
Abstract
The experience of having a rare disorder was summarised in a large study as ‘falling outside the vast field of knowledge of the professionals’. Parents (31 mothers and 17 fathers) of 32 persons with Smith–Magenis syndrome (SMS) participated in this study. A phenomenological approach was used to analyse the data into topics and themes. Four themes emerged: behavioural challenges displayed, parents’ strategies for meeting the challenging behaviours, parents’ experiences of their own competence and parents’ experiences of professionals’ competence and understanding regarding children with SMS and their behaviour challenges. We found that parents of children with SMS experience that they are exposed to severe challenging behaviours from their child. The parents believe that they experience more misunderstandings with professionals and that the challenging behaviours increase because there are some specific characteristics of SMS that professionals are not aware of or do not consider in their support services.
Background
The experience of having a rare disorder was summarized in a large study by Grut et al. (2008b) as ‘falling outside the vast field of knowledge of the professionals’. Because professionals rarely possess knowledge of rare disorders, they do not know how to treat and follow-up the person with the diagnosis and their family (Grut et al., 2008a). Trulsson and Klingberg (2003) found in their qualitative study that professionals’ knowledge about the specific rare disorders is very important for these families. A study in Sweden concluded that parents of children with rare disorders experienced more stress, especially related to their own lack of competence, social isolation and emotional demands, and that they were less satisfied with the services provided by habilitation centres compared to parents of children with more common disabilities (Dellve et al., 2006). Dellve et al. (2006) also found that parents of children with behaviour challenges reported a higher level of stress than parents of children without behaviour challenges.
Smith–Magenis syndrome (SMS) is a rare, complex genetic syndrome caused by an interstitial deletion of chromosome 17p11.2, (Smith et al., 1986) or a mutation on the retinoic acid induced 1 (RAI1) gene (Slager et al., 2003). The disorder is characterized by intellectual disability, multiple congenital anomalies, obesity, neurobehavioural abnormalities and a disrupted circadian sleep–wake pattern (Chen et al., 2015; Poisson et al., 2015). The incidence of SMS is estimated to be 1:15,000–1:25,000 births (Dubourg et al., 2014; Greenberg et al., 1991; Huang et al., 2016). Delayed diagnosis is common, although more widespread recognition of the syndrome and introduction of new genetic technology in the last decade have led to earlier diagnosis (Gropman et al., 2006).
The majority of children and adults with SMS have behavioural problems, including self-injury, tantrums and stereotypies (Gropman et al., 2007; Poisson et al., 2015). Sleep disturbances, such as nocturnal awakenings and daytime sleepiness, are present in 88% of SMS patients and are partly attributed to an inversion of the circadian rhythm of melatonin distribution (De Leersnyder et al., 2001; Poisson et al., 2015). Cognitive impairment ranges from mild to severe, and expressive language delay with or without hearing loss is observed (Madduri et al., 2006; Martin et al., 2006; Osório et al., 2012; Udwin et al., 2001). Autism spectrum disorders (ASDs) have also been identified in almost 90% of the investigated populations with SMS (Laje et al., 2010; Nag et al., 2018; Osório et al., 2015). These unique neurobehavioural problems are challenging for both parents and professionals.
Variable levels of cognitive impairment have been documented through a variety of psychometric tests that assess adaptive behaviour, intelligence quotient and speech and language development (Madduri et al., 2006; Osório et al., 2012). Both behaviour problems and the need for assistance in many situations last into adulthood (Udwin et al., 2001).
Challenging behaviours, communication problems, ASDs and sleep problems are aspects of this disorder that have a great impact on these families’ lives. Hodapp et al. (1998) found that parents of children with SMS reported greater pessimism and parent and family problems compared to families coping with Down syndrome. Other studies about caregivers for children with SMS showed an increased amount of distress in terms of depression, anxiety and sleep problems (Foster et al., 2010). There are also findings that support that the level of stress in caregivers is related to the level of behaviour challenges the child with SMS displays (Fidler et al., 2000; Hodapp et al., 1998). These three studies are all primarily quantitative and use standardized questionnaires. To our knowledge, no other qualitative research regarding parents of children with SMS’ own experiences of handling the behavioural problems has been published. The topic is complex. The possibility to ask open-ended questions may provide answers and insight not found using standardized questionnaires.
The main aim of this study was divided into three areas: (a) explore the parents’ experience of the behavioural problems of SMS, (b) how the parents viewed their own competency and their experiences in handling the behaviour problems their children with SMS display and (c) the type of support the parents obtained for the behavioural problems. We also looked for differences in reports from parents of females with SMS and males with SMS and differences by age.
Methods
Design
This is a qualitative study utilizing a phenomenological approach to investigate the parents’ lived experiences (Creswell, 2013). The researchers decided to use written responses to open-ended questions and in-depth interviews to supplement the written responses. In phenomenological research, significant statements are highlighted, and these statements are divided into themes organized by the description of the parents’ experience of the phenomenon (Creswell, 2013). After descriptions and themes have been obtained, the researcher may revisit the participants again to clarify or validate the data (Creswell, 2013). An important step in phenomenological studies is to set aside your own personal experience by writing it down and bracketing it (Creswell, 2013). Bracketing means that the researcher identifies personal experiences (beliefs, feelings and perceptions) with the phenomenon and sets it aside to be able to focus on the experiences of the participants (Creswell, 2013). Edmund Husserl, the founder of phenomenology, called this epoché and developed it as a method to be better able to describe the phenomenon exactly as experienced (Husserl, 1954 [1939]). In this study, the researchers’ own experiences and preconceptions were written down at the beginning of the project. This was then revisited during the analysis process to ensure that the preconceptions had not influenced the results in a substantial way.
Recruitment and participants
This study was part of a larger study of SMS in Norway, Sweden and Denmark. The participants were recruited through Frambu Resource Centre for Rare Disorders (Frambu) and the Smith–Magenis Foundations in Norway, Sweden and Denmark (family support groups). The organizations disseminated information about the study on their Facebook pages and email lists. Frambu, which is one of nine state-financed centres of expertise administered by the Norwegian National Advisory Unit on Rare Disorders, has its own register, which is based on informed consent. Frambu could therefore send invitations to registered families with a child or an adult with a diagnosis of SMS. Swedish and Danish families were recruited through family support groups, both through information on their Facebook pages and through information given at their annual gatherings. The only inclusion criterion was that they had a son or a daughter with a genetically confirmed diagnosis of SMS, with no age limit. The parents consented to participate in the study. The parents who participated in the oral interviews were recruited through the Norwegian foundation’s Facebook page, where they responded to a request to participate in an interview.
The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (REC # 2015/1026).
A purposive sample of parents of 32 persons with SMS between 1½ years and 50 years participated in this study. Sixteen of the questionnaires were answered in writing by both parents, 15 of the 32 questionnaires only the mother answered, and 1 only the father answered. All the parents answered in writing. All persons with SMS had a genetically confirmed diagnosis of SMS. Four of the persons had RAI1 mutation, the other 28 individuals had a deletion. Of the 32 persons with SMS, 14 were males and 18 females. Thirteen of them were above the age of 18 at the time of the study. Seventeen came from Norway, 11 came from Sweden, and 4 came from Denmark. A convenience sample of four mothers participated in oral interviews were all from Norway, and their children ranged in age from 10 years to 22 years.
Methodological approach
Open-ended questions were provided to the participants to answer in writing through a questionnaire. The questions were stated in their native language (Norwegian, Swedish or Danish), and the participants provided written answers in their native language. All of the authors understand and can read all the three Scandinavian languages in addition to English. The questions were formulated on the basis of a literature review and Frambu’s experience with the population. These are the questionnaire questions (translated into English by the authors): Does your child have behaviour challenges? If yes, please describe: What do you think is the cause of the challenging behaviours? How do you or did you feel about your own competence handling your child’s challenging behaviours? What type of support and/or guidance did you receive for handling your child’s challenging behaviours? What type of support and/or guidance would you have preferred for handling your child’s challenging behaviours? What types of interventions have been tried for your child’s challenging behaviours, and how did they work out?
After an analysis of the written answers from the parents, one particular theme emerged that required more investigation. Therefore, additional oral interviews were completed with four parents. These parents were already part of the study and had provided written answers to the questionnaire. The interviews were audiotaped. These are the questions asked in the oral interviews (translated to English by the authors): Professionals’ lack of knowledge about the disorder was one of the themes that emerged from data collection. Do you have experience with professionals’ lack of knowledge of the disorder, and if so, did the professionals’ lack of knowledge about the disorder impact the guidance and follow-up you received? Do you believe lack of knowledge of SMS in the support system and among professionals have led to challenges for you or your child?
Data analysis
The written data were transferred from handwriting to a computer by one of the researchers and then analysed word for word. The audiotaped interviews were transcribed by the same researcher and analysed word-by-word. All the data were analysed using the phenomenological method described by Creswell (2013). The following stages were used in the data analysis: becoming familiar with the data by reading it repeatedly, developing a list of significant statements and regrouping the significant statements into themes (Creswell, 2013). After the regrouping of statements into themes, four parents were revisited in an interview to clarify, validate and broaden the findings. At the end, both the written data and the interviews were analysed as a whole. The statements were also visually analysed based on demographic data to look for differences by gender or age. The citations were translated to English by the authors.
Results
Two major topics with four themes emerged from analysing the data. Topics with themes and categories are presented in Table 1. Both the written responses and the oral interviews were analysed as a whole. When theme 4 emerged (parents’ experiences of professionals’ competence and understanding regarding children with SMS and their behaviour challenges), a need for clarification and broadening became necessary. Therefore, four oral interviews were included in the study to supplement the written responses.
Topics, themes and categories.
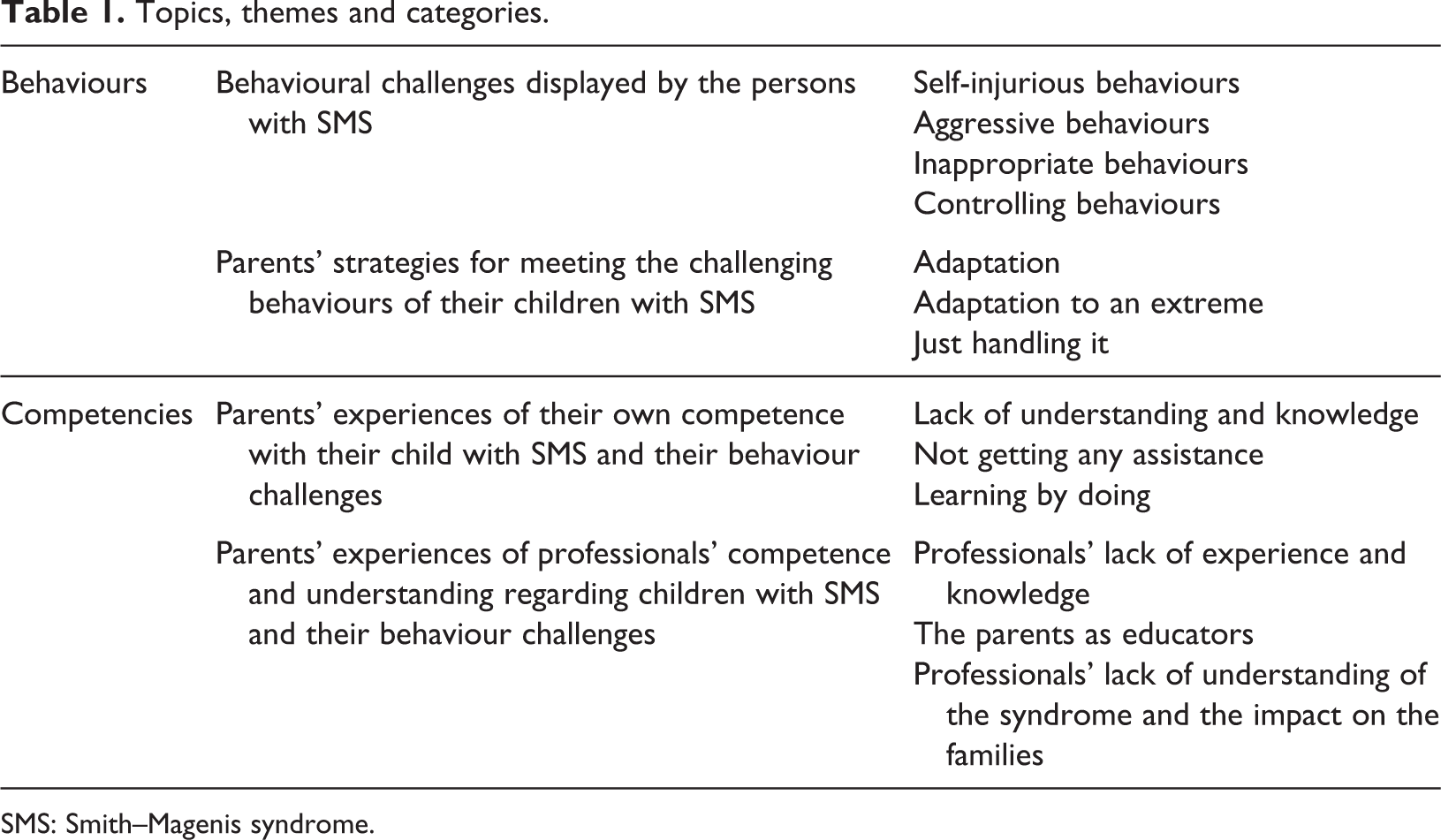
SMS: Smith–Magenis syndrome.
Theme 1: Behavioural challenges displayed by the persons with SMS
Parents described self-injurious behaviours, such as tearing off nails, pinching themselves, hitting themselves and biting their hands. Behaviours such as banging their head into the walls or the bed were also reported. With regard to aggressive behaviours, we found descriptions of screaming, throwing items, destroying items, rage, hitting people around them, kicking and other types of physical attacks on siblings and other family members. As for inappropriate behaviours, we found behaviours such as bad or offensive language, refusing to do as told, undressing, self-stimulation and rapid mood swings. …bothering siblings and doing things she knows is not ok. We also categorize it as challenging behaviour when she talks to strangers and repeatedly asks questions. He needs to be the one who decides. To be in control. …it has been hard because they do not understand why he behaves like this towards us because he doesn’t do that towards them?
There are also more challenging behaviours reported by parents of children under the age of 18 than by parents of adults.
Theme 2: Parents’ strategies for meeting the challenging behaviours of their children with SMS
Parents described common adaptations such as being proactive, providing predictability and aiming at prevention. We adapt everything around him to avoid anxiety, uncertainty, irritations, disappointment, etc. That makes things better. I have learned not to react to everything; today, we live a weird life where I move and act in a certain way not to set of my child When we try to ‘ignore’ the aggressive outburst and just shield others or objects around, the outburst subsides faster. …we have tried everything, begged her to stop, cried in despair, hold her, not hold her…
Theme 3: Parents’ experiences of their own competence with their child with SMS and their behaviour challenges
The parents described their own lack of understanding and knowledge about the syndrome and their handling of the challenging behaviours. They described that anger, frustration and sorrow were caused by the lack of knowledge and that they did not have the strategies or the tools to deal with these behaviours. Some parents said that many of the symptoms were easier to understand when their child was diagnosed with SMS. It would have been good to have the correct diagnosis earlier to adapt in a better way…. if we had known that the sleep issues were because of SMS, we would have acted differently. Now we thought it was because of us…that we didn’t act firmly enough (when he was little). We didn’t understand the reason for the challenging behaviours. We would have taken all the courses and classes if they had been offered. Nothing has been offered from the municipality, only by our own connections and by paying for it ourselves. We have learned different ways to handle the outbursts but have to renew ourselves all the time.
A gender difference was found in parents reporting their own lack of competence and lack of support, with more reports from parents of females with SMS. No age differences were found in this theme.
Theme 4: Parents’ experiences of professionals’ competence and understanding regarding children with SMS and their behaviour challenges
Some parents reported that they had been offered support, but from professionals that didn’t have the necessary specific knowledge of the syndrome, and therefore, the advice and recommendations didn’t fit or work out. They told about how professionals reacted and acted considering the children’s unusual sleep problems, variations in their developmental profiles and the fact that the person with SMS behaved distinctively differently at home towards their parents than outside the home towards professionals. The parents experienced inadequate advice telling them not to let their child sleep during daytime to make her or him sleep better at night; typically, they received this advice when their child was a toddler. They experienced a change when the kindergartens, schools or healthcare centres received information of the syndrome. One parent wrote that when the professionals were informed of the syndrome, the staff made changes leading to a decrease in this child’s outbursts. I think it was because it was not specific to this diagnosis. I think it was that. Because I always experienced that it didn’t fit (the advice).
Some parents expressed that professionals didn’t consider the rare disorder but acted as if the child just had an intellectual disability or ASD. It is not enough to just look at the level of ID…you have to specify things about the syndrome also…I think. …he cannot handle that independence, he doesn’t have a chance. But they all think he does, and the school thinks he does…. It is we that have been educating the preschool, school, and health care centres. I don’t think they understand how bad it is a home. I don’t think they have a chance to understand it…. I had, to be honest, problems to understand it myself, when she was younger.
Discussion
The most important finding from this study is that the parents experienced that there are some specific characteristics of SMS that professionals are not aware of or do not consider in their support services. Parents’ expressed that this lack of understanding exposed them to both more behavioural challenges from their child and more misunderstandings with the professionals. According to the parents, one of these characteristics is the uneven developmental profile. Persons with SMS often have developmental asynchrony with a discrepancy between intellectual development and emotional development in particular. This asynchrony means that they master skills at one level, but their emotional development and reactions are like a small child (Haas-Givler and Finucane, 2014). As one parent said: Because she looks very well-functioning, but she is not well-functioning at all, she needs a lot more support than you see at first glance.
Another important finding in this study is the extreme adaptations some of these families implement. Behaviours such as pretending to be dead to stop your child’s outburst or sleeping outside your child’s bedroom door for years are extreme and indicate to which length these parents are willing to go to take care of their child and themselves. Professional support and guidance in how to handle their child’s behaviours at home will be valuable for these families. Extreme adaptations need to be seen in relation to many parents’ reports that they didn’t receive any help with the behavioural challenges. Some parents were also of the opinion that if they had obtained help, the help would have been given from unqualified or unknowledgeable professionals.
The challenging behaviours in SMS have been described earlier (Sloneem et al., 2011). In the open-ended questionnaire we used in this study, the parents were asked to name the challenging behaviours their child displayed instead of checking them off a list, which is a more common approach in research on behavioural challenges. Self-injury, aggressive behaviours and inappropriate behaviours are well known within the syndrome, even though inappropriate behaviours were more emphasized and more often mentioned by the parents than anticipated and described earlier. Controlling behaviours are not mentioned in the literature in any extensive way. Parents attending courses at Frambu have been talking about these behaviours, but in this study, it came across as a substantial challenge for the families. This type of behaviour is an important topic to explore further.
There have previously been reported a gender difference regarding SMS and ASDs (Nag et al., 2018). A visual inspection of the demographics behind the statements was done in this study, and there might be a gender difference also in other areas than ASD, such as the number of challenging behaviours reported. Parents of females with SMS reported more challenging behaviour, more adaptations and more of a lack of competence and support. Since this is a qualitative study, the results need to be interpreted carefully and further investigated.
A similar visual inspection of the demographics behind the statements was done regarding differences between children below the age of 18 and adults. A difference was found in the number of challenging behaviours reported with more challenging behaviours reported by parents of children under the age of 18. This is the opposite of what is reported earlier in research where the challenging behaviour is found to increase with age (Finucane et al., 2001; Neira-Fresneda and Potocki, 2015; Poisson et al., 2015). Our study included more adults than previous research and that may be one of the reasons for the different results, but this needs further research. This is a qualitative study, and the results need to be interpreted carefully.
Some of the results in this study are similar to other research on parenting a child with a rare disorder (Griffith et al., 2011; Strehle and Middlemiss, 2007). The professionals’ lack of knowledge about the rare disorder was confirmed in Griffith et al.’s study from 2011 (Griffith et al., 2011). Research emphasizes that parents often need information about the main aspects of a specific syndrome and that specific characteristics of genetic syndromes influence the type of guidance the parents require (Pearson et al., 2018). Knowing about specific difficulties associated with a genetic syndrome may help with adapting to the environment in a different and more adequate way (Oliver et al., 2010). Specifically, having information about the link between the genetic disorder and the challenging behaviours seems to lead to a change in attitude among professionals from blaming the parents and the person with the diagnosis to increased optimism with regard to the possibility of change and increased willingness to help (Oliver et al., 2010).
Griffith et al. (2011) studied mothers’ experiences of social care support and medical services for their adult offspring with rare syndromes and found that both the professionals and the mothers first categorized their offspring as a person with an intellectual disability and second with a rare genetic disorder. The parents in our study expressed that they found it difficult that professionals only defined their children as having an intellectual disability or ASD. They experienced that this definition led to an insufficient adaptation of measures and more behaviour challenges.
Research over recent years has focused on how the professionals’ lack of knowledge put a strain on the person with the rare diagnosis and their parents (Haas-Givler and Finucane, 2014). However, with regard to SMS, knowledge is even more important. Some of the specific characteristics of this diagnosis have a substantial negative impact on the person with SMS and the whole family (Poisson et al., 2015). This impact is especially true if the support systems do not acknowledge these specific characteristics and seek advice and training to improve their counselling (Haas-Givler and Finucane, 2014).
In a study by Hodapp et al. (1998) comparing parents of children with SMS and Prader–Willi syndrome, they found a correlation between families’ stress level and the size of their support group, both private and professional. In the SMS group, professionals were more often listed in the families’ support group. Therefore, qualified professionals may be of greater importance to these parents than parents of children with other disorders. Other studies confirm that parents of children with SMS experience higher levels of family problems than parents of children with Down syndrome and Williams syndrome (Fidler et al., 2000) and parents of children with different aetiologies of intellectual disability (Hodapp et al., 1998). Sarimski (1997) found a correlation between parental stress and perceived social support. Our study also supports the findings that families having a family member with SMS are in great distress. Professionals, municipalities and other support systems need to be aware of these families and their overall needs for persistent and competent support.
Some of the results in this study agree with research on persons with disabilities, including research concerning children with behaviour challenges (Awijma et al., 1997; Griffith and Hastings, 2014; Richman et al., 2009). A high level of challenging behaviours have been correlated with elevated parental stress (Richman et al., 2009). A review from 2014 (Griffith and Hastings, 2014) confirms some of the findings from our study: the lack of support for challenging behaviours, the fact that the level of need exceeds the level of services and the lack of skilled support. The review also reported families who were satisfied with their received support, which we also found in our study. Future research should identify the families who are positive about the support they receive and identify the characteristics of both the families and the support so that different types of support systems may learn from it.
Limitations and strengths
One limitation in this study is that we chose to use open-ended questions in the questionnaire. Utilizing qualitative analysis of written responses has been questioned, both because of difficulties interpreting the written answers and the danger of asking leading questions. When asking respondents to write their answers down, you lose the ability to code and analyse body language or clarify orally (Ryen, 2002). It may also be an obstacle, both for the respondents and in the analysis, if the respondents are not comfortable with or have trouble expressing themselves in writing (Creswell, 2013; Ryen, 2002). We still chose this method because, to our knowledge, this study is the first qualitative study of parents of children with SMS focused on behaviours. It was important to be able to include parents from Norway, Sweden and Denmark, and we would have faced complications with both logistics and language if we chose face-to-face interviews. We assess using open-ended questions also as a strength because this opened up for statements and themes that have never before been considered in research on SMS. We added face-to-face interviews with four parents to strengthen and broaden our findings.
A limitation in phenomenological research is that the researchers’ own preconception and experiences may influence the analysis process and the selection of citations.
Limitations in generalizability or transferability are often raised regarding qualitative research (Creswell, 2013; Malterud, 2001). The possibility to transfer the results to similar populations is often a goal in quantitative research, but this is not the main purpose in qualitative research. Some of our results may be unique to the Scandinavian population due to the similarity in the social systems they benefit from. These systems may be different in other countries. It is a strength to the transferability possibilities that we have participants from three different countries and that we have recruited approximately 50% of the known population in both Sweden and Norway.
Conclusions
In this study, we found that parents of children with SMS experience that they are exposed to both more behaviour challenges from their child and more misunderstandings with professionals and they believe that is because there are some specific characteristics of SMS that professionals are not aware of or do not consider in their support services. In particular, the uneven profile and the display of the more severe behaviours directed towards close relatives seems to amplify the parents’ problems. We also found that these parents implement some extreme adaptations to meet the challenging behaviour that their children with SMS display, and there is an unmet need for qualified and knowledgeable support for these families. It is especially important that professionals working with persons with SMS or families where a person is diagnosed with SMS increase their knowledge about the disorder. According to the parents, the professionals need to make an effort to listen to the families regarding what type of support and help they need and try to base their actions on their views.
Footnotes
Authors’ note
The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (REC # 2015/1026).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Norwegian National Advisory Unit on Rare Diseases.