
Abstract
Smith–Magenis syndrome (SMS) is a genetic syndrome most often caused by a deletion on chromosome 17 or more rarely by a mutation in the retinoic acid-induced 1 gene. The aim of this study was to investigate the Developmental Behavior Checklist (DBC) profile of persons with SMS and the associations between behavioural and emotional problems, age, gender, adaptive behaviour and autism symptomatology. Twenty-eight persons with SMS were represented by their parents in this study. DBC Total scores are reduced with age, but they still show a mean that is clearly above the cut-off of 46. The differences between the age groups <9 years and 9–17 years (p = 0.024) and between the age groups <9 years and >18 years (p = 0.007) are significant. We found a significant decrease in behavioural and emotional problems with age in SMS. We did not find a relationship between adapted behaviour and communication and behavioural and emotional problems.
Introduction
Smith–Magenis syndrome (SMS) is a rare, neurobehavioural disorder most often caused by a deletion of chromosome 17p11.2 (Smith et al., 1986) or, more rarely, haploinsufficiency of the retinoic acid-induced 1 (RAI1) gene (Edelman et al., 2007; Slager et al., 2003). The disorder is a multiple congenital anomalies and intellectual disability syndrome (Falco et al., 2017).
More advanced genetic analysis and a more knowledge regarding syndrome have in recent years lead to more patients being diagnosed with SMS earlier than before (Gropman et al., 2006).
The unique neurobehavioural problems displayed by children and adults with SMS are challenging for both parents and professionals. The syndrome’s severe behavioural problems include self-injurious behaviours, such as self-biting, slapping and skin-picking, as well as prolonged outbursts, tantrums and aggressive behaviour (Dykens and Smith, 1998; Finucane et al., 2001). The challenging behaviours are believed to increase with age and intellectual level (Neira-Fresneda and Potocki, 2015). Sleep disturbances, present in 88% of the SMS patients, have been associated with an unusual inverted circadian melatonin rhythm (De Leersnyder et al., 2001; Gropman et al., 2006, 2007; Smith et al., 1998). The sleep disturbances include difficulty getting to sleep, frequent nocturnal awakenings, early sleep offset, and daytime sleepiness with a need for daytime naps (Neira-Fresneda and Potocki, 2015). Early expressive speech delays with and without hearing loss are observed, as are mild-to-severe cognitive deficits (Madduri et al., 2006; Martin et al., 2006; Udwin et al., 2001). Autism spectrum disorders have also been identified in almost 90% of the investigated populations with SMS (Laje et al., 2010; Martin et al., 2006). A recent study found a reversed gender difference in autism symptomatology (Nag et al., 2018). This study only found a gender difference in the Social Relation subscale on the Developmental Behaviour Checklist (DBC) (Nag et al., 2018).
Behavioural and emotional problems (BEPs), communication problems, autism spectrum disorder and sleep problems are aspects of SMS that have significant impacts on the lives of families. Hodapp et al. (1998) found that parents of children with SMS reported greater pessimism and more parent and family problems compared to families coping with Down syndrome (DS). Other studies of caregivers for children with SMS show increased distress in the form of depression, anxiety, and sleep problems (Foster et al., 2010). Additional findings indicate that levels of stress among caregivers are related to the level of behaviour challenges displayed by the child with SMS (Fidler et al., 2000; Hodapp et al., 1998).
The prognosis of the SMS patient is closely linked to their BEP (Poisson et al., 2015), and there is a need for more research that explores relations between BEP and other characteristics.
The aim of this study was to investigate the DBC profile of persons with SMS and the associations between BEP, age and other characteristics, such as gender, communication, autism spectrum disorder (ASD) and adapted behaviour.
Method
Participants
This study was part of a larger assessment study of SMS in Norway, Sweden and Denmark. The study was approved by Ethics Committees in all three countries. Written consent was provided, either by the parents, for persons under 16 years old, or by both the parents and the person with SMS, for persons above 16 years old.
The participants consisted of parents of persons with SMS. Twenty-eight persons with SMS met the inclusion criterion of a genetically confirmed diagnose. Their age was between 5 and 50 years. Eleven of the persons with SMS were adults (above 18 years old). The level intellectual disability was retrieved from medical or pedagogical charts. In two of the participants, the level of intellectual disability was missing. The demographics are displayed in Table 1.
Demographics.
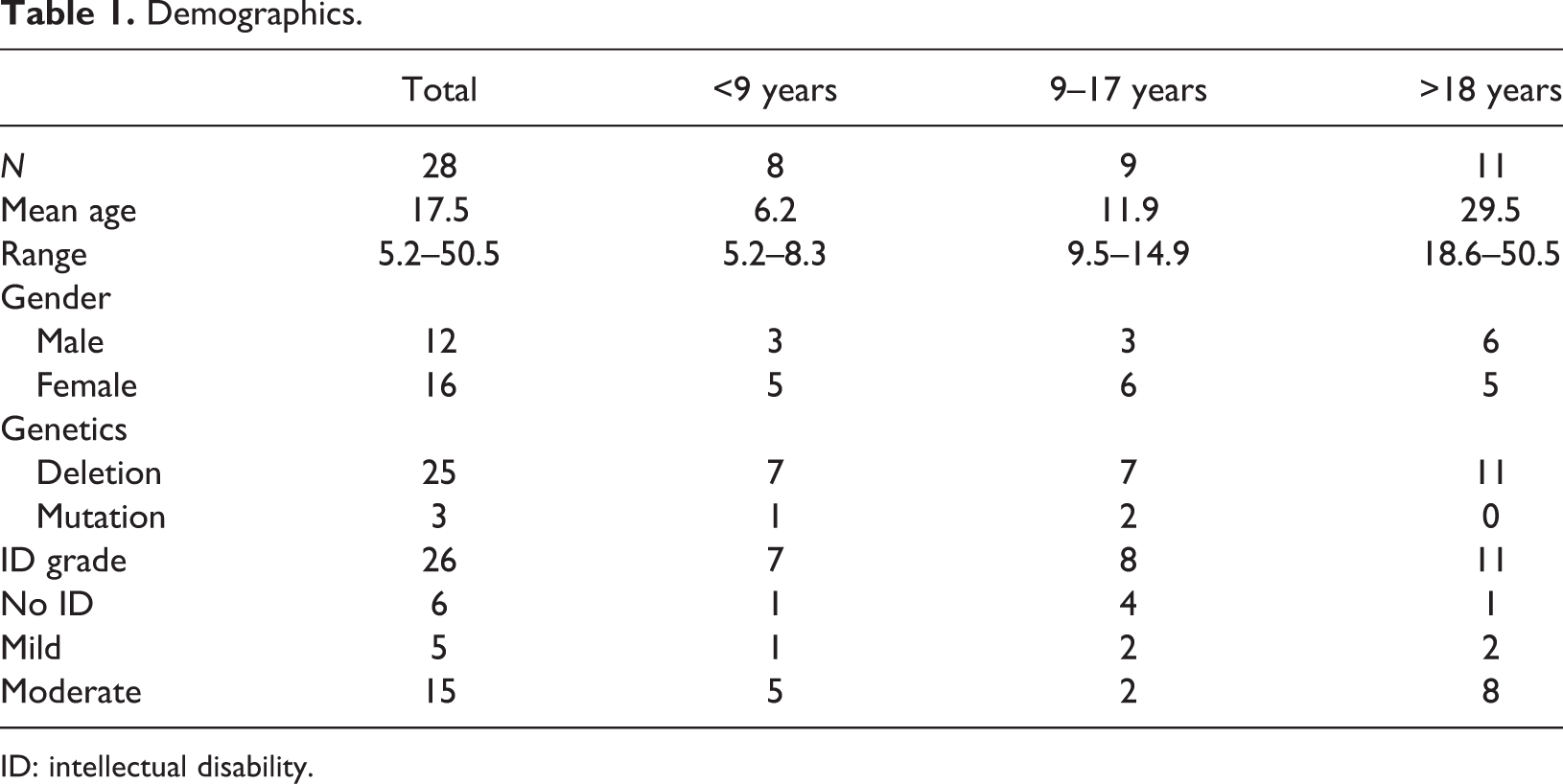
ID: intellectual disability.
Measures
The DBC (Einfeld and Tonge, 1992, 2002) is a questionnaire which is completed by parents or other primary carers or teachers; this questionnaire is used to report problems over a 6-month period. It is an instrument for assessment of a broad range of behavioural and emotional problems of persons with developmental and intellectual disabilities (Dekker et al., 2002; Einfeld and Tonge, 1995). The DBC have a confirmed reliability and validity (Dekker et al., 2002; Einfeld and Tonge, 1995), and has been proven useful to use in research of prevalence of psychopathology in the population of persons with intellectual disabilities (Einfeld and Tonge, 1995).
The Vineland Adapted Behavior Scale II (VABS II) (Sparrow et al., 1984, 2005) is a semi-structured interview. It can be completed by parents or caregivers that is used to assess the everyday skills (adaptive behaviour) of children and adults from birth throughout life. The VABS II is a standardized and validated tool. Many studies have confirmed its reliability and validity. It is widely used, and one of few tools for assessing adaptive behaviours translated to Norwegians with Scandinavian norms (de Bildt et al., 2005; Sparrow et al., 2005). Other studies have found a strong evidence for applicability of VABS in the population with intellectual disabilities (de Bildt et al., 2005).
The Social Communication Questionnaire (SCQ) is a standardized screening tool for the evaluation of communication forms and social function in children or adults in order to exclude autism or an ASD (Rutter et al., 2003). A review of different assessment of rating scales for ASD found the SCQ performing well on psychometric properties and it is useful as a screening instrument (Norris and Lecavalier, 2010).
The Social Responsiveness Scale (SRS) is a 65-item, quantitative parent-reported measure that assesses social impairment associated with autism spectrum disorders (Constantino and Gruber, 2005). Studies have found this instrument valid and reliable for measuring autistic traits (Bölte et al., 2008; Constantino et al., 2003). It has also been deemed usable for research studies of autism spectrum conditions (Constantino et al., 2003).
Data analysis
Statistical Package for the Social Sciences version 23 (IBM) was used for statistical analysis.
Pearson’s r was calculated using bivariate correlation analysis. Significance levels of both 0.05 and 0.01 were used. To make sure basic assumptions for parametric tests were met, the data were checked for normality by visually inspect histogram, Q–Q plot and Shapiro-Wilk’s W test. The data proved normally distributed and therefore parametric tests were used. The participants were divided into three age groups (<9 years, 9–17 years and >18 years) to investigate whether the BEP measured with the DBC changes with age. Social Science Statistics’ online resources were used for calculating effect sizes (Cohen’s D). The T-test was performed to investigate group differences.
Linear regression analyses were conducted with DBC Total as the dependent variable and with ID grade, gender, age, VABS (including the communication subscale), SRS and SCQ as covariates. Due to low sample size, we only included a maximum of four covariates for each model. P–P plots were used to check the normality of residuals. We report the standardized coefficients (β) because we have both dichotomous and continuous predictor variables. Due to modest sample size, we do not correct p-levels for multiple tests, but rather effect sizes for improved interpretation of the comparisons conducted.
Results
Table 2 displays the participants’ scores on VABS II, SCQ and SRS. This information will be used as background to investigate the DBC profiles as well as associations between the characteristics and BEP.
Characteristics of the participants.
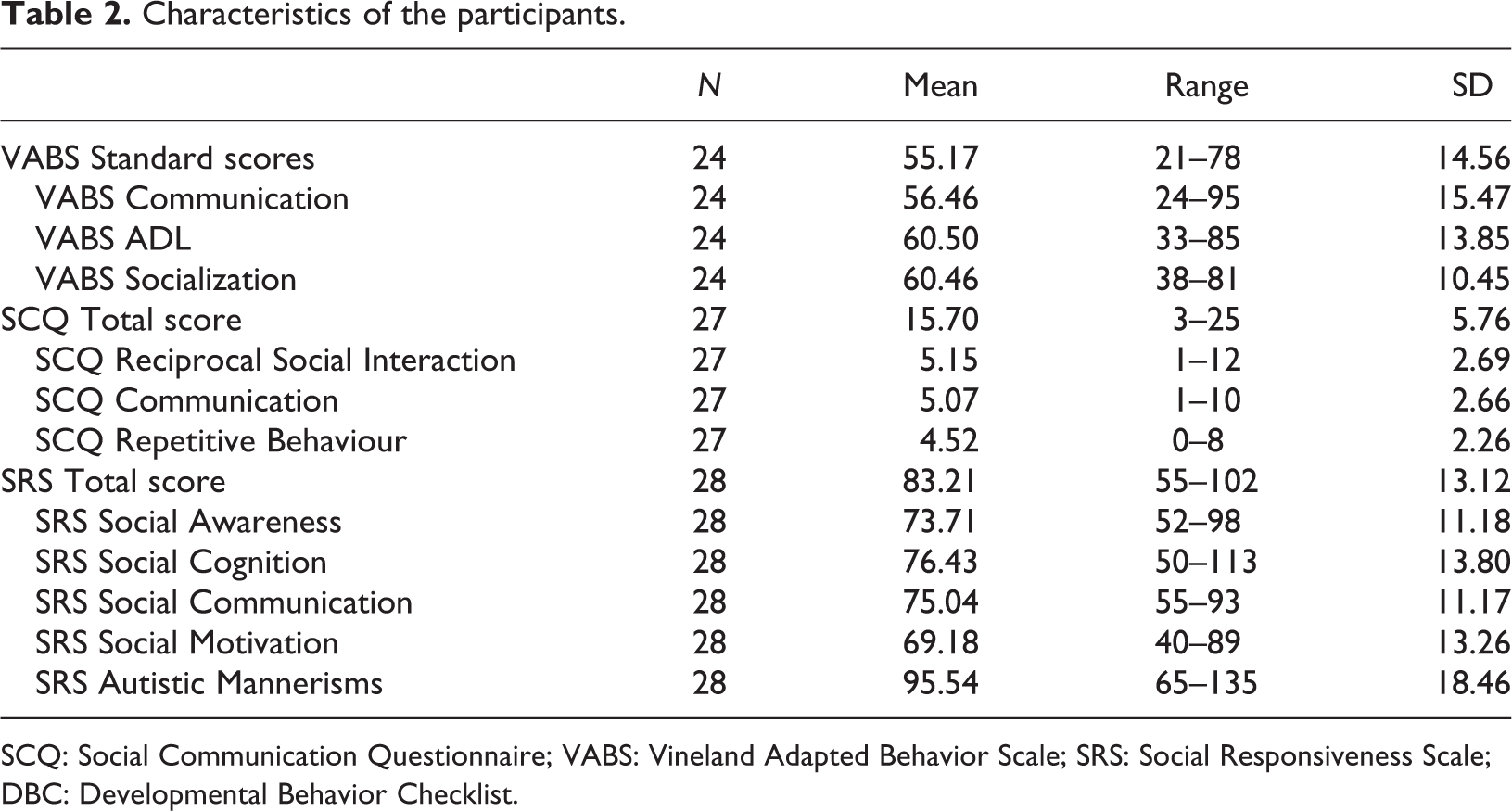
SCQ: Social Communication Questionnaire; VABS: Vineland Adapted Behavior Scale; SRS: Social Responsiveness Scale; DBC: Developmental Behavior Checklist.
Developmental Behavior Checklist
The DBC data from 28 participants were analysed. The results of the DBC Total and subscales are presented in Table 3. A total of 93% of scores were above the cut-off on the DBC Total.
DBC scores (percentiles).
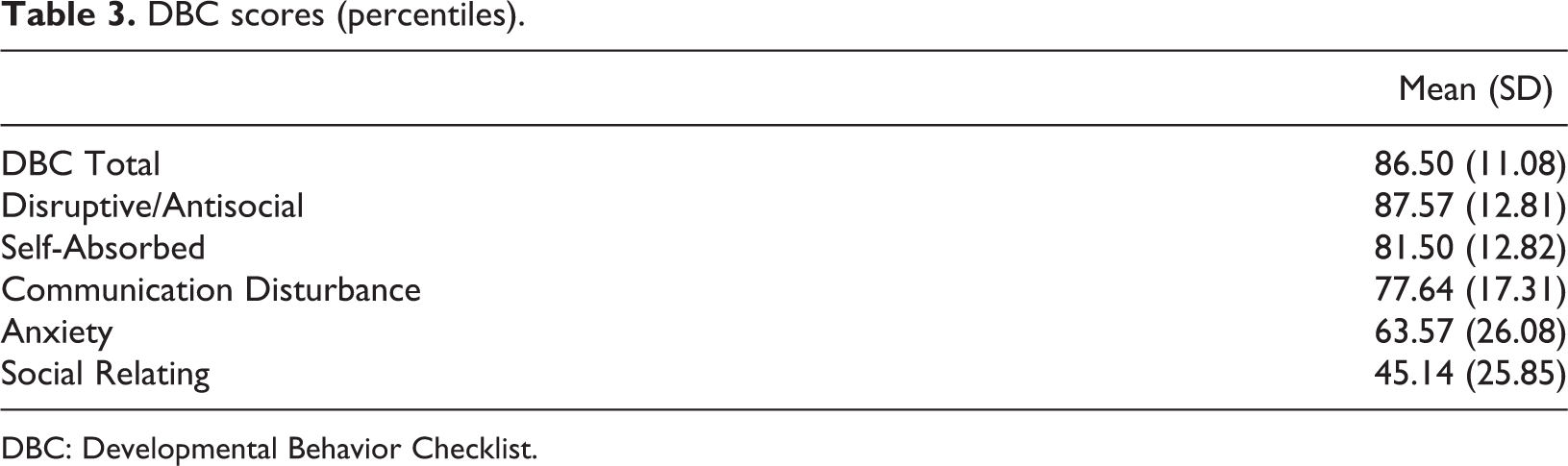
DBC: Developmental Behavior Checklist.
DBC : Relation to age
DBC Total scores are reduced with age, but they still have a mean that is clearly above the cut-off of 46. The DBC Total percentiles had a significant negative correlation with age in the whole group (r = −0.430, p = 0.022). The results of the age groups are shown in Figure 1. The difference between the age group <9 years and that of 9–17 years is significant (p = 0.024), as is that between the age groups of <9 years and >18 years (p = 0.007). There is no significant difference between the age groups of 9–17 years and >18 years.
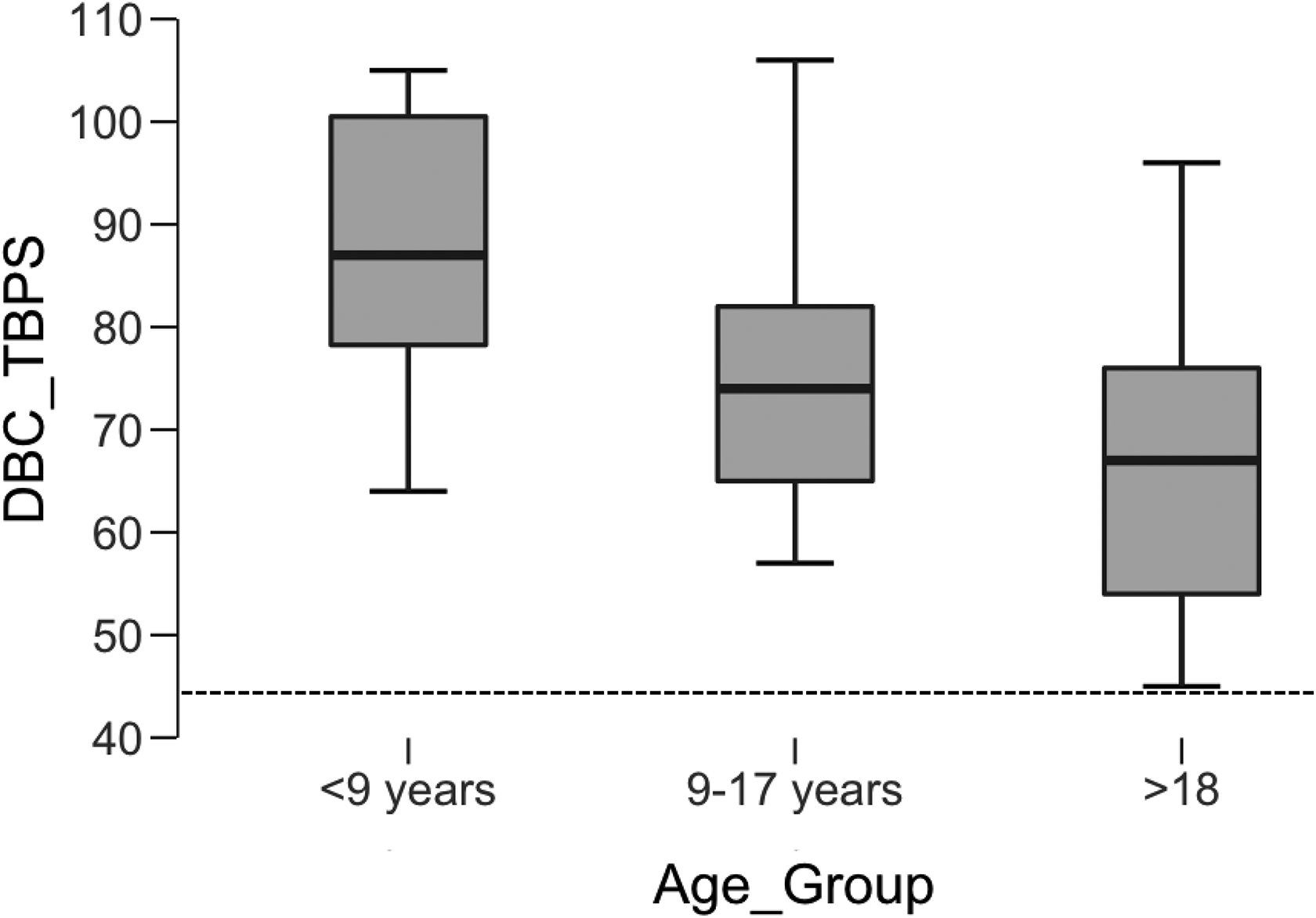
DBC Total score distributed across the age groups. The box indicates the 25th to 75th percentiles, the line in the box indicates the mean and the whiskers the minimum and maximum. The dotted line indicates the cut-off on the DBC.
The mean percentile profile in the different age groups is presented in Table 4. In general, both DBC Total and all subscales, except social relating, are decreasing with age. In both DBC Total and subscale 1–4, the mean percentile in all age groups is relatively high (above 70th percentile). The only exception is in the Anxiety subscale where both age group 2 and 3 have a mean percentile in the 50th percentile. Social relating seems to be a relative strength in SMS with mean percentiles below the 50th percentile.
Mean DBC percentiles across age groups.
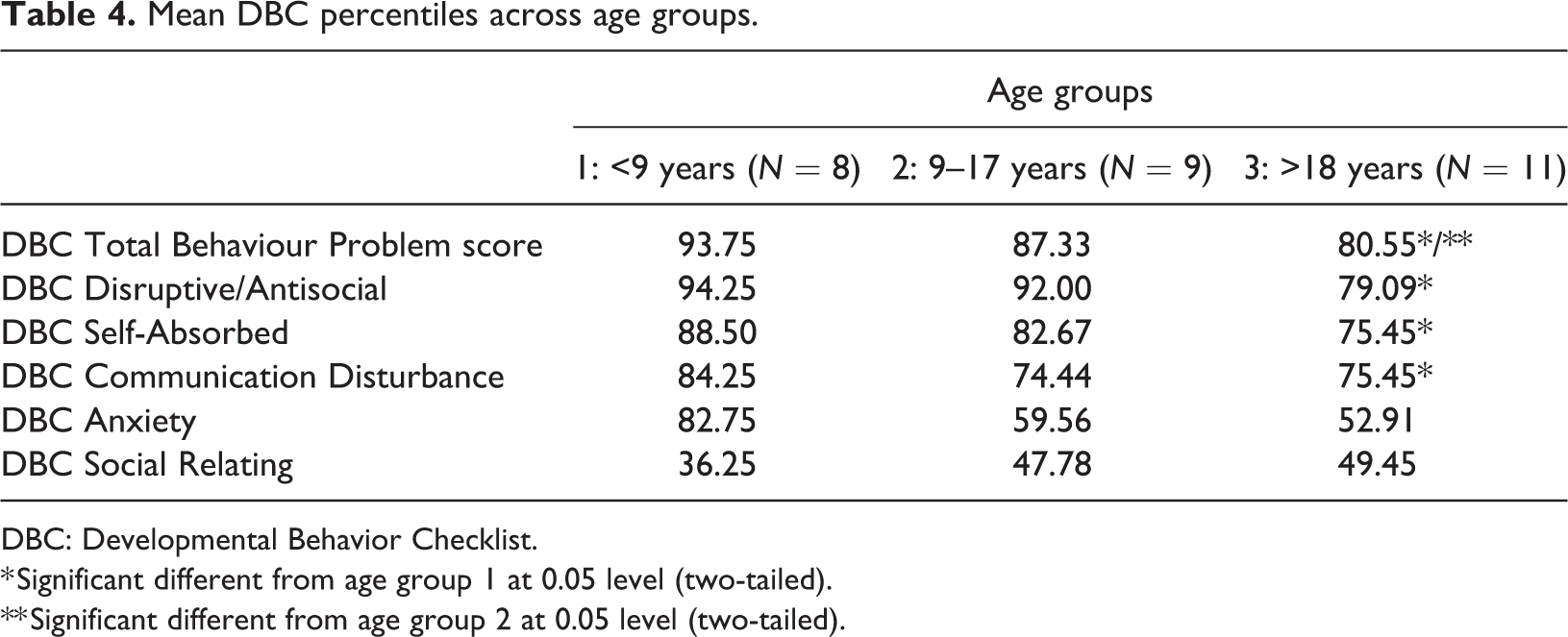
DBC: Developmental Behavior Checklist.
* Significant different from age group 1 at 0.05 level (two-tailed).
** Significant different from age group 2 at 0.05 level (two-tailed).
The mean, SD and significant group differences in each subscale are presented in Table 5. There are significant differences between the youngest and oldest age group in all but the Communication Disturbance and Social Relating subscales. Between the youngest and middle group, there are no significant differences when looking at the p-values, but there is a large effect in the Anxiety subscale using Cohen’s D. Between the middle group and the oldest group, the only significant difference is in the Disruptive/Antisocial subscale. None of the other measures, such as VABS or SCQ, had a similar decrease in scores with age SCQ had an increase in scores with age, but the difference was not significant (p = 0.071, D = 0.29).
DBC across age groups.
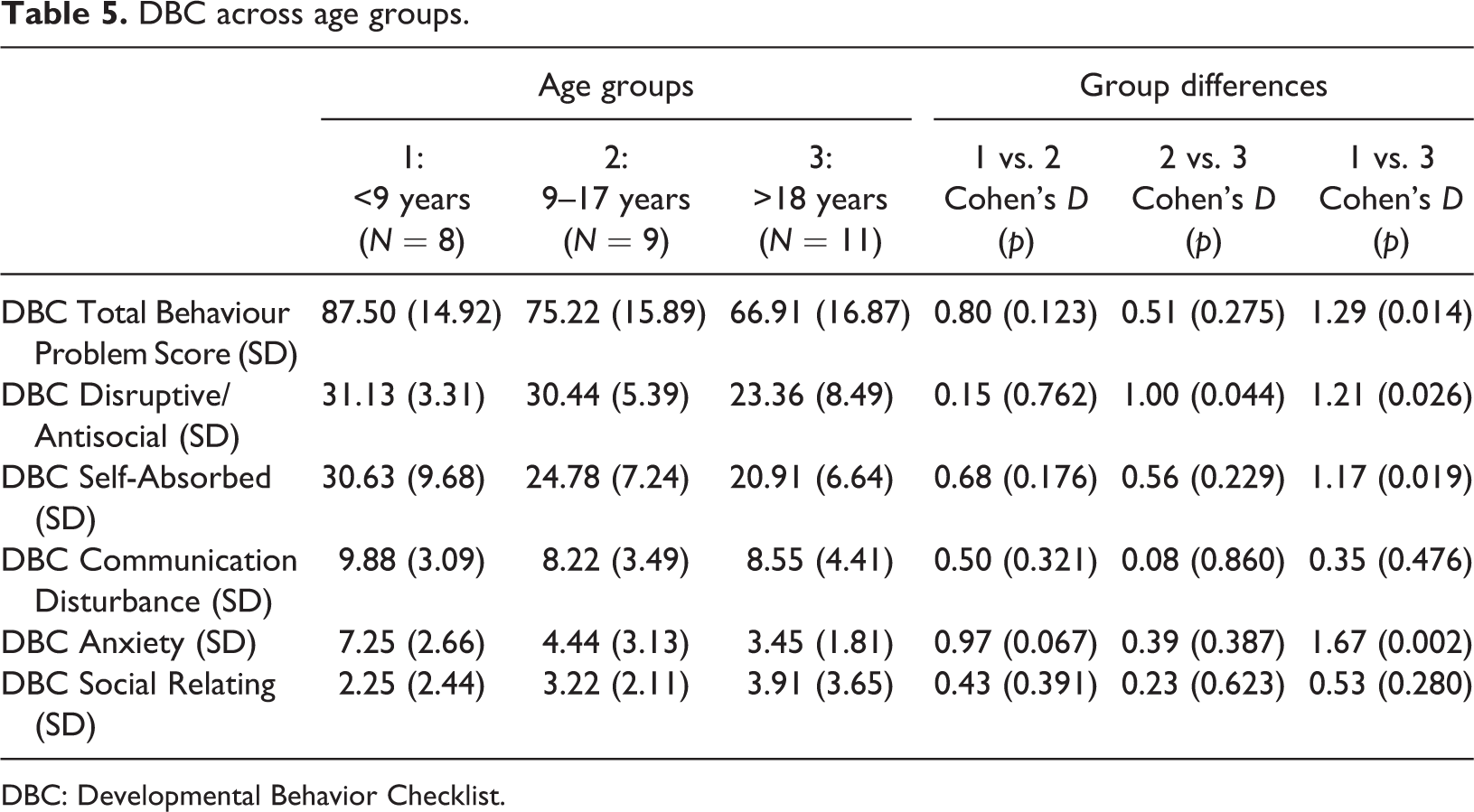
DBC: Developmental Behavior Checklist.
In all subscales, except social relating, there is a decrease with age. In social relating, there is an increase from age group 2 to 3. This decrease is not significant.
Relation to adaptive level
The results are presented in Table 6.
Correlations with DBC.
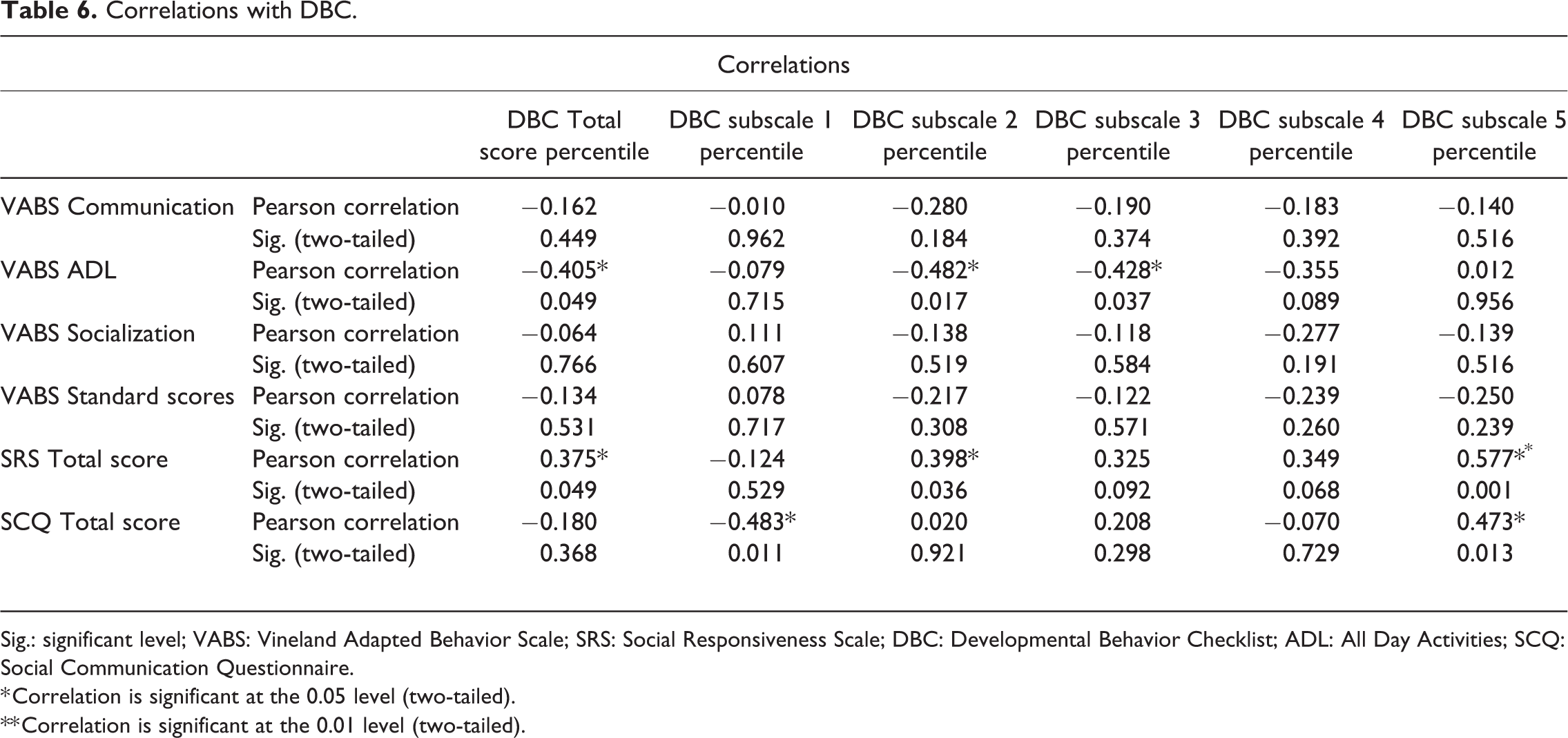
Sig.: significant level; VABS: Vineland Adapted Behavior Scale; SRS: Social Responsiveness Scale; DBC: Developmental Behavior Checklist; ADL: All Day Activities; SCQ: Social Communication Questionnaire.
* Correlation is significant at the 0.05 level (two-tailed).
** Correlation is significant at the 0.01 level (two-tailed).
Both the DBC Total and the DBC subscales for disruptive/antisocial and communication disturbance were related to the VABS ADL subscale with a negative correlation.
SCQ Total had a negative correlation with the disruptive/antisocial subscale and a positive correlation with the Social Relation subscale. SRS Total had a positive correlation with DBC Total score percentile and the subscales self-absorbed and social relating.
Several linear regressions were conducted with DBC Total as the dependent variable and with ID grade, gender, age, VABS (including the communication subscale), SRS and SCQ as covariates. When both gender and age were entered as covariates with VABS and SRS, we obtained a significant model (R2 = 0.64, F = 8.6, p = 0.00039). SRS (β = 0.829, p = 0.00027), age (β = −0.479, p = 0.003) and gender (β = −0.671, p = 0.003) each had an independent contribution to the model. VABS (β = −0.244, p = 0.143) had no independent contribution. Removing gender from the model still yielded a significant model (R2 = 0.42, F = 4.88, p = 0.010). Both SRS (β = −0.42, p = 0.029) and age (β = −0.43, p = 0.021) made independent contributions, but they dropped to the 0.05 level. Including only VABS and SRS did not give a significant model (R2 = 0.24, F = 3.35, p = 0.055). All three models are presented in Table 7.
Regression model summary.
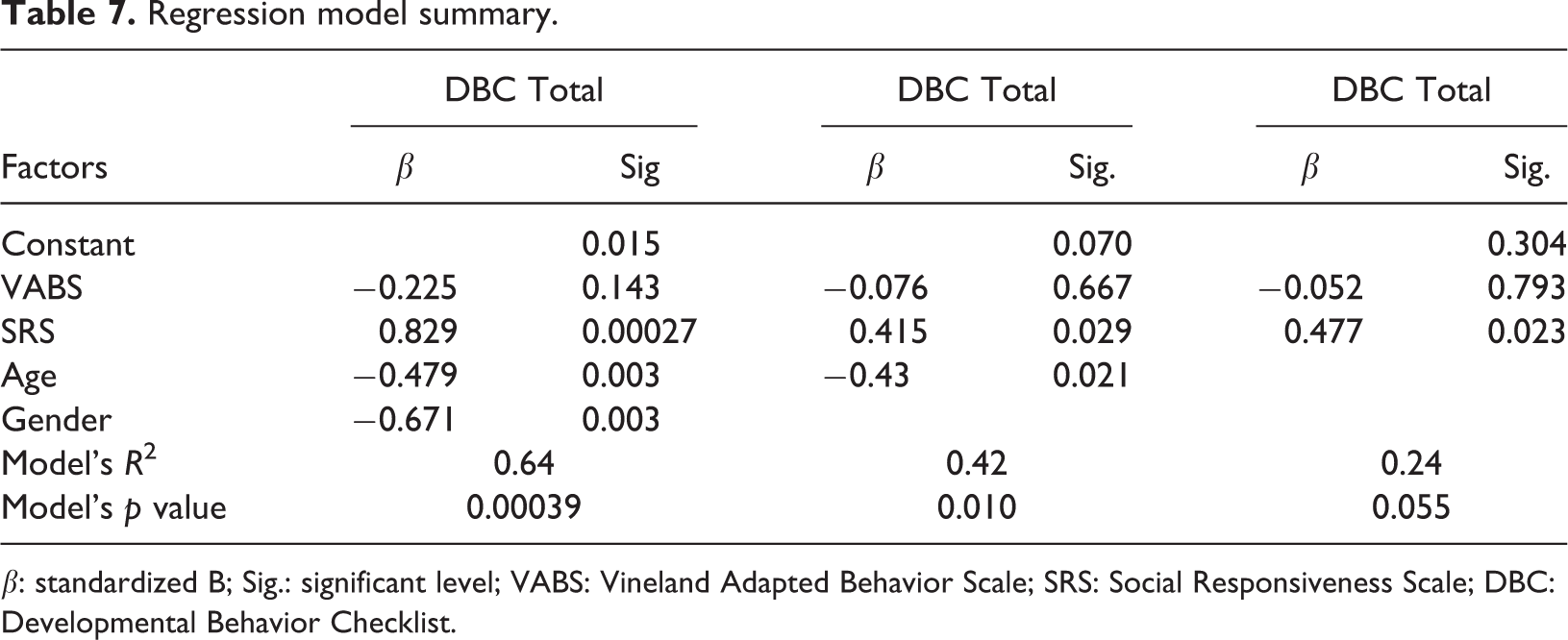
β: standardized B; Sig.: significant level; VABS: Vineland Adapted Behavior Scale; SRS: Social Responsiveness Scale; DBC: Developmental Behavior Checklist.
Discussion
The aim of this study was to investigate the relations between behavioural and emotional problems and other characteristics in SMS, such as communication, adaptive behaviour and autism symptomatology.
We found significant age group differences in the DBC Total, decreasing with age. This finding is the opposite of earlier research that reports an increase in behavioural problems in SMS with age (Finucane et al., 2001; Neira-Fresneda and Potocki, 2015; Poisson et al., 2015). This study included more adults with SMS than did earlier studies, but we still found a decrease in behavioural and emotional problems from age group 1 (<9 years) to age group 2 (9–17 years), even though the decrease was not significant in all subscales. Another study with 267 persons with either Williams syndrome (WS), DS, Fragile X syndrome or Prader–Willis syndrome (PWS) measured behavioural and emotional problems using the DBC two times, 4 years apart (Einfeld et al., 1999). Neither of the syndrome groups in this study had a significant change from time 1 to time 2. Einfeld et al. (1999) found that persons with WS had the highest mean around 55 at time 1, this decreased to less than 50 at time 2. Persons with PWS had an increase from time 1 to time 2 from a mean around 52 to a mean around 57. The mean DBC Total in our sample was higher.
The decrease of behavioural and emotional problems with age is positive information for families that struggle with the behavioural and emotional problems of SMS. It is also important to underline that the levels of behavioural and emotional problems in adults with SMS are still high and far above the cut-off on the DBC Total.
In this study, as many as 93% scored above the cut-off on the DBC Total. The high percentage of persons scored above the cut-off on the DBC Total was not surprising. Earlier research has shown that SMS often scores higher on self-injuries behaviour and aggressive behaviour than other comparable disorders (Arron et al., 2011). In the study by Arron et al. (2011), 92.9% of the population with SMS displayed self-injuries behaviours and 73.8 displayed physical aggression. In earlier research concerning Cornelia de Lange syndrome and Down syndrome, 38 and 31.3% scored above the cut-off (Basile et al., 2007; Bourke et al., 2008), in all age groups, than any of the syndromes investigated by Einfeld et al. (1999). SMS is often compared to PWS, since both syndromes struggle with obesity, but also regarding challenging behaviours (Alaimo et al., 2015; Bouras et al., 1998). In a study utilizing DBC to investigate the behavioural phenotype of PWS, Holland et al. (2003) reported both DBC Total scores and scores on all subscales lower than what we found in any of the three age groups in our study.
Investigating relations between the behavioural and emotional problems and other characteristics in SMS is an important step towards finding treatments that regulate the challenging behaviours that characterize SMS. In this study, we investigated a range of characteristics as they related to SMS, but few of them had a significant relation to the behavioural and emotional problems measured by the DBC.
Both communication and level of intellectual disability have been associated with behavioural problems (McClintock et al., 2003). A large meta-analysis has found a significant association between low language abilities and problem behaviour (Chow and Wehby, 2018). In this study, we did not measure intellectual level and only reported previously measured level of intellectual disability; we did measure adapted behaviour. Neither adaptive behaviour nor communication had a relation with the DBC in this study. A more specific communication and language assessment is needed to investigate whether there is an association between communication issues and challenging behaviour in SMS.
The strongest correlation we found in this study was between SRS and subscale 5 (social relation), which is not surprising. The most interesting correlation, and the one most worthy of further investigation, might be the correlation between the DBC total, several subscales and the VABS ADL subscale.
All participants in our study have known challenging disorders, even though not all of them have a clinical diagnosis of emotional and behavioural disorders in addition to SMS. They have all been in contact with resource centres for rare disorders in Sweden and Norway and their challenging behaviour is followed by either their regional or local professionals. Knowledge regarding how to handle challenging behaviours in SMS are scarce (Poisson et al., 2015) and more research is needed, in addition a continuous effort to spread information to the local communities and professionals close to the families.
In this study, we did not perform a thorough investigation of either intellectual level or communication, and that information is needed to further investigate whether there is a relation between behavioural problems and intellectual disability and communication.
Conclusions
We found a significant decrease in behavioural and emotional problems with age in SMS. We did not find a relationship between, on the one hand, adapted behaviour and communication and, on the other hand, behavioural and emotional problems.
Footnotes
Authors’ note
This study is part of the BUPgen study group and the NeuroDevelop research network.
Acknowledgement
We are thankful to the participants in the study and to the Norwegian, Swedish and Danish SMS Foundations.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
All the participants consented to publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Frambu Resource Centre for Rare Disorders and NevSom, Department of Rare Disorders and Disabilities, Oslo University Hospital.
Ethics approval and consent to participate
This study was approved by the regional ethics committees in Norway, Sweden and Denmark.