severe/profound intellectual disability involved with AAC use. Given communication partners fundamental role in supporting individuals with severe/profound intellectual disability AAC use, uncertain ownership of roles and responsibilities creates an impediment to meeting their communication needs. Further research is required to explore communication partners perceptions of their roles and responsibilities and those of other communication partners when implementing AAC and supporting persons with a severe/profound intellectual disability to communicate and interact. From a practical standpoint, understanding communication partners' perceptions of their roles and responsibilities and those of other partners involved could be valuable for facilitating collaboration between all stakeholders involved. Having knowledge of such perceptions could help to inform organisational policy and direct the future of AAC implementation with persons with severe/profound intellectual disability and their communication partners.
This review focused on communication partners perspectives. Certain methods of AAC were identified that were deemed more suitable in supporting individuals with severe/profound intellectual disability needs. While it was beyond the scope of this review to explore the appropriateness of AAC for persons with severe/profound intellectual disability, this topic merits further investigation. Therefore, it is important to consider the appropriateness of AAC or structured programs in supporting these persons individual communication needs.
Strengths and Limitations of the Review
The findings of this MMSR should be considered in the context of its limitations. The risk of bias was increased by not publishing the review protocol. Language biases may have been introduced as the studies were only published in English, which may have led to relevant studies being missed. Psychology databases were not included. It is recognised that they can cover papers of interest on this topic. However, in consultation with the subject librarian seven databases were selected based on the ‘fit’ with the review topic and the return of relevant results.
The presence of strengths within this MMSR are also acknowledged. Two authors screened the title and abstract of the articles and assessed the full text articles for eligibility. Selection bias was not a feature of this MMSR as all studies were included regardless of their quality rating using the MMAT. The thematic synthesis process was robust. The translation process, through the development of descriptive and analytical themes, was done in a rigorous way that ensured transparency in reporting the results (Thomas and Harden, 2008).
Conclusion
This review provides insight into the experiences of communication partners who communicate with adults with severe/profound intellectual disability through AAC. There is a disconnect between communication partners perceptions of their roles and responsibilities in the use of AAC with adults with severe/profound intellectual disability. Clarity is required about the roles and responsibilities of each communication partner using AAC with adults with severe/profound intellectual disability to increase the likelihood of the individual’s communication needs being met. Therefore, further research is required to explore communication partners’ perceptions of their roles and responsibilities in AAC use with this population to advance understanding, improve communication partnerships and practice.
Supplemental Material
Supplemental Material - Communication partners experiences of communicating with adults with severe/profound intellectual disability through augmentative and alternative communication: A mixed methods systematic review
Supplemental Material for Communication partners experiences of communicating with adults with severe/profound intellectual disability through augmentative and alternative communication: A mixed methods systematic review by Edina Hanley, Anne-Marie Martin, Caroline Dalton, and Elaine Lehane in Journal of Intellectual Disabilities
Footnotes
Acknowledgements
This review is part of the first authors PhD project. We would like to thank Donna O’Doibhlin, the subject librarian for helping to develop the search strategy. We would also like to thank Professor John Browne for the information provided during the module PG7016 Systematic reviews for the health sciences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.