
Abstract
Parents of children with Down syndrome (DS) were interviewed about if their experiences raising their children matched their initial assumptions about parenting a child with DS. A dominant narrative was identified, wherein most parents described initially having negative assumptions, which did not come to fruition; parenting their child was not very different from parenting a typical child. There was also a sub-group of participants who disputed the dominant narrative; parenting their child was challenging and the dominant narrative marginalizes that experience. The findings indicate that although for many parents, having a child with DS is like “taking the scenic route” (i.e., it involves a few more hurdles, but often more rewards), this framing is not always applicable. Therefore, health care providers and support organizations should promote a narrative that encompasses the diversity of parenting a child with DS.
Introduction
Down syndrome (DS), or Trisomy 21, is a genetic condition caused by the presence of extra chromosomal material associated with chromosome 21 (Canadian Down Syndrome Society, N.D.). Individuals with DS may experience the same medical issues as their typically developing peers but have an increased probability of experiencing certain medical conditions, including congenital heart disease, celiac disease, leukemia, hypothyroidism, diabetes, autism, visual and auditory impairments, seizures, and dementia in older age (Grieco et al., 2015). A determination of DS is made either during the pregnancy via prenatal testing, or, postnatally, via karyotyping (Buyukavci et al., 2019). Most parents who have a child with DS became aware of their child’s determination after birth (Skotko, 2005a). However, prenatal determination is not uncommon; it is simply that the majority (an estimated 67–92%) of those who receive a prenatal determination choose to terminate their pregnancy (Mansfield et al., 1999; Natoli et al., 2012).
Concerns about the quality of life for the unborn child are cited as some of the most common reasons for ending a pregnancy because of a prenatal DS determination (Korenromp et al., 2007). These concerns include fear the child will never be independent, concern the “abnormality” will be too severe, concern over the child’s care after their parents’ death, and general worry about the level of respect for children with disabilities in our society. Inversely, continuing a pregnancy with DS is more likely when the decision-maker believes they have social support in parenting a child with DS (Lawson, 2006) and when they have greater knowledge about available services for individuals with disabilities (Roberts et al., 2002).
The historical narrative of having a child with DS often follows a deficit framework (Nelson Goff et al., 2013), with there being a focus on how children with DS interfere with, or disrupt, parent and family functioning (Cahill and Glidden, 1996). The literature has traditionally presented the birth of a child with a disability to lead to a universal parental experience of extreme sadness, all-consuming helplessness and guilt, mental anguish, and a perpetual state of “mourning” (Lalvani, 2008: p. 436) for the typically developing child that could have been. Although parents of children with DS do report certain difficulties more frequently than do parents of typically developing children, such as more behavioral problems (Stores et al., 1998; Gau et al., 2008) and more time spent on caregiving duties (Barnett and Boyce, 1995), parents of children with DS also experience some relative self-reported benefits compared to parents of typically developing children (e.g., less likely to get divorced, greater satisfaction with support from friends and community groups; Erickson and Upshur, 1989; Urbano and Hodapp, 2007). They also report similar levels of marital satisfaction (Van Riper et al., 1992), stress (Stores et al., 1998), family cohesion (Thomas and Olsen, 1993), and confidence in parenting skills (Rodrigue et al., 1992), as families with typically developing children.
The positive adjustment of parents of children with DS relative to parents of children with other intellectual/developmental disabilities has been so prevalent that it has been referred to as the “Down syndrome advantage” (Hodapp et al., 2001; Stoneman, 2007; Corrice and Glidden, 2009; Esbensen and Seltzer, 2011). While some findings have suggested that the advantage can be attributed either solely or largely to confounds such as advanced maternal age or higher income, factors which are independently related to positive adjustment in parents (Blacher and McIntyre, 2006; Stoneman, 2007; Corrice and Glidden, 2009), others have suggested that although the DS advantage is small, it is consistent and can be attributed to higher functioning ability of individuals with DS, which contributes to higher wellbeing for caregivers (e.g. Corrice and Glidden, 2009; Esbensen and Seltzer, 2011). While the debate about the nature of this advantage is ongoing (Flaherty and Glidden, 2000; Corrice, and Glidden, 2009; Esbensen and Seltzer, 2011; Glidden et al., 2014), it is clear that, on average, the adjustment of parents of children with DS resembles the adjustment of parents of typically developing children more than it differs (Glidden et al., 2010).
Despite the positive experiences re-counted by parents of children with DS, parents have reported in several studies that the description of DS they received upon their child’s determination was disproportionately negative (Hedov et al., 2002; Buyukavci et al., 2019). Mothers report that physicians tend to emphasize the negative aspects of the condition, deemphasize the positive, and imply or explicitly state that the birth of a baby with DS is a regrettable happening (Skotko, 2005b). Care providers often focus on “lethality of the condition, morbidity and burden,” (Wallace et al., 2018: p. 660). Those who received the determination prenatally reported feeling pressured by their health care provider to terminate the pregnancy, a finding which is common (e.g., Guon et al., 2014; Wallace et al., 2018).
Advocates and researchers have thus argued that more “balanced information” is needed in advance of prenatal screening, and upon receiving the results of a prenatal determination in order to promote more informed decision making and more positive experiences with health care provision (Roberts et al., 2002; Grant and Flint, 2007; Lawson and Walls-Ingram, 2010; France et al., 2012; Guon et al., 2014). Several researchers have suggested what a “balanced” description should entail (Bryant et al., 2001; Roberts et al., 2002; Williams et al., 2002; Lawson and Walls-Ingram, 2010; France et al., 2012). However, others have argued that although the notion of balance in a description of parenting a child with DS is theoretically desirable, it may be practically impossible, as the experiences of parents are extremely varied (Ahmed et al., 2007; Hippman et al., 2012). Hippman and colleagues (2012) argued that, instead, it would be more helpful to explore the range of possibilities regarding the family experience of raising a child with DS and help families evaluate these possibilities in the context of their own lives.
The current study was intended to contribute to understanding the range of possibilities regarding the family experience of raising a child with DS 1 . In particular, the goal was to investigate how parents of children with DS understand and make meaning of their parenting experience and if there are dominant ways that they do so. This study exemplifies taking a critical stance towards taken-for-granted ways of understanding the world, which is a key principle of constructionism (Burr, 2015).
Methods
Ethical considerations
This study was approved by the University of Saskatchewan Research Ethics Board (November 9, 2016). All participants provided written informed consent prior to the interview process. Any identifying information was replaced with pseudonyms to protect the participants’ identity.
Recruitment
Participants were recruited via the provincial Down Syndrome Society, posters, social media, a university’s online messaging board, and a local organization for individuals with disabilities. Interested participants independently contacted the researcher based on an invitation/request that outlined purposes of the interview, an outline of the interview, and the value of these participants’ contributions.
Participants
Participant determination by year.
Data collection
Participants took part in in-depth interviews that ranged from 19 to 105 minutes in length. All interviews were audio-recorded and later transcribed verbatim. Interviews occurred at a location identified as convenient by the participants. After receiving informed consent from the participants, the narrative interview followed an open-ended format with an initial story request 2 . After several of the first participants spontaneously discussed how their life had changed (or not) because of having a child with DS, this was subsequently included as a standard interview question because it was evidently a salient issue for participants. Responses to this question formed a large part of the analysis presented here. Many participants spoke for over 30 minutes unprompted after the initial narrative request, following which the researcher probed to elicit more detail about salient events, clarify meanings, or if participants did not spontaneously provide information about an issue relevant to the study, the researcher asked them follow-up questions to fill in those gaps.
Data analyses
The narratives were analyzed thematically (see Braun and Clark, 2006; Riessman, 2008) using NVivo as a data organization tool. First, narratives were “lumped” (see Saldana, 2015) into chronological plot points (e.g., “initial reaction to determination”; “turning point”; “retrospective evaluation of initial reaction to determination”; “life now”). Then, data extracts relevant to these plot points were inductively coded in order to identify elements of participants’ experiences that corresponded with or diverged from each other’s and allowed for an analysis of these areas of convergence and divergence. Then, patterns (i.e., repeated words, phrases, thought patterns, or topics in participants’ statements) within each narrative as a whole were explored and described in order to arrive at a core narrative arc of each story. The core narrative arcs were then compared across stories.
Results
Analysis of the data elicited three distinct and salient narratives. There was a dominant narrative—“it’s like taking the scenic route”—in which parents described that their lives are significantly improved because of their child with DS and that parenting them has not turned out to be as challenging as they initially anticipated. Many participants compared parenting a child with DS to parenting a typical child, with a few more hurdles but also often more rewards. Participants’ narratives often included a turning point wherein the devastation of the initial determination eased, their initial concerns were revised, and life became easier. They relayed that the change in trajectory was facilitated by getting used to the idea of DS through time, getting to know their child, and getting to know other parents and children with DS which normalized their experience and provided them with a sense of belonging. There was also a small sub-group (n = 2) of participants who recognized the dominant narrative and challenged it—“not all children with Down syndrome are the same child”. Their children with DS had significant challenges and parenting them was not at all like parenting a typical child. They felt marginalized and silenced in the DS community. In addition, there was one participant who represented the “third narrative”, which is the story of deciding to terminate a pregnancy with a DS determination. Since only one individual who terminated their pregnancy volunteered to participate in the study, the story of people who make this decision remains largely untold here. However, the third narrative converges and diverges with the dominant and sub-narratives of those who had children with DS in interesting ways.
“It’s like taking the scenic route”: The Dominant Narrative
The three types of narratives were indistinguishable at the outset; most participants were devastated when they first received their child’s DS determination: …it felt really desperate and I was devastated. There was so much— more emotion than I’ve ever dealt with. Like, just sobbing my eyes out. My heart felt like it was breaking. I have never cried so hard for so long, or so much. (Camille)
The narratives diverged, however, in their retrospective evaluations of that initial reaction. According to the dominant narrative, that devastation was ultimately an overreaction, and did not play out in parents’ experiences parenting their child: …we got the results back that he had Down syndrome, and it was really hard, I mean, like now it seems like “what’s the big deal?”… like thinking about how I felt before I met him and the fear and the um, “I don’t want that” I just feel awful even thinking it right? Because he’s just awesome. Like I mean he’s a challenge, but so are our other kids. Like just parenting in general is a challenge and so he has different challenges at times, but no more difficult. (Zadie)
“When She Was A Few Months Old It Hit Me... We’re So Lucky”: The Turning Point
According to the dominant narrative, while the time around the determination was one of the most difficult periods in participants’ lives, they eventually experienced a turning point and things began to feel easier. Sometimes participants described a particular moment that was a catalyst for a changed perspective. For example, Arthur recounted a night early on in parenting his new child, in which he had a breakdown, followed by deciding to “suck it up”:
I was home with my kids alone, and I was laying in the grass and thinking, like I just can’t do this, right? … And then I got up and went back in and just I said “Ok I’ve got to suck this up and figure this out” right? … I just remember that moment… Because life doesn’t stop and wait for you to catch up, right? So you’ve got to figure it out.
Often, the change in perspective occurred over time. For example, Joan attributed the positive transition to becoming educated about DS, being guided by community (health/social/educational) supports and services, and connecting with other parents:
That was, it was a tough few months, for sure… and then, it’s just been
— I don’t know, it gets easier. Like it’s just gotten a lot easier. We connected with parents, we networked with parents, our team at [organization] really picked us up and we really just let them kind of take us under their wing and navigated that system. I immersed in the next year in research and finding, you know the best techniques, and we soon found where services were lacking here so we went to [Canadian province] for a few of his services… Um, I felt so much better once I started networking with parents…It was amazing. Just amazing. It was the best therapy I’ve ever had, in life.
A few participants explained that the way they perceived the situation changed when they became exposed to positive messaging from other parents of children with DS. For example, reading parent accounts online made Simone change her perspective on her child’s DS. She went from pitying her family to believing they were lucky to have their new addition:
And then it was when she was three and a half months old, all of a sudden it just like
— and it was quite a sudden change… just probably realizing that she’s not going to be a burden, like she’s going to [pause] be a blessing. And probably a lot of it was from stuff that I found online too. And personal like, everyone, it seemed like everyone who had a kid with Down syndrome felt like they were lucky. And that’s when it kind of hit me, when she was a few months old that we’re actually, like, really lucky.
Acceptance facilitators
Many participants framed their changed perspective as “accepting” the determination and their new life circumstances. When they were probed to explain what facilitated this change, participants described simply taking time to adjust, getting to know their child, and connecting with other parents of children with DS as what made the difference for them. Some participants explained that time, and “go[ing] through your everyday process” (Sylvia), was the biggest factor that helped them to accept the determination. Another parent, Alma, described time as a healer:
Time. I think time was the
– it’s the biggest healer…there was always awesome days…But I would have bad days quite a bit when we first got home. But over time, those bad days just started going away.
One father, Arthur, explained that personal growth over time is what has allowed him to accept his new reality:
Time, mostly, you know. Getting to adjust to it… And it took a long time to come around… it was really tough to integrate…. And I don’t know exactly what made the transition. It was probably I think growing as a person myself, you know, having seven years to mature…
Several participants explained their perspective on the situation changed when they got to know their new children and experienced the positive aspects of parenting them: For me I think it was just spending time just being with him, bonding … and getting to know your baby and the rest pretty much follows because how can you not love them? (Harper)
Another mother, Zadie, explained that once she met her child and discovered their individuality and personality, she changed her mind about what parenting a child with DS would be like:
I mean getting to know [child]…that unknown is gone and there’s this happy kid who’s just like any other kid. I think that learning that part
– people could have told us over and over again, “he’s going to be like every other kid” but I don’t know that it would have sunk in until actually meeting him.
For most parents, connecting with other parents of children with DS and seeing/meeting other children and adults with DS was cited as an extremely positive experience, fostering their acceptance of the determination, and helping them to feel positively about the future. Numerous parents explained that the benefit of talking with other parents was their ability to normalize the situation for them—to hear and see that their child would be, in essence, a child like any other. For example, Edith, explained that talking to a mother of a child with DS was a huge relief because it made her realize that so much of her parenting experience would be like that of a typical parent:
She was telling us stories about her little girl and you know funny things that she did or when she reached a milestone or her birthday… was like really helpful… you could see her growing up and it was like “Oh, ok, she’s just like a normal kid… She’s not as quick to develop as other kids but she seems like pretty cool.” So it was like a big sigh of relief, like I felt like I could breathe again and you know I felt like my little girl wasn’t going to be just this Down syndrome diagnosis. She was going to be like our little girl.
As well as meeting individual parents, joining DS support organizations and feeling a sense of belonging in the larger DS community was an important part of reinterpreting the determination as positive. For example, Joan explained that she first experienced the support of the DS community when she went to a Canadian Down Syndrome Society conference, where she met other parents of children with DS as well as individuals with DS. She described the sense of empowerment and potential that she experienced from the conference:
…we went to the national Down syndrome conference… and that was AMAZING...there were parents of babies, and there were parents of
school-aged
kids, there were parents of toddlers, parents of university students, and there were
self-advocates
there. So I could see people with Down Syndrome… living successful amazing lives… So when we came home from there I said “this is it. I can’t stop this feeling now.”
For Ernest, who first connected with another parent prenatally, meeting them and their child counteracted the stereotypes that he had about DS by confronting him with the individuality of another human:
It takes away the fear, the threat of a person with Down syndrome, right? Like you see the stereotype… but when you see a human you value them as a human.
For several participants, connecting with other parents was a positive experience because it was validating to be around people who understood what they were experiencing: …it’s so refreshing when you find people that are your tribe. Like people that get it. Like some people think they get it, but they only get it so far. There’s other people that have lived it. So even how you express your feelings and the stress of all of the appointments you have to go to. Other people— many other people that were parents of typical children— they don’t get that. They don’t understand that stress of it… it’s refreshing when you can talk to someone and they get it. (Ernest)
“I Kind Of Forget That [They] Have Down Syndrome”: Life Now
Most parents relayed that eventually their life has improved because of their child with DS (“it’s been a positive thing overall…he’s just so awesome”). As Harper stated, they face challenges and have bad days, but overall, the value of their child outweighs the negative experiences:
It’s not always easy. It’s not always rainbows. There are days when you’re ready to toss in the towel, but the good days FAR outweigh the bad and that’s —not that they’re bad but the difficult times I guess I should
say—and
that’s something that I wish I would have been told at the time.
Several parents explained that from their perspective, their child with DS is “one of the best things that ever happened” (Maude) to them and a “blessing” (Jane). Sylvia explained that life with her child is not life as she expected it would be, but that it is better: “you know, I just wanted something that was normal. But [child] is far better than normal.” Likewise, Chloe reflected that her life had changed more than she imagined it would, and that in contrast to what she was expecting when she received the determination, she considers her family to be lucky to have their child with DS:
It’s definitely changed it all. But, more like for the better. More than I could have ever imagined it would ever be. And I often say that realistically we’re the lucky ones because we have [child]. Um, everybody else are the ones missing out. Because they don’t get to experience what we get to experience. Because it truly is amazing.
Most parents relayed that parenting their child is like parenting any other child but with a few more challenges and more time commitment. Agatha compared the extra time raising her child takes to “taking the scenic route”:
…it’s not scary. It’s just like raising any other kid, it just takes a little longer. It’s like, I tell people that it’s like taking the scenic route, and it’s just as fun and just as beautiful.
A few parents described how, in contrast to the focus on DS when their child was first born, the fact that their child has DS is no longer central to their families’ lives, or to their thoughts about their child: …my mom said to me the other day, she goes “you know I kind of forget that [child] has Down syndrome”. Like at the time when you’re pregnant, that’s the only thing you think about; you think that you’re not going to forget or that you couldn’t possibly imagine that you wouldn’t be thinking about it. And you do slowly start to like— it’s like, that’s just [child]. (Ursula)
Kurt explained that he does not parent his child with DS differently than he does his children who do not have DS. He explained that while they anticipated negative change when they received their son’s determination, their lives have changed positively, not because of DS, but simply because of having another individual in their family:
I don’t parent any different. I don’t believe [child] consumes any more or less time than the rest of our children. He probably gets the least amount of attention, quite realistically, right? The fact that he has Down syndrome, you know, hasn’t changed our lives in the way that we thought it would at all. It’s changed
— he’s changed our lives tremendously but not anything more or less than any other child without a Down syndrome diagnosis would.
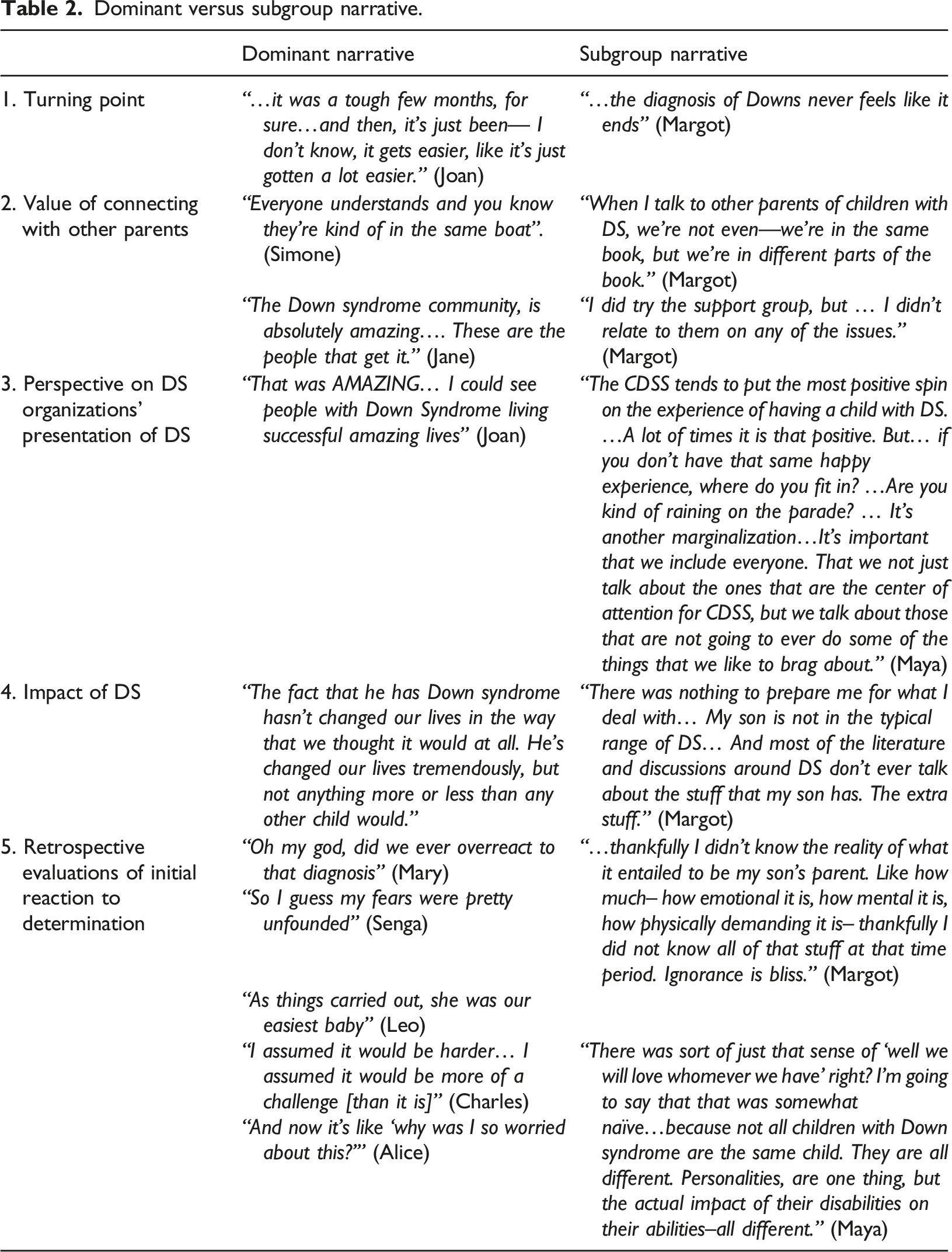
“Not all children with Down syndrome are the same child”: The Sub-Group Narrative
Dominant versus subgroup narrative.
In contrast to the parents who felt understood and empowered by being around other parents of children with DS, parents in the sub-group described feeling silenced by the DS community. One mother felt like no one wants to acknowledge or discuss the difficult aspects of life for many people with DS, and since her son’s life involves many challenges, that leaves her without a sounding board: A lot of us that don’t have high functioning kids get silenced when we mention you know, our experience… there is no one to talk to when your child is not high functioning. There’s no one. Because no one wants to talk about that. (Margot)
Margot also explained that she was concerned that representations of people with DS by DS support organizations and most parents of people with DS tend to focus on high achieving people, when that does not represent the reality for most people with DS. She wondered about the repercussions of this public image for policy about DS:
And
I—what
scares me as a parent, and I see this more and more on social media is they are showing all these savants of Down syndrome people, you know like a lady who’s been a preschool teacher, and dance instructor, and I have concern in terms of policy, and now maybe this is just me thinking too much…but I’m concerned that the government is going to say “well hey, if Down syndrome people can do this, why do they need
one-on-one
support in the education system? Why do they need all this help when they could be a teacher or a dancer, or? So I have concern about all the spotlight being put on the savants, in terms of the reality of it is, is that most of our kids are not going to do that stuff.
While most parents found social support and inspiration in DS support organizations, the subgroup of parents felt marginalized by the narrowly positive view they presented. Although these parents believed that it was appropriate for the DS community to celebrate the accomplishments of individuals with DS, they also perceived the celebration to be disproportionately focused on “high-functioning” individuals with DS. The parents pondered what that meant for the inclusion of them and their child. One mother, Maya, described that what resulted was a kind of marginalization of the sub-group of people with DS that do not fit the narrative of high achievers. She emphasized the importance of celebrating people with all ranges of abilities and that true inclusion means valuing people apart from their accomplishments and making space for and validating all experiences:
It’s important that when research is done about people with Down syndrome, that we include everyone. Right? That we not just talk about the ones that are the centre of attention for CDSS, and so on, but we talk about those that are not going to ever do some of the things that we like to brag about… Because I, at the bottom of my heart I know [child] was supposed to be here, that she was just as valuable as anybody else and that people, again, when people decide whether they are going to terminate or not, they need to understand that, you know what, yeah, you might end up having a child that has MORE needs, and more severe disabilities. That is, that’s life.
“Sometimes people have to make difficult choices for a number of reasons”: The Third Narrative
Only one individual, Judy, who chose to terminate her pregnancy volunteered to participate in the study, so the story of people who make this choice remains largely untold here. However, Judy’s story illustrates some interesting convergences and divergences with the dominant and sub-narratives of those who had children with DS. Her story was not so different from the dominant narrative when she first found out about the possibility of DS. She and her partner had concerns about their capacity to parent a child with a disability (“we were just fairly definite that we weren’t prepared to deal with the level of need that this baby would have”), concerns about the lack of support available to them (“we live on a farm… who the hell would help us out here?“), and concerns about discrimination and isolation for a child with DS (“to be shunned and to not ever fit in”), which align with the concerns of other participants in this study. Judy’s screening showed indicators that their child would likely not survive, which made their decision to terminate more straightforward, but was not ultimately the deciding factor for termination. They did not want to parent a child with DS. Her partner insisted that this was not the child he wanted (“My husband is not very tolerant of people who are different… he just did not want to be the parent of THAT kid.”).
It might be tempting to argue that the couple made their decision to terminate based solely on unfounded negative assumptions about DS, because most parents, in this study and others, end up reporting more positive than negative outcomes of parenting their children with DS, and that parenting a child with DS is not that different from parenting a typical child. However, it is impossible to know if this couple’s concerns would have come to fruition or not. Although many parents of children with DS framed their experience as “taking the scenic route”, the sub-group narrative illustrated that the story is not that simple for everyone. In fact, some of the couple’s concerns were starkly played out in the sub-group’s narrative. For example, during their discussions about termination, Judy relayed that her partner “made the comment, ‘who would ever play with our child?’ and I think he just— the idea of— and he said it would just be heartbreaking”. Although some parents’ children had a different experience, like Alma, who recounted that “he makes every room better. Like whenever he’s around, people will flock to him. ‘Cause he is, he’s a lot of fun”, another mother explained that her child’s lack of friends was indeed extremely challenging for her: Probably the hardest— is the lack of friends for him. That’s really hard. Now I shouldn’t say, ‘cause there is a little boy that lives across the street from us… and he does come over and hang out with [child] occasionally, but I can already see that he’s [pause] moving past, right? That he’d rather do other things, cause my son only likes to do like two or three things. And that, you know, that is hard to watch, because my son loves him, so much. (Margot)
Given the experiences relayed by the sub-group, it is not accurate to say that the couple’s concerns were baseless; there are some parents of children with DS who experience significantly more challenges than others. Like the sub-group, Judy illustrated that she was aware of the dominant narrative, and that although she did not disagree with it per se, she considers it simplistic in relation to the factors that contributed to her decision to terminate:
Because I think there’s a lot of these ‘rah rah!’ you know, ‘Down syndrome people are people too!’ and I
— yeah, they are, but sometimes people have to make difficult choices for a number of reasons.
Discussion
The purpose of the current study was to investigate how parents of children with DS understand and make meaning of their parenting experience and if there are dominant ways that they do so. Most participants relayed that in contrast to what they imagined when they received their child’s determination, raising their child had not been that different from parenting a typical child. They relayed challenges and a slower pace, but an essence that is similar. This dominant narrative that likens parenting a child with DS to “taking the scenic route” aligns with previous research with parents of children with DS who have framed their experience as simply “a change in plans” (Van Riper, 2007), or “not what you were expecting, but… still a beautiful journey” (Pillay et al., 2012). The narrative also aligns with previous research which has suggested that the adjustment of parents of children with DS resembles the adjustment of parents of typically developing children more than it differs (Cunningham, 1996; Glidden et al., 2010). In the present study, these parents tended to experience distress immediately after their child’s determination but subsequently experience a turning point wherein the devastation of the initial determination eased, their initial concerns were revised, and life became easier. Getting used to the idea of DS through time, getting to know their child, and getting to know other parents and children with DS which normalized their experience and provided them with a sense of belonging appear to be integral factors in changing their experience.
The sub-group narrative challenged the dominant narrative, or at least the universality of the “scenic route” experience. In contrast to the dominant group, this minority of participants reported significant challenges in parenting their child with DS, did not experience a turning point where raising their child became easier, and retrospectively underestimated the impact that DS would have on their lives. Unlike the majority who felt understood and empowered by engaging with other parents and DS organizations, the subgroup felt marginalized and silenced. To them, the “scenic route” narrative applied to “high-functioning” children with DS and did not reflect their experience. Although only two participants composed the sub-group narrative, the subgroup narrative might be underrepresented, given the social pressure to align with the dominant narrative.
The presence of the sub-narrative legitimates some of the concerns that motivated Judy’s termination in the third narrative. As she imagined, parenting a child with DS can be very challenging. Other research has also reported that a small proportion of parents of children with DS experience more stress, anxiety, and depression than parents with typically developing children (Noh et al., 1989; Sanders and Morgan, 1997; Padeliadu, 1998; Roach et al., 1999; Gau et al., 2008). There are various explanations for why some parents with DS “thrive” and others “have difficulty adapting” (Van Riper, 2007). Most studies indicate that the child’s level of cognitive ability is not related to parental well-being (Manuel et al., 2003; Glidden and Schoolcraft 2007; Grein and Glidden, 2015). Rather, the child’s behavioural phenotype tends to be one of the strongest predictors, with more behavioural challenges being indicative of lower parental well-being (Sloper et al., 1991; Cunningham, 1996; Stores et al., 1998; Hauser-Cram et al., 2001; Hodapp et al., 2003; Abbeduto et al., 2004; Most et al., 2006; Bourke et al., 2008; Esbensen and Seltzer, 2011; Pillay et al., 2012). The number and severity of health problems is also predictive of lower levels of parental adaptation (Skotko et al., 2011; Pillay et al., 2012), and indeed the two participants in the sub-group had children with additional conditions that are sometimes comorbid with DS. Finally, parents’ emotional stability is also predictive of higher levels of well-being as is family accord (Grein and Glidden, 2015) and an affirming style of problem solving (Van Riper, 2007).
Notably, Esbensen and Seltzer (2011) found that social support was not related to parental well-being, an outcome that even they questioned. In the present study, the dominant group extolled the positive impact of meeting other parents of children with DS. But the subgroup disagreed that interacting with other parents was helpful. Parents in the subgroup described support groups as relying on the dominant narrative, which left them feeling marginalized. Given the present findings, it might be that the effects of social support on well-being are mediated by the feelings of being understood and normalized by one’s peers, which is more likely to occur when their experiences have been highly similar to one’s own.
The results of this study indicate challenges for counselling parents about screening, testing and termination decisions. What should a prospective parent, who might have concerns about parenting a child with DS, be told about DS? Parents have been dissatisfied with the overly negative and medical portrayal of DS when they received their determination (Hedov et al., 2002; Skotko, 2005a, 2005b; Nelson Goff et al., 2013). They have called for more positive information to be provided, a request that is based in evidence given the overwhelmingly positive experience relayed by many parents of children with DS. However, as evidenced by some experiences represented in the current study, some parents experience significant challenges, and believe the dominant narrative paints an exaggeratedly positive picture. Although most parents in this study are “taking the scenic route,” that is not applicable or relatable to all parents of children with DS. This is what presents the challenge of how to frame DS when a determination is delivered or when termination is considered—there is not one story to tell.
The results of this study support the suggestion by Hippman et al. (2012) which was to explore the range of possibilities regarding the experience of raising a child with DS and help families to evaluate these possibilities in the context of their own lives. This includes communicating the range of outcomes for individuals with DS, which could be conveyed with stories or videos, as well as helping families to imagine how a child with DS would interact with their lives. Parents could be encouraged to consider variables such as their own coping style, the strength of their relationship with their partner, and the support available to them (to name a few), and how these variables would interact with the various outcomes of DS. The narratives explicated in this study also provide insight into the range of possibilities that can be presented to parents.
The results of this study also present challenges for support organizations, because they highlight a segment of their population who may be underserved. Many participants emphasized that they were inspired by the work of support organizations, particularly the way that support organizations highlight the achievements and abilities of people with DS. However, there is a segment of parents who appear to need a different kind of support. It may be of value, for example, to create conversation circles for parents of children who experience a higher number of DS-related health complications, so that they have a venue to normalize their experience, share information, and feel a sense of being understood and belonging. It also may be beneficial to create informational resources that can be provided to parents of children with relatively more DS-related complications. Finally, this group may need additional advocacy for educational, financial, and social supports given the higher demands of parenting their children.
Limitations
While the findings shed light on the various experiences and interpretations of parenting a child with DS, there are several limitations of the current work. First, it is unknown how representative the sample of parents is, given that they self-selected to participate. Therefore, it is an inherent weakness of the study that there are experiences that may not be represented in the data. Specifically, the story of those who choose to terminate is largely untold here and should be a focus of future research. Another limitation is that the sample was almost exclusively composed of people who received their determination in one Canadian province. Therefore, the extent to which the results generalize to other locations depends on the extent to which their sociocultural context and health care systems resembles the context and systems in that province. Moreover, Canada is a country where there is relatively robust economic and social support for families and children with disabilities. The experiences of parents in contexts with lower levels of support are likely less positive than those relayed here. The findings and implications are also unlikely to apply straightforwardly to contexts where abortion is illegal, or contexts where access to and legality of abortion is more restricted than it is in Canada.
A final limitation worth mentioning is our inability to objectively evaluate previous decisions. Post-decisional dissonance is an uncomfortable feeling after a decision which is caused by concern that we may have made “the wrong” choice. We tend to reduce this uncomfortable feeling by enhancing the attractiveness of the chosen alternative and devaluing the rejected alternative (Brehm, 1956). That is, when asked afterward, we usually believe we have made the right choice. The implication is that most people will view their children as “worth the trouble” and most people will also evaluate their terminations as “the right choice”. This makes post-decision evaluations about whether continuing or terminating a pregnancy was the best choice, fraught with personal bias. Coupled with the confirmation bias, whereby we search for information that confirms our beliefs and interpret information in a way that is more in line with our existing beliefs (Nickerson, 1998), objective accounts of what parenting a child with DS is like are functionally impossible to obtain. However, as Becker (1997) has stated, narratives “reflect people’s experience, as they see it and as they wish to have others see it” (p. 25, emphasis added). That is, what has been presented in this analysis was not intended to be an objective account of parenting a child with DS, but how these participants have made sense of this change to their life course. Their sense making may indeed include what Nussbaum (2001) and Khader (2011) call adaptive preferences, which are preferences formed due to social circumstances for a condition which might not objectively be best for them. However, as Khader points out, holding these preferences is not necessarily irrational; when circumstances will not change, as they will not with a definitive DS determination, framing the experience of parenting a child with DS as “taking the scenic route” may be a highly rational response, and therefore, these actors can still be considered reliable sources of information on their experience. Moreover, as Kaposy (2018) explained, reframing the experience positively is part of effective coping and not an indication that their assessment of the situation is distorted.
Conclusion
The present research contributes to a growing body of evidence suggesting that despite how care providers tend to frame parenting a child with DS (negatively), most parents experience it positively. However, a monolithic positive portrayal of parenting a child with DS is also not likely helpful, as it may serve to marginalize and silence those parents whose experience does not match the dominant “scenic route” narrative. Therefore, health care providers and support organizations should promote a narrative that encompasses the diversity of parenting a child with DS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article draws on research supported by the Social Sciences and Humanities Research Council.