
Abstract
This literature review was designed to establish the effects of sedentary behaviour on the physical health of adults with an intellectual disability. Sedentary behaviour is defined as any waking behaviour characterized by an energy expenditure of ≤1.5 METs while in a sitting, lying or reclining posture. An extensive search was executed in six databases: EMBASE, Medline, CINAHL, PsycINFO, ASSIA and Web of Science. Following screening, 18 articles remained for inclusion in the review. A thematic analysis using the Braun and Clarke six step process resulted in the identification of seven broad health areas. Studies showed a prevalence of obesity, multimorbidity and metabolic syndrome as well as elevated levels of sedentary behaviour in adults with an intellectual disability. This literature review demonstrated that sedentary behaviour could be a contributor to the poor health which is common in adults with an intellectual disability. However to date the body of evidence does not confirm a cause-and-effect relationship.
Introduction
In order to understand the physical health effects of sedentary behaviour, it is important to understand what health is and what it means to be healthy. The constitution of the World Health Organisation (WHO) states that health does not just refer to the absence of disease but is a complete state of social, physical and mental well-being and represents a fundamental right for all (World Health Organisation, 1995). Conversely, a cross-sectional study found that people with physical disabilities felt their disability did not define their state of health but rather that an absence of illness was what made them healthy (Nazli, 2012). The perception of being healthy does not necessarily correspond with reports on health conditions. Over 73% of adults with an intellectual disability who participated in The Intellectual Disability Supplement to the Irish Longitudinal Study on Aging (IDS-TILDA) perceived their health as “very good” or “good” despite multimorbidity levels in excess of 71% (Lynch, 2021; McCarron et al., 2013). This perception of good health was retained and sometimes exceeded across the 10 years of the study (Lynch, 2021; McCarron, 2011; McCarron et al., 2014, 2017). In general adults with an intellectual disability have shorter life spans than their counterparts in the general population, dying approximately 19 years earlier and from different causes (Cooper et al., 2020; McCarron et al., 2015). A Brazilian proxy-based study of adults aged 35–60 years showed that after 5 years, despite the relatively young age profile, adults with intellectual disability had more physical and mental health issues than controls (Guilhota et al., 2016). Worldwide, Ischaemic heart disease was the primary cause of death in the general population (Khan et al., 2020). A leading contributor to heart disease is overweight and obesity which was observed in almost 80% of a cohort of adults with intellectual disability but although these Cardiovascular disease (CVD) risk factors were prevalent, heart disease was not the main cause of death (McCarron et al., 2017). Instead, for adults with an intellectual disability choking and respiratory infections were the leading causes of death (Cooper et al., 2020; World Health Organisation, 2020). However the shorter lifespan combined with the considerable multimorbidity rates observed in the intellectual disability population compared to the general population warrant further research and attention to cardiovascular risk factors such as sedentary behaviour (SB) and physical inactivity are essential until a greater understanding of these behaviours is obtained.
While both SB and physical inactivity are typified by low energy expenditure they are different and should be addressed separately. SB has been defined as ‘any waking behaviour characterized by an energy expenditure of ≤1.5 METs while in a sitting, lying or reclining posture’ for example watching television or working on a computer while physical inactivity is not achieving the WHO recommended activity levels for health (Tremblay et al., 2017; World Health Organisation, 2016). A review of systematic reviews on the effects of SB on health found that SB could be an important contributor to health irrespective of physical activity (PA) levels (Rezende et al., 2014). In fact in the general population, there is evidence to suggest that increased sedentary time is associated with greater risks for all-cause mortality, an increase in metabolic risk factors, the incidence of CVD, type 2 diabetes risks and certain types of cancer (Biswas et al., 2015; Chomistek et al., 2013; Edwardson et al., 2012; Krishnan et al., 2009; Lynch et al., 2018). Hence while studies on the general population indicate that there may be health issues associated with increased time in SB, only limited information is available for adults with an intellectual disability. The aim of this literature review is to understand the physical health effects of sedentary behaviour in the adult intellectual disability population.
Methods
Research question
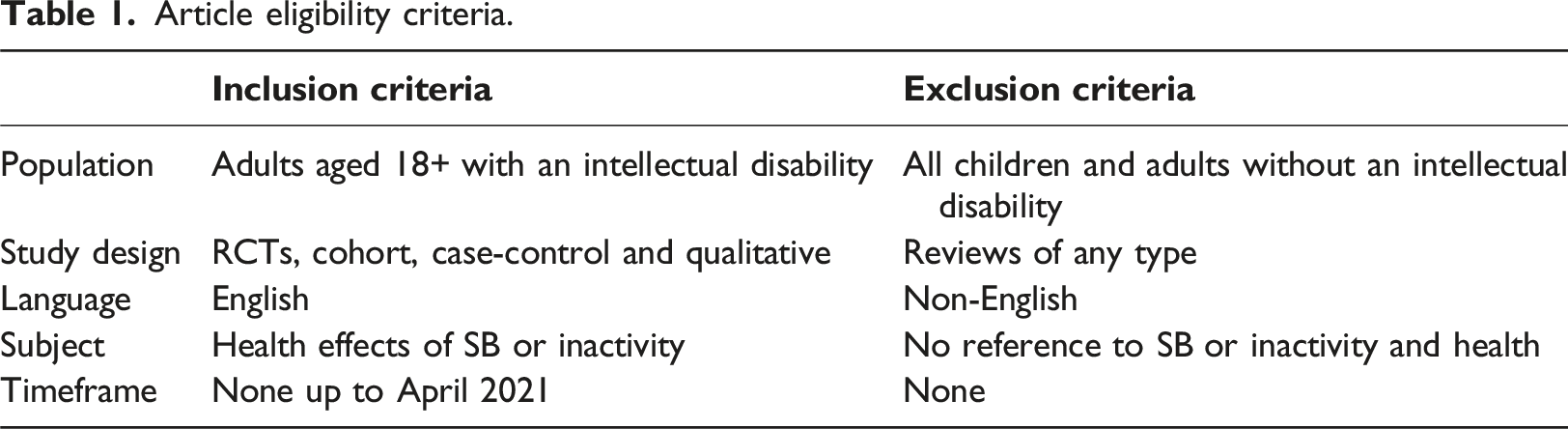
The PICO approach was used to define the research question for this literature review as follows: • P [Population or problem]: Adults aged 18+ with an Intellectual Disability • I [Intervention or exposure]: Sedentary behaviour (SB) level in line with the definition of SB • C [Comparison]: Individuals with all levels of intellectual disability living in residential, institutional or hospital settings, community group homes, with family or independently • O [Outcome]: Physical health effects of SB
The research question to be addressed was:
“What are the physical health effects of sedentary behaviour on adults with an intellectual disability?”
Search
Article eligibility criteria.
Information sources
A subject librarian assisted with performing the search for this literature review. The following six databases were searched: • EMBASE • Medline • CINAHL • PsycINFO • ASSIA • Web of Science
In addition, any reviews about health and sedentary behaviour that were discovered during the search process were searched for appropriate references.
Search strategy
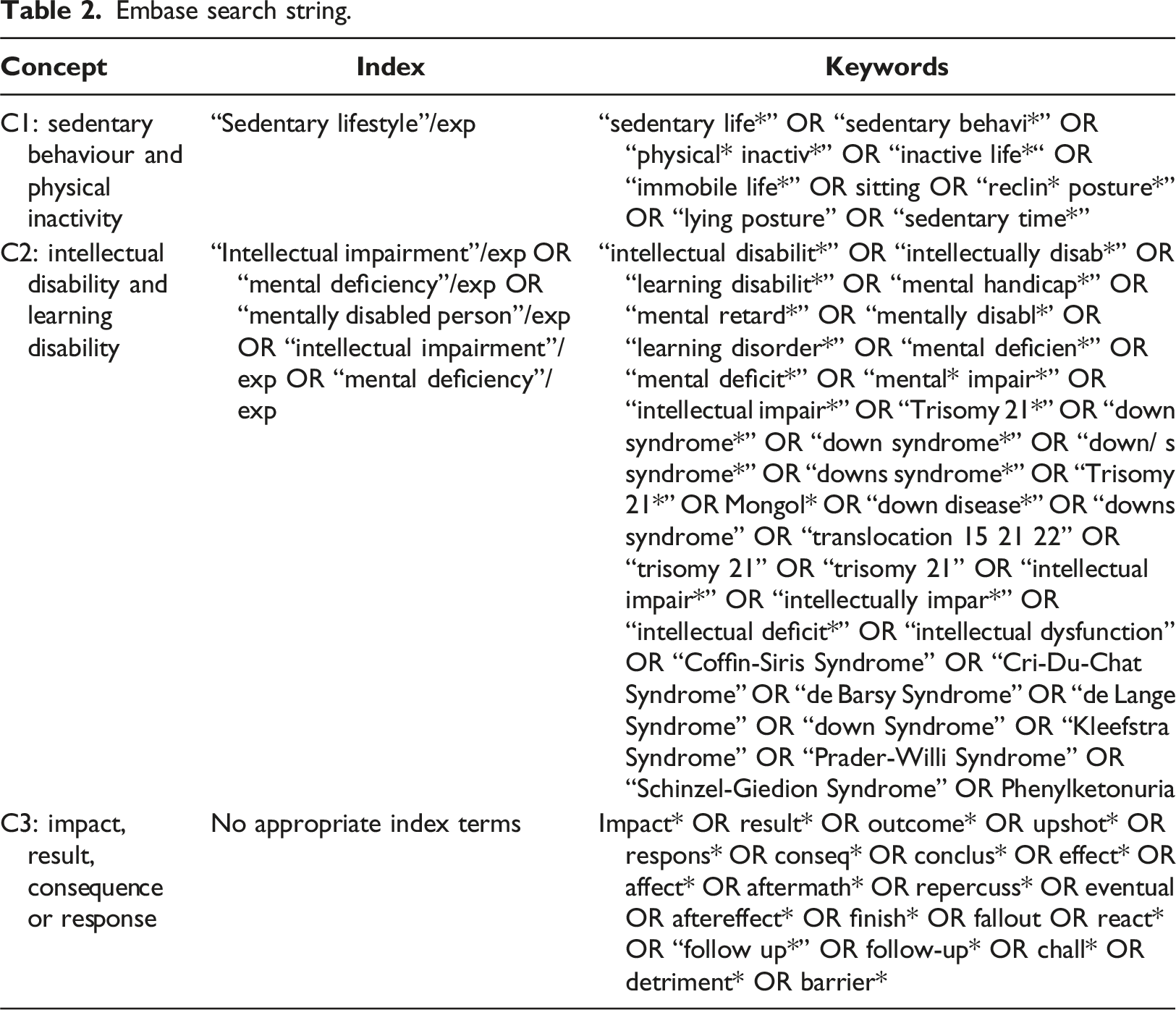
Embase search string.
Screening process
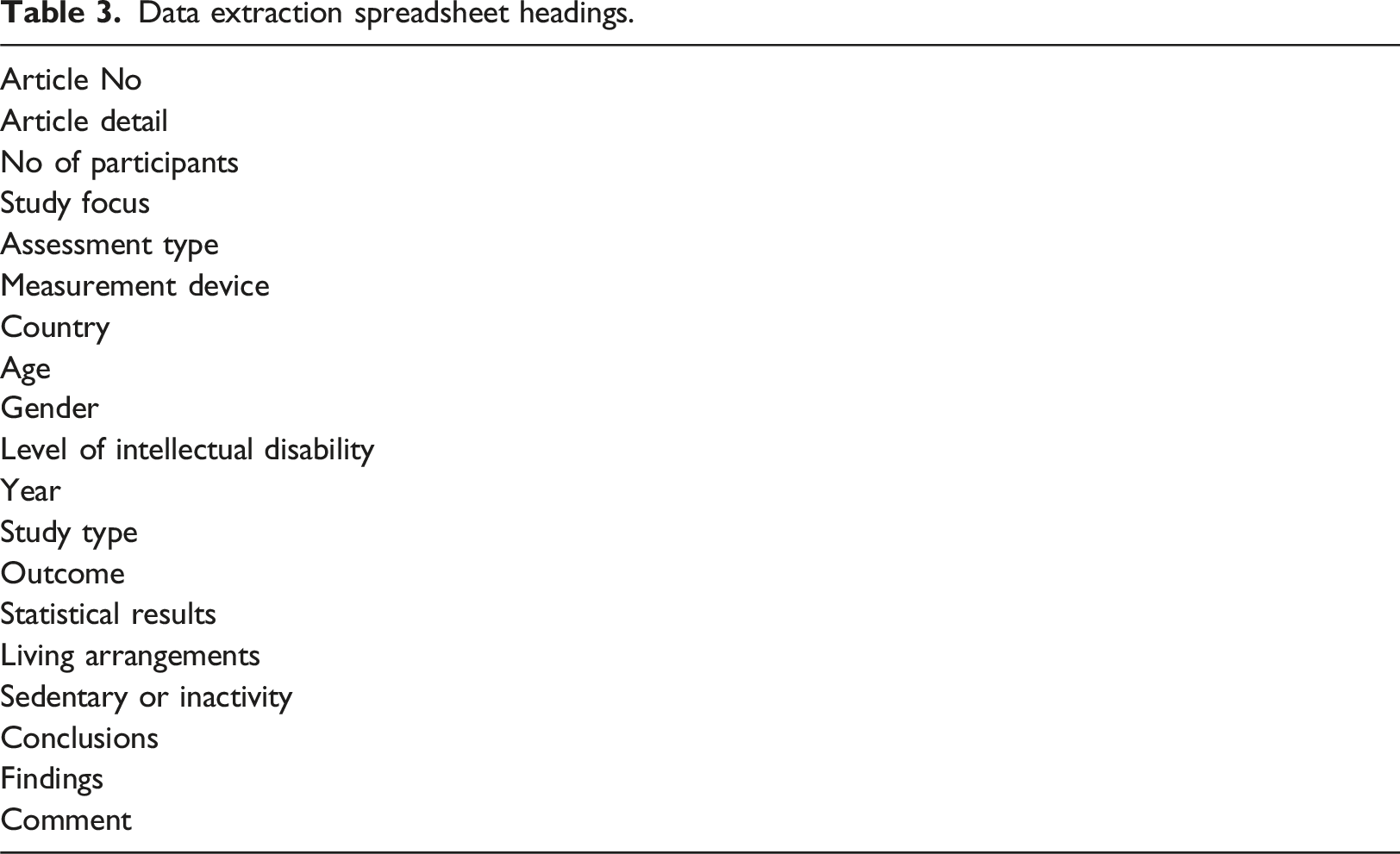
A PRISMA flow diagram was used to illustrate the article screening process. See Figure 1. The articles output from the search were imported into Covidence, which was used as the screening management tool. Duplicates were removed and all articles were screened by title and abstract by the assessor, who then executed a full article review on 27 articles. These 27 articles consisted of 6 articles unearthed from reviews and 21 articles from the original search. This screening process was verified by another assessor. Data from the 27 articles was summarised in an excel spreadsheet. The headings used in this data extraction spreadsheet are shown in Table 3. Prisma search. Data extraction spreadsheet headings.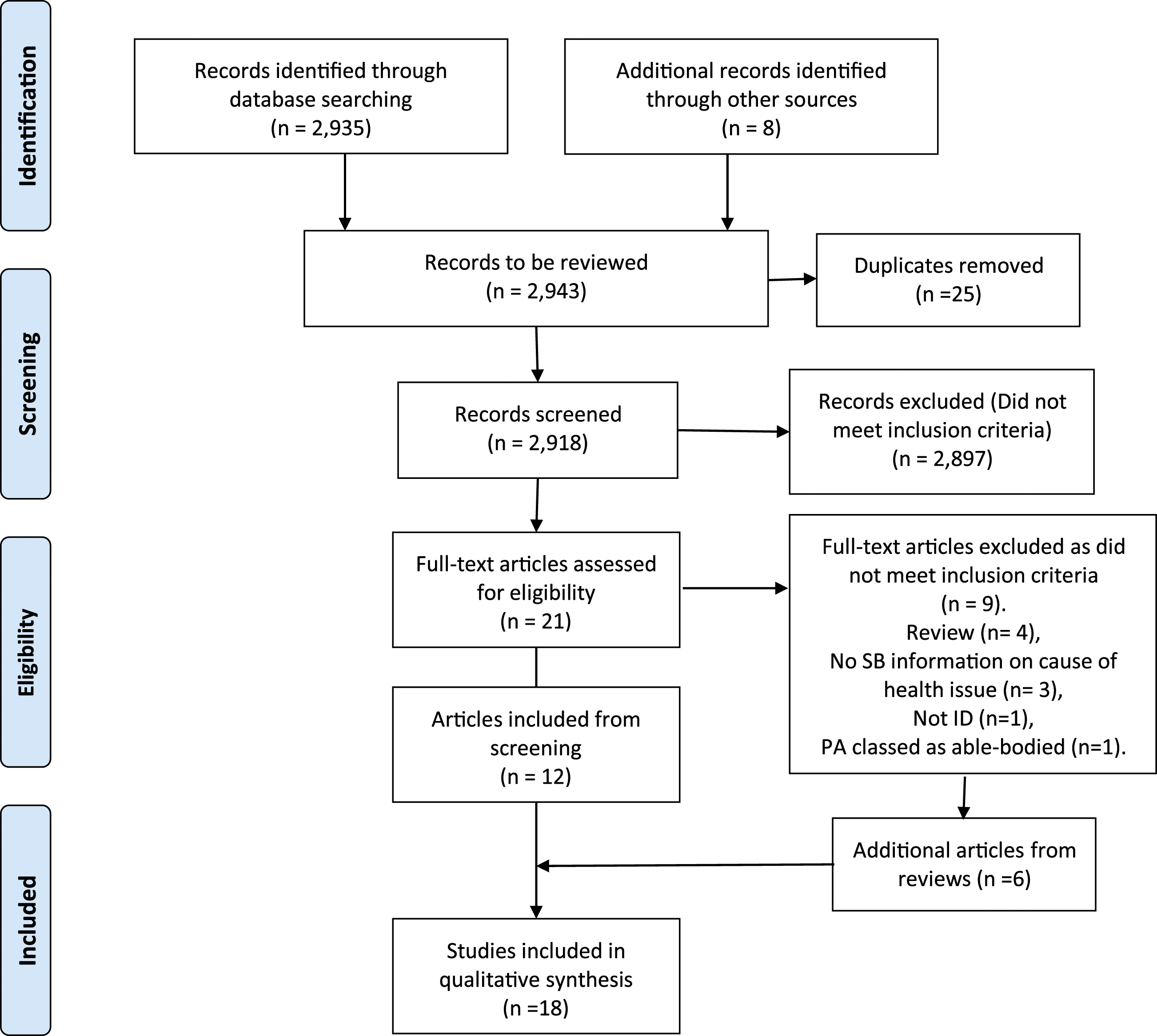
Data synthesis
Six step thematic analysis process.
Results
Final article summary.
Health themes and measurement.
Metabolic syndrome
Metabolic syndrome is the presence of a collection of coronary risk factors which increase the risk of heart disease, stroke and diabetes (Swarup et al., 2021). A Metabolic syndrome prevalence of 25% was found in a Dutch older intellectual disability population of 470 people but a significant relationship was not found between physical inactivity, as specified by the WHO, and metabolic syndrome (p = 0.26) (World Health Organisation, 2020). However, the observed levels of metabolic syndrome in this intellectual disability population were significantly higher than those observed in the general Dutch population, especially for those with mild intellectual disability but females were overrepresented by a ratio of 3:1 (De Winter et al., 2010). A Korean study with 17 participants with mild and moderate intellectual disability showed that metabolic syndrome risk factors of total cholesterol and LDL-cholesterol levels were significantly positively correlated to objectively measured physical activity (PA) levels. In addition, the study which had 3X more men than women, found that HbA1c was a predictor for PA (Kim and Yi, 2018).
Overweight and obesity
A Dutch study as part of the large cross-sectional study, Healthy Aging and Intellectual Disability (HA-ID), which investigated overweight and obesity in older adults with intellectual disability defined physical inactivity as taking <7,500 steps per day. Observed obesity levels were higher than in the general population (25.6% vs 9.6%) and a significant relationship between inactivity and obesity as measured by waist circumference and higher body fat levels, was found. These observed elevated levels of central obesity are a concern due to the potential increase of cardiovascular risks and link to Metabolic syndrome (De Winter et al., 2012). Engagement in moderate PA (MVPA) and hours spent watching TV were factors that were significantly associated with obesity levels in a longitudinal study on adults with intellectual disability. PA and sedentary levels were assessed by a single question and showed that almost one third of participants did not do any MVPA. While the obesity levels in the intellectual disability cohort ranged from 26 to 54% higher than those seen in the general population, the morbid obesity levels observed in the younger adults were twice that seen in the general population (Hsieh et al. 2014).
Multimorbidity and diabetes
In a UK study multimorbidity, which was defined as having two or more chronic conditions which negatively impact health and had a prevalence of 61.2%, was found to have significant associations with self-reported SB and doing less activity in a week, in a group of adults with intellectual disability. Obesity was the most common multimorbid condition seen with over 68.5% of participants being either obese or overweight (Tyrer et al., 2019). Of concern is that younger adults with intellectual disability were more than 14 times likely to be multimorbid than similar age groups in the general population (57.1 vs 4%).
An interview-based cross-sectional study on 147 participants with mild to moderate intellectual disability and Type 2 diabetes who lived in the community, demonstrated that over 79% had additional co-morbidities: cardiovascular disease (40%) and high cholesterol (16%) were the most prevalent. SB levels were high with only 26% reporting some level of activity daily but intensities were not assessed. In addition, over 20% had higher than recommended HbA1c levels and over 87% were overweight or obese (Bryant et al., 2018).
Cardiovascular
Wells et al. (1997) used health check and PA questionnaires to garner PA levels and CVD risk factors in a cross-sectional study with 120 participants. Over 51% of intellectual disability participants had done some form of moderate intensity activity in the preceding 4 weeks, compared to over 93% in a control group while over 48% of the intellectual disability participants had done no moderate intensity activity. There was a greater incidence of high body mass index (BMI) in the intellectual disability group, who were significantly heavier than the control group. In addition several intellectual disability participants had abnormal cholesterol levels. The study concluded that people with intellectual disability had higher risk factors for CVD and stroke than the general population. However, the study had no objective activity measures, the PA questionnaire was not validated and there was no information available on the amount of time spent being active. Moss (2009) looked at changes in Coronary heart disease after a PA intervention to assess risk. Pre-intervention results indicated that over 85% of the participants were inactive (i.e. they did not do any MVPA) and 67% were overweight or obese. However being active was classified as doing one or more session of MVPA a week which does not comply with WHO guidelines. Higher than recommended levels of glucose concentrations were observed in 28% of participants which could lead to increased risks of heart disease (Moss, 2009). Cardiovascular risk factors were investigated in a 2009 study on 470 older adults of all levels of intellectual disability but which had more females and more participants with moderate to severe intellectual disabilities in Holland. Results showed that while over 68% of participants had insufficient exercise levels, central overweight levels of 70.4%, hypertension of 36.8% and diabetes rates of 8.7% were similar to levels seen in the general population. However hypercholesterolemia levels were higher at 31.8% and SB was not investigated (de Winter et al., 2009, 2010). A recent longitudinal study showed that obesity and diabetes were significant predictors of high cholesterol and potentially heart disease in adults with intellectual disability. In this sample 925 participants, 57.2%, completed a 5-year follow-up. Almost 28% of participants were inactive, 36% were obese and 7.1% had diabetes. However, this study did not realise a significant relationship between elevated cholesterol and inactivity but measures of activity were by self-report and doing any form of activity would have registered as being active (1 = inactive, 0 = not inactive) (Murthy and Hsieh, 2021).
A 2012 study investigated the effect of physical inactivity on cardiac atrophy in people with an intellectual disability. Results indicate that cardiac size is significantly smaller in people with an intellectual disability compared to controls and that this cardiac atrophy was acquired through lifestyle habits such as more time in SB. The left ventricular (LV) mass index was inversely correlated with level of intellectual disability and positively related to PA levels and LV stiffness was significantly higher in adults with an intellectual disability compared to the control group. Physical activity levels of people with an intellectual disability were almost 2x less than the controls (p < 0.001) (Vis et al., 2012).
General health
Havercamp et al. (2004) found that compared to adults with no disabilities, adults with intellectual disability were significantly more likely to have fair or poor general health status and be sedentary, with over 33% reportedly having had no exercise in the previous month. However there were no objective measurements or quantifiable amounts of time in activity or SB specified. This 2004 study, which had a large sample size and was representative of all levels of intellectual disability, did not show any significant difference in the obesity or overweight status of the different groups which differs from later studies. Similarly Haider et al. (2013) found that, adults with intellectual disability had SB levels that were almost five times that of the general population (31.1 vs 5.3%), were perceived to have more “fair” or “poor” health, to have diabetes and were significantly more likely to be obese or underweight compared to the general population but concluded that this may be an under-representation due to the intellectual disability participants being identified from an administrative database. A pan-European cross-sectional study assessing the health of people with intellectual disability found that more than half the sample did little or no PA and were classed as sedentary and 41.4% did light activities for about 4 h per week. The study discovered that activity levels decreased with age and the number of people with intellectual disability diagnosed with diabetes, osteoporosis and hypertension increased with age but conclusions were not generalisable as samples were small and unrepresentative of the intellectual disability population in each country (Haveman et al., 2011).
A study assessing the correlates of SB found that physical and mental problems, assessed by a “yes” or “no” answer to a question, were significantly associated with objectively measured SB in a group of 152 adults with intellectual disability of all levels. This average measured sedentary behaviour was found to be 72.9% (Harris et al., 2018).
Bone mineral density
A study comparing bone mineral density (BMD) levels between individuals with Down syndrome (DS), intellectual disability and non-intellectual disability showed that individuals with DS had significantly less BMD than the other two groups. In addition, both intellectual disability groups had significantly less minutes PA per week but there was only a significant relationship between PA, as determined by walking levels, and BMD levels in the DS group which could pose increased risks of osteoporosis (Geijer et al., 2014).
Body oxidation
Research has implicated oxidative stress (OS), which is caused by an imbalance between free radical and antioxidant activity, in disease progression (Shruthi et al., 2021). Nitric oxide (NO) is an example of a free radical and is an inflammatory. Although the specificity of serum OS values has been questioned, a study showed significant elevated levels of serum global OS and NO levels in a group of sedentary adults with moderate or profound intellectual disability in residential care, as compared to an active control group (Carmeli et al., 2015). A second study which investigated the differences in plasma total antioxidant status using vitamin and enzyme levels between active and inactive female adults from a residential setting with unspecified intellectual disability levels, found that plasma vitamin levels were significantly lower in the inactive group, indicating that PA could have a protective effect on the antioxidant defence system (Carmeli et al., 2007). Although activity levels were not specified.
Discussion
Sedentary behaviour (SB) has only recently been recognised as a significant contributor to poor health outcomes (World Health Organisation, 2020). This literature review provides an insight into the emergence of SB as a significant risk factor for multiple diseases that affect adults with an intellectual disability and thus on the overall physical health of this population. It underscores the requirement for detailed studies investigating specific health problems for adults with intellectual disability and their relationship to SB using objective measurements. The results of this literature review have demonstrated that there is a scarcity of research into the effects of SB on the physical health of adults with an intellectual disability, with only eight articles directly investigating the effects of SB on any form of physical health, despite SB prevalence being identified at over 60% in adults with an intellectual disability (Lynch et al., 2021) and the fact that in the general population SB has been shown to have such detrimental effects (López-Valenciano et al., 2020; Owen et al., 2014; Vasankari et al., 2017).
Globally the leading cause of death is ischaemic heart disease and stroke and overall deaths due to diabetes increased by 70% in the 20 years from 2000 to 2019 (Vos et al., 2020; World Health Organisation, 2020). Coincidently levels of SB also increased for European adults in the same timeframe and have been linked to increased disease risk and health problems including cardiovascular disease (CVD), type 2 diabetes, obesity and some cancers (López-Valenciano et al., 2020; Owen et al., 2014; Vasankari et al., 2017). The leading cause of death worldwide is CVD and adults with an intellectual disability have increased risk factors for CVD as demonstrated by significantly higher BMI, greater obesity and inactivity levels, lack of moderate intensity PA, and elevated cholesterol levels (De Winter et al., 2010; Murthy and Hsieh, 2021; Wells et al., 1997; World Health Organisation, 2020). Furthermore, cardiac atrophy, which is a decrease in the myocardial mass, and can be associated with adverse health outcomes, was observed in adults with intellectual disability who exercised significantly less than the controls (Chyrchel et al., 2018; Vis et al., 2012).
According to the US Department of Health, Metabolic syndrome is the term used to describe a cluster of risk factors which can lead to health issues like heart disease and diabetes. Abdominal obesity, high triglyceride levels, high blood pressure and low HDL-cholesterol are examples of risk factors which can contribute to Metabolic syndrome (US Department of Health, 2020). Irrespective of activity level, increased time and fewer breaks in SB were found to be significantly related to a metabolic syndrome rate of 48.6% in a group of US older adults who were sedentary for over 65% of measured time spent wearing an accelerometer (Bankoski et al., 2011). There were no similar studies in the intellectual disability community looking specifically at SB and metabolic syndrome and although higher levels of metabolic syndrome were seen in a Dutch intellectual disability population, no significant relationship was found with PA but SB was not investigated (De Winter et al., 2010). An unsignificant relationship was found between high cholesterol and inactivity despite 36% of the 925 participants being obese while an inverse relationship was observed between levels of diabetes, osteoporosis and hypertension and activity levels as an intellectual disability cohort aged (Haveman et al., 2011; Murthy and Hsieh, 2021). Similarly, the WHO’s definition of metabolic syndrome requires the presence of at least three risk factors i.e. insulin resistance and two risks of either obesity, dyslipidemia or hypertension (Alberti and Zimmet, 1998). While these risk factors are highly prevalent in the intellectual disability population, studies evaluating them collectively are rare so it is difficult to ascertain the actual prevalence of metabolic syndrome. However, obesity and overweight, key risk factors in metabolic syndrome, have been shown to be a critical problem in intellectual disability studies. For example, in Tyrer et al. (2019), 68.5% of intellectual disability participants were either overweight or obese while another intellectual disability study showed 87% of participants were overweight or obese and morbid obesity levels were twice that in the general population (Bryant et al., 2018; Hsieh et al., 2014). Ryan et al. (2021) found that overweight and obesity levels were in excess of 69% in a cohort of older adults with intellectual disability and that those who were obese were nine times more likely to have respiratory issues, which was the largest cause of death for this population (O’Leary et al., 2018). In another study, elevated obesity levels were significantly related to activity levels, but sedentary levels were not investigated (De Winter et al., 2012). Moss (2009) discovered that 67% of their study participants were obese with 28% having elevated glucose levels, while over 85% did not achieve recommended PA levels. Equally, sedentary levels of five times the general population were seen in an intellectual disability cohort who were significantly more likely to be overweight (Haider et al., 2013). A 2004 study by Havercamp and colleagues also found that people with intellectual disability were more sedentary that the controls but conversely there were not significant differences in weight status (Havercamp et al., 2004). Despite the overall negative health effects of obesity, a study found that obesity had a protective effect for osteoporosis, a degenerative disease which increases bone fragility, where obese adults had higher bone mineral density (BMD) than normal-weight participants (Qiao et al., 2020).
Bone mineral density (BMD) is a measure of the strength and integrity of bones and low measures are indicative of the presence of osteoporosis (Kanis et al., 1994; US Department of Health and Human Service, 2004). A cross-sectional study highlighted the poor bone status of a cohort of adults with intellectual disability, where over 30% and 40% had osteopenia and osteoporosis respectively, indicating an increased risk of fracture due to diminished bone integrity (Burke et al., 2019). Another study which compared post-fracture mortality rates between privately insured adults with and without an intellectual disability showed that those with an intellectual disability were at a greater risk of mortality a year after the event occurred (Whitney et al., 2019), emphasising the importance of improving the bone health of adults with an intellectual disability. The National Health and Nutrition Examination Survey (NHANES) study showed a negative association between time spent sedentary and femur BMD, independent of PA level in neurotypical women (Chastin et al., 2014). A study which compared PA and BMD for a group of adults with and without intellectual disability, found that adults with an intellectual disability had lower BMD and that there was a significant relationship between BMD and PA level only in adults with down syndrome (DS), who consequently had an increased risk of osteoporosis (Geijer et al., 2014). While DS is a known contributor to decreased BMD it is a concern that all adults with intellectual disability had low BMD and warrants further investigation of risk factors (Angelopoulou et al., 1999). Thus bone health appears to be an issue for adults with intellectual disability irrespective of aetiology and while a causal relationship has not been explored with SB, it is something that warrants investigation.
Oxidative Stress (OS) is caused by an imbalance in the body whereby an excess of reactive products (free radicals) can lead to cell and tissue damage and consequent progression of diseases like diabetes and hypertension (Pizzino et al., 2017; Taniyama and Griendling, 2003). Two studies investigated the oxidative status of people with intellectual disability, one looking at sedentary behaviour and the other at PA. Comparisons between sedentary and active groups showed raised levels of free radicals were present in the sedentary group (Carmeli et al., 2015). The second study concluded that PA had a protective effect on the body’s antioxidant status when higher plasma vitamin levels were discovered in an active group of adults with intellectual disability compared to an inactive group, although the level of PA was unspecified (Carmeli et al., 2007). Antioxidants such as vitamins and minerals are capable of neutralising these damaging free radicals and protecting the body from disease (Dal and Sigrist, 2016). Unfortunately, the dietary intake for people with intellectual disability has been noted to be poor, with high energy foods and less nutrient-dense selections prevalent, irrespective of their living circumstances, so they may not be getting the required antioxidants from food to combat the negative effects of sedentary behaviour (Adolfsson et al., 2008; Hamzaid et al., 2020).
Multimorbidity is defined as having two or more chronic health issues (van Den Akker et al., 1996). Chronic health conditions, also known as noncommunicable diseases, last for more than 1 year and require ongoing medical care (CDC, 2021). The primary chronic conditions of cardiovascular disease, respiratory disease, cancer and diabetes account for 80% of deaths, with the main contributors of disease coming from the environment, behavioural, physiological and genetic factors (World Health Organisation, 2016). Adults with intellectual disability are at a greater risk of having more chronic health conditions and more likely to lead a sedentary lifestyle (Havercamp et al., 2004). A multimorbidity rate of 71% was observed in the IDS-TILDA longitudinal study, where hypertension and gastrointestinal disease were ubiquitous (McCarron et al., 2013). Sedentary levels were found to be significantly correlated with multimorbidity in a group of adults with intellectual disability while another study showed that over 79% of adults with intellectual disability who had diabetes, also had other health issues like high cholesterol and CVD (Bryant et al., 2018; Tyrer et al., 2019). Although multimorbidity and SB appear to be more widespread in adults with intellectual disability, limited studies have investigated the link, while in the general population these two aspects of health have been studied and a relationship well established (Lewis et al., 2016; Thorp et al., 2011; Vankampfort et al., 2017). In addition, the Irish Longitudinal Study on Aging (TILDA) proposed that a linear dose-dependent association between chronic health conditions and sedentary minutes per day existed (Kandola et al., 2020).
An observation in some studies was that people with a milder intellectual disability who lived more independently were more at risk of unhealthy behaviours and needed more guidance on health risks (de Winter et al., 2009).
People with intellectual disability have significantly poorer health and health outcomes than their peers in the general population (Emerson et al., 2016). In addition, some studies found that people with intellectual disability were more likely to perceive themselves as being in “poor” or “fair” health (Haider et al., 2013; Havercamp et al., 2004). Furthermore, in a group of adults with intellectual disability, perceived physical and mental problems were significantly associated with sedentary levels of 72.9% (Harris et al., 2018). Thus this population’s self-perceived and measured ill-health could be related to elevated sedentary levels. However while the information showing a contributory effect between sedentary behaviour and poorer health in the intellectual disability population is not conclusive, existing studies have shown that higher levels of sedentary behaviour are present in the intellectual disability population, who predominately feel they are not in good health and have more issues being overweight and obese, have excessive chronic health conditions and suffer from metabolic syndrome.
Conclusion
This literature review has demonstrated that sedentary behaviour (SB) could be a contributor to the poor health which is common in adults with an intellectual disability. The limited studies have shown a prevalence of obesity, multimorbidity and metabolic syndrome as well as elevated levels of SB. However the body of evidence, which is primarily focussed on cross-sectional studies to date does not confirm a cause-and-effect relationship. Further research is required looking specifically at sedentary behaviour and its effect on particular health aspects of adults with an intellectual disability like the excessive obesity levels, multimorbidity and metabolic syndrome. These studies should ideally use objective measurements for accuracy. Thus an in-depth understanding of the health effects of sedentary behaviour on adults with an intellectual disability may be achieved and suitable recommendations made to expediate change, health improvements and consequently improved quality of life for this vulnerable population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the IDS-TILDA-2018-1 which is funded by the Health Research Board and the Department of Health: [details omitted for double-anonymized peer review].